
SPECT/CT Radiomics for Differentiating between Enchondroma and Grade I Chondrosarcoma




Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Image Acquisition
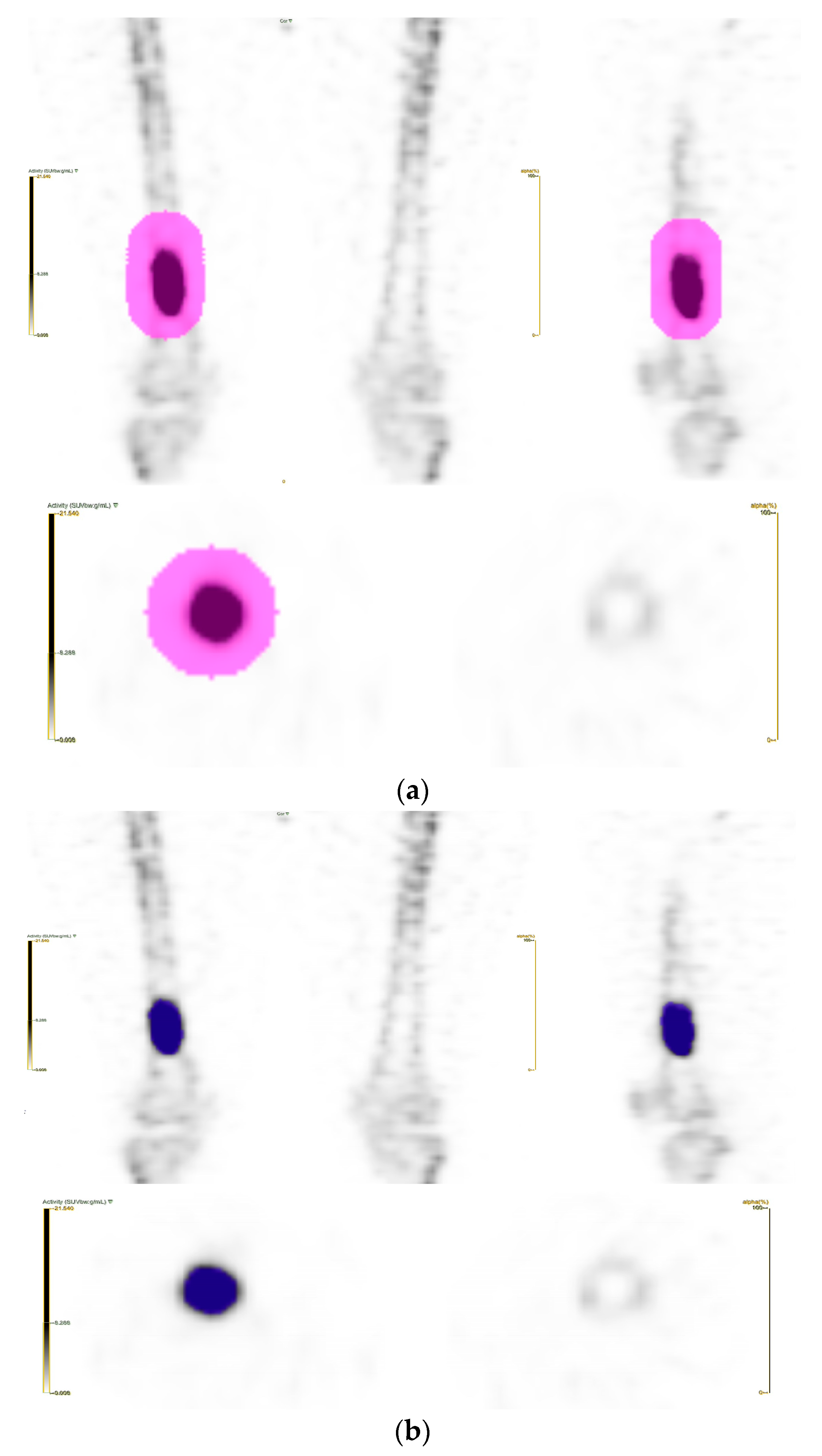
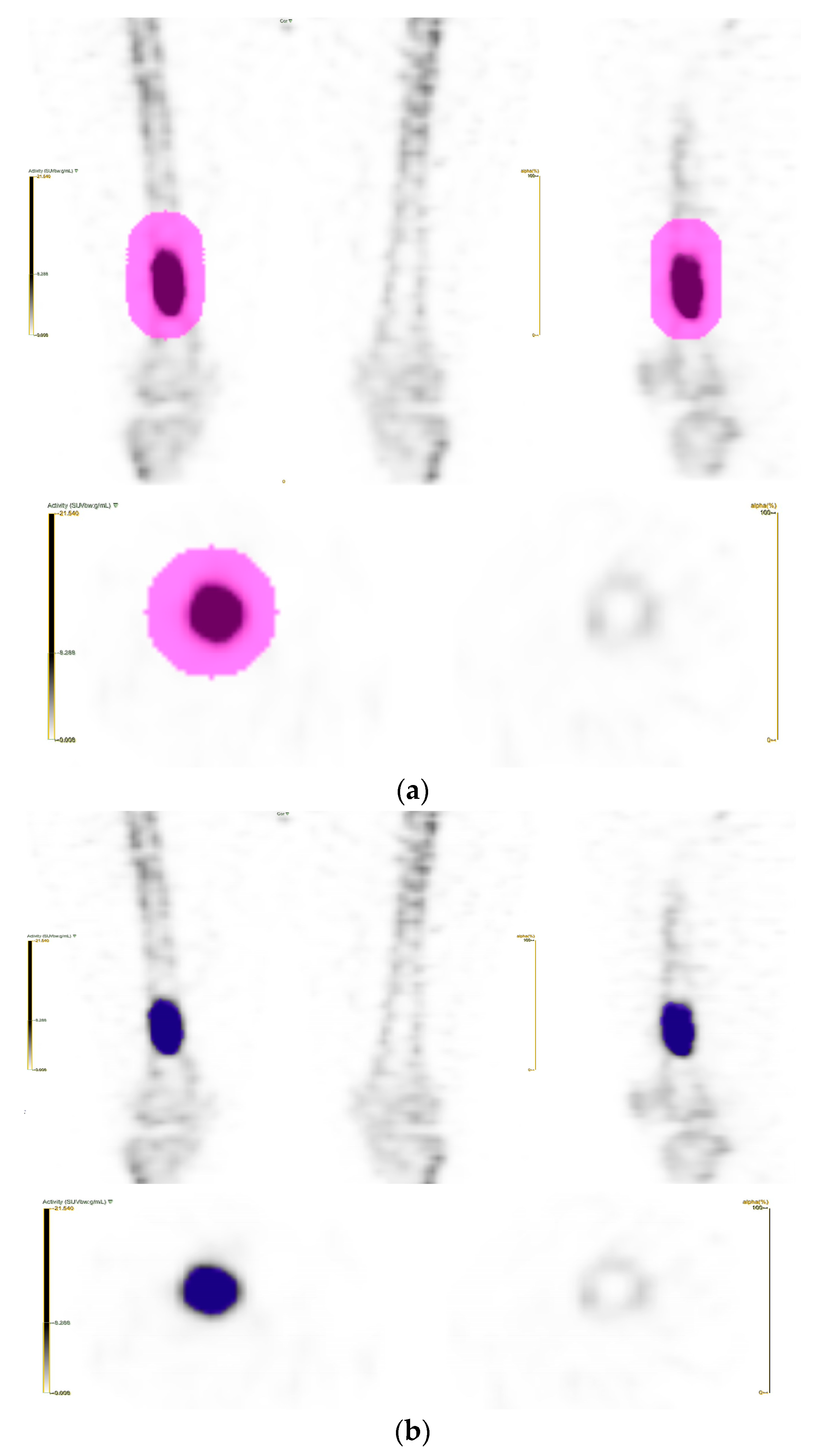
2.3. Segmentation and Feature Extraction
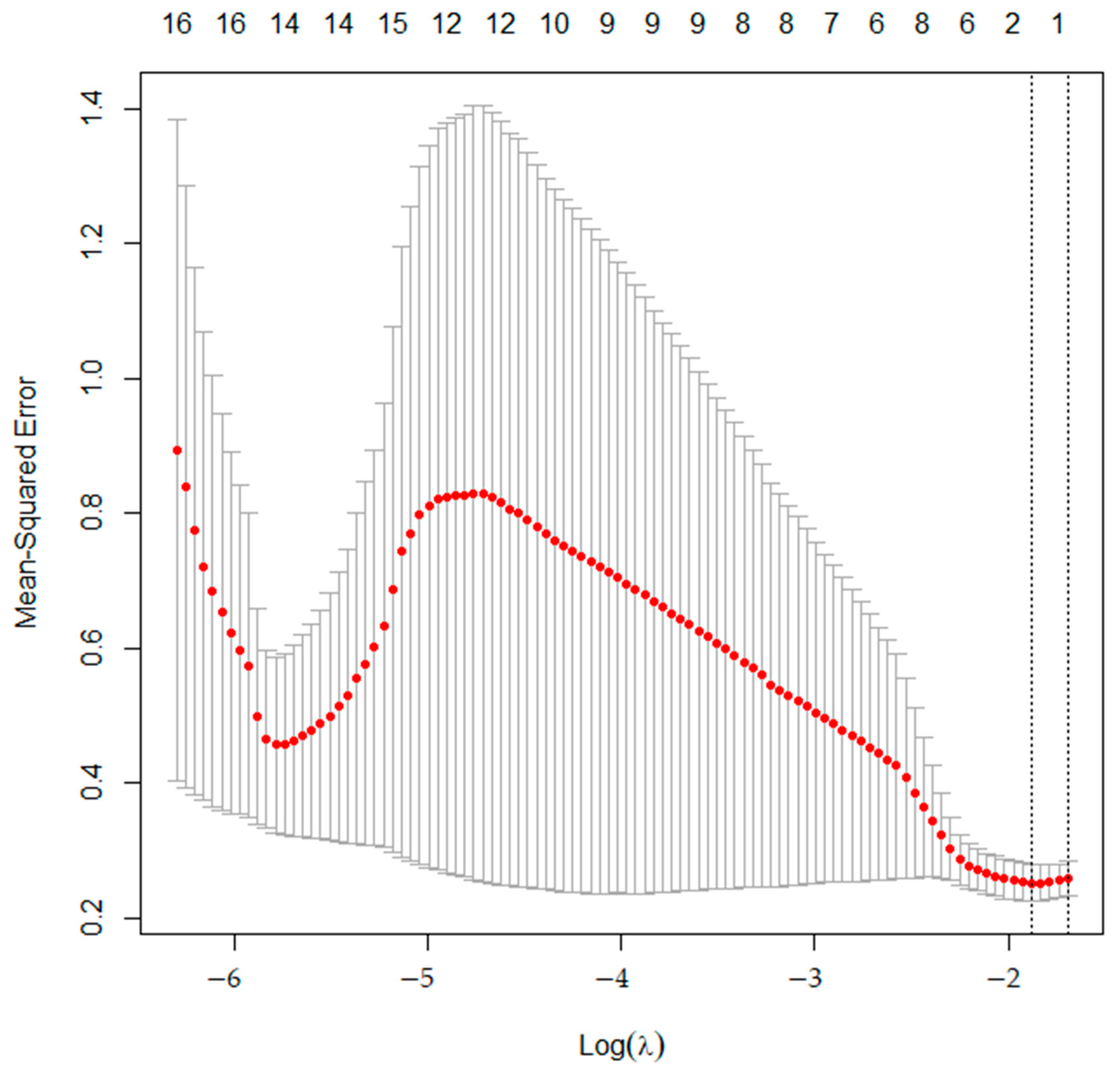
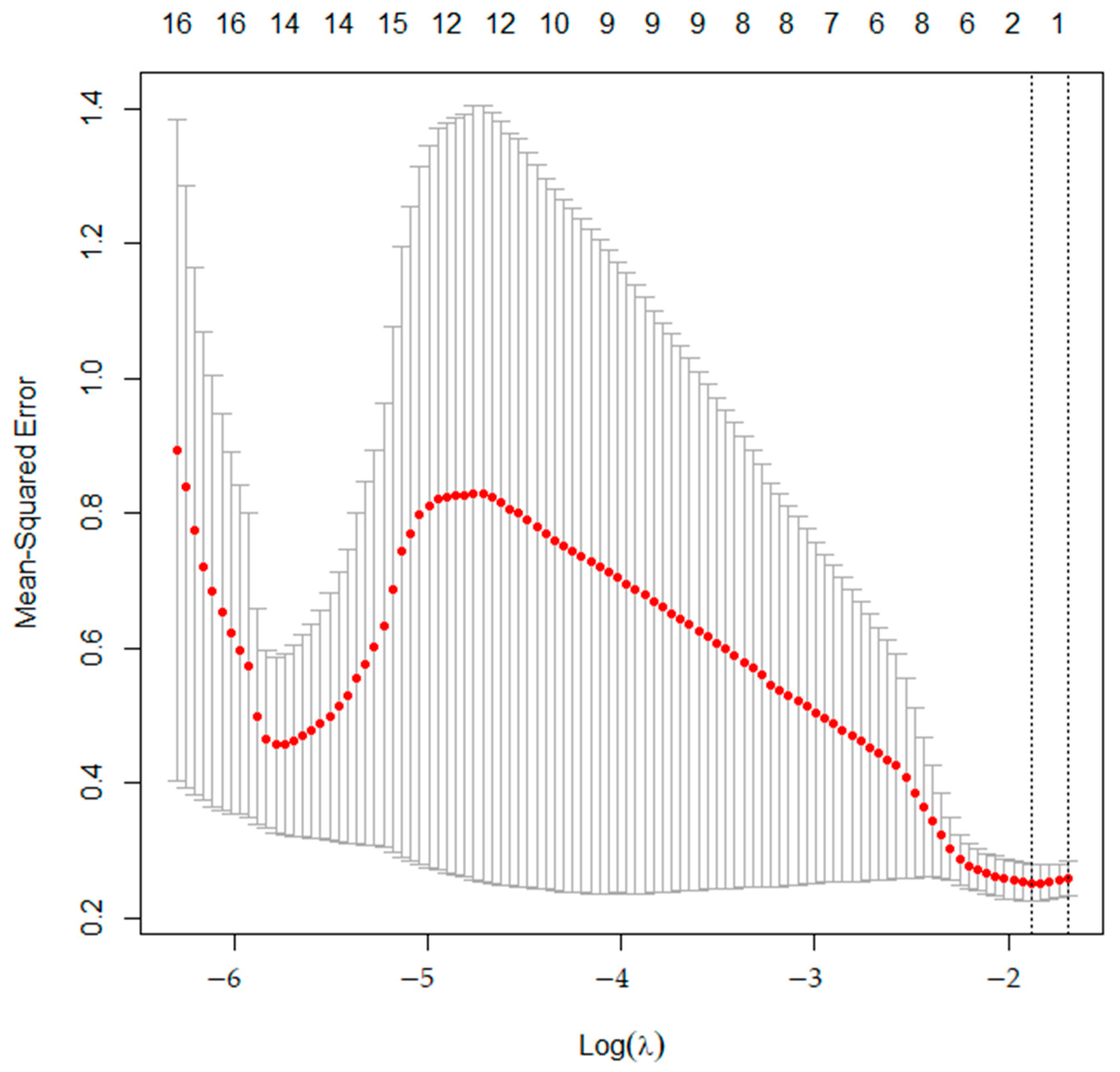
2.4. Feature Selection and Statistical Analysis
3. Results
3.1. Demographics
3.2. Statistical Analysis
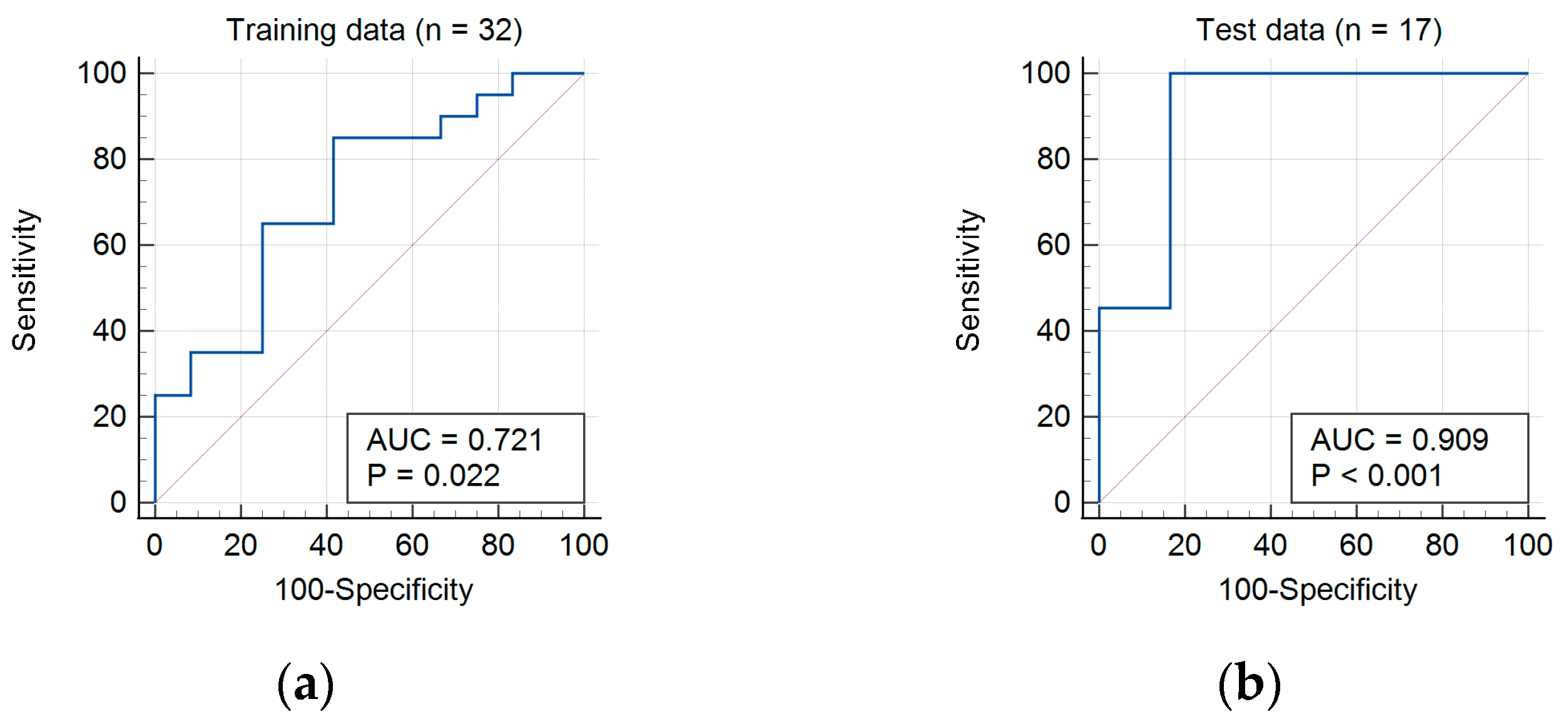
3.2.1. Training Data
3.2.2. Test Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. WHO Classification of Tumours: Soft Tissue and Bone Tumours; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Qasem, S.A.; DeYoung, B.R. Cartilage-forming tumors. Semin. Diagn. Pathol. 2014, 31, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Skeletal Lesions Interobserver Correlation among Expert Diagnosticians (SLICED) Study Group. Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J. Bone Jt. Surg. Am. 2007, 89, 2113–2123. [Google Scholar] [CrossRef]
- Hudson, T.M.; Chew, F.S.; Manaster, B.J. Radionuclide bone scanning of medullary chondrosarcoma. AJR Am. J. Roentgenol. 1982, 139, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.L.; Willowson, K.P. Quantitative SPECT/CT: SPECT joins PET as a quantitative imaging modality. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.H.; Han, E.J.; Chang, K.B.; Joo, M.W. Quantitative SPECT/CT for differentiating between enchondroma and grade I chondrosarcoma. Sci. Rep. 2020, 10, 10587. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Choi, H.; Paeng, J.C.; Cheon, G.J. Radiomics in Oncological PET/CT: A Methodological Overview. Nucl. Med. Mol. Imaging 2019, 53, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Chicklore, S.; Goh, V.; Siddique, M.; Roy, A.; Marsden, P.K.; Cook, G.J.R. Quantifying tumour heterogeneity in 18F-FDG PET/CT imaging by texture analysis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhang, K.; Le, H.; Jiang, Y.; Li, W.; Geng, Y.; Li, S.; Hong, G. Radiomics Nomograms Based on Non-enhanced MRI and Clinical Risk Factors for the Differentiation of Chondrosarcoma from Enchondroma. J. Magn. Reson. Imaging 2021, 54, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Erdem, F.; Tamsel, İ.; Demirpolat, G. The use of radiomics and machine learning for the differentiation of chondrosarcoma from enchondroma. J. Clin. Ultrasound 2023, 51, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Emmert-Streib, F.; Dehmer, M. High-Dimensional LASSO-Based Computational Regression Models: Regularization, Shrinkage, and Selection. Mach. Learn. Knowl. Extr. 2019, 1, 359–383. [Google Scholar] [CrossRef]
- Eefting, D.; Schrage, Y.M.; Geirnaerdt, M.J.A.; Le Cessie, S.; Taminiau, A.H.M.; Bovée, J.V.M.G.; Hogendoorn, P.C.W. Assessment of Interobserver Variability and Histologic Parameters to Improve Reliability in Classification and Grading of Central Cartilaginous Tumors. Am. J. Surg. Pathol. 2009, 33, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Murphey, M.D.; Flemming, D.J.; Boyea, S.R.; Bojescul, J.A.; Sweet, D.E.; Temple, H.T. Enchondroma versus chondrosarcoma in the appendicular skeleton: Differentiating features. RadioGraphics 1998, 18, 1213–1237. [Google Scholar] [CrossRef]
- Feliciani, G.; Fioroni, F.; Grassi, E.; Bertolini, M.; Rosca, A.; Timon, G.; Galaverni, M.; Iotti, C.; Versari, A.; Iori, M.; et al. Radiomic Profiling of Head and Neck Cancer: 18F-FDG PET Texture Analysis as Predictor of Patient Survival. Contrast Media Mol. Imaging 2018, 2018, 3574310. [Google Scholar] [CrossRef] [PubMed]
- Waterton, J.C.; Pylkkanen, L. Qualification of imaging biomarkers for oncology drug development. Eur. J. Cancer 2012, 48, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Trunk, G.V. A Problem of Dimensionality: A Simple Example. IEEE Trans. Pattern Anal. Mach. Intell. 1979, PAMI-1, 306–307. [Google Scholar] [CrossRef] [PubMed]
- Bach, F.R. Bolasso: Model consistent lasso estimation through the bootstrap. In Proceedings of the 25th International Conference on Machine Learning, Helsinki, Finland, 5–9 July 2008. [Google Scholar]
- Tixier, F.; Le Rest, C.C.; Hatt, M.; Albarghach, N.; Pradier, O.; Metges, J.-P.; Corcos, L.; Visvikis, D. Intratumor heterogeneity characterized by textural features on baseline 18F-FDG PET images predicts response to concomitant radiochemotherapy in esophageal cancer. J. Nucl. Med. 2011, 52, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Cilengir, A.H.; Evrimler, S.; Serel, T.A.; Uluc, E.; Tosun, O. The diagnostic value of magnetic resonance imaging-based texture analysis in differentiating enchondroma and chondrosarcoma. Skelet. Radiol. 2023, 52, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Training Data | Test Data | |
|---|---|---|
| Patients (n) | 32 | 17 |
| Median age (range), years | 54 (31–45) | 49 (19–70) |
| Sex | ||
| Male | 9 (28.1%) | 6 (35.3%) |
| Female | 23 (71.9%) | 11 (64.7%) |
| Diagnosis | ||
| Enchondroma | 20 (62.5%) | 11 (64.8%) |
| Grade 1 chondrosarcoma | 12 (37.5%) | 6 (35.2%) |
| Skeletal distribution | ||
| Femur | 16 | 6 |
| Humerus | 13 | 9 |
| Tibia | 2 | |
| Fibula | 1 | 2 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Coefficient | p | Coefficient | p | |
| SUVmean | −0.35 | 0.052 | ||
| SUVmax | −0.36 | 0.043 | ||
| Volume | −0.29 | 0.107 | ||
| CoarsenessNGLDM | 0.29 | 0.112 | ||
| ZLNUGLZLM | −0.38 | 0.032 | −0.38 | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.; Choi, W.H.; Joo, M.W.; Ha, S.; Chung, Y.-A. SPECT/CT Radiomics for Differentiating between Enchondroma and Grade I Chondrosarcoma. Tomography 2023, 9, 1868-1875. https://doi.org/10.3390/tomography9050148
Yoon H, Choi WH, Joo MW, Ha S, Chung Y-A. SPECT/CT Radiomics for Differentiating between Enchondroma and Grade I Chondrosarcoma. Tomography. 2023; 9(5):1868-1875. https://doi.org/10.3390/tomography9050148
Chicago/Turabian StyleYoon, Hyukjin, Woo Hee Choi, Min Wook Joo, Seunggyun Ha, and Yong-An Chung. 2023. "SPECT/CT Radiomics for Differentiating between Enchondroma and Grade I Chondrosarcoma" Tomography 9, no. 5: 1868-1875. https://doi.org/10.3390/tomography9050148
APA StyleYoon, H., Choi, W. H., Joo, M. W., Ha, S., & Chung, Y.-A. (2023). SPECT/CT Radiomics for Differentiating between Enchondroma and Grade I Chondrosarcoma. Tomography, 9(5), 1868-1875. https://doi.org/10.3390/tomography9050148