
Automated Landmark Annotation for Morphometric Analysis of Distal Femur and Proximal Tibia

 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Data and Workflow
2.1.1. Manual Segmentation
2.1.2. Manual Landmark Annotation
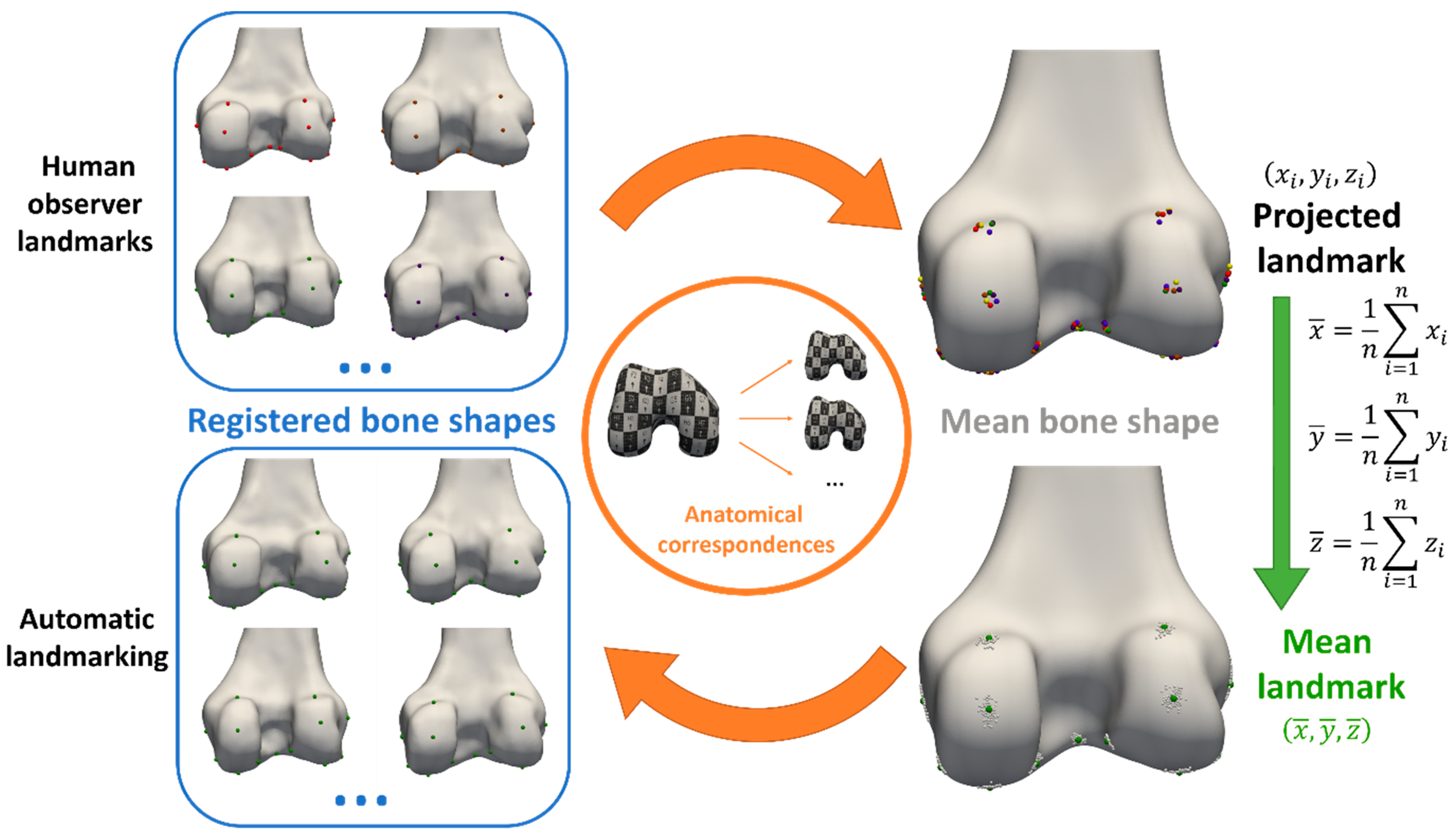
2.1.3. Automated Landmark Annotation
Registration of 3D Bone and Cartilage Models
Landmark Propagation
3. Observations
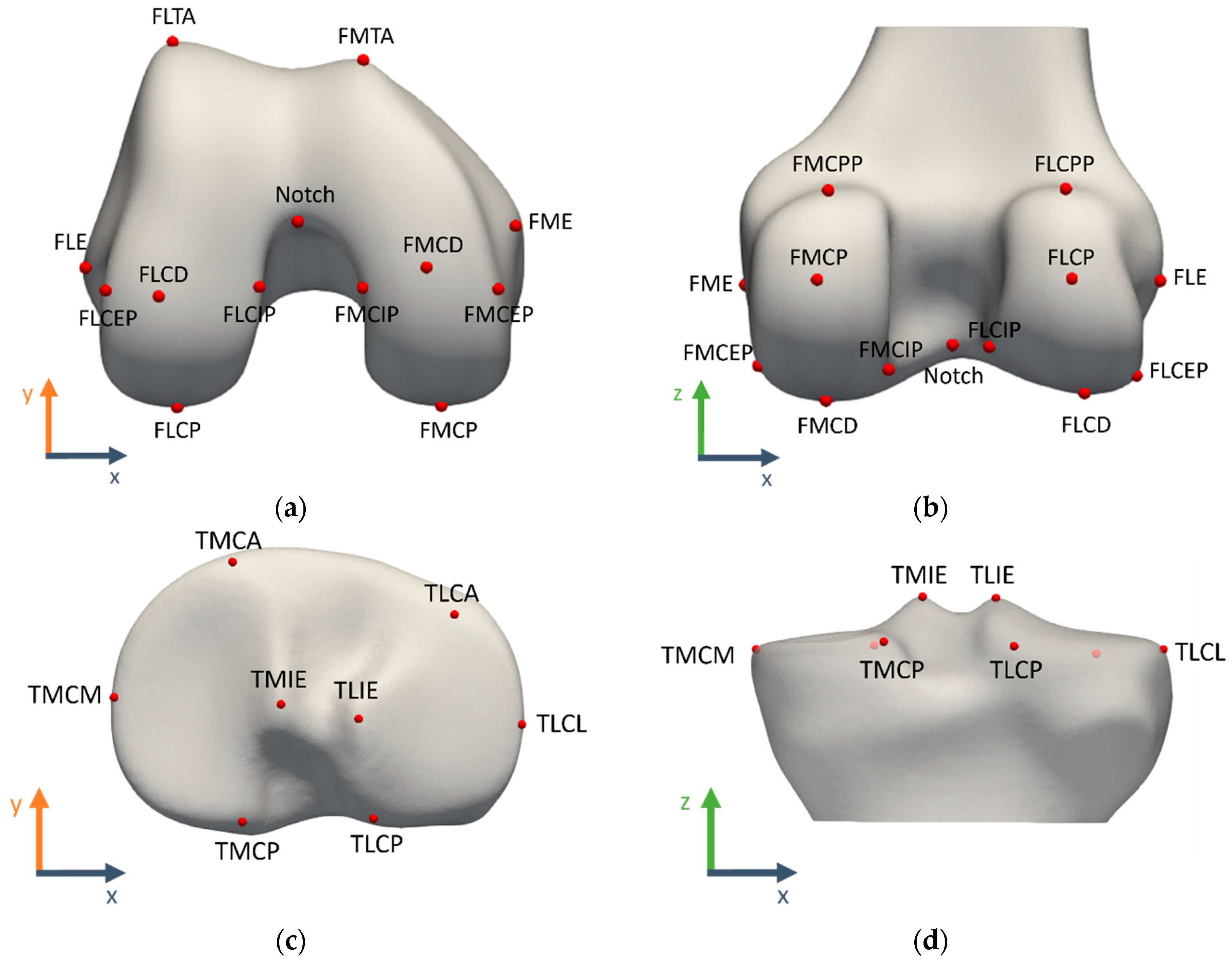
3.1. Landmark Definitions
3.1.1. Reference Coordinate System Definition
- x-axis (mediolateral): parallel to the femoral posterior condylar line, defined by the FMCP and FLCP landmarks (mean of 3 observers as ground truth)
- y-axis (anteroposterior): common perpendicular to the x- and z-axes
- z-axis (proximodistal): MRI patient table movement direction
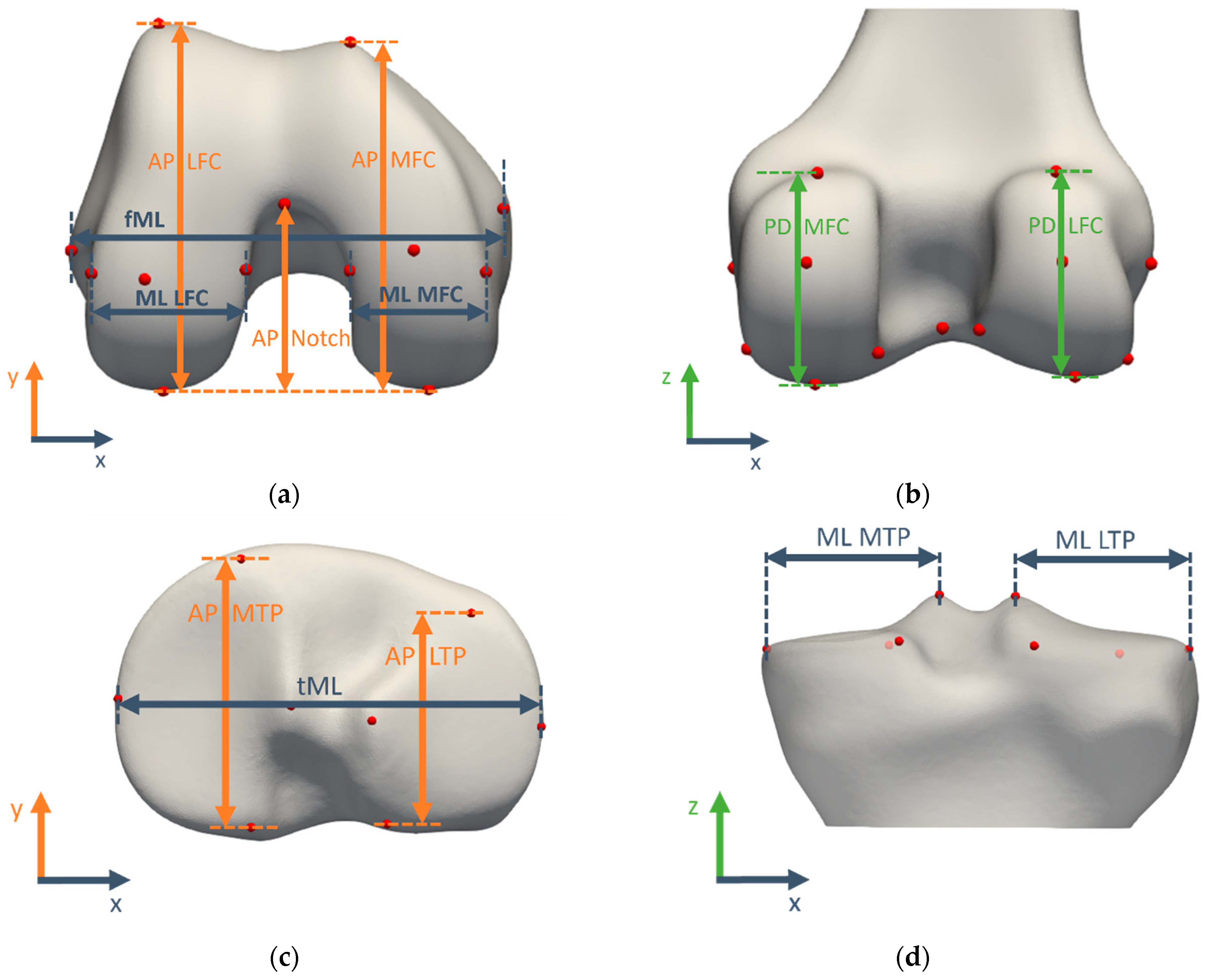
3.1.2. Morphometric Measurement Definitions
3.2. Validation Study for Manual Morphometric Analysis
3.2.1. Landmark Validation
3.2.2. Measurement Validation
3.3. Validation Study for Automated Morphometric Analysis
3.3.1. Automated Landmark Validation
3.3.2. Automated Measurement Validation
3.4. Time Consumption
3.5. Statistical Analysis
3.5.1. Landmark Positions
3.5.2. Measurements
4. Results
4.1. Validation Study for Manual Morphometric Analysis
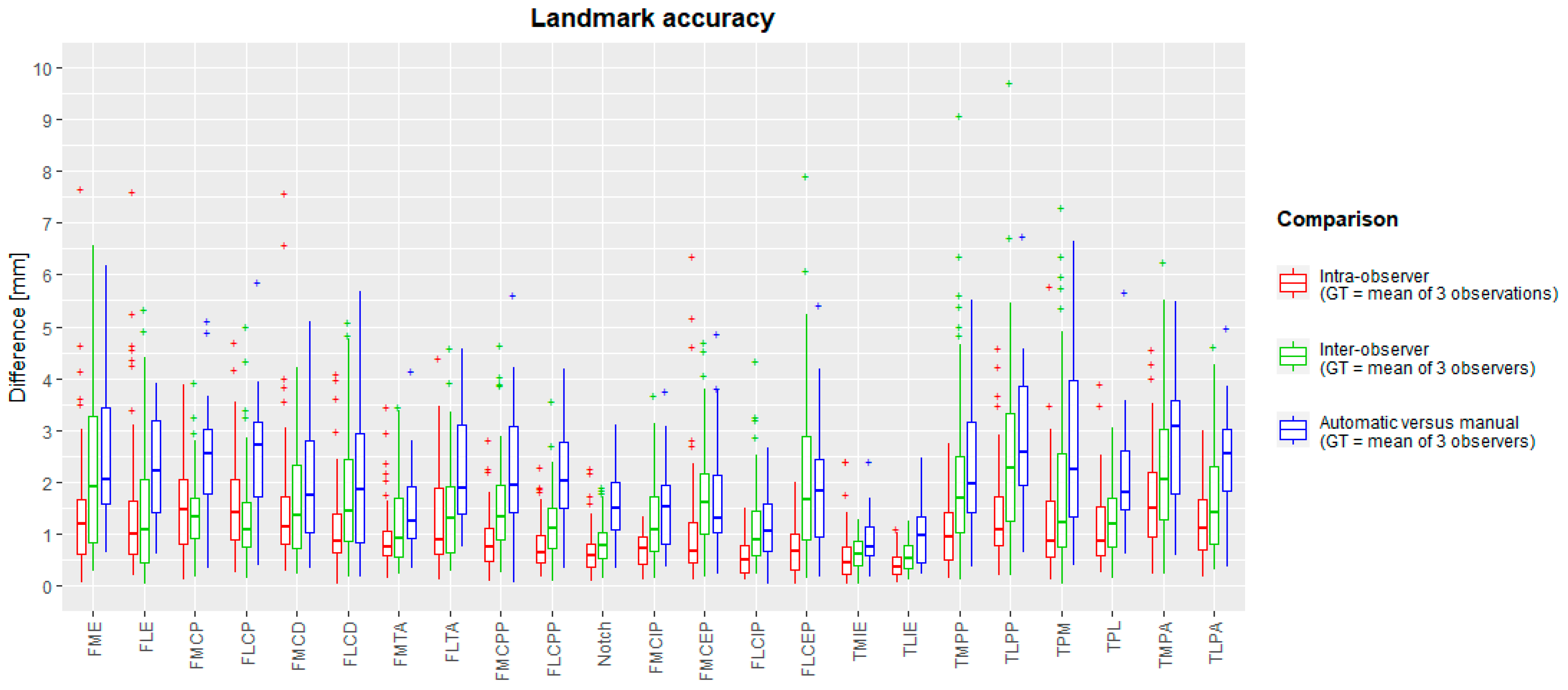
4.1.1. Manual Landmark Position Validation
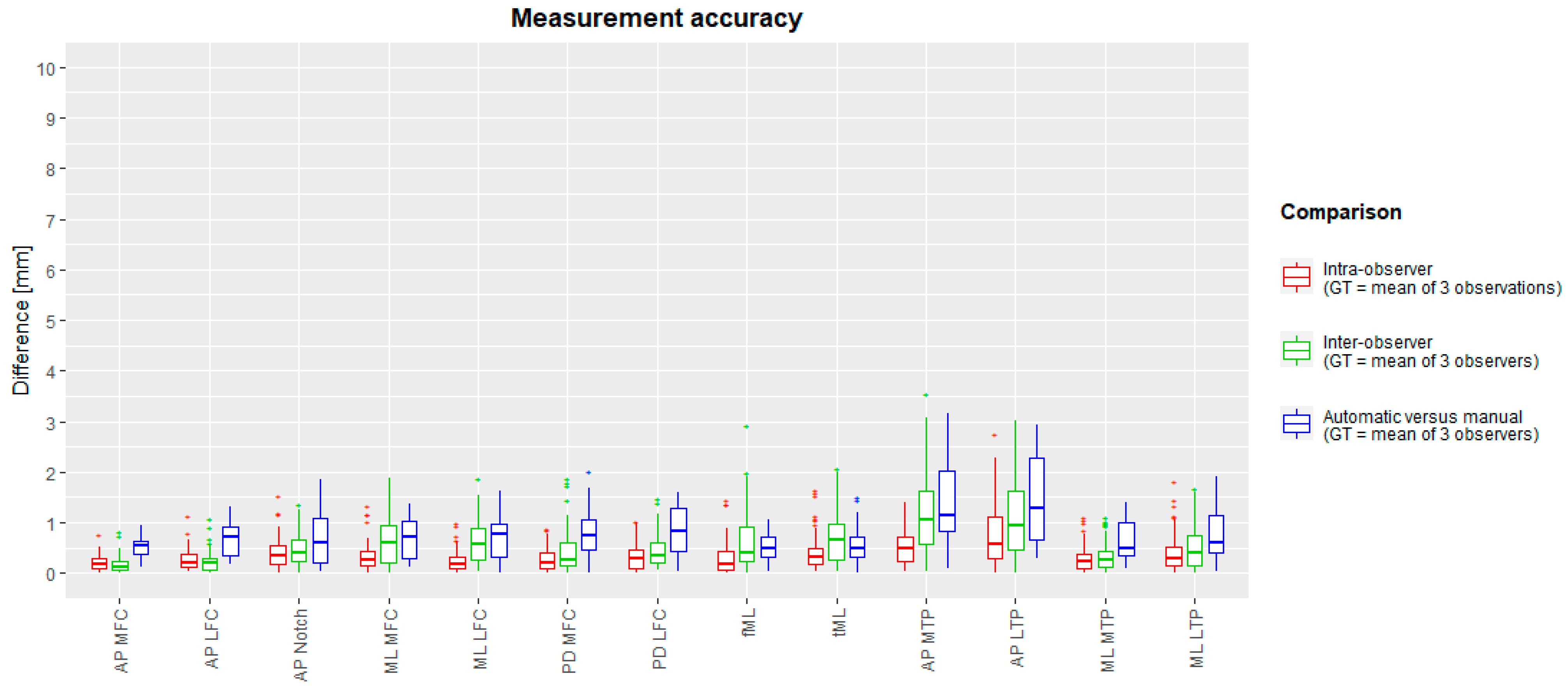
4.1.2. Manual Measurement Validation
4.2. Validation Study for Automated Morphometric Analysis
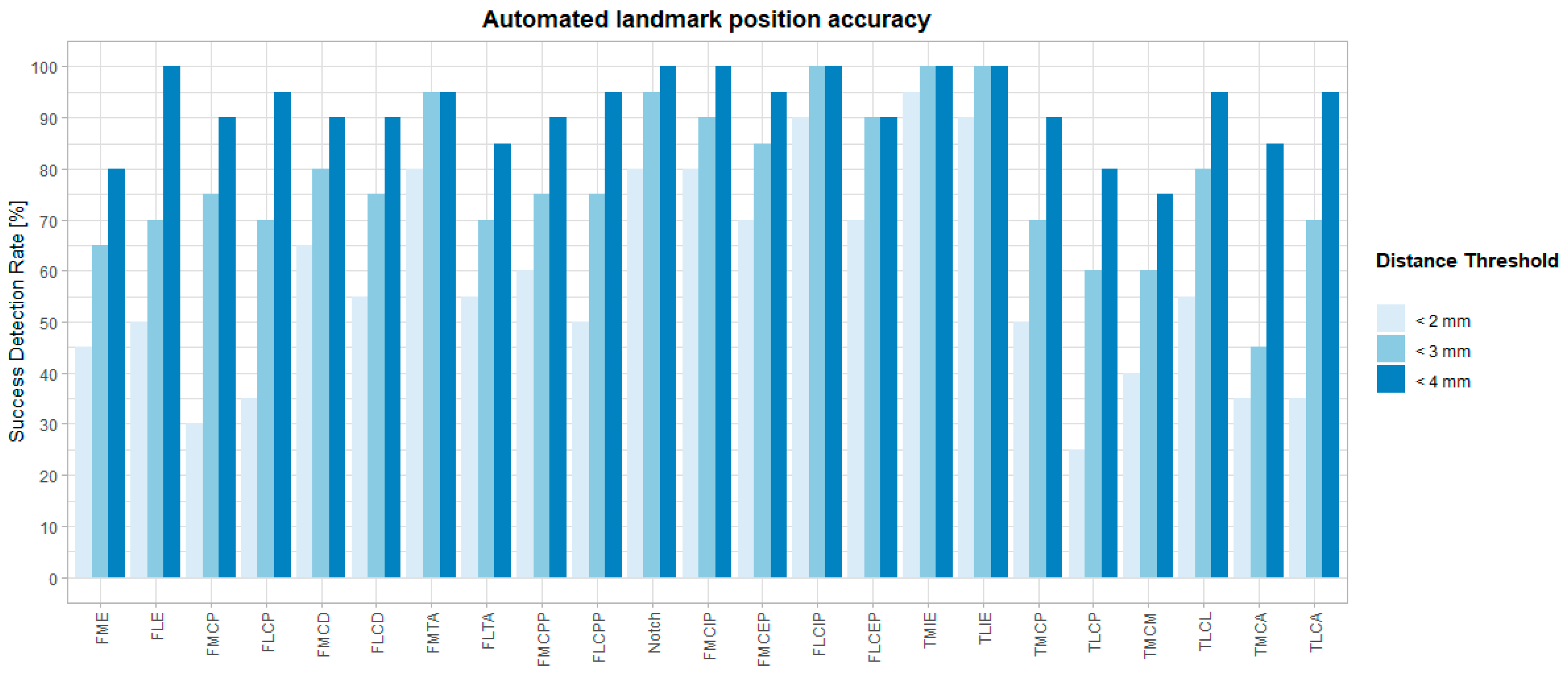
4.2.1. Automated Landmark Validation
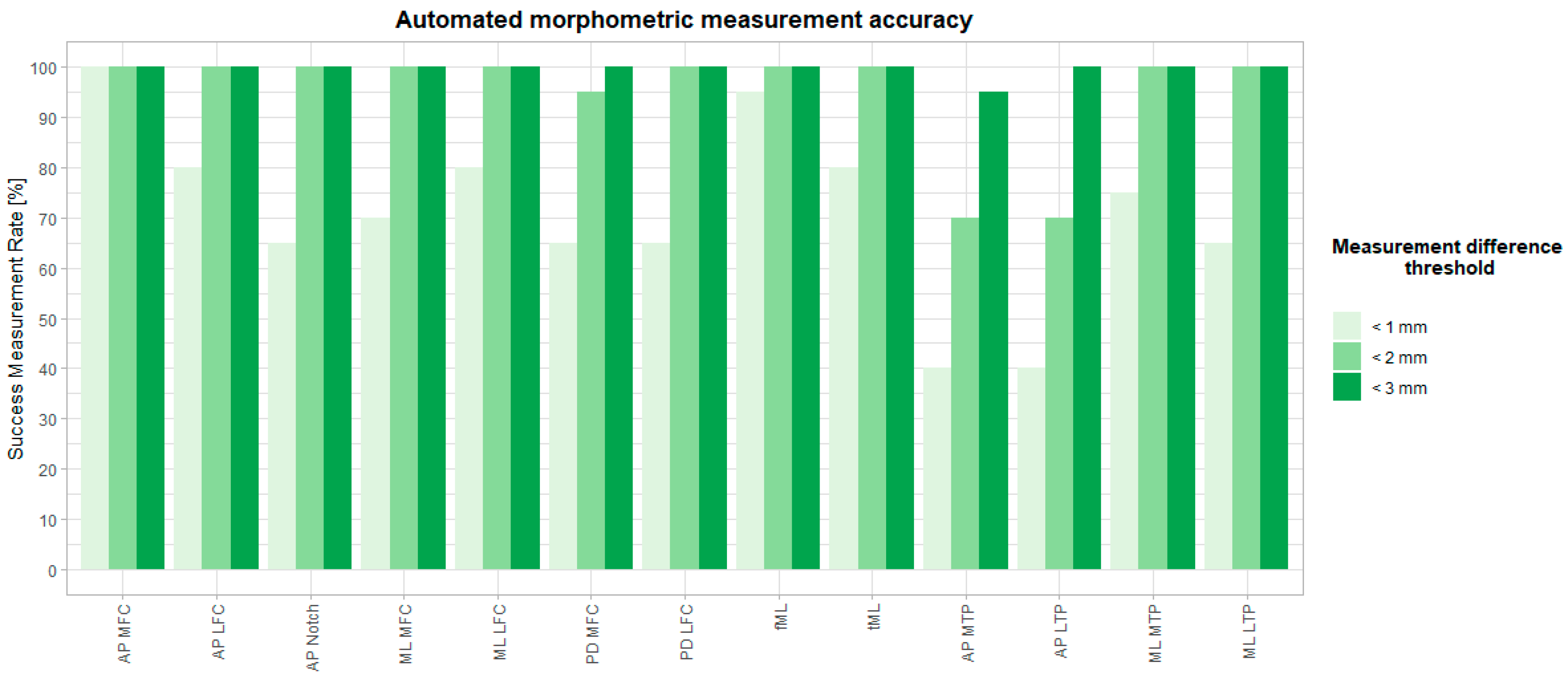
4.2.2. Automated Measurement Validation
4.3. Time Consumption
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beeler, S.; Vlachopoulos, L.; Jud, L.; Sutter, R.; Fürnstahl, P.; Fucentese, S.F. Contralateral MRI scan can be used reliably for three-dimensional meniscus sizing—Retrospective analysis of 160 healthy menisci. Knee 2019, 26, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Bermejo, E.; Taniguchi, K.; Ogawa, Y.; Martos, R.; Valsecchi, A.; Mesejo, P.; Ibáñez, O.; Imaizumi, K. Automatic landmark annotation in 3D surface scans of skulls: Methodological proposal and reliability study. Comput. Methods Programs Biomed. 2021, 210, 106380. [Google Scholar] [CrossRef]
- Danckaers, F.; Huysmans, T.; Lacko, D.; Ledda, A.; Verwulgen, S.; Van Dongen, S.; Sijbers, J. Correspondence Preserving Elastic Surface Registration with Shape Model Prior. In Proceedings of the 2014 22nd International Conference on Pattern Recognition, Stockholm, Sweden, 24–28 August 2014; pp. 2143–2148. [Google Scholar]
- Van Dyck, P.; Smekens, C.; Roelant, E.; Vande Vyvere, T.; Snoeckx, A.; De Smet, E. 3D CAIPIRINHA SPACE versus standard 2D TSE for routine knee MRI: A large-scale interchangeability study. Eur. Radiol. 2022, 32, 6456–6467. [Google Scholar] [CrossRef] [PubMed]
- Fürmetz, J.; Sass, J.; Ferreira, T.; Jalali, J.; Kovacs, L.; Mück, F.; Degen, N.; Thaller, P.H. Three-dimensional assessment of lower limb alignment: Accuracy and reliability. Knee 2019, 26, 185–193. [Google Scholar] [CrossRef]
- Gamer, M.; Lemon, J.; Fellows, I.; Singh, P. irr: Various Coefficients of Interrater Reliability and Agreement, R Package Version 0.84.1. 2019. Available online: https://cran.r-project.org/web/packages/irr/irr.pdf (accessed on 20 February 2024).
- Grammens, J.; Van Haver, A.; Danckaers, F.; Booth, B.; Sijbers, J.; Verdonk, P. Small medial femoral condyle morphotype is associated with medial compartment degeneration and distinct morphological characteristics: A comparative pilot study. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 1777–1789. [Google Scholar] [CrossRef]
- Gupta, A.; Kharbanda, O.P.; Sardana, V.; Balachandran, R.; Sardana, H.K. A knowledge-based algorithm for automatic detection of cephalometric landmarks on CBCT images. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1737–1752. [Google Scholar] [CrossRef]
- Van Haver, A.; De Roo, K.; De Beule, M.; Van Cauter, S.; Audenaert, E.; Claessens, T.; Verdonk, P. Semi-automated landmark-based 3D analysis reveals new morphometric characteristics in the trochlear dysplastic femur. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2698–2708. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Harris, S.; Zhou, T.; Roby, G.B.; Preston, B.; Rivière, C. Which method for femoral component sizing when performing kinematic alignment TKA? An in silico study. Orthop. Traumatol. Surg. Res. 2023, 110, 103769. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Kuiper, R.J.A.; Seevinck, P.R.; Viergever, M.A.; Weinans, H.; Sakkers, R.J.B. Automatic Assessment of Lower-Limb Alignment from Computed Tomography. J. Bone Jt. Surg. 2023, 105, 700–712. [Google Scholar] [CrossRef]
- MacLeod, A.R.; Roberts, S.A.; Gill, H.S.; Mandalia, V.I. A simple formula to control posterior tibial slope during proximal tibial osteotomies. Clin. Biomech. 2023, 110, 106125. [Google Scholar] [CrossRef] [PubMed]
- Martin Bland, J.; Altman Douglas, G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- van der Merwe, J.; van den Heever, D.J.; Erasmus, P. Variability, agreement and reliability of MRI knee landmarks. J. Biomech. 2019, 95, 109309. [Google Scholar] [CrossRef]
- Nguyen, V.; Alves Pereira, L.F.; Liang, Z.; Mielke, F.; Van Houtte, J.; Sijbers, J.; De Beenhouwer, J. Automatic landmark detection and mapping for 2D/3D registration with BoneNet. Front. Vet. Sci. 2022, 9, 923449. [Google Scholar] [CrossRef]
- Peeters, W.; Van Haver, A.; Van den Wyngaert, S.; Verdonk, P. A landmark-based 3D analysis reveals a narrower tibial plateau and patella in trochlear dysplastic knees. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2224–2232. [Google Scholar] [CrossRef]
- Porto, A.; Rolfe, S.; Maga, A.M. ALPACA: A fast and accurate computer vision approach for automated landmarking of three-dimensional biological structures. Methods Ecol. Evol. 2021, 12, 2129–2144. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing (Version 4.2.1); R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Richard, A.H.; Parks, C.L.; Monson, K.L. Accuracy of standard craniometric measurements using multiple data formats. Forensic. Sci. Int. 2014, 242, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Ridel, A.; Demeter, F.; Galland, M.; L’abbé, E.; Vandermeulen, D.; Oettlé, A. Automatic landmarking as a convenient prerequisite for geometric morphometrics. Validation on cone beam computed tomography (CBCT)—Based shape analysis of the nasal complex. Forensic. Sci. Int. 2020, 306, 110095. [Google Scholar] [CrossRef]
- Schroeder, W.; Martin, K.; Lorensen, B. The Visualization Toolkit, 4th ed.; Kitware: Clifton Park, NY, USA, 2006. [Google Scholar]
- Seim, H.; Kainmueller, D.; Heller, M.; Zachow, S.; Hege, H.-C. Automatic extraction of anatomical landmarks from medical image data: An evaluation of different methods. In Proceedings of the 2009 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Boston, MA, USA, 28 June–1 July 2009; pp. 538–541. [Google Scholar]
- Serafin, M.; Baldini, B.; Cabitza, F.; Carrafiello, G.; Baselli, G.; Del Fabbro, M.; Sforza, C.; Caprioglio, A.; Tartaglia, G.M. Accuracy of automated 3D cephalometric landmarks by deep learning algorithms: Systematic review and meta-analysis. Radiol. Med. 2023, 128, 544–555. [Google Scholar] [CrossRef]
- Smith, A.C.; Boaks, A. How “standardized” is standardized? A validation of postcranial landmark locations. J. Forensic. Sci. 2014, 59, 1457–1465. [Google Scholar] [CrossRef]
- Valette, S.; Chassery, J.M.; Prost, R. Generic remeshing of 3D triangular meshes with metric-dependent discrete voronoi diagrams. IEEE Trans. Vis. Comput. Graph. 2008, 14, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Victor, J.; Van Doninck, D.; Labey, L.; Innocenti, B.; Parizel, P.M.; Bellemans, J. How precise can bony landmarks be determined on a CT scan of the knee? Knee 2009, 16, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Wilke, F.; Matthews, H.; Herrick, N.; Dopkins, N.; Claes, P.; Walsh, S. Automated 3D Landmarking of the Skull: A Novel Approach for Craniofacial Analysis. bioRxiv 2024. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronym | Landmark | Definition |
|---|---|---|
| FME | Femoral medial epicondyle | The most anterior and distal osseous prominence over the medial aspect of the 3D distal femur. |
| FLE | Femoral lateral epicondyle | The most anterior and distal osseous prominence over the lateral aspect of the 3D distal femur. |
| FMCP | Femoral medial condyle posterior | The most posterior point of the medial condyle on the 3D femur. |
| FLCP | Femoral lateral condyle posterior | The most posterior point of the lateral condyle on the 3D femur. |
| FMCD | Femoral medial condyle distal | The most distal point on the medial condyle on the 3D femur. |
| FLCD | Femoral lateral condyle distal | The most distal point on the lateral femoral condyle on the 3D femur. |
| FMTA | Femoral medial trochlea anterior | The most anterior point of the medial trochlea on the 3D femur. |
| FLTA | Femoral lateral trochlea anterior | The most anterior point of the lateral trochlea on the 3D femur. |
| FMCPP | Femoral medial condyle posterior proximal | The most proximal point of the cartilage at the posterior medial condyle on the 3D femur. Verified on a sagittal MRI view. |
| FLCPP | Femoral lateral condyle posterior proximal | The most proximal point of the cartilage at the posterior lateral condyle on the 3D femur. Verified on a sagittal MRI view. |
| Notch | Femoral notch | The most anterior point in the middle of the femoral notch on a caudal to cranial view of the 3D femur |
| FMCIP | Femoral medial condyle internal point | The most lateral point of the cartilage of the medial condyle on a caudal to cranial view of the 3D femur, at the level of one third of the notch depth anteroposteriorly. Verified on a coronal MRI view. |
| FMCEP | Femoral medial condyle external point | The most medial point of the cartilage of the medial condyle on a caudal to cranial view of the 3D femur, at the level of one third of the notch depth anteroposteriorly. Verified on a coronal MRI view. |
| FLCIP | Femoral lateral condyle internal point | The most medial point of the cartilage of the lateral condyle on a caudal to cranial view of the 3D femur, at the level of one third of the notch depth anteroposteriorly. Verified on a coronal MRI view. |
| FLCEP | Femoral lateral condyle external point | The most lateral point of the cartilage of the lateral condyle on a caudal to cranial view of the 3D femur, at the level of one third of the notch depth anteroposteriorly. Verified on a coronal MRI view. |
| TMIE | Tibial medial intercondylar eminence | The most proximal or highest point of the medial intercondylar eminence. |
| TLIE | Tibial lateral intercondylar eminence | The most proximal or highest point of the lateral intercondylar eminence. |
| TMCP | Tibial medial condyle posterior | The most posterior and lateral point of the medial compartment on the 3D tibia. Verified on a sagittal MRI view. |
| TLCP | Tibial lateral condyle posterior | The most posterior and medial point of the lateral compartment on the 3D tibia. Verified on a sagittal MRI view. |
| TMCM | Tibial medial condyle medial | The most medial point of the tibial plateau on the 3D tibia, axially aligned following the posterior condylar line of the corresponding femur. |
| TLCL | Tibial lateral condyle lateral | The most lateral point of the tibial plateau on the 3D tibia, axially aligned following the posterior condylar line of the corresponding femur. |
| TMCA | Tibial medial condyle anterior | The most anterior point on the cartilage of the medial tibial plateau (on a sagittal MRI view) |
| TLCA | Tibial lateral condyle anterior | The most anterior point on the cartilage of the lateral tibial plateau (on a sagittal MRI view) |
| Measurement Abbreviation | Measurement Definition | Between Landmarks | Measurement Projection Axis |
|---|---|---|---|
| AP MFC | Anteroposterior size of the medial femoral condyle | FMCP, FMTA | y (AP) |
| AP LFC | Anteroposterior size of the lateral femoral condyle | FLCP, FLTA | y (AP) |
| AP notch | Anteroposterior size of the femoral notch | FMCP, Notch (FLCP, Notch) | y (AP) |
| fML | Mediolateral size of the distal femur | FME, FLE | x (ML) |
| ML MFC | Mediolateral size of the medial femoral condyle | FMCIP, FMCEP | x (ML) |
| ML LFC | Mediolateral size of the lateral femoral condyle | FLCIP, FLCEP | x (ML) |
| ML notch | Mediolateral size of the femoral notch | FMCIP, FLCIP | x (ML) |
| PCL | Posterior condylar line | FMCP, FLCP | x (ML) |
| PD MFC | Proximodistal size of the medial femoral condyle | FMCPP, FMCD | z (PD) |
| PD LFC | Proximodistal size of the lateral femoral condyle | FLCPP, FLCD | z (PD) |
| AP MTP | Anteroposterior size of the medial tibial plateau | TMCP, TMCA | y (AP) |
| AP LTP | Anteroposterior size of the lateral tibial plateau | TLCP, TLCA | y (AP) |
| tML | Mediolateral size of the tibial plateau | TMCM, TLCL | x (ML) |
| ML MTP | Mediolateral size of the medial tibial plateau | TMCM, TMIE | x (ML) |
| ML LTP | Mediolateral size of the lateral tibial plateau | TLCL, TLIE | x (ML) |
| Measurement | ICCintra | ICCinter | Measurement | ICCintra | ICCinter |
|---|---|---|---|---|---|
| AP MFC | 1 | 1 | AP MTP | 1 | 0.999 |
| AP LFC | 1 | 1 | AP LTP | 0.999 | 0.998 |
| ML MFC | 0.937 | 0.796 | ML MTP | 0.953 | 0.94 |
| ML LFC | 0.985 | 0.922 | ML LTP | 0.955 | 0.935 |
| PD MFC | 0.983 | 0.947 | tML | 0.986 | 0.968 |
| PD LFC | 0.976 | 0.958 | fML | 0.991 | 0.969 |
| AP Notch | 1 | 1 |
| Landmark Acronym | Mean (SD) Intra-Observer | Mean (SD) Inter-Observer | Mean (SD) Inter-Method | Landmark Acronym | Mean (SD) Intra-Observer | Mean (SD) Inter-Observer | Mean (SD) Inter-Method |
|---|---|---|---|---|---|---|---|
| FME | 1.43 (1.26) | 2.21 (1.59) | 2.59 (1.48) | FMCIP | 0.69 (0.35) | 1.26 (0.78) | 1.56 (0.88) |
| FLE | 1.52 (1.45) | 1.47 (1.28) | 2.31 (1.07) | FMCEP | 1.05 (1.18) | 1.74 (1.03) | 1.70 (1.22) |
| FMCP | 1.52 (0.91) | 1.40 (0.77) | 2.51 (1.23) | FLCIP | 0.54 (0.32) | 1.13 (0.84) | 1.08 (0.70) |
| FLCP | 1.59 (1.02) | 1.33 (0.95) | 2.54 (1.28) | FLCEP | 0.70 (0.50) | 2.08 (1.59) | 1.93 (1.25) |
| FMCD | 1.56 (1.33) | 1.56 (1.02) | 1.98 (1.26) | TMIE | 0.57 (0.49) | 0.62 (0.30) | 0.90 (0.53) |
| FLCD | 1.14 (0.87) | 1.85 (1.30) | 2.06 (1.54) | TLIE | 0.41 (0.25) | 0.58 (0.30) | 1.05 (0.68) |
| FMTA | 0.91 (0.65) | 1.21 (0.83) | 1.47 (0.91) | TMCP | 0.99 (0.60) | 2.13 (1.67) | 2.29 (1.33) |
| FLTA | 1.23 (0.90) | 1.44 (0.98) | 2.25 (1.20) | TLCP | 1.38 (0.94) | 2.58 (1.76) | 2.86 (1.45) |
| FMCPP | 0.85 (0.56) | 1.55 (0.96) | 2.25 (1.34) | TMCM | 1.19 (1.01) | 1.87 (1.72) | 2.75 (1.88) |
| FLCPP | 0.78 (0.49) | 1.16 (0.65) | 2.14 (0.99) | TLCL | 1.12 (0.76) | 1.23 (0.61) | 2.13 (1.18) |
| Notch | 0.69 (0.47) | 0.82 (0.46) | 1.51 (0.66) | TMCA | 1.64 (0.98) | 2.31 (1.34) | 2.84 (1.39) |
| All landmarks | 1.07 (0.92) | 1.53 (1.22) | 2.05 (1.30) | TLCA | 1.21 (0.66) | 1.63 (1.00) | 2.41 (1.15) |
| Measurement | Mean (SD) Intra-Observer | Mean (SD) Inter-Observer | Mean (SD) Inter-Method | Measurement | Mean (SD) Intra-Observer | Mean (SD) Inter-Observer | Mean (SD) Inter-Method |
|---|---|---|---|---|---|---|---|
| AP MFC | 0.21 (0.16) | 0.18 (0.17) | 0.54 (0.21) | AP MTP | 0.50 (0.33) | 1.19 (0.77) | 1.39 (0.91) |
| AP LFC | 0.28 (0.22) | 0.23 (0.22) | 0.67 (0.36) | AP LTP | 0.74 (0.64) | 1.11 (0.81) | 1.46 (0.92) |
| ML MFC | 0.33 (0.28) | 0.61 (0.42) | 0.66 (0.41) | ML MTP | 0.30 (0.27) | 0.35 (0.30) | 0.65 (0.41) |
| ML LFC | 0.24 (0.22) | 0.62 (0.43) | 0.69 (0.45) | ML LTP | 0.42 (0.40) | 0.50 (0.42) | 0.75 (0.57) |
| PD MFC | 0.29 (0.22) | 0.45 (0.45) | 0.80 (0.51) | tML | 0.43 (0.38) | 0.70 (0.47) | 0.57 (0.45) |
| PD LFC | 0.33 (0.25) | 0.43 (0.32) | 0.85 (0.51) | fML | 0.30 (0.35) | 0.63 (0.60) | 0.51 (0.28) |
| AP Notch | 0.40 (0.31) | 0.46 (0.31) | 0.69 (0.53) | All measurements | 0.36 (0.35) | 0.56 (0.55) | 0.78 (0.60) |
| Measurement | ICC | Measurement | ICC | Measurement | ICC |
|---|---|---|---|---|---|
| AP MFC | 1 | AP Notch | 1 | AP MTP | 0.999 |
| AP LFC | 1 | PD MFC | 0.961 | AP LTP | 0.999 |
| ML MFC | 0.926 | PD LFC | 0.951 | ML MTP | 0.944 |
| ML LFC | 0.966 | fML | 0.995 | ML LTP | 0.956 |
| tML | 0.993 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grammens, J.; Van Haver, A.; Lumban-Gaol, I.; Danckaers, F.; Verdonk, P.; Sijbers, J. Automated Landmark Annotation for Morphometric Analysis of Distal Femur and Proximal Tibia. J. Imaging 2024, 10, 90. https://doi.org/10.3390/jimaging10040090
Grammens J, Van Haver A, Lumban-Gaol I, Danckaers F, Verdonk P, Sijbers J. Automated Landmark Annotation for Morphometric Analysis of Distal Femur and Proximal Tibia. Journal of Imaging. 2024; 10(4):90. https://doi.org/10.3390/jimaging10040090
Chicago/Turabian StyleGrammens, Jonas, Annemieke Van Haver, Imelda Lumban-Gaol, Femke Danckaers, Peter Verdonk, and Jan Sijbers. 2024. "Automated Landmark Annotation for Morphometric Analysis of Distal Femur and Proximal Tibia" Journal of Imaging 10, no. 4: 90. https://doi.org/10.3390/jimaging10040090
APA StyleGrammens, J., Van Haver, A., Lumban-Gaol, I., Danckaers, F., Verdonk, P., & Sijbers, J. (2024). Automated Landmark Annotation for Morphometric Analysis of Distal Femur and Proximal Tibia. Journal of Imaging, 10(4), 90. https://doi.org/10.3390/jimaging10040090