
The Effect of Chronic Dietary Protein Manipulation on Amino Acids’ Profile and Position Sense in the Elderly Suffering from Type 2 Diabetes Mellitus


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Description and Eligibility Criteria
2.2. Study Design
2.3. Dietary Assessment
2.4. Anthropometric Characteristics and Appendicular Lean Mass Assessment
2.5. Hematological Measurements
2.6. Muscle Strength Assessment
2.7. Position Sense Assessment
2.8. Statistical Analysis
3. Results
3.1. Dietary Assessment
3.2. Anthropometric Characteristics and Appendicular Lean Mass Assessment
3.3. Hematological Measurements
3.4. Muscle Strength Assessment
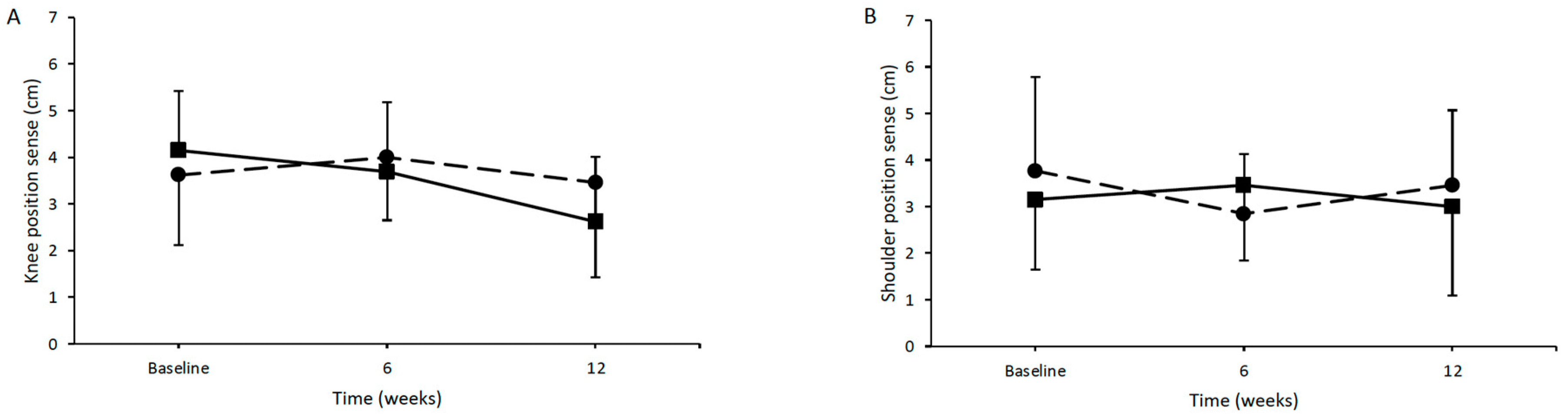
3.5. Position Sense Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2011, 34 (Suppl. S1), S62–S69. [Google Scholar] [CrossRef] [PubMed]
- Argyropoulou, D.; Geladas, N.D.; Nomikos, T.; Paschalis, V. Exercise and Nutrition Strategies for Combating Sarcopenia and Type 2 Diabetes Mellitus in Older Adults. J. Funct. Morphol. Kinesiol. 2022, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Onder, G.; Bernabei, R. Sarcopenia and diabetes: Two sides of the same coin. J. Am. Med. Dir. Assoc. 2013, 14, 540–541. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diabetes Action Now: An Initiative of the World Health Organization and the International Diabetes Federation. 2004. Available online: https://www.who.int/publications/i/item/diabetes-action-now (accessed on 15 November 2023).
- Khazrai, Y.M.; Defeudis, G.; Pozzilli, P. Effect of diet on type 2 diabetes mellitus: A review. Diabetes/Metab. Res. Rev. 2014, 30, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: A comprehensive review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Polito, R.; La Torre, M.E.; Moscatelli, F.; Cibelli, G.; Valenzano, A.; Panaro, M.A.; Monda, M.; Messina, A.; Monda, V.; Pisanelli, D.; et al. The Ketogenic Diet and Neuroinflammation: The Action of Beta-Hydroxybutyrate in a Microglial Cell Line. Int. J. Mol. Sci. 2023, 24, 3102. [Google Scholar] [CrossRef]
- Gannon, M.C.; Nuttall, F.Q. Control of blood glucose in type 2 diabetes without weight loss by modification of diet composition. Nutr. Metab. 2006, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Newsholme, P.; Brennan, L.; Rubi, B.; Maechler, P. New insights into amino acid metabolism, beta-cell function and diabetes. Clin. Sci. 2005, 108, 185–194. [Google Scholar] [CrossRef]
- Cuthbertson, D.; Smith, K.; Babraj, J.; Leese, G.; Waddell, T.; Atherton, P.; Wackerhage, H.; Taylor, P.M.; Rennie, M.J. Anabolic signaling deficits underlie amino acid resistance of wasting, aging muscle. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2005, 19, 422–424. [Google Scholar] [CrossRef]
- Sinclair, A.; Morley, J.E.; Rodriguez-Mañas, L.; Paolisso, G.; Bayer, T.; Zeyfang, A.; Bourdel-Marchasson, I.; Vischer, U.; Woo, J.; Chapman, I.; et al. Diabetes mellitus in older people: Position statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J. Am. Med. Dir. Assoc. 2012, 13, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Opizzi, A.; Antoniello, N.; Boschi, F.; Iadarola, P.; Pasini, E.; Aquilani, R.; Dioguardi, F.S. Effect of essential amino acid supplementation on quality of life, amino acid profile and strength in institutionalized elderly patients. Clin. Nutr. 2011, 30, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Gang, X.; Wang, G.; Xiao, X.; Li, Z.; Jiang, Z.; Wang, G. A cross-sectional study: Associations between sarcopenia and clinical characteristics of patients with type 2 diabetes. Medicine 2020, 99, e18708. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Hatef, B.; Bahrpeyma, F.; Mohajeri Tehrani, M.R. The comparison of muscle strength and short-term endurance in the different periods of type 2 diabetes. J. Diabetes Metab. Disord. 2014, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Cetinus, E.; Buyukbese, M.A.; Uzel, M.; Ekerbicer, H.; Karaoguz, A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2005, 70, 278–286. [Google Scholar] [CrossRef]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef]
- Wander, P.L.; Boyko, E.J.; Leonetti, D.L.; McNeely, M.J.; Kahn, S.E.; Fujimoto, W.Y. Greater hand-grip strength predicts a lower risk of developing type 2 diabetes over 10 years in leaner Japanese Americans. Diabetes Res. Clin. Pract. 2011, 92, 261–264. [Google Scholar] [CrossRef]
- Sun, Z.; Liu, L.; Liu, N.; Liu, Y. Muscular response and adaptation to diabetes mellitus. Front. Biosci. 2008, 13, 4765–4794. [Google Scholar] [CrossRef][Green Version]
- Joshi, S.A.; Patel, V.D.; Eapen, C.; Hariharan, K. Proportion and distribution of upper extremity musculoskeletal disorders and its association with disability in type 2 diabetes mellitus. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2022, 35, 597–604. [Google Scholar] [CrossRef]
- Van Eetvelde, B.L.M.; Lapauw, B.; Proot, P.; Vanden Wyngaert, K.; Helleputte, S.; Stautemas, J.; Cambier, D.C.; Calders, P. The impact of diabetic neuropathy on the distal versus proximal comparison of weakness in lower and upper limb muscles of patients with type 2 diabetes mellitus: A cross-sectional study. J. Musculoskelet. Neuronal Interact. 2021, 21, 464–474. [Google Scholar] [PubMed]
- Majjad, A.; Errahali, Y.; Toufik, H.; Djossou, J.H.; Ghassem, M.A.; Kasouati, J.; Maghraoui, A.E. Musculoskeletal Disorders in Patients with Diabetes Mellitus: A Cross-Sectional Study. Int. J. Rheumatol. 2018, 2018, 3839872. [Google Scholar] [CrossRef] [PubMed]
- Paschalis, V.; Nikolaidis, M.G.; Giakas, G.; Jamurtas, A.Z.; Pappas, A.; Koutedakis, Y. The effect of eccentric exercise on position sense and joint reaction angle of the lower limbs. Muscle Nerve 2007, 35, 496–503. [Google Scholar] [CrossRef]
- Paschalis, V.; Nikolaidis, M.G.; Giakas, G.; Jamurtas, A.Z.; Koutedakis, Y. Differences between arms and legs on position sense and joint reaction angle. J. Strength Cond. Res. 2009, 23, 1652–1655. [Google Scholar] [CrossRef] [PubMed]
- Paschalis, V.; Nikolaidis, M.G.; Theodorou, A.A.; Giakas, G.; Jamurtas, A.Z.; Koutedakis, Y. Eccentric exercise affects the upper limbs more than the lower limbs in position sense and reaction angle. J. Sports Sci. 2010, 28, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Weerakkody, N.; Percival, P.; Morgan, D.L.; Gregory, J.E.; Proske, U. Matching different levels of isometric torque in elbow flexor muscles after eccentric exercise. Exp. Brain Res. 2003, 149, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Asiri, F.; Reddy, R.S.; Narapureddy, B.R.; Raizah, A. Comparisons and Associations between Hip-Joint Position Sense and Glycosylated Hemoglobin in Elderly Subjects with Type 2 Diabetes Mellitus-A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 15514. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, L.R.; Boucher, A.; Simonovich, E. Patients with type 2 diabetes demonstrate proprioceptive deficit in the knee. World J. Diabetes 2018, 9, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Noohu, M.M.; Verma, S.; Singla, D.; Hussain, M.E. Effect of sensorimotor training on balance measures and proprioception among middle and older age adults with diabetic peripheral neuropathy. Gait Posture 2019, 74, 114–120. [Google Scholar] [CrossRef]
- Brockett, C.; Warren, N.; Gregory, J.E.; Morgan, D.L.; Proske, U. A comparison of the effects of concentric versus eccentric exercise on force and position sense at the human elbow joint. Brain Res. 1997, 771, 251–258. [Google Scholar] [CrossRef]
- Dedrick, M.E.; Clarkson, P.M. The effects of eccentric exercise on motor performance in young and older women. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Food and Nutrition Board of the Institute of Medicine, The National Academies Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Wareham, N.J.; Jakes, R.W.; Rennie, K.L.; Schuit, J.; Mitchell, J.; Hennings, S.; Day, N.E. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2003, 6, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Van Staveren, W.A.; Ocké, M.C.; de Vries, J.H. Estimation of dietary intake. In Present Knowledge in Nutrition, 11th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2012; pp. 1012–1026. [Google Scholar]
- Rhodes, D.G.; Morton, S.; Myrowitz, R.; Moshfegh, A.J. Food and Nutrient Database for Dietary Studies 2019–2020: An application database for national dietary surveillance. J. Food Compos. Anal. 2023, 123, 105547. [Google Scholar] [CrossRef]
- Pischon, T.; Boeing, H.; Hoffmann, K.; Bergmann, M.; Schulze, M.B.; Overvad, K.; van der Schouw, Y.T.; Spencer, E.; Moons, K.G.; Tjønneland, A.; et al. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2008, 359, 2105–2120. [Google Scholar] [CrossRef] [PubMed]
- Czernichow, S.; Kengne, A.P.; Stamatakis, E.; Hamer, M.; Batty, G.D. Body mass index, waist circumference and waist-hip ratio: Which is the better discriminator of cardiovascular disease mortality risk? Evidence from an individual-participant meta-analysis of 82 864 participants from nine cohort studies. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Lee, J.S.; Kuller, L.H.; Boudreau, R.; De Rekeneire, N.; Harris, T.B.; Kritchevsky, S.; Tylavsky, F.A.; Nevitt, M.; et al. Excessive loss of skeletal muscle mass in older adults with type 2 diabetes. Diabetes Care 2009, 32, 1993–1997. [Google Scholar] [CrossRef]
- Demirtas, L.; Degirmenci, H.; Akbas, E.M.; Ozcicek, A.; Timuroglu, A.; Gurel, A.; Ozcicek, F. Association of hematological indicies with diabetes, impaired glucose regulation and microvascular complications of diabetes. Int. J. Clin. Exp. Med. 2015, 8, 11420–11427. [Google Scholar] [PubMed]
- Farooqui, R.; Afsar, N.; Afroze, I.A. Role and significance of hematological parameters in diabetes mellitus. Ann. Pathol. Lab. Med. 2019, 6, A158–A162. [Google Scholar] [CrossRef]
- Methenitis, S.; Mouratidis, A.; Manga, K.; Chalari, E.; Feidantsis, K.; Arnaoutis, G.; Arailoudi-Alexiadou, X.; Skepastianos, P.; Hatzitolios, A.; Mourouglakis, A.; et al. The importance of protein intake in master marathon runners. Nutrition 2021, 86, 111154. [Google Scholar] [CrossRef]
- Walsh, L.D.; Hesse, C.W.; Morgan, D.L.; Proske, U. Human forearm position sense after fatigue of elbow flexor muscles. J. Physiol. 2004, 558 Pt 2, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Li, Y.; Tobias, D.K.; Pan, A.; Hu, F.B. Dietary Protein Intake and Risk of Type 2 Diabetes in US Men and Women. Am. J. Epidemiol. 2016, 183, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Borack, M.S.; Volpi, E. Efficacy and safety of leucine supplementation in the elderly. J. Nutr. 2016, 146, 2625S–2629S. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.K. Sarcopenia: A contemporary health problem among older adult populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Bahadoran, Z.; Esfandyari, S.; Azizi, F. Dietary Protein and Amino Acid Profiles in Relation to Risk of Dysglycemia: Findings from a Prospective Population-Based Study. Nutrients 2017, 9, 971. [Google Scholar] [CrossRef] [PubMed]
- Solerte, S.B.; Gazzaruso, C.; Bonacasa, R.; Rondanelli, M.; Zamboni, M.; Basso, C.; Locatelli, E.; Schifino, N.; Giustina, A.; Fioravanti, M. Nutritional supplements with oral amino acid mixtures increases whole-body lean mass and insulin sensitivity in elderly subjects with sarcopenia. Am. J. Cardiol. 2008, 101, S69–S77. [Google Scholar] [CrossRef] [PubMed]
- Hanach, N.I.; McCullough, F.; Avery, A. The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: A systematic review and meta-analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Alemán-Mateo, H.; Carreón, V.R.; Macías, L.; Astiazaran-García, H.; Gallegos-Aguilar, A.C.; Ramos Enriquez, J.R. Nutrient-rich dairy proteins improve appendicular skeletal muscle mass and physical performance, and attenuate the loss of muscle strength in older men and women subjects: A single-blind randomized clinical trial. Clin. Interv. Aging 2014, 1517–1525. [Google Scholar] [CrossRef]
- Børsheim, E.; Bui, Q.U.T.; Tissier, S.; Kobayashi, H.; Ferrando, A.A.; Wolfe, R.R. Effect of amino acid supplementation on muscle mass, strength and physical function in elderly. Clin. Nutr. 2008, 27, 189–195. [Google Scholar] [CrossRef]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2018, 37, 2260–2270. [Google Scholar] [CrossRef] [PubMed]
- Abila, B.; Wilson, J.F.; Marshall, R.W.; Richens, A. Exercise-induced hand tremor: A possible test for beta 2-adrenoceptor selectivity in man? Br. J. Clin. Pharmacol. 1986, 22, 104–107. [Google Scholar]
- Moore, J.B.; Korff, T.; Kinzey, S.J. Acute effects of a single bout of resistance exercise on postural control in elderly persons. Percept. Mot. Ski. 2005, 100 Pt 1, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Allen, T.J. Damage to skeletal muscle from eccentric exercise. Exerc. Sport Sci. Rev. 2005, 33, 98–104. [Google Scholar] [CrossRef]
- Mueller, M.J.; Sorensen, C.J.; McGill, J.B.; Clark, B.R.; Lang, C.E.; Chen, L.; Bohnert, K.L.; Hastings, M.K. Effect of a Shoulder Movement Intervention on Joint Mobility, Pain, and Disability in People with Diabetes: A Randomized Controlled Trial. Phys. Ther. 2018, 98, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.M.; Clark, B.R.; McGill, J.B.; Mueller, M.J. Upper extremity impairments, pain and disability in patients with diabetes mellitus. Physiotherapy 2015, 101, 147–154. [Google Scholar] [CrossRef]
- Reuben, D.B.; Seeman, T.E.; Keeler, E.; Hayes, R.P.; Bowman, L.; Sewall, A.; Hirsch, S.H.; Wallace, R.B.; Guralnik, J.M. Refining the categorization of physical functional status: The added value of combining self-reported and performance-based measures. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 1056–1061. [Google Scholar] [CrossRef]


{kind=link}
| Control Group (Men = 6, Women = 7) | Intervention Group (Men = 7, Women = 6) | |
|---|---|---|
| Age (years) | 59.31 ± 6.82 | 60.62 ± 6.84 |
| Height (cm) | 166.15 ± 11.53 | 168.85 ± 9.38 |
| Weight (kg) | 92.27 ± 24.26 | 80.88 ± 13.91 |
| Body mass index | 33.16 ± 7.48 | 28.34 ± 4.29 |
| Group | Baseline | 6 Weeks | 12 Weeks | ptime | pgroup | ptime*group | R | |
|---|---|---|---|---|---|---|---|---|
| Energy (kcal) | CG | 2052 ± 616 | 2137 ± 623 | 2102 ± 569 | 0.40 | 0.60 | 0.89 | - |
| IG | 1947 ± 181 | 2032 ± 246 | 2027 ± 257 | 0.25 | ||||
| Protein (g/kg/day) | CG | 0.80 ± 0.22 | 0.85 ± 0.20 | 0.94 ± 0.16 | 0.13 | <0.05 | <0.05 | - |
| IG | 0.81 ± 0.17 | 1.21 ± 0.18 a | 1.42 ± 0.12 bc | <0.05 | ||||
| Tryptophan (mg/kg/day) | CG | 5.75 ± 2.33 | 6.37 ± 2.98 | 7.34 ± 3.01 | 0.27 | <0.05 | 0.16 | 8 |
| IG | 6.06 ± 2.56 | 8.25 ± 2.45 a | 9.87 ± 2.99 b | <0.05 | ||||
| Threonine (mg/kg/day) | CG | 20.24 ± 8.80 | 21.50 ± 10.32 | 25.55 ± 10.91 | 0.30 | <0.05 | 0.18 | 28 |
| IG | 21.03 ± 9.98 | 28.37 ± 9.53 a | 34.16 ± 11.02 b | <0.05 | ||||
| Isoleucine (mg/kg/day) | CG | 22.28 ± 10.20 | 24.10 ± 11.82 | 28.99 ± 13.80 | 0.28 | <0.05 | 0.21 | 23 |
| IG | 22.84 ± 11.04 | 31.11 ± 10.47 a | 38.49 ± 12.92 b | <0.05 | ||||
| Leucine (mg/kg/day) | CG | 37.19 ± 15.48 | 40.28 ± 19 | 47.19 ± 20.26 | 0.30 | <0.01 | 0.23 | 49 |
| IG | 40.4 ± 19.13 | 53.98 ± 18.69 | 63.74 ± 20.35 b | <0.05 | ||||
| Lysine (mg/kg/day) | CG | 34.09 ± 17.63 | 35.12 ± 19.56 | 44.24 ± 21.75 | 0.31 | <0.05 | 0.29 | 48 |
| IG | 36.07 ± 19.12 | 46.71 ± 19.54 | 60.51 ± 21.12 bc | <0.05 | ||||
| Valine (mg/kg/day) | CG | 24.71 ± 9.93 | 26.80 ± 12.66 | 32.02 ± 14.19 | 0.25 | <0.05 | 0.33 | 32 |
| IG | 27.21 ± 13.38 | 35.36 ± 12.46 | 42.16 ± 14.47 b | <0.05 | ||||
| Histidine (mg/kg/day) | CG | 14.12 ± 7.04 | 14.28 ± 6.64 | 16.79 ± 7.47 | 0.51 | <0.05 | 0.11 | 18 |
| IG | 14.01 ± 6.22 | 19.42 ± 7.62 | 23.5 ± 6.97 b | <0.05 | ||||
| Methionine + cysteine (mg/kg/day) | CG | 18.60 ± 8.39 | 19.95 ± 10.19 | 23.94 ± 10.82 | 0.27 | <0.05 | 0.21 | 23 |
| IG | 19.40 ± 9.85 | 25.96 ± 9.36 a | 31.84 ± 10.77 b | <0.05 | ||||
| Phenylananine + tyrosine (mg/kg/day) | CG | 37.06 ± 14.98 | 39.90 ± 18.78 | 47.09 ± 20.40 | 0.27 | <0.05 | 0.23 | 48 |
| IG | 39.43 ± 18.67 | 52.53 ± 18.10 a | 61.92 ± 20.53 b | <0.05 |
| Group | Baseline | 6 Weeks | 12 Weeks | ptime | pgroup | ptime*group | |
|---|---|---|---|---|---|---|---|
| Weight (kg) | CG | 92.27 ± 24.26 | 91.91 ± 23.64 | 91.25 ± 21.97 | 0.56 | 0.17 | 0.66 |
| IG | 80.88 ± 13.91 | 81 ± 14.04 | 80.68 ± 14.06 | 0.39 | |||
| Body mass index | CG | 33.16 ± 7.48 | 33.02 ± 7.06 | 32.77 ± 6.12 | 0.54 | 0.06 | 0.61 |
| IG | 28.34 ± 4.29 | 28.40 ± 4.47 | 28.28 ± 4.47 | 0.40 | |||
| Waist circumference (cm) | CG | 103.77 ± 17.81 | 103.23 ± 18.14 | 102.5 ± 16.07 | 0.50 | 0.33 | 0.67 |
| IG | 97.81 ± 14.18 | 96.38 ± 14.13 a | 96.23 ± 13.98 b | <0.05 | |||
| Hip circumference (cm) | CG | 112.27 ± 13.89 | 111.69 ± 14.37 | 110.92 ± 13.29 | 0.30 | 0.20 | 0.98 |
| IG | 106.15 ± 8.79 | 105.54 ± 8.98 | 104.73 ± 8.19 | 0.07 | |||
| Waist/hip ratio | CG | 0.92 ± 0.09 | 0.92 ± 0.09 | 0.92 ± 0.09 | 0.90 | 0.85 | 0.61 |
| IG | 0.92 ± 0.09 | 0.91 ± 0.08 a | 0.92 ± 0.09 | 0.25 | |||
| Appendicular lean mass (kg) | CG | 22.78 ± 6.35 | - | 20.95 ± 6.38 b | <0.05 | 0.51 | <0.05 |
| IG | 20.08 ± 4.66 | - | 20.57 ± 5.04 | 0.29 |
| Group | Baseline | 6 Weeks | 12 Weeks | ptime | pgroup | ptime*group | |
|---|---|---|---|---|---|---|---|
| WBC (103/uL) | CG | 6.90 ± 1.94 | 7.58 ± 1.90 | 7.41 ± 1.74 | 0.50 | 0.140 | 0.50 |
| IG | 5.99 ± 1.88 | 6.78 ± 2.65 | 6.25 ± 2.17 | 0.14 | |||
| HGB (g/dL) | CG | 14.61 ± 2.88 | 16.80 ± 5.92 | 14.64 ± 1.51 | 0.26 | 0.38 | 0.86 |
| IG | 14.57 ± 2.03 | 14.24 ± 1.87 | 15.21 ± 4.67 | 0.53 | |||
| RBC (10⁶/uL) | CG | 4.87 ± 0.74 | 5.61 ± 1.51 | 5.19 ± 0.61 | 0.24 | 0.25 | 0.88 |
| IG | 5.09 ± 0.52 | 6.28 ± 3.53 | 5.34 ± 1.21 | 0.45 | |||
| HCT (%) | CG | 44.54 ± 8.48 | 51.37 ± 16.6 | 44.91 ± 3.59 | 0.25 | 0.37 | 0.17 |
| IG | 44.51 ± 5.24 | 43.46 ± 4.57 | 46.61 ± 13.14 | 0.49 | |||
| PLT (103/uL) | CG | 262.00 ± 97.88 | 274.00 ± 140.87 | 281.43 ± 79.36 | 0.58 | 0.67 | 0.29 |
| IG | 240.00 ± 56.57 | 257.50 ± 38.43 | 227.13 ± 58.50 | 0.23 |
| Group | Baseline | 6 Weeks | 12 Weeks | ptime | pgroup | ptime*group | |
|---|---|---|---|---|---|---|---|
| Knee extension (kg) | CG | 27.60 ± 8.30 | 26.00 ± 7.40 | 25.10 ± 8.50 b | <0.05 | 0.613 | <0.05 |
| IG | 26.10 ± 6.20 | 27.60 ± 6.60 | 29.50 ± 7.00 bc | <0.05 | |||
| Shoulder extension (kg) | CG | 16.80 ± 7.70 | 16.70 ± 7.80 | 15.70 ± 7.10 | <0.05 | <0.05 | <0.05 |
| IG | 14.00 ± 4.70 | 14.40 ± 4.80 | 15.60 ± 5.10 bc | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argyropoulou, D.; Nomikos, T.; Terzis, G.; Karakosta, M.; Aphamis, G.; Geladas, N.D.; Paschalis, V. The Effect of Chronic Dietary Protein Manipulation on Amino Acids’ Profile and Position Sense in the Elderly Suffering from Type 2 Diabetes Mellitus. J. Funct. Morphol. Kinesiol. 2024, 9, 62. https://doi.org/10.3390/jfmk9020062
Argyropoulou D, Nomikos T, Terzis G, Karakosta M, Aphamis G, Geladas ND, Paschalis V. The Effect of Chronic Dietary Protein Manipulation on Amino Acids’ Profile and Position Sense in the Elderly Suffering from Type 2 Diabetes Mellitus. Journal of Functional Morphology and Kinesiology. 2024; 9(2):62. https://doi.org/10.3390/jfmk9020062
Chicago/Turabian StyleArgyropoulou, Dionysia, Tzortzis Nomikos, Gerasimos Terzis, Myrto Karakosta, George Aphamis, Nickos D. Geladas, and Vassilis Paschalis. 2024. "The Effect of Chronic Dietary Protein Manipulation on Amino Acids’ Profile and Position Sense in the Elderly Suffering from Type 2 Diabetes Mellitus" Journal of Functional Morphology and Kinesiology 9, no. 2: 62. https://doi.org/10.3390/jfmk9020062
APA StyleArgyropoulou, D., Nomikos, T., Terzis, G., Karakosta, M., Aphamis, G., Geladas, N. D., & Paschalis, V. (2024). The Effect of Chronic Dietary Protein Manipulation on Amino Acids’ Profile and Position Sense in the Elderly Suffering from Type 2 Diabetes Mellitus. Journal of Functional Morphology and Kinesiology, 9(2), 62. https://doi.org/10.3390/jfmk9020062