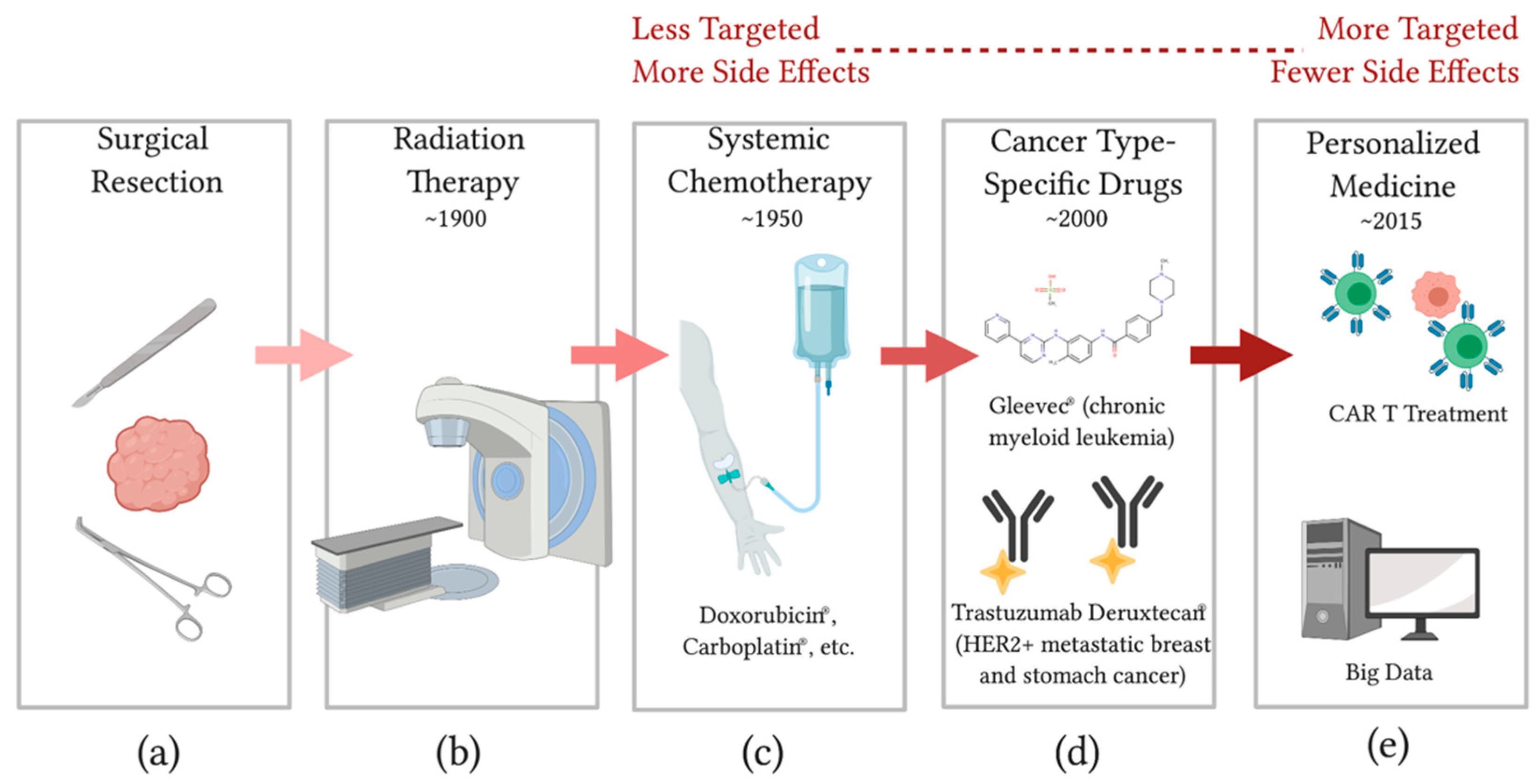
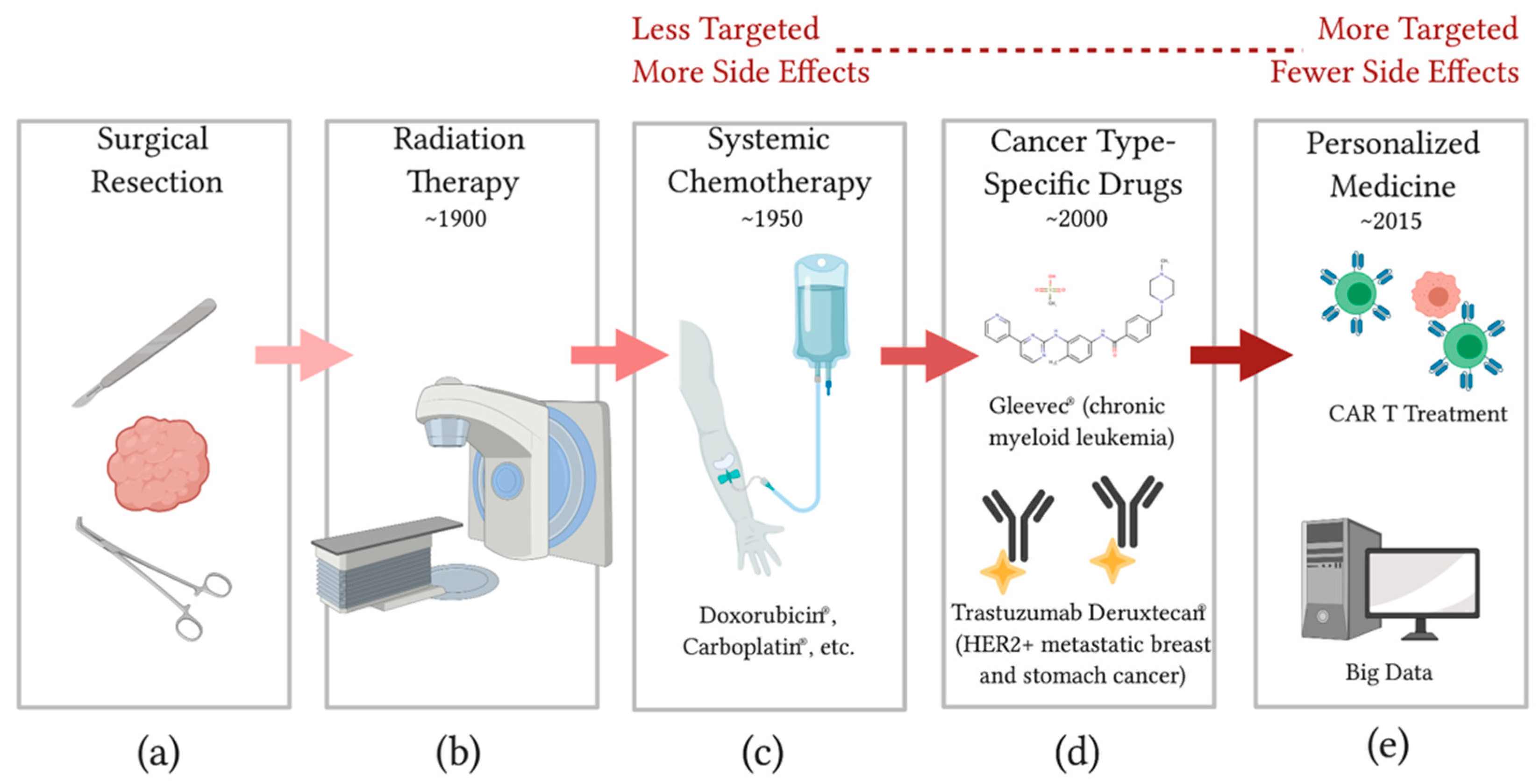
Advancing Therapies for Cancer—From Mustard Gas to CAR T


{kind=link}
Abstract
:1. Introduction
2. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Sudhakar, A. History of cancer, ancient and modern treatment methods. J. Cancer Sci. Ther. 2009, 1, 1–4. [Google Scholar] [CrossRef] [Green Version]
- DeVita, V.T.; Chu, E. A history of cancer chemotherapy. Cancer Res. 2008, 68, 8643–8653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.L. War! What is it good for? Mustard gas medicine. Can. Med. Assoc. J. 2017, 189, E321–E322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coates, A.; Abraham, S.; Kaye, S.; Sowerbutts, T.; Frewin, C.; Fox, R.; Tattersall, M. On the receiving end—Patient perception of the side-effects of cancer chemotherapy. Eur. J. Cancer Clin. Oncol. 1983, 19, 203–208. [Google Scholar] [CrossRef]
- Friedman, A.A.; Letai, A.; Fisher, D.E.; Flaherty, K.T. Precision medicine for cancer with next-generation functional diagnostics. Nat. Rev. Cancer 2015, 15, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Herrero, E.; Fernandez-Medarde, A. Advanced targeted therapies in cancer: Drug nanocarriers, the future of chemotherapy. Eur. J. Pharm. Biopharm. 2015, 93, 52–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.T.; Tan, Y.J.; Oon, C.E. Molecular targeted therapy: Treating cancer with specificity. Eur. J. Pharmacol. 2018, 834, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Boluda, J.C.; Cervantes, F. Imatinib mesylate (Gleevec, Glivec): A new therapy for chronic myeloid leukemia and other malignancies. Drugs Today 2002, 38, 601. [Google Scholar] [CrossRef]
- Chen, S.; Song, Z.; Zhang, A. Small-molecule immuno-oncology therapy: Advances, challenges and new directions. Curr. Top. Med. Chem. 2019, 19, 180–185. [Google Scholar] [CrossRef]
- Imai, K.; Takaoka, A. Comparing antibody and small-molecule therapies for cancer. Nat. Rev. Cancer 2006, 6, 714–727. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N. Engl. J. Med. 2019, 382, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Tsurutani, J.; Takahashi, S.; Iwata, H.; Krop, I.; Redfern, C.; Sagara, Y.; Doi, T.; Park, H.; Murthy, R.K.; et al. Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-positive breast cancer previously treated with trastuzumab emtansine: A dose-expansion, phase 1 study. Lancet Oncol. 2019, 20, 816–826. [Google Scholar] [CrossRef]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996, 271, 1734–1736. [Google Scholar] [CrossRef] [Green Version]
- Stern, L.A.; Jonsson, V.D.; Priceman, S.J. CAR T cell therapy progress and challenges for solid tumors. Cancer Treat. Res. 2020, 180, 297–326. [Google Scholar] [CrossRef]
- Cappello, P.; Novelli, F. Next generation of cancer immunotherapy calls for combination. Oncoscience 2017, 4, 19–20. [Google Scholar] [CrossRef]
- He, L.; Kulesskiy, E.; Saarela, J.; Turunen, L.; Wennerberg, K.; Aittokallio, T.; Tang, J. Methods for high-throughput drug combination screening and synergy scoring. Methods Mol. Biol. 2018, 1711, 351–398. [Google Scholar] [CrossRef]
- Kantarjian, H.; Yu, P.P. Artificial intelligence, big data, and cancer. JAMA Oncol. 2015, 1, 573–574. [Google Scholar] [CrossRef]
- Kather, J.N.; Charoentong, P.; Suarez-Carmona, M.; Herpel, E.; Klupp, F.; Ulrich, A.; Schneider, M.; Zoernig, I.; Luedde, T.; Jaeger, D.; et al. High-throughput screening of combinatorial immunotherapies with patient-specific in silico models of metastatic colorectal cancer. Cancer Res. 2018, 78, 5155–5163. [Google Scholar] [CrossRef] [Green Version]
- Kondo, J.; Ekawa, T.; Endo, H.; Yamazaki, K.; Tanaka, N.; Kukita, Y.; Okuyama, H.; Okami, J.; Imamura, F.; Ohue, M.; et al. High-throughput screening in colorectal cancer tissue-originated spheroids. Cancer Sci. 2018, 110, 345–355. [Google Scholar] [CrossRef]
- Low, S.-K.; Zembutsu, H.; Nakamura, Y. Breast cancer: The translation of big genomic data to cancer precision medicine. Cancer Sci. 2017, 109, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarrell, D.K.; Drake, S.; Brown, M.A. Advancing Therapies for Cancer—From Mustard Gas to CAR T. Sci 2020, 2, 90. https://doi.org/10.3390/sci2040090
Jarrell DK, Drake S, Brown MA. Advancing Therapies for Cancer—From Mustard Gas to CAR T. Sci. 2020; 2(4):90. https://doi.org/10.3390/sci2040090
Chicago/Turabian StyleJarrell, Dillon K., Seth Drake, and Mark A. Brown. 2020. "Advancing Therapies for Cancer—From Mustard Gas to CAR T" Sci 2, no. 4: 90. https://doi.org/10.3390/sci2040090
APA StyleJarrell, D. K., Drake, S., & Brown, M. A. (2020). Advancing Therapies for Cancer—From Mustard Gas to CAR T. Sci, 2(4), 90. https://doi.org/10.3390/sci2040090