Abstract
Objective: To characterize the difference in uptake of virtual care for urinary tract infections (UTIs) by demographic variables in the COVID-19 era. Methods: We conducted a retrospective review of outpatient encounters for UTIs across a large health care system. The cohort was defined as patients with an encounter diagnosis of UTI via in-person or virtual care (telephone or technology-supported care), between March 1, 2020, and February 28, 2021. Analysis was limited to the first UTI encounter of the year for each patient. We compared the use of in-person and virtual visits by demographic variables using chi-square tests and multivariate logistic regression. Results: A total of 6744 patients, with a mean age of 61 years, were seen for UTI during the study period. The majority of patients were White (85.5%) and female (83.7%), and were seen in person (55.9%). Of those seen virtually, 52.0% participated in telephone-only visits, and 47.9% were seen via technology-supported care, using video or chat-based platforms. On multivariate logistic regression, age under 30, lowest-quartile income, male sex, and a primary language other than English increased the odds that patients had been seen in person. Among those seen virtually, age over 50 significantly increased the odds of a telephone visit, as did being Black or Native American, having a lower-quartile income, and speaking a non-English primary language. Conclusions: Although the expansion in virtual care has given some patients easier access to necessary care, the “digital divide” has worsened existing disparities for certain vulnerable populations. We demonstrate a difference in uptake of virtual health care by age, race, primary language, and income.
1. Introduction
The COVID-19 pandemic forced a rapid expansion in virtual medical care[1,2]. Although this transition has facilitated the provision of care for some patients, other vulnerable populations may have not been afforded the same access: prior studies have demonstrated less uptake of virtual visits among patients who are older or Black, and patients with Medicaid/Medicare coverage[3].
Telemedicine has distinct advantages: virtual visits obviate the need for travel and its associated costs and decrease the risk of exposure to pathogens such as COVID-19. When telemedicine works well it can provide efficient, convenient access to medical professionals and can even prevent unnecessary emergency department visits[4].The downsides of telemedicine include limitations in physical examination and testing, and the requirement for technology, with its associated costs and learning curve. Virtual care can be difficult or impossible for the 25% of American adults who do not have broadband internet at home, the 20% who do not have access to a smartphone, or those who require an interpreter[5].
Urinary tract infections (UTIs) are common, accounting for 7 million medical visits per year in the United States, and cost roughly $1.6 billion dollars annually[6]. Patients of all gender and racial identity groups, and of all ages and socioeconomic levels get UTIs, and are treated by providers from a range of specialties. Many uncomplicated UTIs can be safely managed on virtual platforms, as physical examination is relatively unnecessary, and urine testing is optional[7,8,9]. These factors make UTI an ideal candidate for examining the dynamics of virtual care in the wake of the COVID-19 pandemic.
The increase in use of telemedicine that has occurred since the onset of COVID-19 pandemic comes with an opportunity to improve access for patients. Which patients have benefited from this expansion in care and who has been left behind? We aim to evaluate the impact of patient demographics on the utilization of virtual care for the management of UTIs. Our secondary aim is to characterize the demographics of those using different strata of virtual care, namely telephone versus technology-supported care (TSC) visits, defined as video or chat-based platforms.
2. Methods
Setting and data
M Health Fairview is a large health care system with 10 hospitals, as well as an academic quaternary care center and 60 primary care clinics serving urban, suburban, and rural Minnesotans. Electronic health records were aggregated by the University of Minnesota’s centralized informatics center and de-identified before analysis. Patients were included in this study if they consented to inclusion in research studies upon establishing care with M Health Fairview. This study was approved by the M Health Fairview hospitals and the University of Minnesota institutional review board.
We defined our cohort as any patient with an ICD-10 code diagnosis of UTI (codes N10, N11, N30, N39, N99) in an ambulatory setting between March 1, 2020, and February 28, 2021. The time period was chosen to coincide with the first year of the COVID-19 pandemic in Minnesota (the first documented COVID-19 case in Minnesota was on March 6, 2020). This was a period of rapid transition to virtual care for all patients, including those seen in urgent care and outpatient clinics across numerous specialties, in primary care as well as specialty care clinics such as urology. UTIs diagnosed during emergency room visits or hospital admissions were excluded. Data regarding encounter type included in-person office visits and virtual/telehealth encounters: telephone, video visits, and text-based chat visits via OnCare, a chat-based platform for virtual care. Patients log in from a computer or smartphone and text with a clinician. The case is reviewed, and the provider responds via text or email with a diagnosis and treatment plan within an hour. Similar platforms have been developed across other health systems in response to COVID-19 and have demonstrated the ability to provide convenient, cost-effective, and timely care for a range of conditions without need for an in-person visit[10].
Patient demographic variables documented include age, race, and zip code of residence. Patients younger than 18 years and without zip code information were excluded, as were those who lived out of state. Median household income was assigned based on zip code using United States Census Integrated Public Use Microdata Series[11]. Median household income was divided into quartiles and analyzed as a categorical variable.
Encounter type (in-person versus virtual and telephone versus TSC) was our primary outcome measure. Univariate analysis was conducted using chi-square tests. Multivariate logistic regression was used to identify the impact of clinically significant demographic variables on encounter type.
3. Results
Of the 6744 visits for UTI, 3773 visits (55.9%) were conducted in person, and the remainder on one of the virtual platforms. The majority of patients were White (85.9%) and female (83.7%). The average age at the time of encounter was 59 years, and over a third of patients were 70 or older (Table 1).

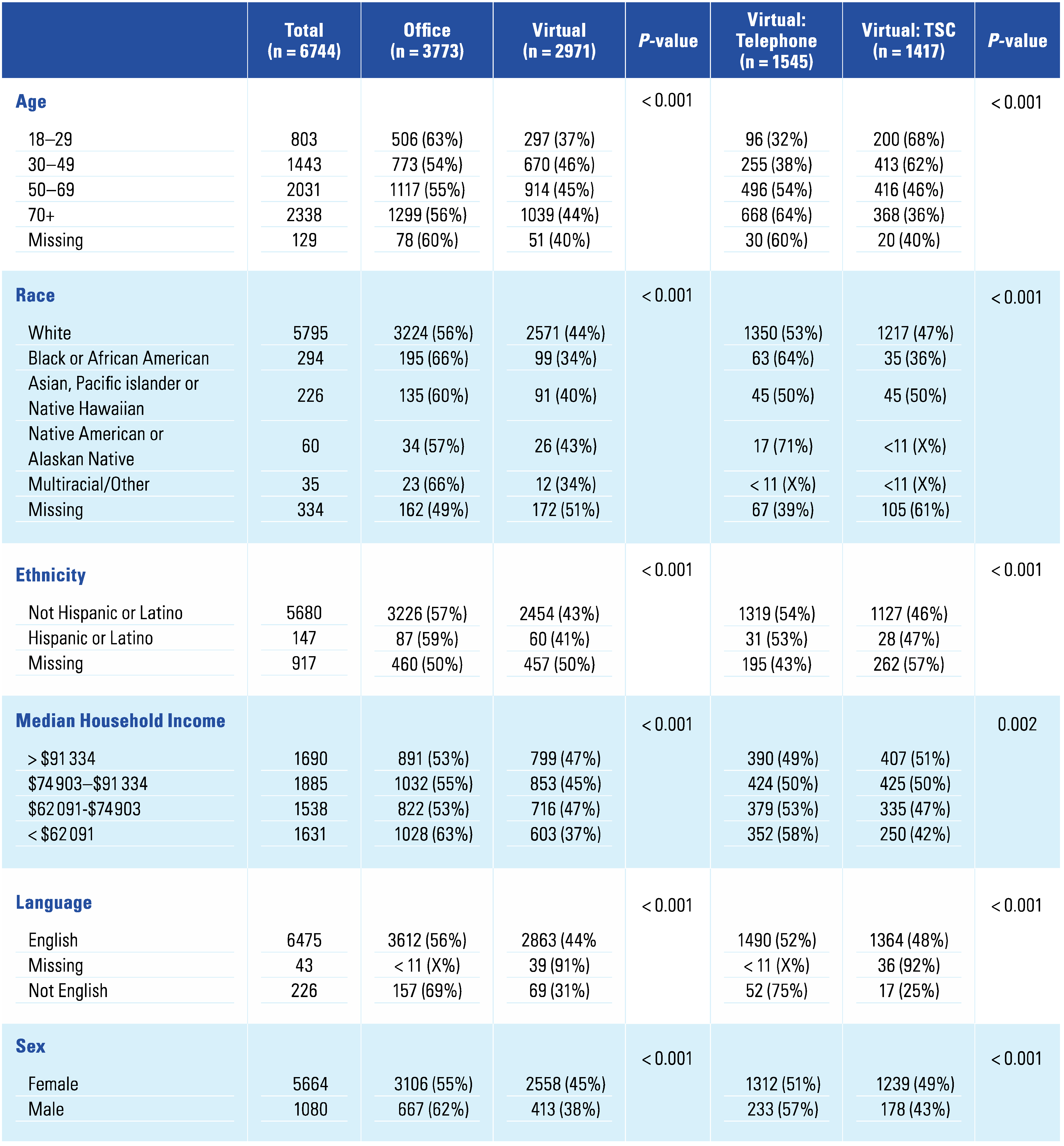
Table 1.
Demographic variables by encounter type patient demographics.
3.1. Office visit versus virtual visit
Patients < 30 years old were more likely than other age groups to be seen in person (63% of < 30-year-olds seen in-person versus 54% for 30 to 49 years, 55% for 50 to 69 years, and 56% for those over 70 years, P < 0.001). Black or African American patients were more likely to be seen in person (66.3% of Black patients seen in person versus 55.6% of White patients and 59.7% of Asian American or Pacific Islander patients, P < 0.001). Patients in the lowest income quartile were seen in person more often than patients in higher income categories. Patients who listed a language other than English as their primary language were also significantly more likely to attend an in-person visit (69.5% of non-English primary versus 55.8% of English primary language, P < 0.001). A larger proportion of men than women attended in-person visits (62% versus 55%, P < 0.001) (Table 1).
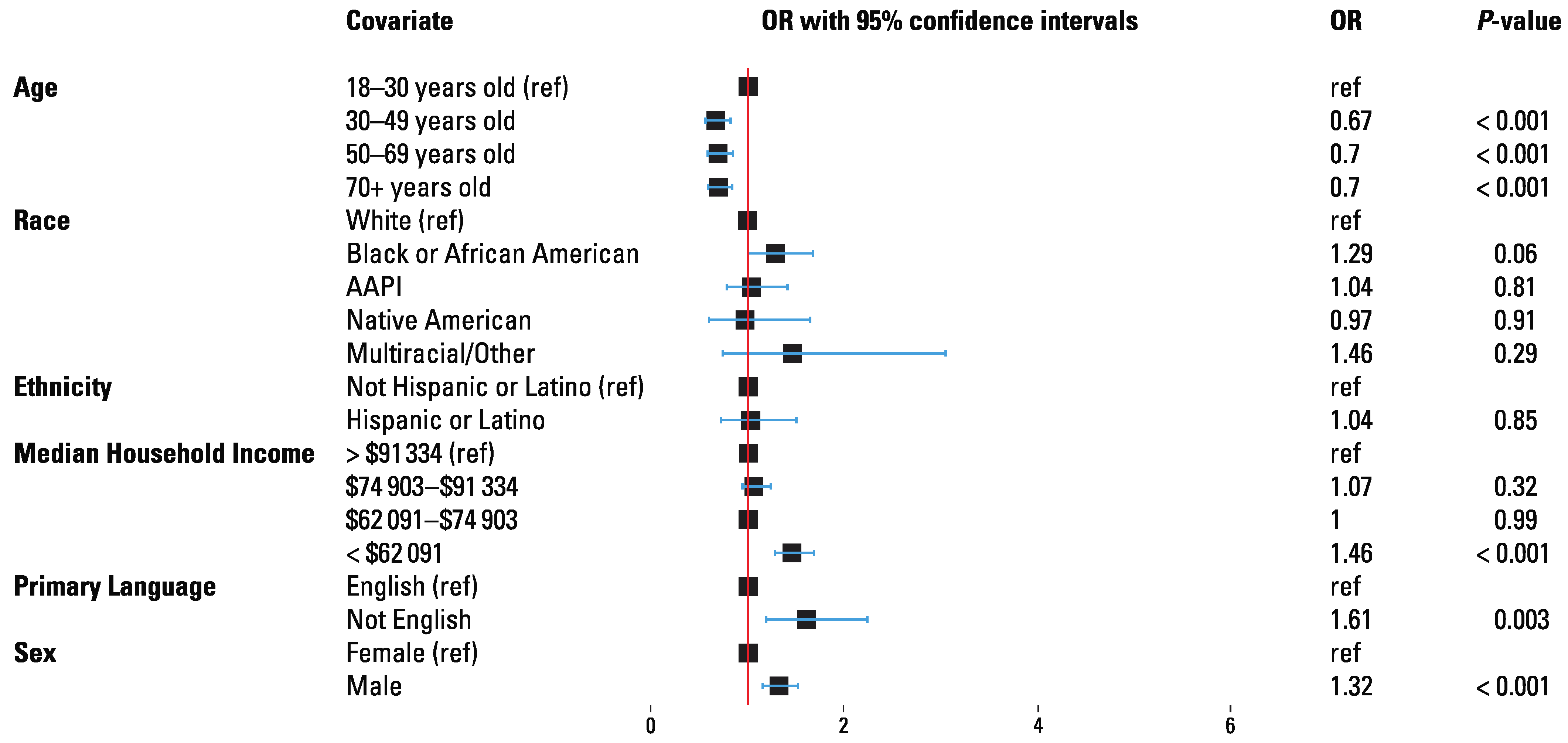
On multivariate logistic regression, age over 30 decreased the odds of being seen in person (OR 0.67 to 0.70, P < 0.01). Lowest income quartile (OR 1.46, P < 0.001), primary language other than English (OR 1.61, P = 0.003), and male sex (OR 1.32, P < 0.001) increased the odds of being seen in person (Figure 1).
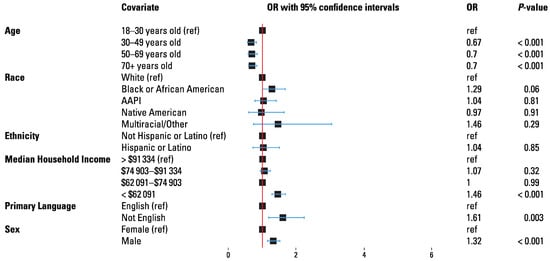
Figure 1.
Multivariate logistic regression analysis describing odds of in person visit as compared with virtual visit.
3.2. Virtual visits: telephone versus TSC
Of the virtual encounters, 52.0% were telephone-only visits, and 47.7% were conducted via TSC, defined as video or chat-based platforms; 9 (< 1%) did not fit into any of the virtual encounter type categories. The majority (68%) of virtual visit patients under the age of 30 used TSC as opposed to telephone-only care. Patients over the age 70 were twice as likely to participate in a telephone-only visit as in a TSC visit (64.3% versus 35.4%, P < 0.001). Black and Native American patients participating in virtual visits were far more likely to have telephone-only visits than any other race group. Patients whose primary language was not English were significantly more likely to have a telephone visit than were native English speakers (75.4% versus 52.0%, P < 0.001). Men were slightly more likely than women to have telephone-only visits (57% versus 51%, P = 0.048) (Table 1).
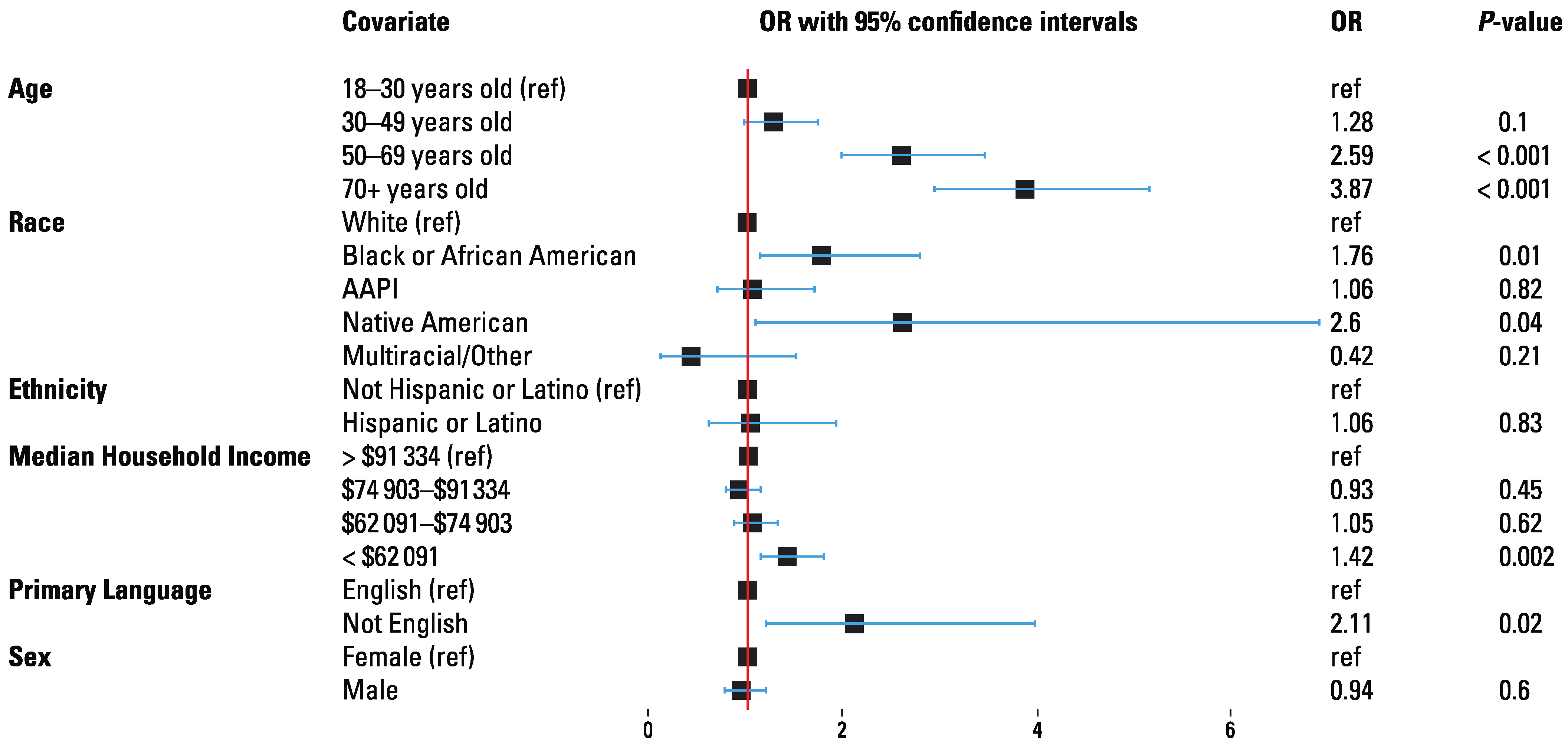
On multivariate logistic regression, age > 50 (age 50 to 69 OR 2.59, P < 0.001 and age > 70 OR 3.9, P < 0.001), being Black (OR 1.8, P = 0.014) or Native American/Alaskan Native (OR 2.6, P = 0.04), income < $62 091 (OR 1.42, P = 0.002), and primary language other than English (OR 2.1, P = 0.016) increased the odds of having a telephone rather than a TSC visit (Figure 2). Sex did not demonstrate a significant effect.
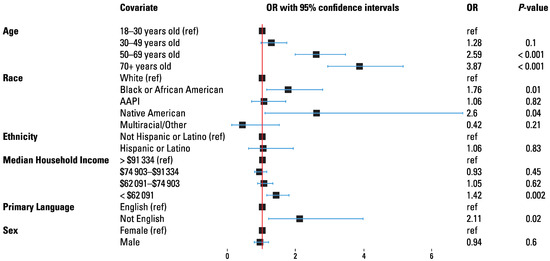
Figure 2.
Multivariate logistic regression analysis describing odds of telephone visit as compared with TSC.
4. Discussion
The rapid expansion in virtual care since the start of the COVID-19 pandemic has been profound[2] and likely permanent. Unfortunately, not all patients have benefited from this increased access to medical professionals. We demonstrate disparities in access to virtual care among a number of traditionally marginalized and vulnerable populations, including patients who are Black, those with low income, those for whom English is not the primary language, and patients over 70 years. The discrepancies in uptake of virtual, and specifically, TSC visits, identified here largely parallel known disparities in all fields of medical care. The etiology of these differences is multifactorial, with likely contributing factors including systemic racism, concerns about COVID-19 infection, availability of interpreters, as well as access to and comprehension of required technology. As has been obvious since the beginning of the pandemic, this virus has amplified health care disparities among the most vulnerable[12,13].
We found that those who were Black were less likely to use virtual care and, within the category of virtual care, had lower use of TSC than telephone visits. In a study of over 100 000 virtual visits between March and August of 2020, Luo et al. found that White and higher income patients were more likely to use video platforms, while Black and lower income patients were more likely to have telephone-only encounters[14]. Our findings parallel these observations. Similar studies conducted prior to the COVID-19 pandemic warned of this digital divide. One study by Mitchell et al. demonstrated significantly less use of technology for health-related purposes among Black patients after accounting for other demographic characteristics, education, and health conditions[15]. Availability of reliable broadband internet and digital literacy are generally lower in minority and low-income populations, making access to virtual care more difficult[16]. Medical mistrust and concern about privacy may also contribute to lower rates of virtual care use among some populations[15].
Patients over 70 in our study were less likely to access virtual care and less likely to use video, as has been observed previously[15,17]. Older age is associated with slower rates of technology adoption, lower technologic literacy, and lower use of digital health technology, although this use is increasing[17]. In addition, age-related decreases in visual acuity and fine motor skills can make virtual visits less accessible to older adults[16,18].
Our finding that women were more likely to use virtual visits than men is consistent with prior studies[15,19]. Some authors have postulated that higher uptake of virtual care among women is related to the increase in domestic burdens on women as result of the COVID-19 pandemic[19] or due to lower concern about COVID-19 infection among men[17]. Interestingly, higher uptake of virtual care was noted among women prior to the COVID-19 pandemic. This shift may be attributed to convenience, as women are thought to be more likely to be “juggling work, childcare, and other responsibilities”[20]. Specific to this study, men by definition have “complicated” UTIs, which may be more amenable to in-person care because of the higher risk of anatomic abnormalities and need for urine culture.
Patients who reported a primary language other than English were less likely to use virtual care, and less likely to use video visits. Difficulties with telemedicine for those with limited English proficiency have been well documented, from challenges of navigating patient portals to coordinating interpreter assistance[21,22]. Despite improved quality of interpreter-assisted virtual care when video is available[23], only 20% of telemedicine patients whose first language was not English had a video visit in our study.
But are telephone visits inferior to video visits? One systematic review attempting to answer this question suggests that physicians made fewer medical errors and had greater diagnostic accuracy on video compared with audio-only visits[24]. In this study we compare access to telephone-only to TSC visits, which includes video and chat-based visits.
Although it seems likely that virtual care will continue in some capacity in the post-pandemic world, the future of telephone-only visits remains less certain. The passage of the Coronavirus Aid, Relief, and Economic Security (CARES) Act in the United States allowed the Centers for Medicare Services to reimburse providers for telemedicine visits during the public health emergency, including coverage of audio-only visits in some circumstances. If all payers do not make this change permanent, it is likely that vulnerable populations will lose access to virtual care[25]. Virtual care has the potential to improve outcomes for underserved communities but in the United States, this requires systemic change with federal support[26]. Broadband internet access— and the access to credible medical information and full use of telehealth that it affords—has been identified as an important social determinant of health[27]. Expansions in access to broadband internet, use of cloud-based video conferencing platforms with lower bandwidth requirements, and public education on the availability of virtual care are possible interventions to reduce the digital divide[28].
This study demonstrates disparities in access to telemedicine by race, income, age, sex, and primary language, indicating a need for additional infrastructure to support this technology boom. Though the rise in virtual care has been advantageous for some, these hastily constructed systems are allowing our most vulnerable patients to fall through the cracks.
As with any retrospective review, this study is limited by the possibility of unmeasured confounding variables. Because our focus was on the effect of demographic variables on encounter type, we did not include clinical variables in our analysis; the complexity of the UTI or the patient’s comorbidities may push a patient or provider to prefer an office visit over virtual care. Race and ethnicity information were missing for a portion of the patients in this cohort. To reduce the risk of bias we included these patients in the final analysis. Other factors that may have had an impact on type of visit, including insurance status, distance from care, and patient preference, were not included. This study does not include long-term follow-up data to assess adequacy of virtual UTI management.
This is the first study to our knowledge that characterizes the demographic profile of patients seen for UTI by encounter type in the COVID-19 era. Limitations are mitigated by the large sample size with over 6000 unique patients examined.
5. Conclusion
In this study of over 6000 patients seen for UTI between March 2020 and 2021, we demonstrate that many of the commonly seen demographic predictors of reduced access to medical care also predict for lower use of virtual care and, specifically, technology-supported virtual care (versus telephone care). These include being over 70, being Black, and having a primary language other than English.
Acknowledgments
IRB Approval: study approved by University of Minnesota Institutional Review Board, study number STUDY00012449.
Competing Interests
MDF: none. JAA: none. STG: none. LH: none. SB: none. SPE: consultant and speaker for Boston Scientific, PI of clinical trial and consultant for Urotronic, investment interest for Percuvision.
Author Contributions
MDF, JA, STG, and SPE contributed to the design and implementation of the research, STG to the analysis of the results. LH and SB contributed to the writing of the manuscript. SPE conceived the original and supervised the project.
References
- Bhatia, R.S.; Chu, C.; Pang, A.; et al. Virtual care use before and during the COVID-19 pandemic: a repeated cross-sectional study. CMAJ Open 2021, 9, E107–E114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc 2020, 27, 1132–1135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pierce, R.P.; Stevermer, J.J. Disparities in use of telehealth at the onset of the COVID-19 public health emergency. J Telemed Telecare 2023, 29, 3–9. [Google Scholar] [CrossRef]
- Shah, M.N.; Wasserman, E.B.; Wang, H.; Gillespie, S.M.; Noyes, K.; Wood, N.E.; et al. High-intensity telemedicine decreases emergency department use by senior living community residents. Telemed J E Health 2016, 22, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Katzow, M.W.; Steinway, C.; Jan, S. Telemedicine and health disparities during COVID-19. Pediatrics 2020, 146, e20201586. [Google Scholar] [CrossRef]
- Medina, M.; Castillo-Pino, E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol 2019, 11, 1756287219832172. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.A.; Penza, K.S.; Myers, J.F.; Furst, J.W.; Pecina, J.L. Comparison of evisit management of urinary symptoms and urnary tract infections with standard care. Telemed J E Health 2020, 26, 639–644. [Google Scholar] [CrossRef]
- Novara, G.; Checcucci, E.; Crestani, A.; Abrate, A.; Esperto, F.; Pavan, N.; et al. Telehealth in urology: a systematic review of the literature. how much can telemedicine be useful during and after the COVID-19 pandemic? Eur Urol 2020, 78, 786–811. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.L.; Balk, E.M.; Crisp, C.C.; Antosh, D.D.; Murphy, M.; Halder, G.E.; et al. A guide for urogynecologic patient care utilizing telemedicine during the COVID-19 pandemic: review of existing evidence. Int Urogynecol J 2020, 31, 1063–1089. [Google Scholar] [CrossRef]
- Melmed, S. Chat with a doctor: using asynchronous virtual care access for on-demand physician advice iproc. 2017, 3, e18. [Google Scholar] [CrossRef]
- U.S. Census Bureau. Zip code median income, 2015-2019 American Community Survey 5-year estimates. 2019. [Google Scholar]
- Kirksey, L.; Tucker, D.L.; Taylor, E., Jr.; Solaru, K.T.W.; Modlin, C.S., Jr. Pandemic superimposed on epidemic; COVID-19 disparities in Black Americans. J Natl Med Assoc 2021, 113, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Javier-DesLoges, J.; Meagher, M.; Soliman, S.; Yuan, J.; Hakimi, K.; Ghali, F.; et al. Disparities in telemedicine utilization for urology patients during the COVID-19 pandemic. Urology 2022, 163, 76–80. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luo, J.; Tong, L.; Crotty, B.H.; Somai, M.; Taylor, B.; Osinski, K.; et al. Telemedicine adoption during the COVID-19 pandemic: gaps and inequalities. Appl Clin Inform 2021, 12, 836–844. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mitchell, U.A.; Chebli, P.G.; Ruggiero, L.; Muramatsu, N. The digital divide in health-related technology use: the significance of race/ethnicity. Gerontologist 2019, 59, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Mamedova, S.; Pawlowski, E. A description of U.S. adults who are not digitally literate. U.S. Department of Education. 2018:33. https://nces.ed.gov/pubs2018/2018161.pdf.
- Eberly, L.A.; Kallan, M.J.; Julien, H.M.; Haynes, N.; Khatana, S.A.M.; Nathn, A.S.; et al. Patient characteristics associated with telemedicine access for primary and specialty ambulatory care during the COVID-19 pandemic. JAMA Netw Open 2020, 3, e2031640. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.M.; Lipsitz, S.R.; Linder, J.A. Trends in seniors’ use of digital health technology in the United States, 2011-2014. JAMA 2016, 316, 538–540. [Google Scholar] [CrossRef]
- Lattimore, CM.; Kane, WJ.; Fleming, M.A., 2nd; Martin, A.N.; Mehaffey, J.H.; Smolkin, M.E.; et al. Disparities in telemedicine utilization among surgical patients during COVID-19. PLoS One 2021, 16, e0258452. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Polinski, J.M.; Barker, T.; Gagliano, N.; Sussman, A.; Brennan, T.A.; Shrank, W.H. Patients’ satisfaction with and preference for telehealth visits. J Gen Intern Med 2016, 31, 269–275. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tan-McGrory, A.; Schwamm, L.H.; Kirwan, C.; Betancourt, J.R.; Barreto, E.A. Addressing virtual care disparities for patients with limited English proficiency. Am J Manag Care 2022, 28, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Nouri, S.; Khoong, E.C.; Lyles, C.R.; Karliner, L. Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catalyst 2020. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0123.
- Lion, K.C.; Brown, J.C.; Ebel, B.E.; Klein, E.J.; Strelitz, B.; Gutman, C.K.; et al. Effect of telephone vs video interpretation on parent comprehension, communication, and utilization in the pediatric emergency department: a randomized clinical trial. JAMA Pediatr 2015, 169, 1117–1125. [Google Scholar] [CrossRef]
- Rush, K.L.; Howlett, L.; Munro, A.; Burton, L. Videoconference compared to telephone in healthcare delivery: a systematic review. Int J Med Inform 2018, 118, 44–53. [Google Scholar] [CrossRef]
- Anderson, K.E.; McGinty, E.E.; Presskreischer, R.; Barry, C.L. Reports of forgone medical care among US adults during the initial phase of the COVID-19 pandemic. JAMA Netw Open 2021, 4, e2034882. [Google Scholar] [CrossRef]
- Agate, S. Unlocking the power of telehealth: increasing access and services in underserved, urban areas. Harvard Kennedy School Journal of Hispanic Policy 2017, 29, 85–96. Available online: https://hjhp.hkspublications.org/wp-content/uploads/sites/15/2019/03/HJHP-_-Volume-29-_-2017.pdf (accessed on 6 March 2022).
- Benda, N.C.; Veinot, T.C.; Sieck, C.J.; Ancker, J.S. Broadband internet access is a social determinant of health! Am J Public Health 2020, 110, 1123–1125. [Google Scholar] [CrossRef]
- Barbosa, W.; Zhou, K.; Waddell, E.; Myers, T.; Dorsey, E.R. Improving access to care: telemedicine across medical domains. Annu Rev Public Health 2021, 42, 463–481. [Google Scholar] [CrossRef]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.