
Comparison of Aneurysmal and Non-Aneurysmal Spontaneous Cervical Artery Dissections in a Large Multicenter Cohort



 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
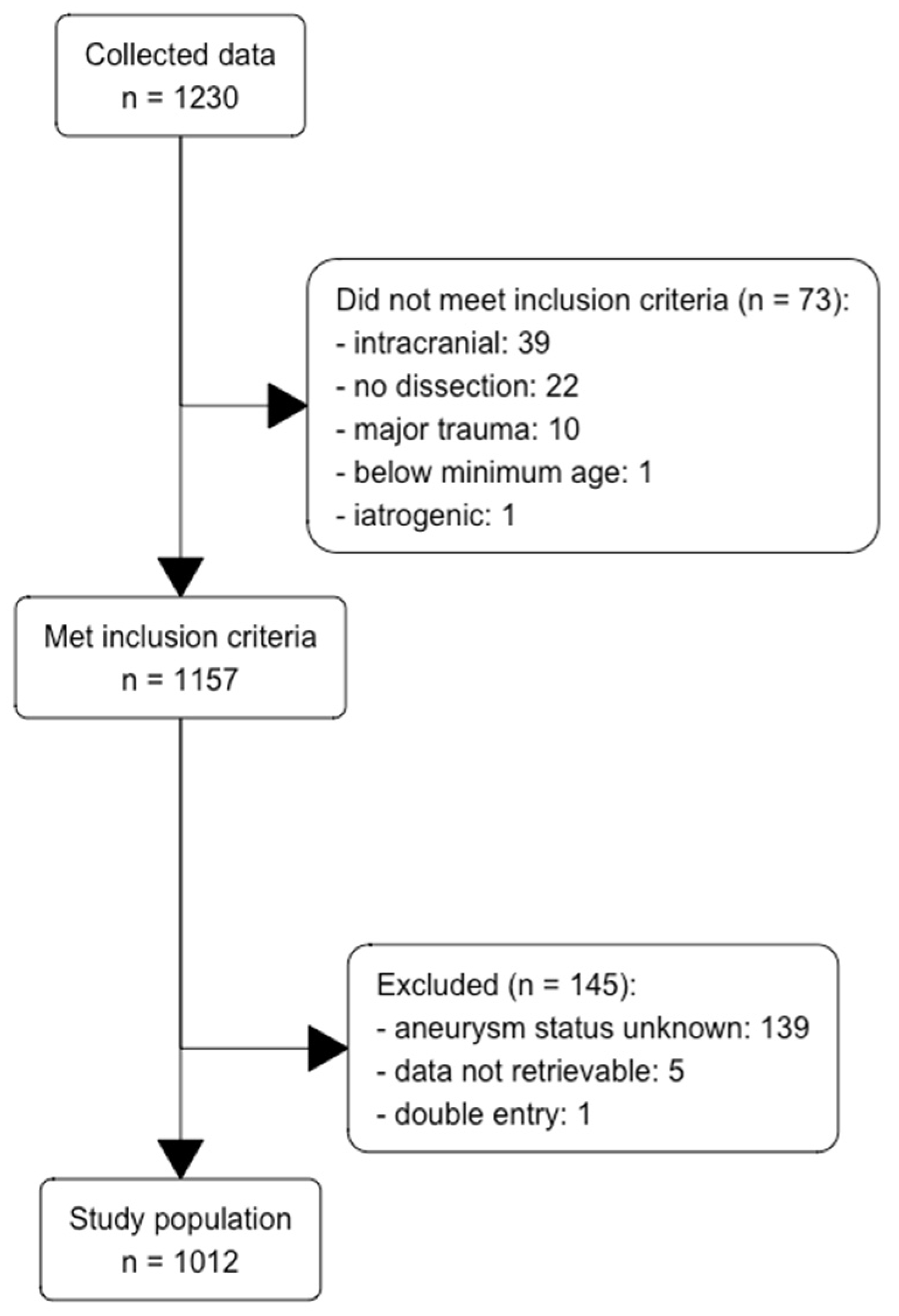
3.1. Description of Patients
3.2. Comparison of Patients with and without DAs
4. Discussion
4.1. Risk Factors
4.2. Symptoms
4.3. Outcome
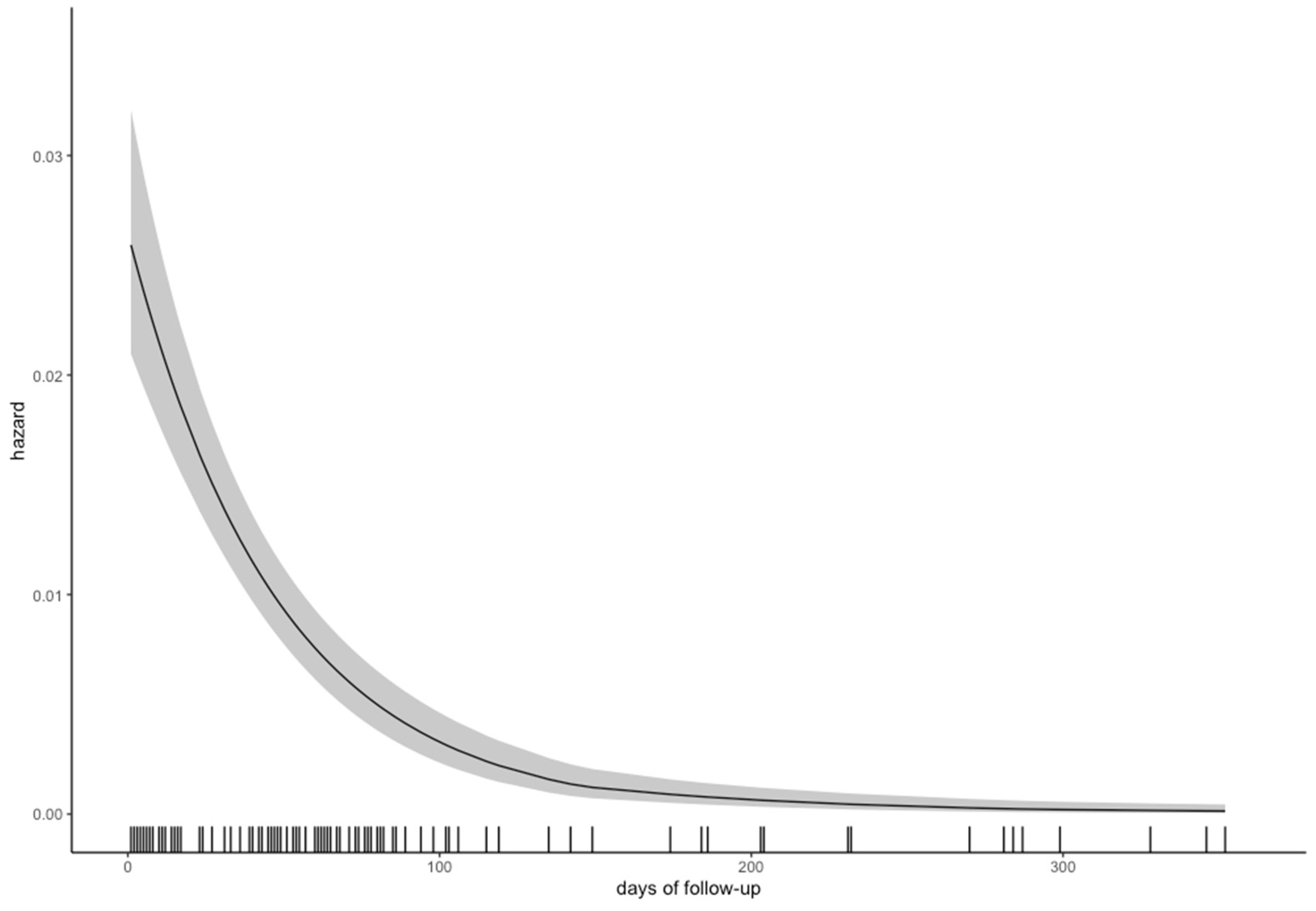
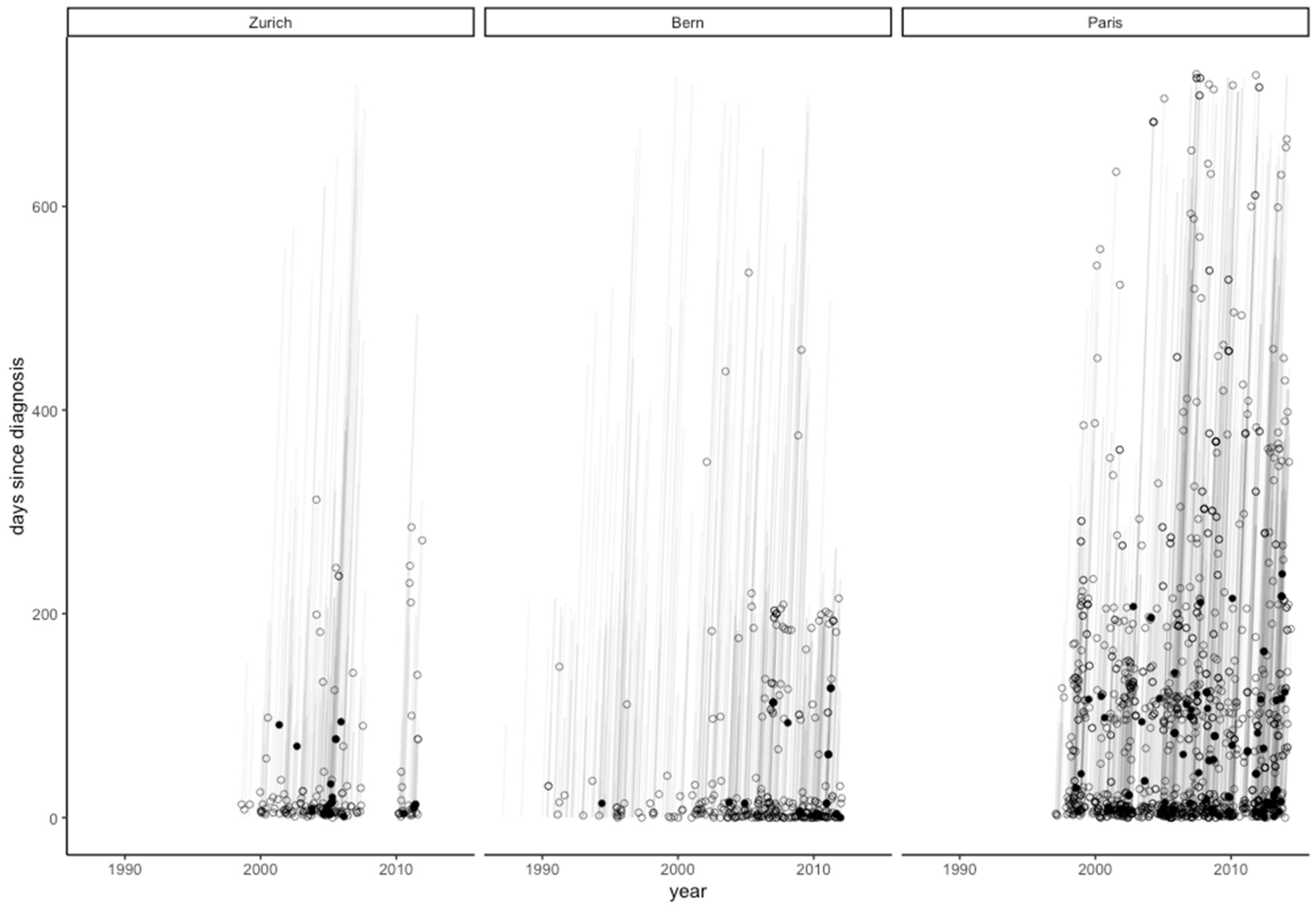
4.4. Time Course
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients Included in Analysis | No Aneurysm | Aneurysm | Univariate Analysis | |
|---|---|---|---|---|
| n (% Missing Data) | Median (IQR)/ n (%) | Median (IQR)/ n (%) | p-Value | |
| Age | 1004 (0.0) | 45.0 (38.0 to 52.0) | 44.5 (38.0 to 52.0) | 1 |
| Female sex | 1004 (0.0) | 399 (43.8) | 48 (51.1) | 0.405 |
| Days to diagnosis | 1004 (0.0) | 5.0 (2.0 to 12.0) | 7.0 (5.0 to 15.0) | 0.006 |
| Vessel affected | 1004 (0.0) | 0.567 * | ||
| ICA | 589 (64.7) | 44 (46.8) | ||
| VA | 275 (30.2) | 28 (29.8) | ||
| ICA + VA | 46 (5.1) | 22 (23.4) | ||
| Multiple dissections | 1004 (0.0) | 146 (16.0) | 34 (36.2) | 0.195 * |
| Fever and infection | 919 (8.5) | 86 (10.3) | 7 (8.0) | 0.872 |
| Minor trauma | 1001 (0.3) | 206 (22.7) | 21 (22.8) | 1 |
| Connective tissue disease | 998 (0.6) | 0.429 | ||
| Family history | Family history | 16 (1.8) | ||
| Diagnosed | Diagnosed | 17 (1.9) | ||
| Family history of ischemic stroke | 987 (1.7) | 126 (14.1) | 11 (11.8) | 0.884 |
| Smoking | 996 (0.8) | 0.088 | ||
| Former | Former | 123 (13.6) | ||
| Current | Current | 263 (29.1) | ||
| Arterial hypertension | 1003 (0.1) | 199 (21.9) | 25 (26.6) | 0.564 |
| Hypercholesterolemia | 842 (16.1) | 417 (54.2) | 31 (43.1) | 0.301 |
| Migraine | 971 (3.3) | 0.336 | ||
| Without aura | Without aura | 167 (19.0) | ||
| With aura | With aura | 87 (9.9) | ||
| Diabetes mellitus | 1003 (0.1) | 20 (2.2) | 2 (2.1) | 1 |
| Hormonal anticonception | 431 (3.6) | 120 (31.1) | 9 (20.0) | 0.336 |
| Headache | 1002 (0.2) | 656 (72.2) | 64 (68.1) | 0.669 |
| VAS headache | 445 (38.2) | 7.0 (5.0 to 8.0) | 7.0 (6.0 to 10.0) | 0.311 |
| Thunderclap headache | 893 (11.1) | 51 (6.3) | 9 (11.0) | 0.311 |
| Cervical pain | 1001 (0.3) | 412 (45.4) | 48 (51.6) | 0.484 |
| VAS cervical pain | 248 (46.1) | 6.0 (5.0 to 8.0) | 7.0 (5.8 to 8.0) | 0.274 |
| Radiculopathy | 996 (0.8) | 5 (0.6) | 0 (0.0) | 1 |
| Spinal infarction | 1004 (0.0) | 1 (0.1) | 0 (0.0) | 1 |
| Subarachnoid hemorrhage | 1002 (0.2) | 13 (1.4) | 7 (7.4) | 0.018 |
| Horner’s syndrome | 701 (0.0) | 306 (48.2) | 27 (40.9) | 0.311 |
| Tinnitus | 700 (0.1) | 62 (9.8) | 11 (16.7) | 0.311 |
| Cranial nerve palsy | 701 (0.0) | 45 (7.1) | 12 (18.2) | 0.195 |
| Amaurosis fugax | 1002 (0.2) | 69 (7.6) | 2 (2.1) | 0.284 |
| Retinal infarction | 1004 (0.0) | 5 (0.5) | 2 (2.1) | 0.311 |
| Transient ischemic attack | 1002 (0.2) | 264 (29.1) | 20 (21.3) | 0.311 |
| Number of transient ischemic attacks | 275 (3.2) | 1.0 (1.0 to 2.0) | 1.0 (1.0 to 1.5) | 0.952 |
| Ischemic stroke | 1004 (0.0) | 483 (53.1) | 26 (27.7) | <0.0001 |
| NIHSS baseline | 500 (1.8) | 5.0 (2.0 to 14.0) | 4.0 (1.0 to 7.0) | 0.417 |
| Early recurrent stroke | 946 (5.8) | 8 (0.9) | 4 (4.5) | 0.126 |
| Late recurrent stroke | 946 (5.8) | 8 (0.9) | 0 (0.0) | 1 |
| Early recurrent TIA | 947 (5.7) | 14 (1.6) | 4 (4.5) | 0.284 |
| Late recurrent TIA | 947 (5.7) | 15 (1.7) | 0 (0.0) | 1 |
| Recurrent dissection | 949 (5.5) | 37 (4.3) | 3 (3.3) | 1 |
| Rankin Scale after 3 months | 401 (21.2) | 1.0 (1.0 to 3.0) | 0.0 (0.0 to 1.0) | 0.018 |
| Death after 3 months | 818 (18.5) | 9 (1.2) | 0 (0.0) | 1 |
| No Dissecting Aneurysm | Dissecting Aneurysm | Multivariate Analysis | ||
|---|---|---|---|---|
| n (%) | n (%) | Odds Ratio (95% CI) | p-Value | |
| Ischemic stroke | 483 (53.1) | 26 (27.7) | 0.36 (0.22–0.57) | <0.0001 |
References
- Völker, W.; Dittrich, R.; Grewe, S.; Nassenstein, I.; Csiba, L.; Herczeg, L.; Borsay, B.A.; Robenek, H.; Kuhlenbäumer, G.; Ringelstein, E.B. The Outer Arterial Wall Layers Are Primarily Affected in Spontaneous Cervical Artery Dissection. Neurology 2011, 76, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Luken, M.G.; Ascherl, G.F.; Correll, J.W.; Hilal, S.K. Spontaneous Dissecting Aneurysms of the Extracranial Internal Carotid Artery. Clin. Neurosurg. 1979, 26, 353–375. [Google Scholar] [CrossRef] [PubMed]
- Benninger, D.H.; Gandjour, J.; Georgiadis, D.; Stöckli, E.; Arnold, M.; Baumgartner, R.W. Benign Long-Term Outcome of Conservatively Treated Cervical Aneurysms Due to Carotid Dissection. Neurology 2007, 69, 486–487. [Google Scholar] [CrossRef] [PubMed]
- Djouhri, H.; Guillon, B.; Brunereau, L.; Lévy, C.; Bousson, V.; Biousse, V.; Arrivé, L.; Tubiana, J.M. MR Angiography for the Long-Term Follow-Up of Dissecting Aneurysms of the Extracranial Internal Carotid Artery. AJR Am. J. Roentgenol. 2000, 174, 1137–1140. [Google Scholar] [CrossRef] [PubMed]
- Daou, B.; Hammer, C.; Chalouhi, N.; Starke, R.M.; Jabbour, P.; Rosenwasser, R.H.; Tjoumakaris, S. Dissecting Pseudoaneurysms: Predictors of Symptom Occurrence, Enlargement, Clinical Outcome, and Treatment. J. Neurosurg. 2016, 125, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Debette, S.; Grond-Ginsbach, C.; Bodenant, M.; Kloss, M.; Engelter, S.; Metso, T.; Pezzini, A.; Brandt, T.; Caso, V.; Touzé, E.; et al. Differential Features of Carotid and Vertebral Artery Dissections: The CADISP Study. Neurology 2011, 77, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; King, A.; Madigan, J.; Levi, C.; Norris, J.W.; Markus, H.S. Prognosis of Carotid Dissecting Aneurysms: Results from CADISS and a Systematic Review. Neurology 2017, 88, 646–652. [Google Scholar] [CrossRef] [PubMed]
- van Laarhoven, C.J.H.C.M.; Arnold, M.; Danilova, M.; Dreval, M.; Ferrari, E.; Goeggel Simonetti, B.; Gralla, J.; Heldner, M.; Kalashnikova, L.; Mancuso, M.; et al. Delayed Development of Aneurysmal Dilatations in Patients with Extracranial Carotid Artery Dissections. Eur. J. Vasc. Endovasc. Surg. 2022, 64, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Guillon, B.; Brunereau, L.; Biousse, V.; Djouhri, H.; Lévy, C.; Bousser, M.G. Long-Term Follow-up of Aneurysms Developed during Extracranial Internal Carotid Artery Dissection. Neurology 1999, 53, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Touzé, E.; Randoux, B.; Méary, E.; Arquizan, C.; Meder, J.F.; Mas, J.L. Aneurysmal Forms of Cervical Artery Dissection: Associated Factors and Outcome. Stroke 2001, 32, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Mokri, B. Traumatic and Spontaneous Extracranial Internal Carotid Artery Dissections. J. Neurol. 1990, 237, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Foreman, P.M.; Griessenauer, C.J.; Falola, M.; Harrigan, M.R. Extracranial Traumatic Aneurysms Due to Blunt Cerebrovascular Injury. J. Neurosurg. 2014, 120, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- von Babo, M.; De Marchis, G.M.; Sarikaya, H.; Stapf, C.; Buffon, F.; Fischer, U.; Heldner, M.R.; Gralla, J.; Jung, S.; Simonetti, B.G.; et al. Differences and Similarities between Spontaneous Dissections of the Internal Carotid Artery and the Vertebral Artery. Stroke 2013, 44, 1537–1542. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.G.; Altman, D.G.; Stavola, B.L.D. Quantification of the Completeness of Follow-Up. Lancet 2002, 359, 1309–1310. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Miyachi, S.; Yoshida, J. Animal Models of Cervical Artery Dissection. In Handbook on Cerebral Artery Dissection; Karger Publishers: Basel, Switzerland, 2005; Volume 20, pp. 1–11. [Google Scholar] [CrossRef]
- Sturzenegger, M.; Huber, P. Cranial Nerve Palsies in Spontaneous Carotid Artery Dissection. J. Neurol. Neurosurg. Psychiatry 1993, 56, 1191–1199. [Google Scholar] [CrossRef]
- Wessels, T.; Röttger, C.; Kaps, M.; Traupe, H.; Stolz, E. Upper Cranial Nerve Palsy Resulting from Spontaneous Carotid Dissection. J. Neurol. 2005, 252, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, J.; Newell, D.W.; Sturzenegger, M.; Mayberg, M.R.; Winn, H.R. Transcranial Doppler in the Evaluation of Internal Carotid Artery Dissection. Stroke 1996, 27, 1226–1230. [Google Scholar] [CrossRef]
- Pelkonen, O.; Tikkakoski, T.; Leinonen, S.; Pyhtinen, J.; Lepojärvi, M.; Sotaniemi, K. Extracranial Internal Carotid and Vertebral Artery Dissections: Angiographic Spectrum, Course and Prognosis. Neuroradiology 2003, 45, 71–77. [Google Scholar] [CrossRef]
- Debette, S.; Leys, D. Cervical-Artery Dissections: Predisposing Factors, Diagnosis, and Outcome. Lancet Neurol. 2009, 8, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Wessels, T.; Mosso, M.; Krings, T.; Klötzsch, C.; Harrer, J.U. Extracranial and Intracranial Vertebral Artery Dissection: Long-Term Clinical and Duplex Sonographic Follow-Up. J. Clin. Ultrasound 2008, 36, 472–479. [Google Scholar] [CrossRef]
- Paciaroni, M.; Caso, V.; Agnelli, G. Magnetic Resonance Imaging, Magnetic Resonance and Catheter Angiography for Diagnosis of Cervical Artery Dissection. In Handbook on Cerebral Artery Dissection; Karger Publishers: Basel, Switzerland, 2005; Volume 20, pp. 102–118. [Google Scholar] [CrossRef]
- Leclerc, X.; Lucas, C.; Godefroy, O.; Tessa, H.; Martinat, P.; Leys, D.; Pruvo, J.P. Helical CT for the Follow-up of Cervical Internal Carotid Artery Dissections. AJNR Am. J. Neuroradiol. 1998, 19, 831–837. [Google Scholar] [PubMed]
- Heldner, M.R.; Nedelcheva, M.; Yan, X.; Slotboom, J.; Mathier, E.; Hulliger, J.; Verma, R.K.; Sturzenegger, M.; Jung, S.; Bernasconi, C.; et al. Dynamic Changes of Intramural Hematoma in Patients with Acute Spontaneous Internal Carotid Artery Dissection. Int. J. Stroke 2015, 10, 887–892. [Google Scholar] [CrossRef] [PubMed]




| Number of Patients Included in Analysis | No Dissecting Aneurysm | Dissecting Aneurysm | |
|---|---|---|---|
| n (% Missing Data) | n (%) | n (%) | |
| Hospital | 1012 (0.0) | ||
| Zurich | 131 (15.2) | 17 (11.3) | |
| Bern | 315 (36.6) | 21 (13.9) | |
| Paris | 415 (48.2) | 113 (74.8) | |
| Number of dissections | 1012 (0.0) | ||
| 1 | 728 (84.6) | 105 (69.5) | |
| 2 | 116 (13.5) | 31 (20.5) | |
| 3 | 15 (1.7) | 9 (6.0) | |
| 4 | 2 (0.2) | 6 (4.0) | |
| Number of aneurysms | 1012 (0.0) | ||
| 1 | 0 (0.0) | 136 (90.1) | |
| 2 | 0 (0.0) | 14 (9.3) | |
| 3 | 0 (0.0) | 1 (0.7) | |
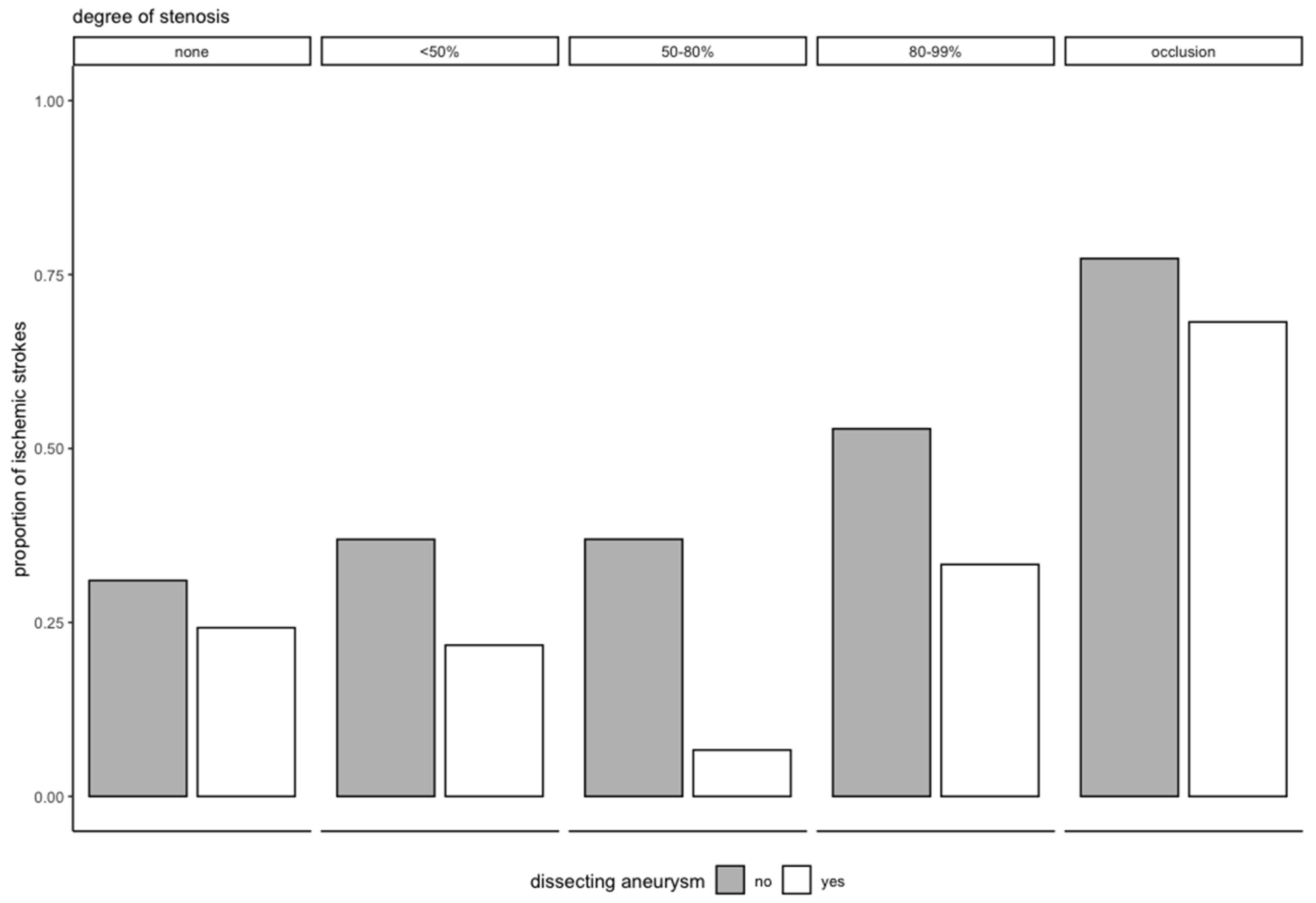
| Degree of stenosis | 858 (15.2) | ||
| None | 58 (8.0) | 33 (25.0) | |
| <50% | 111 (15.3) | 23 (17.4) | |
| 50–80% | 46 (6.3) | 15 (11.4) | |
| 80–99% | 229 (31.5) | 39 (29.5) | |
| Occlusion | 282 (38.8) | 22 (16.7) |
| Number of Patients Included in Analysis | No Dissecting Aneurysm | Dissecting Aneurysm | Univariate Analysis | |
|---|---|---|---|---|
| n (% Missing Data) | Median (IQR)/ n (%) | Median (IQR)/ n (%) | p-Value | |
| Age | 1012 (0.0) | 45.0 (38.0 to 52.0) | 46.0 (38.5 to 52.0) | 0.77 |
| Female sex | 1012 (0.0) | 373 (43.3) | 78 (51.7) | 0.368 |
| Days to diagnosis | 1012 (0.0) | 5.0 (2.0 to 12.0) | 7.0 (3.0 to 14.5) | 0.143 |
| Vessel affected | 1012 (0.0) | 0.701 * | ||
| ICA | 551 (64.0) | 87 (57.6) | ||
| VA | 268 (31.1) | 38 (25.2) | ||
| ICA + VA | 42 (4.9) | 26 (17.2) | ||
| Multiple dissections | 1012 (0) | 134 (15.6) | 46 (30.5) | 0.441 * |
| Fever and infection | 927 (8.4) | 85 (10.8) | 9 (6.3) | 0.417 |
| Minor trauma | 1009 (0.3) | 190 (22.1) | 38 (25.5) | 0.626 |
| Connective tissue disease | 1006 (0.6) | 0.484 | ||
| Family history | 15 (1.8) | 2 (1.3) | ||
| Diagnosed | 15 (1.8) | 6 (4.0) | ||
| Family history of ischemic stroke | 994 (1.8) | 121 (14.3) | 16 (10.7) | 0.569 |
| Smoking | 1003 (0.9) | 0.731 | ||
| Former | 117 (13.7) | 24 (16.1) | ||
| Current | 242 (28.3) | 38 (25.5) | ||
| Arterial hypertension | 1011 (0.1) | 188 (21.9) | 38 (25.2) | 0.626 |
| Hypercholesterolemia | 849 (16.1) | 390 (53.8) | 62 (50.0) | 0.668 |
| Migraine | 979 (3.3) | 0.668 | ||
| Without aura | 159 (19.1) | 30 (20.3) | ||
| With aura | 82 (9.9) | 19 (12.8) | ||
| Diabetes mellitus | 1011 (0.1) | 18 (2.1) | 4 (2.6) | 0.701 |
| Hormonal anticonception | 435 (3.5) | 115 (31.9) | 16 (21.3) | 0.387 |
| Local symptoms | 1012 (0.0) | 773 (89.8) | 138 (91.4) | 0.731 |
| Ischemic symptoms | 1012 (0.0) | 621 (72.1) | 70 (46.4) | <0.0001 |
| Headache | 1010 (0.2) | 614 (71.5) | 111 (73.5) | 0.751 |
| VAS headache | 447 (38.3) | 7.0 (5.0 to 8.0) | 7.0 (6.0 to 9.0) | 0.626 |
| Thunderclap headache | 900 (11.1) | 48 (6.3) | 13 (9.8) | 0.417 |
| Cervical pain | 1009 (0.3) | 391 (45.5) | 72 (48.0) | 0.731 |
| VAS cervical pain | 249 (46.2) | 6.0 (5.0 to 8.0) | 6.5 (5.0 to 8.0) | 0.491 |
| Radiculopathy | 1004 (0.8) | 4 (0.5) | 1 (0.7) | 0.701 |
| Spinal infarction | 1012 (0.0) | 1 (0.1) | 0 (0.0) | 1 |
| Subarachnoid hemorrhage | 1010 (0.2) | 13 (1.5) | 7 (4.6) | 0.143 |
| Horner’s syndrome in carotid dissection | 706 (0.0) | 280 (47.2) | 54 (47.8) | 1 |
| Tinnitus | 1010 (0.2) | 63 (7.3) | 18 (11.9) | 0.373 |
| Cranial nerve palsy | 1012 (0.0) | 66 (7.7) | 15 (9.9) | 0.626 |
| Amaurosis fugax | 1010 (0.2) | 64 (7.5) | 7 (4.6) | 0.565 |
| Retinal infarction | 1012 (0.0) | 5 (0.6) | 2 (1.3) | 0.565 |
| Transient ischemic attack | 1010 (0.2) | 250 (29.1) | 34 (22.7) | 0.417 |
| Number of transient ischemic attacks | 275 (3.2) | 1.0 (1.0 to 2.0) | 1.0 (1.0 to 1.0) | 0.626 |
| Ischemic stroke | 1012 (0.0) | 468 (54.4) | 44 (29.1) | <0.0001 |
| NIHSS baseline | 503 (1.8) | 5.0 (2.0 to 14.0) | 4.0 (1.0 to 11.0) | 0.417 |
| Early recurrent stroke | 954 (5.7) | 8 (1.0) | 5 (3.4) | 0.209 |
| Late recurrent stroke | 954 (5.7) | 6 (0.7) | 2 (1.4) | 0.484 |
| Early recurrent TIA | 955 (5.6) | 13 (1.6) | 5 (3.4) | 0.46 |
| Late recurrent TIA | 955 (5.6) | 16 (2.0) | 0 (0.0) | 1 |
| Recurrent dissection | 957 (5.4) | 35 (4.3) | 7 (4.8) | 0.626 |
| Rankin Scale after 3 months | 403 (21.3) | 1.0 (1.0 to 3.0) | 0.0 (0.0 to 1.0) | 0.007 |
| Favorable Rankin Scale after 3 months | 403 (21.3) | 200 (54.5) | 29 (80.6) | 0.048 |
| death after 3 months | 825 (18.5) | 9 (1.3) | 0 (0.0) | 0.633 |
| No Dissecting Aneurysm | Dissecting Aneurysm | Multivariate Analysis | ||
|---|---|---|---|---|
| n (%) | n (%) | Odds Ratio (95% CI) | p-Value | |
| Ischemic stroke | 468 (54.4) | 44 (29.1) | 0.41 (0.28–0.60) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinsiepe, V.K.; Sarikaya, H.; Mordasini, P.R.; Wegener, S.; Inauen, C.; Baumgartner, P.; Jung, S.; Antonenko, K.; Fischer, U.; Gralla, J.; et al. Comparison of Aneurysmal and Non-Aneurysmal Spontaneous Cervical Artery Dissections in a Large Multicenter Cohort. Clin. Transl. Neurosci. 2024, 8, 18. https://doi.org/10.3390/ctn8020018
Steinsiepe VK, Sarikaya H, Mordasini PR, Wegener S, Inauen C, Baumgartner P, Jung S, Antonenko K, Fischer U, Gralla J, et al. Comparison of Aneurysmal and Non-Aneurysmal Spontaneous Cervical Artery Dissections in a Large Multicenter Cohort. Clinical and Translational Neuroscience. 2024; 8(2):18. https://doi.org/10.3390/ctn8020018
Chicago/Turabian StyleSteinsiepe, Valentin K., Hakan Sarikaya, Pasquale R. Mordasini, Susanne Wegener, Corinne Inauen, Philipp Baumgartner, Simon Jung, Kateryna Antonenko, Urs Fischer, Jan Gralla, and et al. 2024. "Comparison of Aneurysmal and Non-Aneurysmal Spontaneous Cervical Artery Dissections in a Large Multicenter Cohort" Clinical and Translational Neuroscience 8, no. 2: 18. https://doi.org/10.3390/ctn8020018