
Whole-Neck Non-Contrast-Enhanced MR Angiography Using Velocity Selective Magnetization Preparation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preliminary In-Vivo Experiments
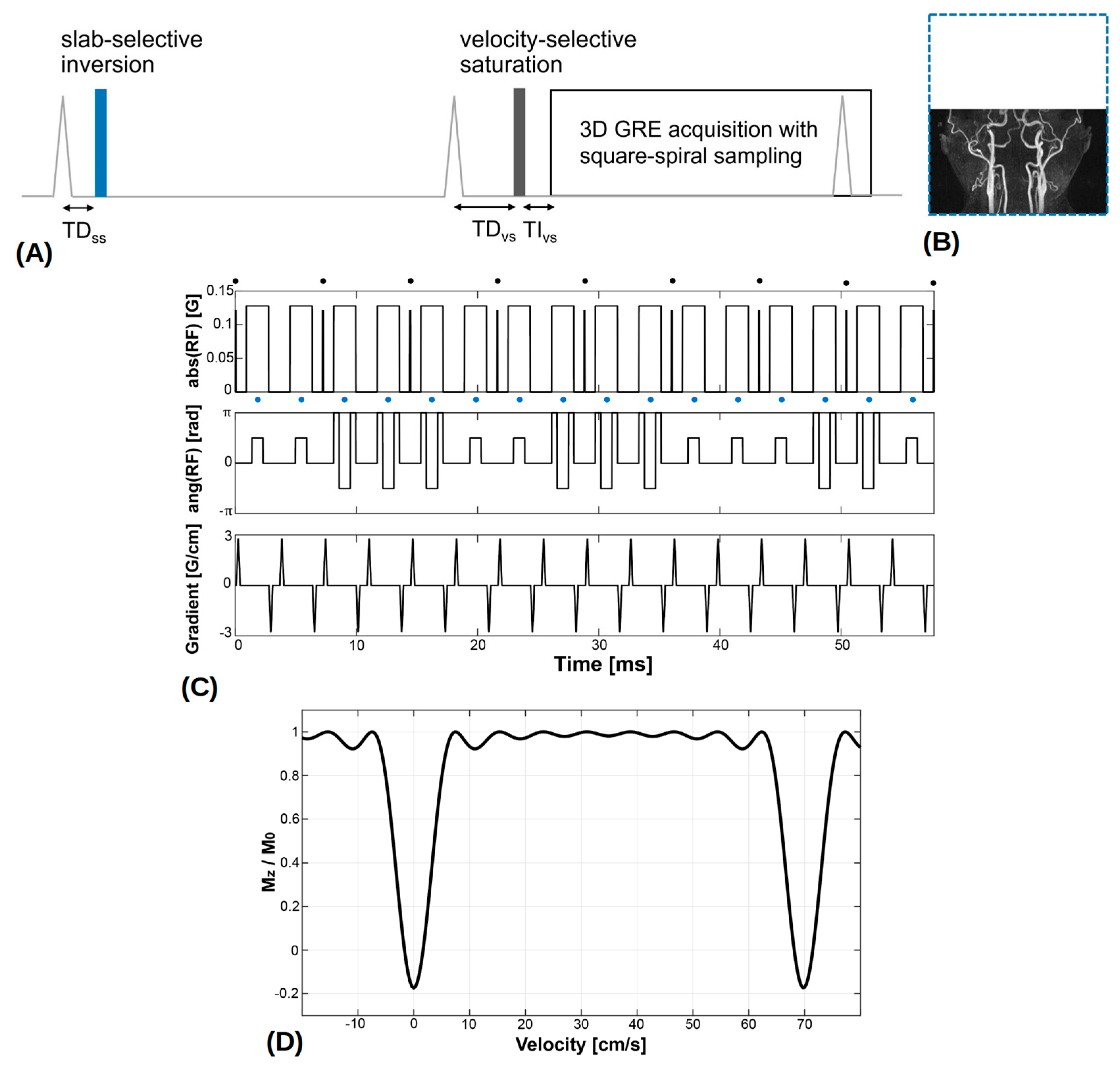
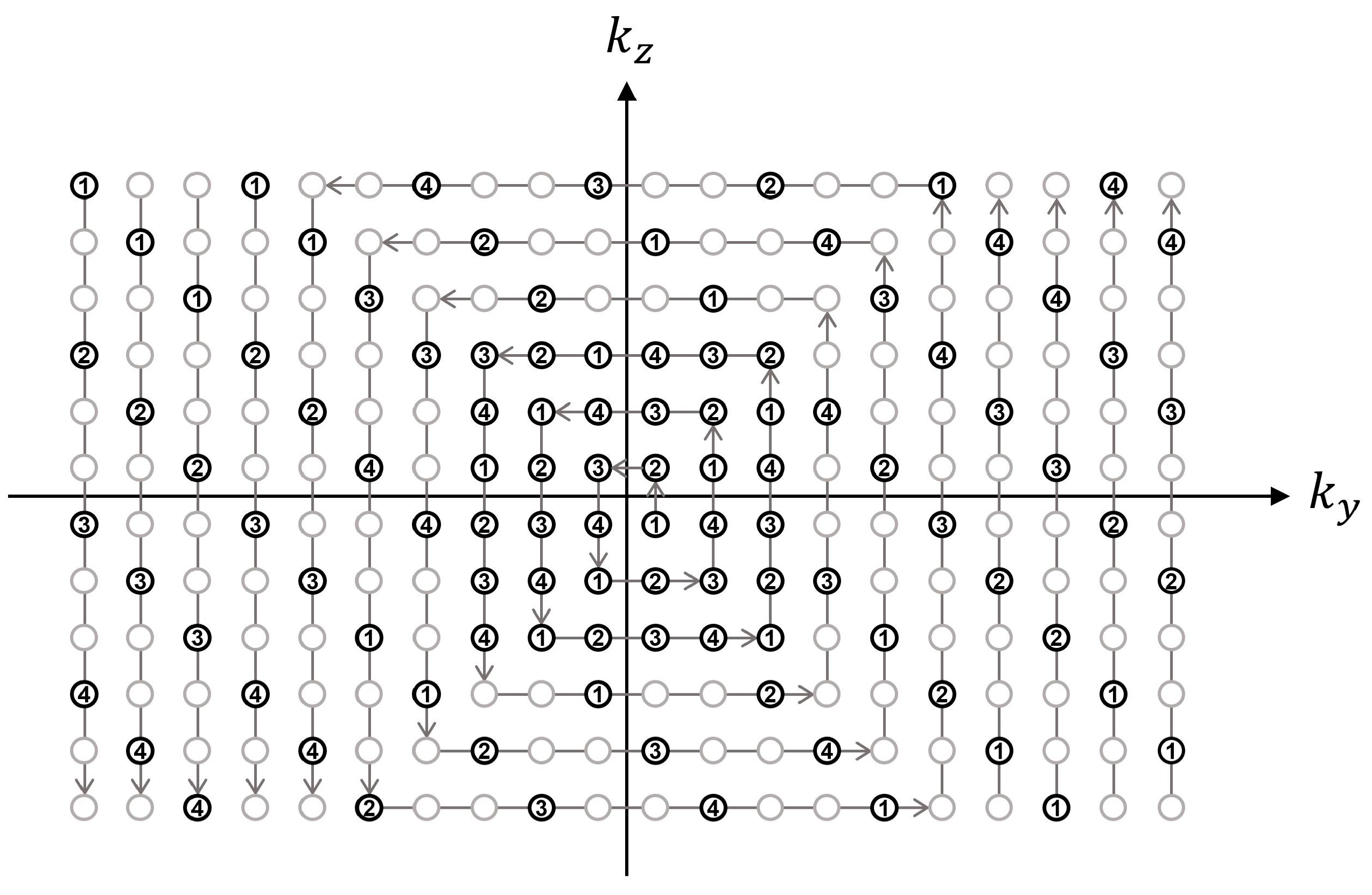
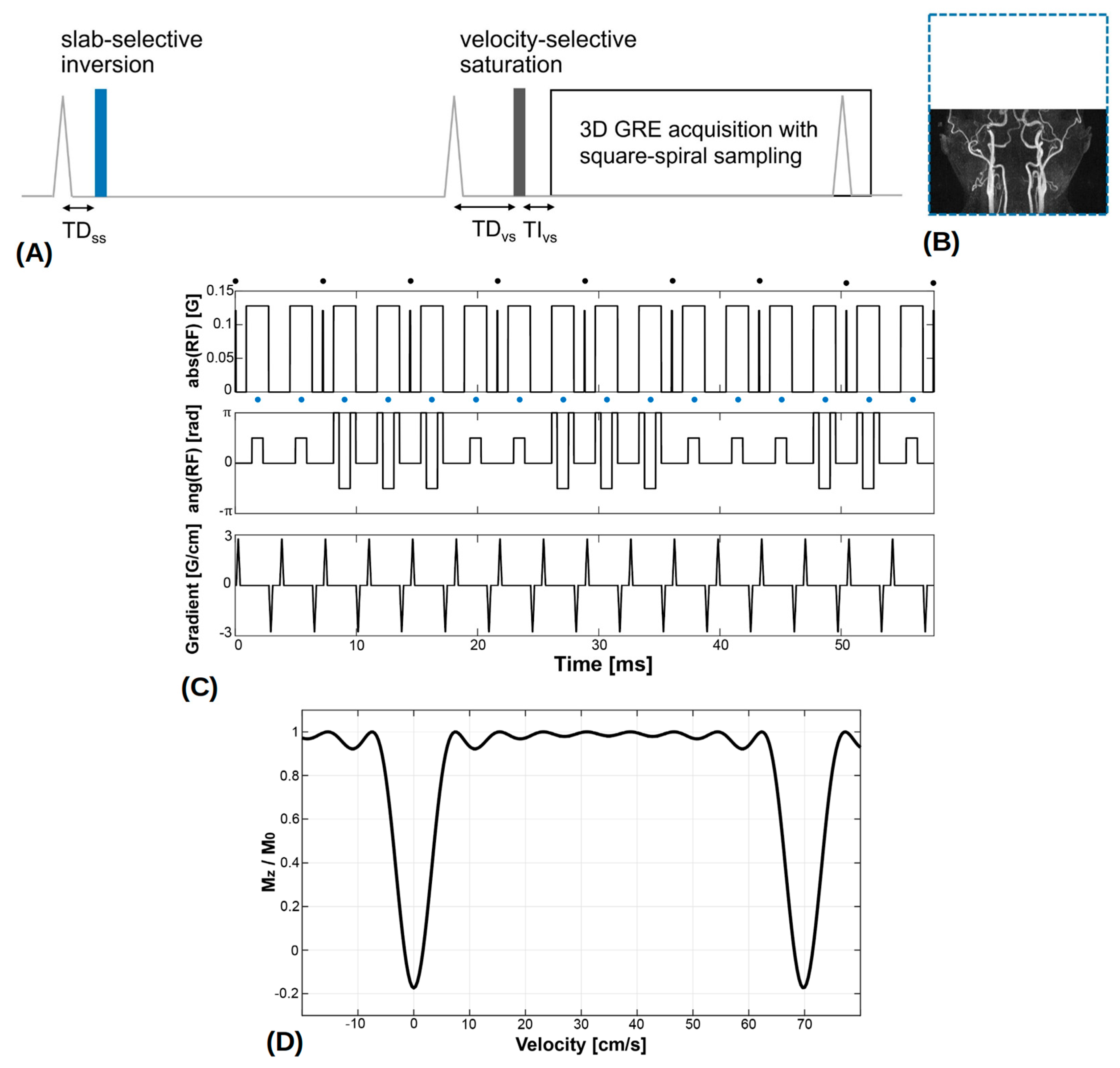
2.2. VS-MRA Pulse Sequence
2.3. MRA Experiments and Analysis
3. Results
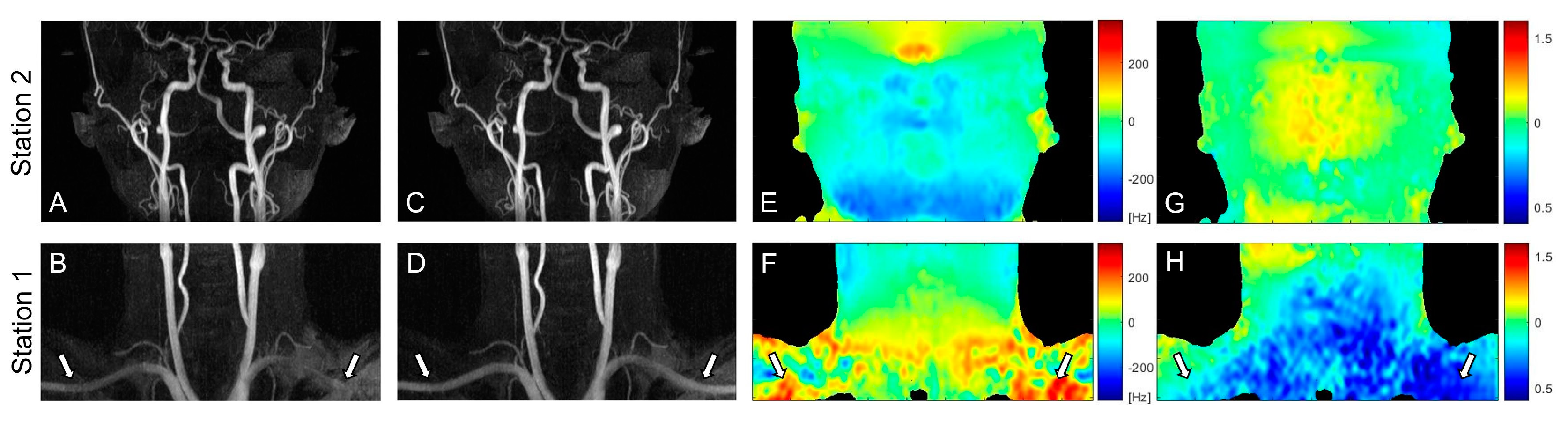
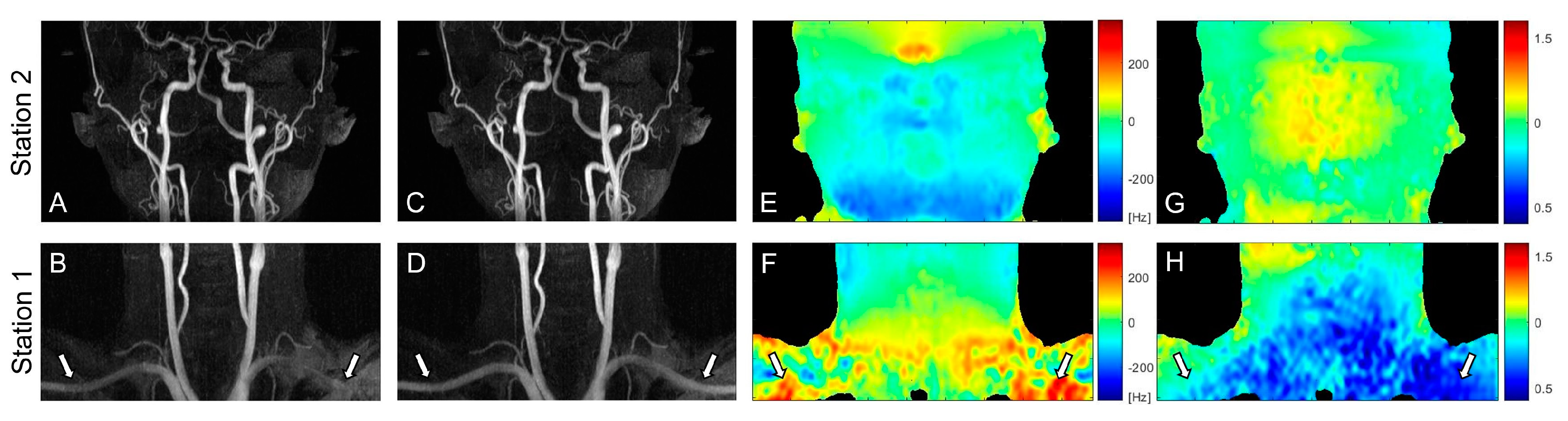
3.1. PC Flow and Field Mappings
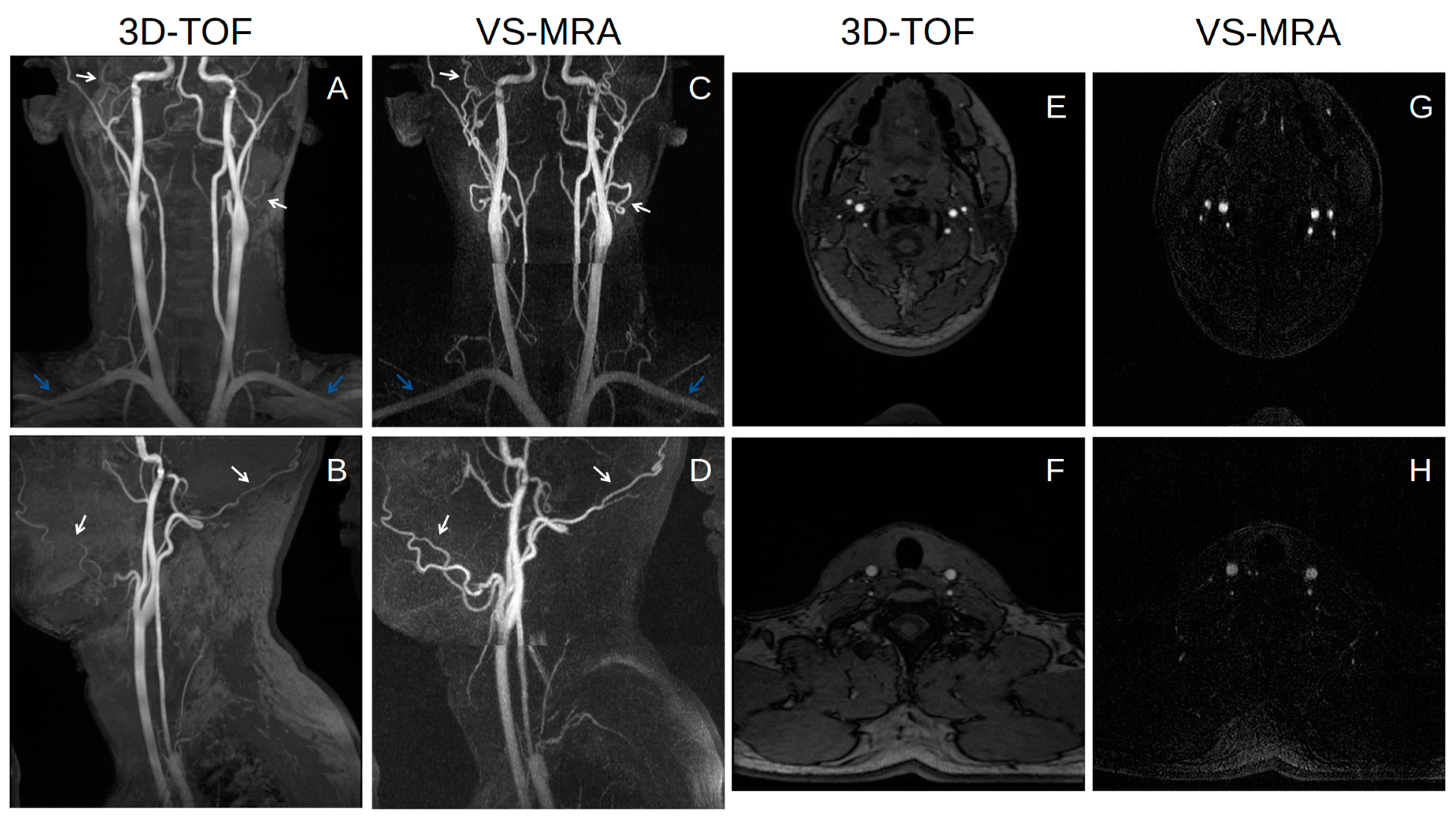
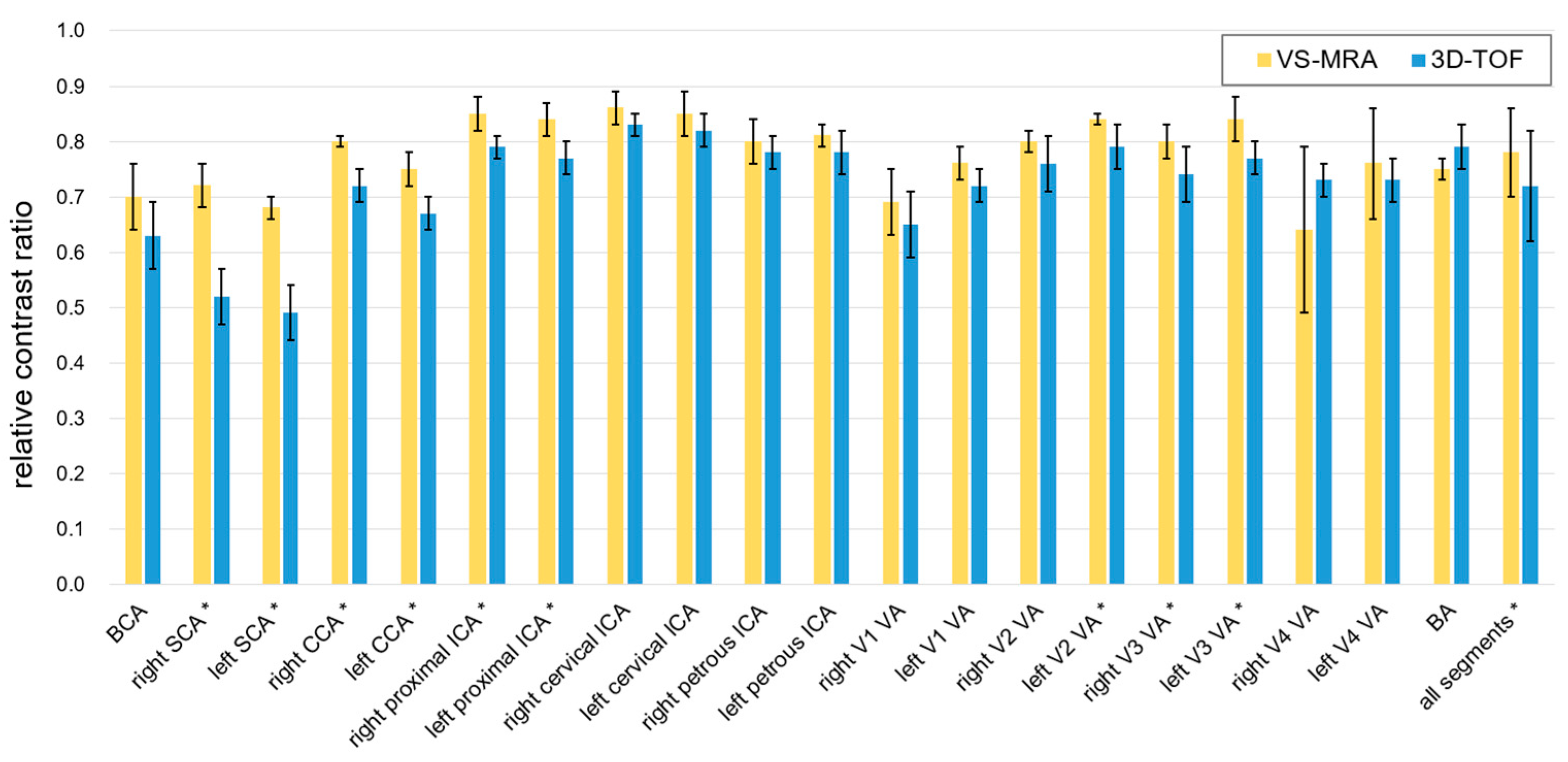
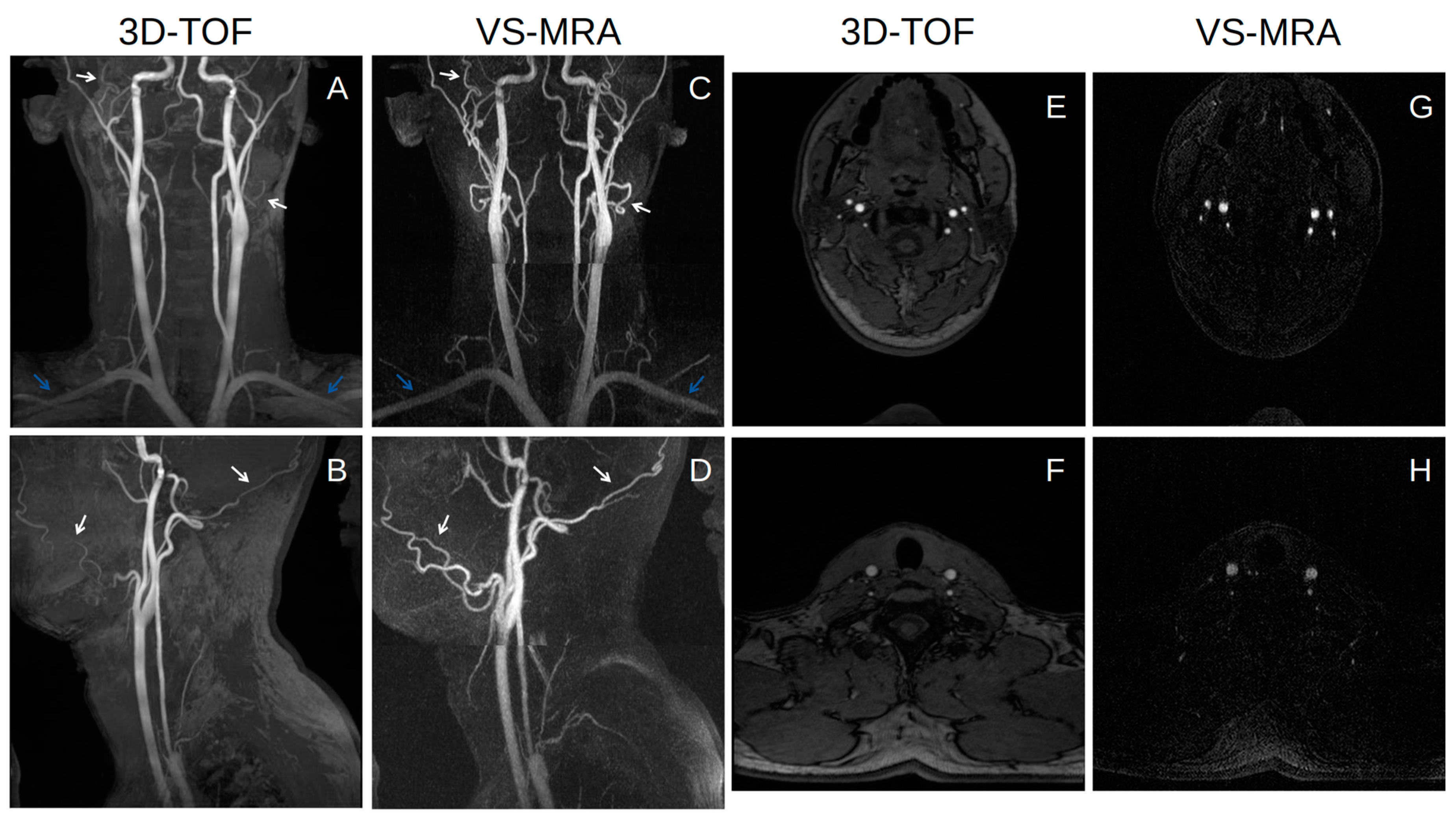
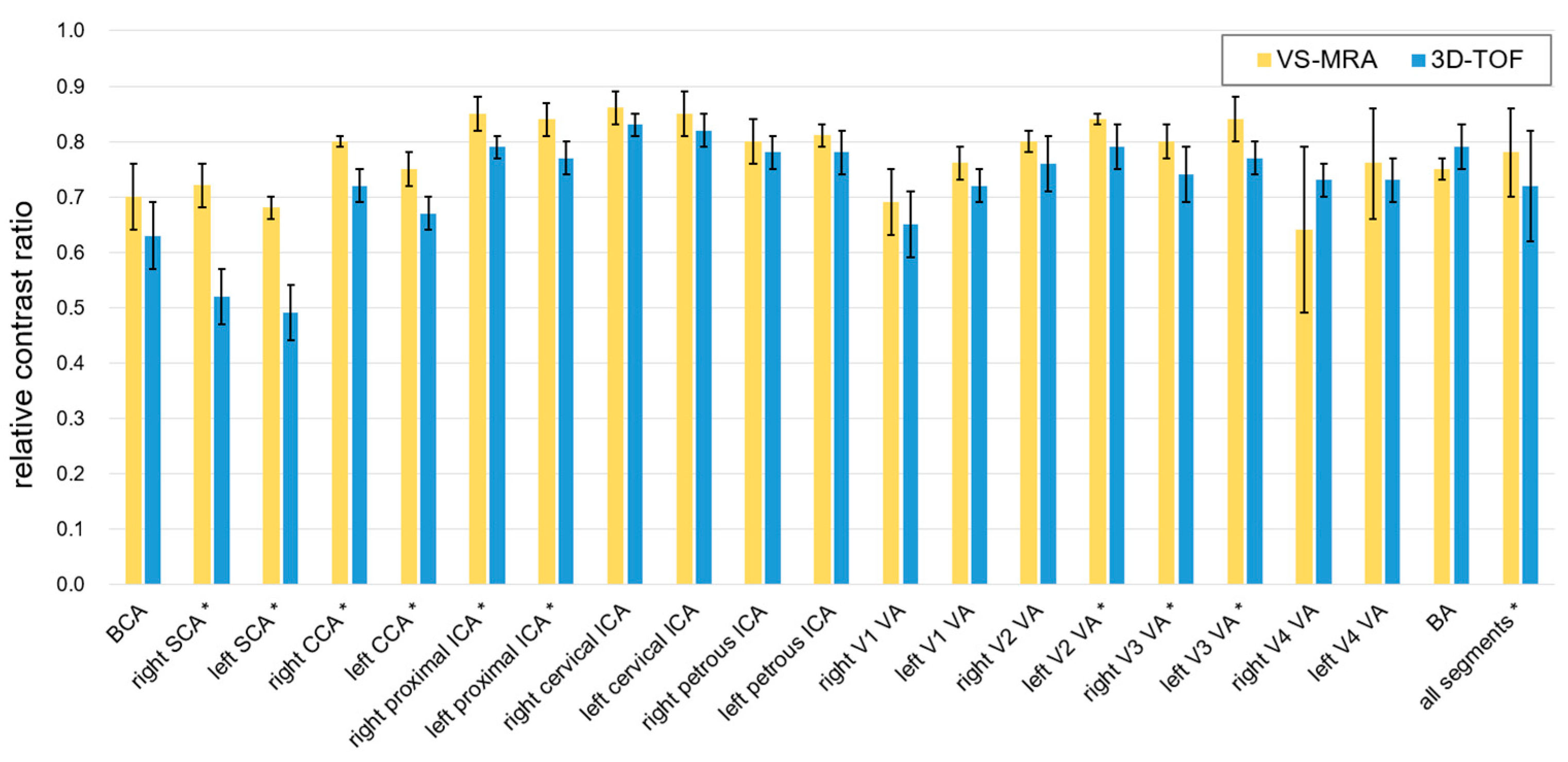
3.2. Neck MRA Experiments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuo, P.H.; Kanal, E.; Abu-Alfa, A.K.; Cowper, S.E. Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis. Radiology 2007, 242, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Lee, V.S. Nonenhanced MR angiography. Radiology 2008, 248, 20–43. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, H.S. NSF: Still relevant. J. Magn. Reson. Imaging 2014, 40, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Shin, T. Principles of Magnetic Resonance Angiography Techniques. Investig. Magn. Reason. Imaging 2021, 25, 209–217. [Google Scholar] [CrossRef]
- Masaryk, T.J.; Laub, G.A.; Modic, M.T.; Ross, J.S.; Haacke, E.M. Carotid-CNS MR flow imaging. Magn. Reson. Med. 1990, 14, 308–314. [Google Scholar] [CrossRef]
- Laub, G.A. Time-of-flight method of MR angiography. Magn. Reson. Imaging Clin. N. Am. 1995, 3, 391–398. [Google Scholar] [CrossRef]
- Hitoshi, K. Time-Spatial Labeling Inversion Tag (t-SLIT) using a Selective IR-Tag On/Off Pulse in 2D and 3D half-Fourier FSE as Arterial Spin Labeling. ISMRM 2002, 10, 145. [Google Scholar]
- Katoh, M.; Buecker, A.; Stuber, M.; Günther, R.W.; Spuentrup, E. Free-breathing renal MR angiography with steady-state free-precession (SSFP) and slab-selective spin inversion: Initial results. Kidney Int. 2004, 66, 1272–1278. [Google Scholar] [CrossRef] [Green Version]
- Edelman, R.R.; Sheehan, J.J.; Dunkle, E.; Schindler, N.; Carr, J.; Koktzoglou, I. Quiescent-interval single-shot unenhanced magnetic resonance angiography of peripheral vascular disease: Technical considerations and clinical feasibility. Magn. Reson. Med. 2010, 63, 951–958. [Google Scholar] [CrossRef] [Green Version]
- Ward, E.V.; Galizia, M.S.; Usman, A.; Popescu, A.R.; Dunkle, E.; Edelman, R.R. Comparison of quiescent inflow single-shot and native space for nonenhanced peripheral MR angiography. J. Magn. Reson. Imaging 2013, 38, 1531–1538. [Google Scholar] [CrossRef] [Green Version]
- Shin, T.; Worters, P.W.; Hu, B.S.; Nishimura, D.G. Non-contrast-enhanced renal and abdominal MR angiography using velocity-selective inversion preparation. Magn. Reson. Med. 2013, 69, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.; Hu, B.S.; Nishimura, D.G. Off-resonance-robust velocity-selective magnetization preparation for non-contrast-enhanced peripheral MR angiography. Magn. Reson. Med. 2013, 70, 1229–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, Q.; Shin, T.; Schär, M.; Guo, H.; Chen, H.; Qiao, Y. Velocity-selective magnetization-prepared non-contrast-enhanced cerebral MR angiography at 3 Tesla: Improved immunity to B0/B1 inhomogeneity. Magn. Reson. Med. 2016, 75, 1232–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, T.; Qin, Q.; Park, J.Y.; Crawford, R.S.; Rajagopalan, S. Identification and reduction of image artifacts in non–contrast-enhanced velocity-selective peripheral angiography at 3T. Magn. Reson. Med. 2016, 76, 466–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Xu, F.; Schär, M.; Liu, J.; Shin, T.; Zhao, Y.; van Zijl, P.C.; Wasserman, B.A.; Qiao, Y.; Qin, Q. Whole-brain arteriography and venography: Using improved velocity-selective saturation pulse trains. Magn. Reson. Med. 2018, 79, 2014–2023. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.; Qin, Q. Characterization and suppression of stripe artifact in velocity-selective magnetization-prepared unenhanced MR angiography. Magn. Reson. Med. 2018, 80, 1997–2005. [Google Scholar] [CrossRef]
- Shin, T.; Menon, R.G.; Thomas, R.B.; Cavallo, A.U.; Sarkar, R.; Crawford, R.S.; Rajagopalan, S. Unenhanced velocity-selective MR angiography (VS-MRA): Initial clinical evaluation in patients with peripheral artery disease. J. Magn. Reson. Imaging 2019, 49, 744–751. [Google Scholar] [CrossRef]
- Watson, J.D.B.; Grasu, B.; Menon, R.; Pensy, R.; Crawford, R.S.; Shin, T. Novel, non-gadolinium-enhanced magnetic resonance imaging technique of pedal artery aneurysms. J. Vasc. Surg. Cases Innov. Tech. 2017, 3, 87–89. [Google Scholar] [CrossRef] [Green Version]
- Zhu, D.; Li, W.; Liu, D.; Liu, G.; Pei, Y.; Shin, T.; Sedaghat, F.; Qin, Q. Non-contrast-enhanced abdominal MRA at 3 T using velocity-selective pulse trains. Magn. Reson. Med. 2020, 84, 1173–1183. [Google Scholar] [CrossRef]
- Sacolick, L.I.; Wiesinger, F.; Hancu, I.; Vogel, M.W. B1 mapping by Bloch-Siegert shift. Magn. Reson. Med. 2010, 63, 1315–1322. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, M.A.; King, K.F.; Zhou, X.J. Handbook of MRI Pulse Sequences, 1st ed.; Elsevier Academic Press: Burlington, MA, USA, 2004; pp. 177–212. [Google Scholar] [CrossRef]
- Lustig, M.; Pauly, J.M. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn. Reson. Med. 2010, 64, 457–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atanasova, I.P.; Kim, D.; Lim, R.P.; Storey, P.; Kim, S.; Guo, H.; Lee, V.S. Noncontrast MR angiography for comprehensive assessment of abdominopelvic arteries using quadruple inversion-recovery preconditioning and 3D balanced steady-state free precession imaging. J. Magn. Reson. Imaging 2011, 33, 1430–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellman, P.; McVeigh, E.R. Image reconstruction in SNR units: A general method for SNR measurement. Magn. Reson. Med. 2005, 54, 1439–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, O.; Raya, J.G.; Reeder, S.B.; Reiser, M.F.; Schoenberg, S.O. Measurement of signal-to-noise ratios in MR images: Influence of multichannel coils, parallel imaging, and reconstruction filters. J. Magn. Reson. Imaging 2007, 26, 375–385. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Rahman Siddiquee, M.M.; Tajbakhsh, N.; Liang, J. Unet++: A nested u-net architecture for medical image segmentation. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Jiang, Z.; Dong, J.; Hou, Y.; Liu, B. Attention gate resU-Net for automatic MRI brain tumor segmentation. IEEE Access 2020, 8, 58533–58545. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.J.; Choi, S.H.; Park, J.; Shin, T. Whole-Neck Non-Contrast-Enhanced MR Angiography Using Velocity Selective Magnetization Preparation. Tomography 2023, 9, 60-69. https://doi.org/10.3390/tomography9010006
Park CJ, Choi SH, Park J, Shin T. Whole-Neck Non-Contrast-Enhanced MR Angiography Using Velocity Selective Magnetization Preparation. Tomography. 2023; 9(1):60-69. https://doi.org/10.3390/tomography9010006
Chicago/Turabian StylePark, Chan Joo, Seung Hong Choi, Jaeseok Park, and Taehoon Shin. 2023. "Whole-Neck Non-Contrast-Enhanced MR Angiography Using Velocity Selective Magnetization Preparation" Tomography 9, no. 1: 60-69. https://doi.org/10.3390/tomography9010006
APA StylePark, C. J., Choi, S. H., Park, J., & Shin, T. (2023). Whole-Neck Non-Contrast-Enhanced MR Angiography Using Velocity Selective Magnetization Preparation. Tomography, 9(1), 60-69. https://doi.org/10.3390/tomography9010006