
Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
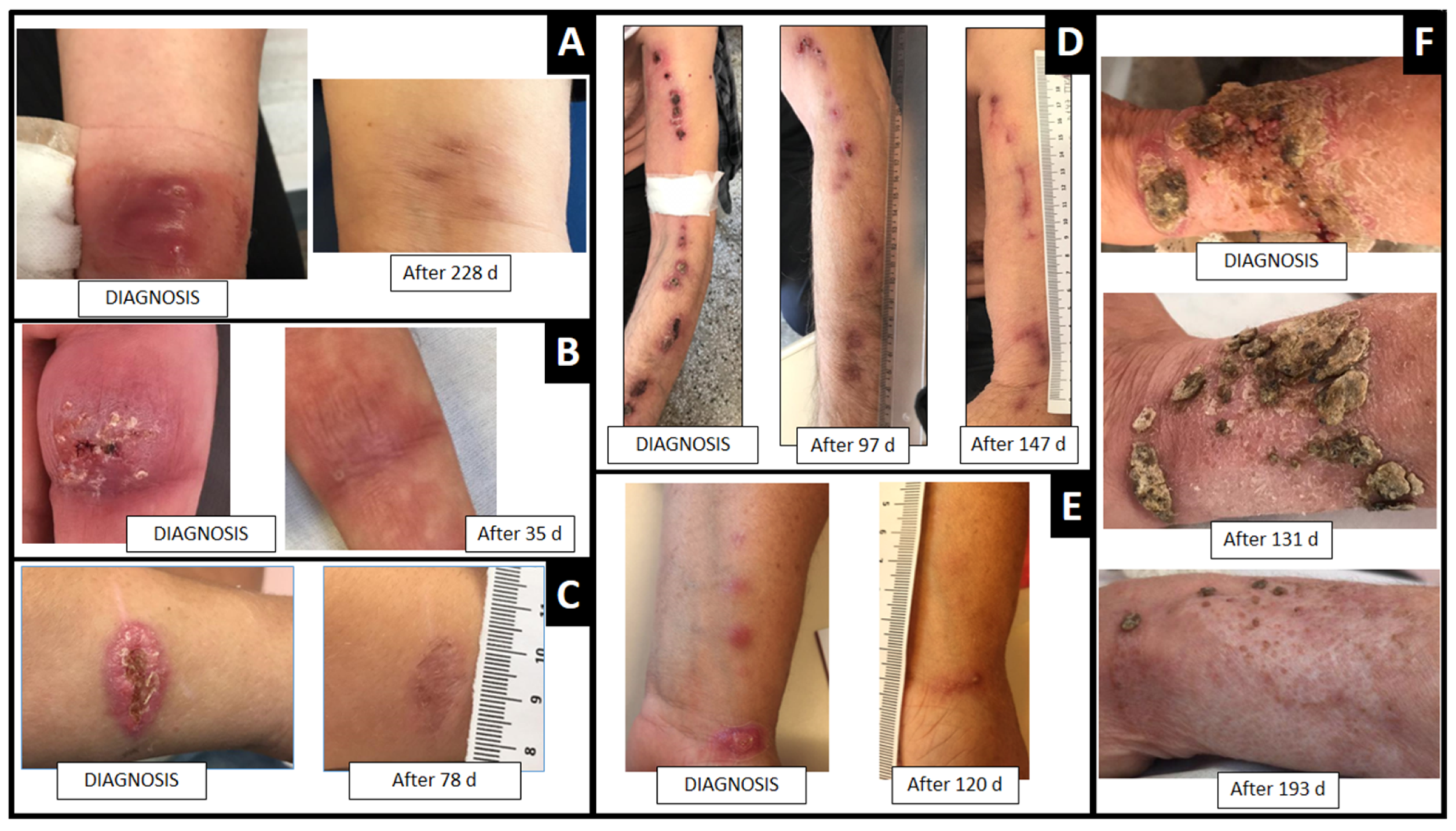
3.1. Adult Cases
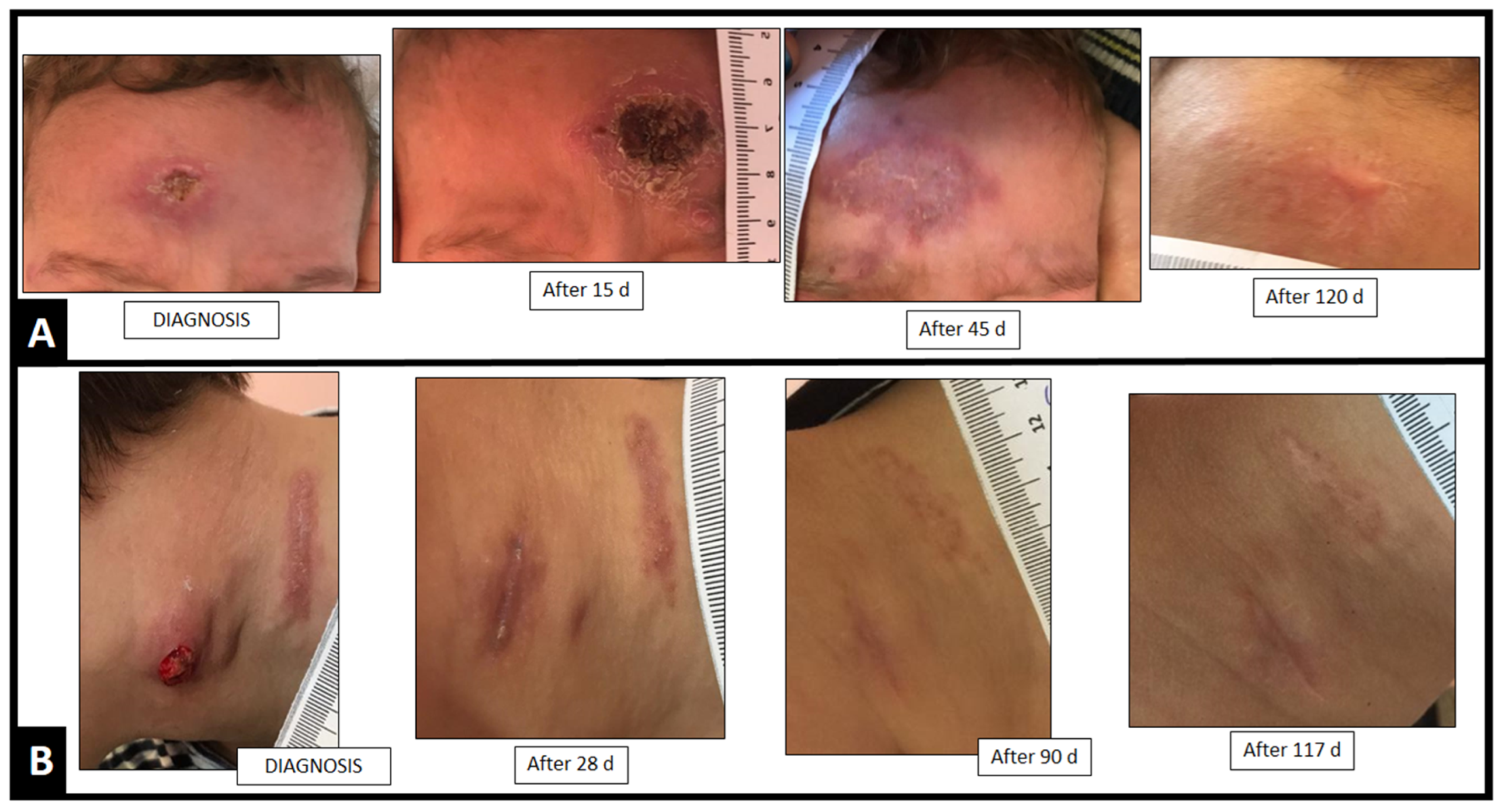
3.2. Pediatric Cases
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gremião, I.D.F.; Oliveira, M.M.E.; de Miranda, L.H.M.; Freitas, D.F.S.; Pereira, S.A. Geographic Expansion of Sporotrichosis, Brazil. Emerg. Infect. Dis. 2020, 26, 621–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, M.B.d.L.; Schubach, A.O.; de Oliveira, R.d.V.C.; Martins, E.B.; Teixeira, J.L.; Wanke, B. Treatment of Cutaneous Sporotrichosis with Itraconazole—Study of 645 Patients. Clin. Infect. Dis. 2011, 52, e200–e206. [Google Scholar] [CrossRef] [PubMed]
- Brandolt, T.M.; Madrid, I.M.; Poester, V.R.; Sanchotene, K.O.; Basso, R.P.; Klafke, G.B.; Rodrigues, M.d.L.; Xavier, M.O. Human Sporotrichosis: A Zoonotic Outbreak in Southern Brazil, 2012–2017. Med. Mycol. 2018, 57, 527–533. [Google Scholar] [CrossRef]
- Kauffman, C.A.; Bustamante, B.; Chapman, S.W.; Pappas, P.G. Clinical Practice Guidelines for the Management of Sporotrichosis: 2007 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 1255–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Terra, P.P.; Rodrigues, A.M.; Fernandes, G.F.; Nishikaku, A.S.; Burger, E.; de Camargo, Z.P. Exploring Virulence and Immunogenicity in the Emerging Pathogen Sporothrix brasiliensis. PLoS Negl. Trop. Dis. 2017, 11, e0005903. [Google Scholar] [CrossRef]
- Falcão, E.M.M.; Pires, M.C.d.S.; Andrade, H.B.; Gonçalves, M.L.C.; Almeida-Paes, R.; do Valle, A.C.F.; Bastos, F.I.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Zoonotic Sporotrichosis with Greater Severity in Rio de Janeiro, Brazil: 118 Hospitalizations and 11 Deaths in the Last 2 Decades in a Reference Institution. Med. Mycol. 2019, 58, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; Oliveira, M.M.E.; Freitas, D.F.S.; Valle, A.C.F.d.; Gutierrez-Galhardo, M.C.; Zancopé-Oliveira, R.M. Refractory Sporotrichosis Due to Sporothrix brasiliensis in Humans Appears to Be Unrelated to in Vivo Resistance. Med. Mycol. 2017, 55, 507–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonifaz, A.; Saúl, A.; Paredes-Solis, V.; Fierro, L.; Rosales, A.; Palacios, C.; Araiza, J. Sporotrichosis in Childhood: Clinical and Therapeutic Experience in 25 Patients. Pediatr. Dermatol. 2007, 24, 369–372. [Google Scholar] [CrossRef]
- Caus, A.L.O.; Zanotti, R.L.; Faccini-Martínez, Á.A.; Paterlini, G.V.; Falqueto, A. Epidemiological and Clinical Aspects of Sporotrichosis in Espírito Santo State, Southeast Brazil: A Study of Three Decades (1982–2012). Am. J. Trop. Med. Hyg. 2019, 100, 706–713. [Google Scholar] [CrossRef] [Green Version]
- Macotela-Ruiz, E.; Nochebuena-Ramos, E. Esporotricosis En Algunas Comunidades Rurales de La Sierra Norte de Puebla. Informe de 55 Casos (Septiembre 1995–Diciembre 2005). Gac. Med. Mex. 2006, 142, 377–380. [Google Scholar]
- Yamada, K.; Zaitz, C.; Framil, V.M.d.S.; Muramatu, L.H. Cutaneous Sporotrichosis Treatment with Potassium Iodide. A 24 Year Experience in São Paulo State, Brazil. Rev. Inst. Med. Trop. São Paulo 2011, 53, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.; Mahajan, V.K.; Singh Chauhan, P.; Mehta, K.S.; Sharma, A.; Sharma, J. The Clinico-Epidemiological Characteristics and Therapeutic Experience of 152 Patients with Cutaneous Sporotrichosis: A 10-Year Retrospective Study from India. Int. J. Dermatol. 2021, 60, 99–106. [Google Scholar] [CrossRef]
- Sivagnanam, S.; Bannan, A.M.; Chen, S.C.A.; Ralph, A.P. Sporotrichosis (Sporothrix Schenckii Infection) in the New South Wales Mid-North Coast, 2000–2010. Med. J. Aust. 2012, 196, 588–590. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Yao, L.; Zhong, S.X.; Tian, Y.P.; Liu, Y.Y.; Li, S.S. Infant Sporotrichosis in Northeast China: A Report of 15 Cases. Int. J. Dermatol. 2011, 50, 522–529. [Google Scholar] [CrossRef]
- Takenaka, M.; Yoshizaki, A.; Utani, A.; Nishimoto, K. A Survey of 165 Sporotrichosis Cases Examined in Nagasaki Prefecture from 1951 to 2012. Mycoses 2014, 57, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.M.; Tang, J.J.; Gill, P.; Chang, C.C.; Baba, R. Cutaneous Sporotrichosis: A Six-Year Review of 19 Cases in a Tertiary Referral Center in Malaysia. Int. J. Dermatol. 2012, 51, 702–708. [Google Scholar] [CrossRef]
- Sharkey-Mathis, P.K.; Kauffman, C.A.; Graybill, J.R.; Stevens, D.A.; Hostetler, J.; Cloud, G.; Dismukes, W.E. Treatment of Sporotrichosis with Itraconazole. Am. J. Med. 1993, 95, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.M.; Teixeira, M.d.M.; de Hoog, G.S.; Schubach, T.M.P.; Pereira, S.A.; Fernandes, G.F.; Bezerra, L.M.L.; Felipe, M.S.; de Camargo, Z.P. Phylogenetic Analysis Reveals a High Prevalence of Sporothrix brasiliensis in Feline Sporotrichosis Outbreaks. PLoS Negl. Trop. Dis. 2013, 7, e2281. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.M.; Hoog, G.S.; Camargo, Z.P. Molecular Diagnosis of Pathogenic Sporothrix Species. PLoS Negl. Trop. Dis. 2015, 9, e0004190. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.; Procop, G.; Dufresne, P.; Espinel-Ingroff, A.; Fuller, J.; Ghannoum, M.; Hanson, K.; Holliday, D.; Kovanda, L.; Ostrosky-Zeichner, L.; et al. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, M38ED3, 3rd ed.; Clinical And Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Espinel-Ingroff, A.; Abreu, D.P.B.; Almeida-Paes, R.; Brilhante, R.S.N.; Chakrabarti, A.; Chowdhary, A.; Hagen, F.; Córdoba, S.; Gonzalez, G.M.; Govender, N.P.; et al. Multicenter, International Study of MIC/MEC Distributions for Definition of Epidemiological Cutoff Values for Sporothrix Species Identified by Molecular Methods. Antimicrob. Agents Chemother. 2017, 61, e01057-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, G.R.; Le, T.; Chindamporn, A.; Kauffman, C.A.; Alastruey-Izquierdo, A.; Ampel, N.M.; Andes, D.R.; Armstrong-James, D.; Ayanlowo, O.; Baddley, J.W.; et al. Global Guideline for the Diagnosis and Management of the Endemic Mycoses: An Initiative of the European Confederation of Medical Mycology in Cooperation with the International Society for Human and Animal Mycology. Lancet Infect. Dis. 2021, 21, e364–e374. [Google Scholar] [CrossRef]
- Poester, V.R.; Munhoz, L.S.; Larwood, D.; Martinez, M.; Stevens, D.A.; Xavier, M.O. Potential Use of Nikkomycin Z as an Anti- Sporothrix Spp. Drug. Med. Mycol. 2020, 59, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Poester, V.R.; Munhoz, L.S.; Nogueira, C.W.; Zeni, G.R.; Stevens, D.A.; Xavier, M.O. Diphenyl diselenide alone and in combination with itraconazole against Sporothrix schenckii s.s. and Sporothrix globosa. Braz. J. Microbiol. 2021, 52, 1271–1274. [Google Scholar] [CrossRef] [PubMed]
- Poester, V.R.; Munhoz, L.S.; Benelli, J.L.; Klafke, G.B.; Nogueira, C.W.; Zeni, G.R.; Stevens, D.A.; Larwood, D.; Xavier, M.O. Synergism of nikkomycin Z in combination with diphenyl diselenide against Sporothrix spp. Curr. Microbiol. 2021, 78, 2905–2909. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
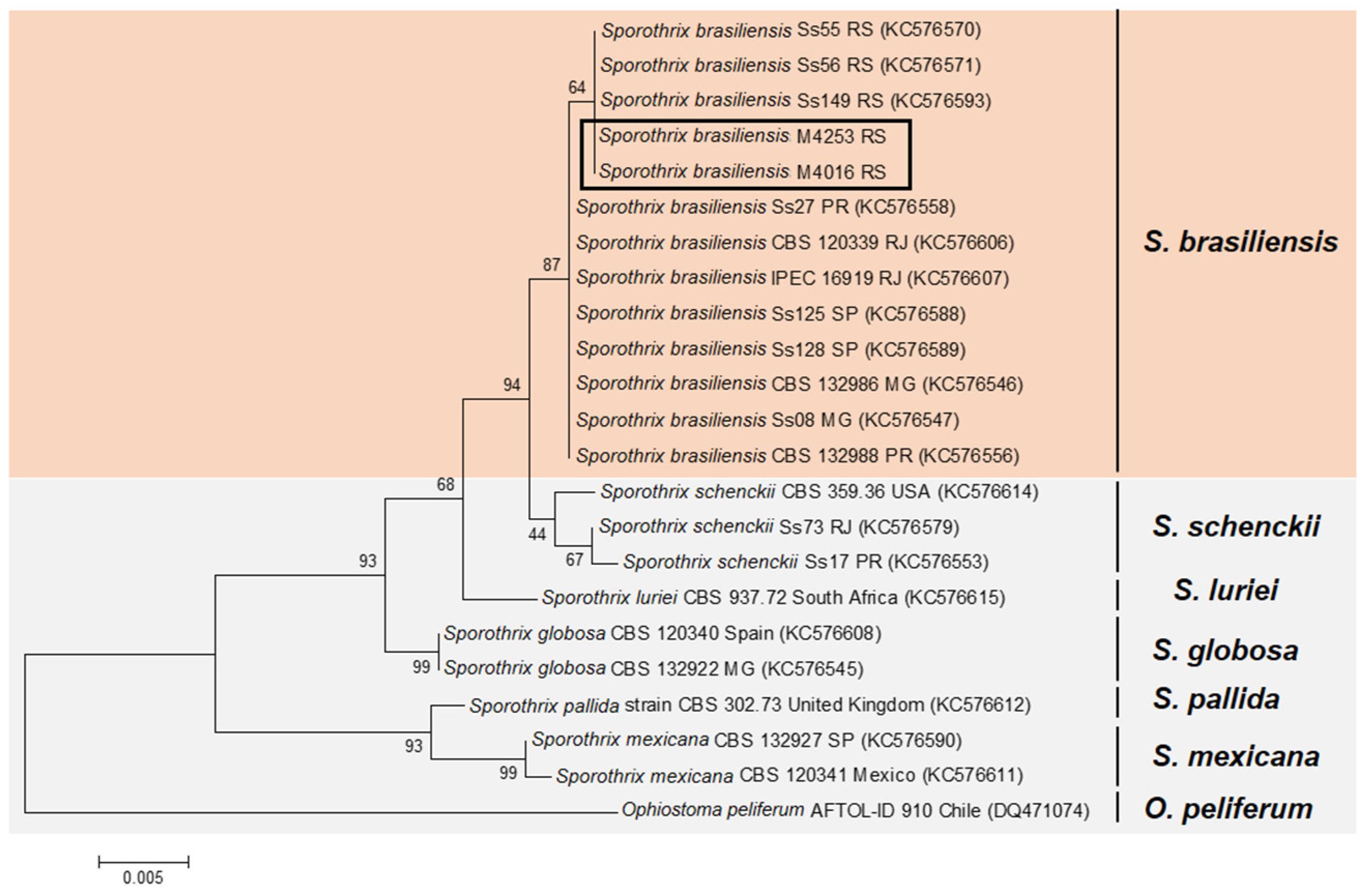
| Isolate Code | Species | Geographic Origin | GenBank EF1α |
|---|---|---|---|
| CBS 120339 | S. brasiliensis | Rio de Janeiro, RJ, Brazil | KC576606 |
| IPEC 16919 | S. brasiliensis | Rio de Janeiro, RJ, Brazil | KC576607 |
| Ss55 | S. brasiliensis | Rio Grande, RS, Brazil | KC576570 |
| Ss56 | S. brasiliensis | Rio Grande, RS, Brazil | KC576571 |
| Ss149 | S. brasiliensis | Pelotas, RS, Brazil | KC576593 |
| M4016 | S. brasiliensis | Rio Grande, RS, Brazil | OL853841 |
| M4253 | S. brasiliensis | Rio Grande, RS, Brazil | OL853842 |
| CBS 132988 | S. brasiliensis | Curitiba, PR, Brazil | KC576556 |
| Ss27 | S. brasiliensis | Curitiba, PR, Brazil | KC576558 |
| Ss125 | S. brasiliensis | Campinas, SP, Brazil | KC576588 |
| Ss128 | S. brasiliensis | Campinas, SP, Brazil | KC576589 |
| CBS 132986 | S. brasiliensis | Belo Horizonte, MG, Brazil | KC576546 |
| Ss08 | S. brasiliensis | Belo Horizonte, MG, Brazil | KC576547 |
| CBS 359.36 | S. schenckii | United States of America | KC576614 |
| Ss73 | S. schenckii | Rio de Janeiro, RJ, Brazil | KC576579 |
| Ss17 | S. schenckii | Curitiba, PR, Brazil | KC576553 |
| CBS 120340 | S. globosa | Spain | KC576608 |
| CBS 132922 | S. globosa | Belo Horizonte, MG, Brazil | KC576545 |
| CBS 120341 | S. mexicana | Mexico | KC576611 |
| CBS 132927 | S. mexicana | São Paulo, SP, Brazil | KC576590 |
| CBS 937.72 | S. luriei | South Africa | KC576615 |
| CBS 302.73 | S. pallida | United Kingdom | KC576612 |
| AFTOL-ID 910 | Ophiostoma piliferum | Chile | DQ471074 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poester, V.R.; Basso, R.P.; Stevens, D.A.; Munhoz, L.S.; de Souza Rabello, V.B.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Zanchi, M.; Benelli, J.L.; Xavier, M.O. Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis. J. Fungi 2022, 8, 70. https://doi.org/10.3390/jof8010070
Poester VR, Basso RP, Stevens DA, Munhoz LS, de Souza Rabello VB, Almeida-Paes R, Zancopé-Oliveira RM, Zanchi M, Benelli JL, Xavier MO. Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis. Journal of Fungi. 2022; 8(1):70. https://doi.org/10.3390/jof8010070
Chicago/Turabian StylePoester, Vanice Rodrigues, Rossana Patricia Basso, David A. Stevens, Lívia Silveira Munhoz, Vanessa Brito de Souza Rabello, Rodrigo Almeida-Paes, Rosely Maria Zancopé-Oliveira, Mariza Zanchi, Jéssica Louise Benelli, and Melissa Orzechowski Xavier. 2022. "Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis" Journal of Fungi 8, no. 1: 70. https://doi.org/10.3390/jof8010070
APA StylePoester, V. R., Basso, R. P., Stevens, D. A., Munhoz, L. S., de Souza Rabello, V. B., Almeida-Paes, R., Zancopé-Oliveira, R. M., Zanchi, M., Benelli, J. L., & Xavier, M. O. (2022). Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis. Journal of Fungi, 8(1), 70. https://doi.org/10.3390/jof8010070