
Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
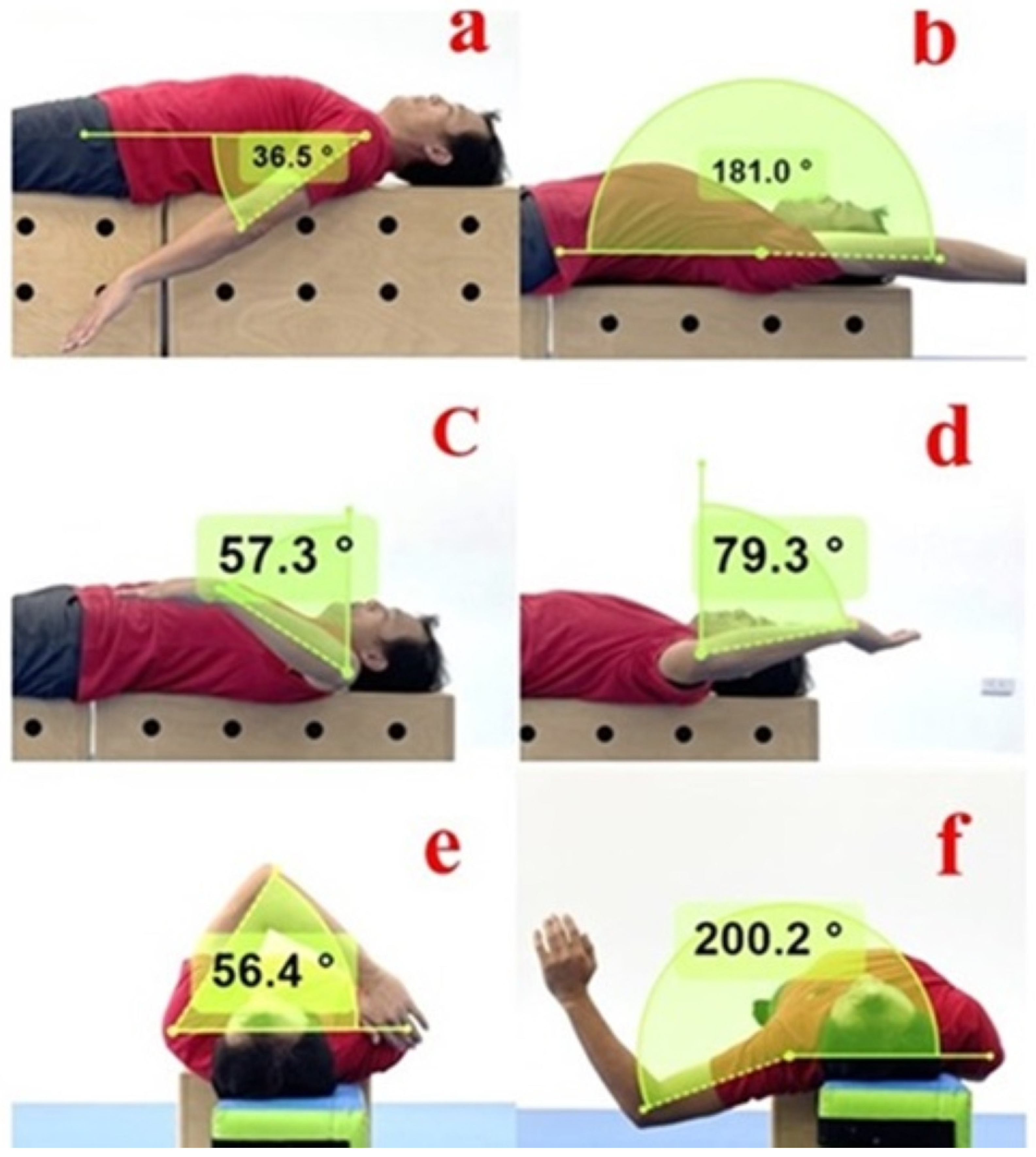
2.2. Procedure
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Escamilla, R.; Fleisig, G.; Barrentine, S.; Andrews, J.; Moorman, C., 3rd. Kinematic and kinetic comparisons between American and Korean professional baseball pitchers. Sports Biomech. 2022, 1, 213–228. [Google Scholar] [CrossRef]
- Forthomme, B.; Croisier, J.L.; Ciccarone, G.; Crielaard, J.M.; Cloes, M. Factors correlated with volleyball spike velocity. Am. J. Sports Med. 2005, 33, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Stickley, C.D.; Hetzler, R.K.; Freemyer, B.G.; Kimura, I.F. Isokinetic peak torque ratios and shoulder injury history in adolescent female volleyball athletes. J. Athl. Train. 2008, 43, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Obana, K.K.; Singh, P.; Namiri, N.K.; Levine, W.N.; Parsons, B.O.; Trofa, D.P.; Parisien, R.L. The Finger, wrist, and shoulder are the most commonly injured areas in youth volleyball players but the incidence of injuries decreased overall between 2012 and 2022. Arthrosc. Sports Med. Rehabil. 2024, 6, 100862. [Google Scholar] [CrossRef]
- Kilic, O.; Maas, M.; Verhagen, E.; Zwerver, J.; Gouttebarge, V. Incidence, aetiology and prevention of musculoskeletal injuries in volleyball: A systematic review of the literature. Eur. J. Sport Sci. 2017, 17, 765–793. [Google Scholar] [CrossRef] [PubMed]
- Delgado, J.; Jaramillo, D.; Chauvin, N.A. Imaging the injured pediatric athlete: Upper extremity. Radiographics 2016, 36, 1672–1687. [Google Scholar] [CrossRef] [PubMed]
- Laor, T.; Jaramillo, D. MR imaging insights into skeletal maturation: What is normal? Radiology 2009, 250, 28–38. [Google Scholar] [CrossRef]
- Cools, A.M.; Palmans, T.; Johansson, F.R. Age-related, sport-specific adaptions of the shoulder girdle in elite adolescent tennis players. J. Athl. Train. 2014, 49, 647–653. [Google Scholar] [CrossRef]
- Lu, Y.; Chen, P.; Chou, W.Y.; Yang, C.P.; Sheu, H.; Tang, H.C.; Weng, C.J.; Chiu, J.C. Relationship between shoulder and elbow range of motion and ultrasonographic structural abnormalities in the elbow of Taiwanese high school baseball players. BMC Sports Sci. Med. Rehabil. 2024, 16, 44. [Google Scholar] [CrossRef]
- Frisch, K.E.; Clark, J.; Hanson, C.; Fagerness, C.; Conway, A.; Hoogendoorn, L. High prevalence of nontraumatic shoulder pain in a regional sample of female high school volleyball athletes. Orthop. J. Sports Med. 2017, 5, 2325967117712236. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. The disabled throwing shoulder: Spectrum of pathology Part I: Pathoanatomy and biomechanics. Arthroscopy 2003, 19, 404–420. [Google Scholar] [CrossRef] [PubMed]
- Manske, R.; Wilk, K.E.; Davies, G.; Ellenbecker, T.; Reinold, M. Glenohumeral motion deficits: Friend or foe? Int. J. Sports Phys. Ther. 2013, 8, 537–553. [Google Scholar] [PubMed]
- Borsa, P.A.; Laudner, K.G.; Sauers, E.L. Mobility and stability adaptations in the shoulder of the overhead athlete: A theoretical and evidence-based perspective. Sports Med. 2008, 38, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Reagan, K.M.; Meister, K.; Horodyski, M.B.; Werner, D.W.; Carruthers, C.; Wilk, K. Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players. Am. J. Sports Med. 2002, 30, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Mizoguchi, Y.; Akasaka, K.; Otsudo, T.; Hall, T. Physical function characteristics in Japanese high school volleyball players with low back pain: A case-controlled study. Medicine 2020, 99, e23178. [Google Scholar] [CrossRef]
- Baltaci, G.; Johnson, R.; Kohl, H., 3rd. Shoulder range of motion characteristics in collegiate baseball players. J. Sports Med. Phys. Fitness 2001, 41, 236–242. [Google Scholar]
- Downar, J.M.; Sauers, E.L. Clinical measures of shoulder mobility in the professional baseball player. J. Athl. Train. 2005, 40, 23–29. [Google Scholar]
- Schmalzl, J.; Walter, H.; Rothfischer, W.; Blaich, S.; Gerhardt, C.; Lehmann, L.J. GIRD syndrome in male handball and volleyball players: Is the decrease of total range of motion the turning point to pathology? J. Back Musculoskelet Rehabil. 2022, 35, 755–762. [Google Scholar] [CrossRef]
- Alqarni, A.M.; Nuhmani, S.; Muaidi, Q.I. Glenohumeral internal rotation deficit in volleyball players with and without a history of shoulder pain. Res. Sports Med. 2024, 32, 225–234. [Google Scholar] [CrossRef]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Clarkson, H.M. Musculoskeletal Assessment: Joint Range of Motion, Muscle Testing, and Function, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Lin, J.J.; Yang, J.L. Reliability and validity of shoulder tightness measurement in patients with stiff shoulders. Man. Ther. 2006, 11, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Vad, V.B.; Gebeh, A.; Dines, D.; Altchek, D.; Norris, B. Hip and shoulder internal rotation range of motion deficits in professional tennis players. J. Sci. Med. Sport 2003, 6, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Harput, G.; Guney, H.; Toprak, U.; Kaya, T.; Colakoglu, F.F.; Baltaci, G. Shoulder-rotator strength, range of motion, and acromiohumeral distance in asymptomatic adolescent volleyball attackers. J. Athl. Train. 2016, 51, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Challoumas, D.; Stavrou, A.; Dimitrakakis, G. The volleyball athlete’s shoulder: Biomechanical adaptations and injury associations. Sports Biomech. 2017, 16, 220–237. [Google Scholar] [CrossRef]
- Lo, C.-L.; Hsueh, Y.-H.; Wang, C.-H.; Chang, H.-Y. Comparison of the acute effects of Kinesio Taping and Sleeper Stretching on the shoulder rotation range of motion, manual muscle strength, and sub-acromial space in pitchers with Glenohumeral Internal Rotation Deficit. Medicina 2021, 57, 102. [Google Scholar] [CrossRef]
- Mizoguchi, Y.; Suzuki, K.; Shimada, N.; Naka, H.; Kimura, F.; Akasaka, K. Prevalence of glenohumeral internal rotation deficit and sex differences in range of motion of adolescent volleyball players: A case-control study. Healthcare 2022, 10, 2263. [Google Scholar] [CrossRef]
- Mine, K.; Nakayama, T.; Milanese, S.; Grimmer, K. Effectiveness of stretching on posterior shoulder tightness and Glenohumeral Internal-Rotation Deficit: A systematic review of randomized controlled trials. J Sport Rehabil. 2017, 26, 294–305. [Google Scholar] [CrossRef]
- Clarsen, B.; Bahr, R.; Andersson, S.H.; Munk, R.; Myklebust, G. Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: A prospective cohort study. Br. J. Sports Med. 2014, 48, 1327–1333. [Google Scholar] [CrossRef]
- Kibler, W.B.; Kuhn, J.E.; Wilk, K.; Sciascia, A.; Moore, S.; Laudner, K.; Ellenbecker, T.; Thigpen, C.; Uhl, T. The disabled throwing shoulder: Spectrum of pathology-10-year update. Arthroscopy 2013, 29, 141–161. [Google Scholar] [CrossRef]
- Kinsella, S.D.; Thomas, S.J.; Huffman, G.R.; Kelly, J.D., 4th. The thrower’s shoulder. Orthop. Clin. North Am. 2014, 45, 387–401. [Google Scholar] [CrossRef]
- Matthews, M.J.; Green, D.; Matthews, H.; Swanwick, E. The effects of swimming fatigue on shoulder strength, range of motion, joint control, and performance in swimmers. Phys. Ther. Sport. 2017, 23, 118–122. [Google Scholar] [CrossRef]
- Buoite Stella, A.; Cargnel, A.; Raffini, A.; Mazzari, L.; Martini, M.; Ajčević, M.; Accardo, A.; Deodato, M.; Murena, L. Shoulder tensiomyography and isometric strength in swimmers before and after a fatiguing protocol. J. Athl. Train. 2024, 59, 738–744. [Google Scholar] [CrossRef]

{kind=link}
| ROM | Dominant Side | Non-Dominant Side | Difference Between Bilateral Sides # | p | Cohen’s d |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| SE | 51.43 ± 4.60 | 52.74 ± 6.44 | −1.31 ± 5.03 | 0.106 | 0.24 |
| SF | 177.55 ± 9.00 | 178.17 ± 8.04 | −0.62 ± 4.32 | 0.368 | 0.07 |
| IR | 42.17 ± 11.23 | 52.14 ± 10.46 | −9.97 ± 10.25 | 0.000 * | 0.92 |
| ER | 94.96 ± 10.02 | 89.83 ± 7.84 | 5.13 ± 9.10 | 0.001 * | 0.57 |
| TROM | 137.11 ± 13.09 | 141.96 ± 13.22 | −4.85 ± 12.72 | 0.021 * | 0.37 |
| Sadd | 44.87 ± 8.10 | 39.60 ± 7.24 | 5.27 ± 6.50 | 0.000 * | 0.69 |
| Sabd | 216.46 ± 10.08 | 215.52 ± 11.38 | 0.94 ± 7.15 | 0.417 | 0.08 |
| ROM | Non-GIRD (N = 25) | GIRD (N = 15) | |||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | p | Cohen’s d | Mean ± SD | p | Cohen’s d | ||
| SE | D | 52.25 ± 4.75 | 0.035 * | 0.35 | 50.05 ± 4.14 | 0.817 | 0.07 |
| ND | 54.13 ± 5.51 | 50.43 ± 7.37 | |||||
| SF | D | 177.11 ± 9.53 | 0.726 | 0.01 | 178.29 ± 8.30 | 0.245 | 0.17 |
| ND | 177.25 ± 7.90 | 179.71 ±8.31 | |||||
| IR | D | 44.69 ± 10.87 | 0.007 * | 0.47 | 37.95 ± 10.87 | 0.000 * | 1.72 |
| ND | 49.45 ± 9.54 | 56.63 ± 10.68 | |||||
| ER | D | 96.21 ± 9.46 | 0.000 * | 0.84 | 92.87 ± 10.89 | 0.543 | 0.15 |
| ND | 88.83 ± 8.10 | 91.51 ± 7.35 | |||||
| TROM | D | 140.88 ± 11.81 | 0.056 | 0.21 | 130.81 ± 13.06 | 0.000 * | 1.37 |
| ND | 138.26 ± 12.66 | 148.13 ± 12.12 | |||||
| Sadd | D | 43.30 ± 8.05 | 0.002 * | 0.58 | 47.49 ± 7.74 | 0.002 * | 0.88 |
| ND | 38.90 ± 7.07 | 40.78 ± 7.61 | |||||
| Sabd | D | 218.80 ± 8.59 | 0.257 | 0.20 | 212.71 ± 11.41 | 0.656 | 0.05 |
| ND | 216.89 ± 10.07 | 213.33 ±13.29 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, K.-Y.; Wu, W.-L.; Chiu, C.-W.; Cheng, S.-C.; Chang, H.-Y. Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players. J. Funct. Morphol. Kinesiol. 2025, 10, 67. https://doi.org/10.3390/jfmk10010067
Chou K-Y, Wu W-L, Chiu C-W, Cheng S-C, Chang H-Y. Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players. Journal of Functional Morphology and Kinesiology. 2025; 10(1):67. https://doi.org/10.3390/jfmk10010067
Chicago/Turabian StyleChou, Kun-Yu, Wan-Ling Wu, Chun-Wen Chiu, Shih-Chung Cheng, and Hsiao-Yun Chang. 2025. "Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players" Journal of Functional Morphology and Kinesiology 10, no. 1: 67. https://doi.org/10.3390/jfmk10010067
APA StyleChou, K.-Y., Wu, W.-L., Chiu, C.-W., Cheng, S.-C., & Chang, H.-Y. (2025). Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players. Journal of Functional Morphology and Kinesiology, 10(1), 67. https://doi.org/10.3390/jfmk10010067