
Wedge Resection and Optimal Solutions for Invasive Pulmonary Fungal Infection and Long COVID Syndrome—A Case Report and Brief Literature Review

 ,
,  , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Detailed Case Description
2.1. Clinical Findings
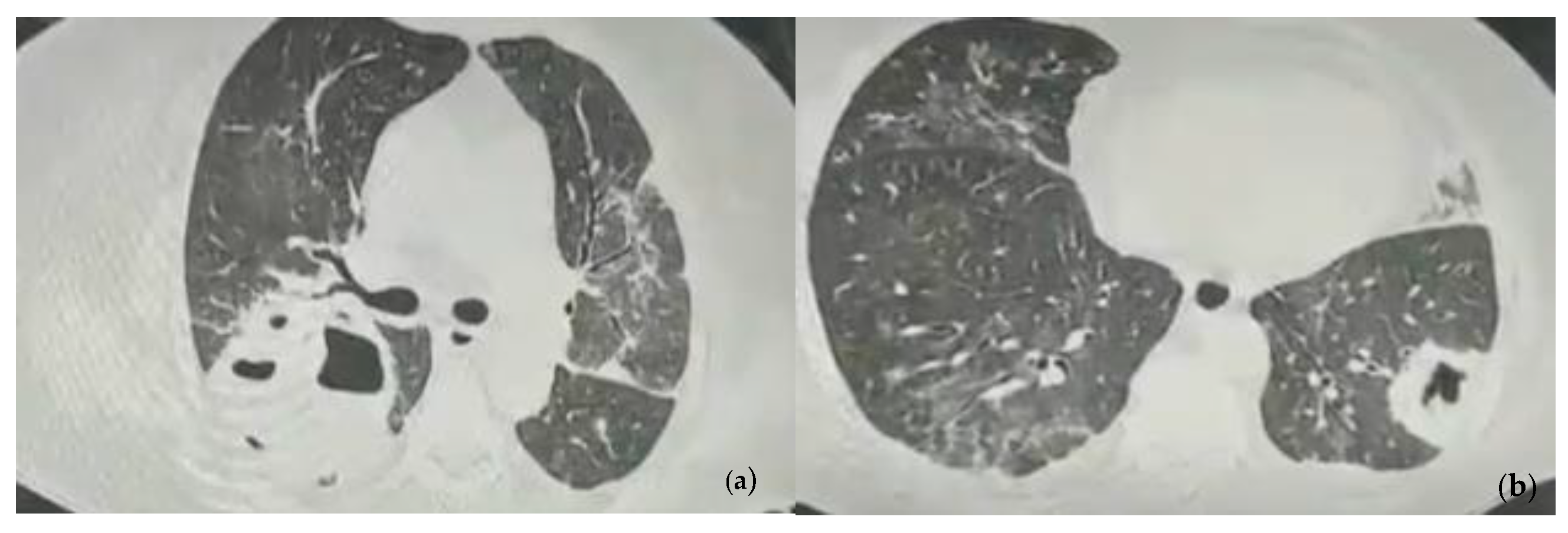
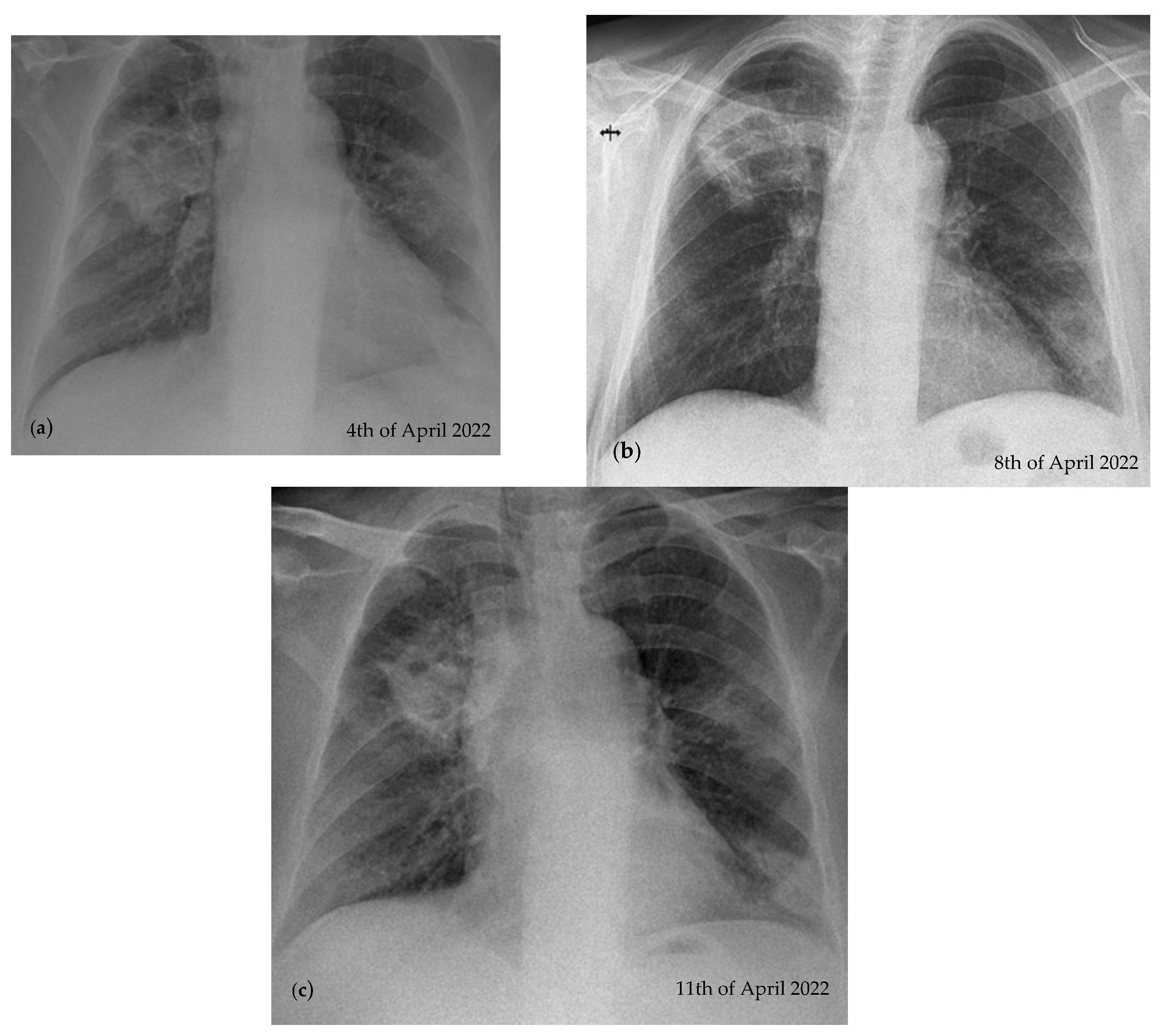
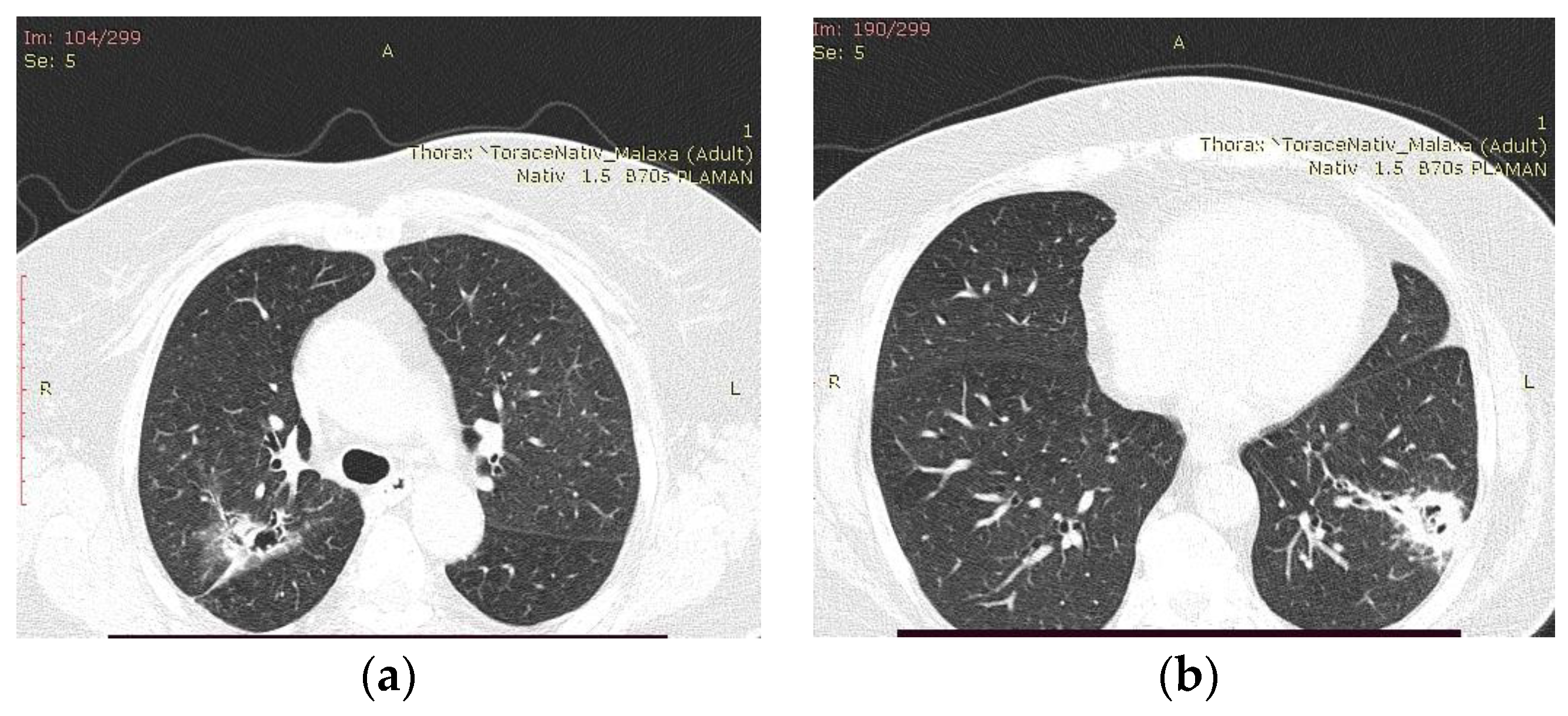
2.2. Blood Workup, Functional Tests, Bronchoscopy, and Radiological Findings
2.3. Treatment and Monitoring
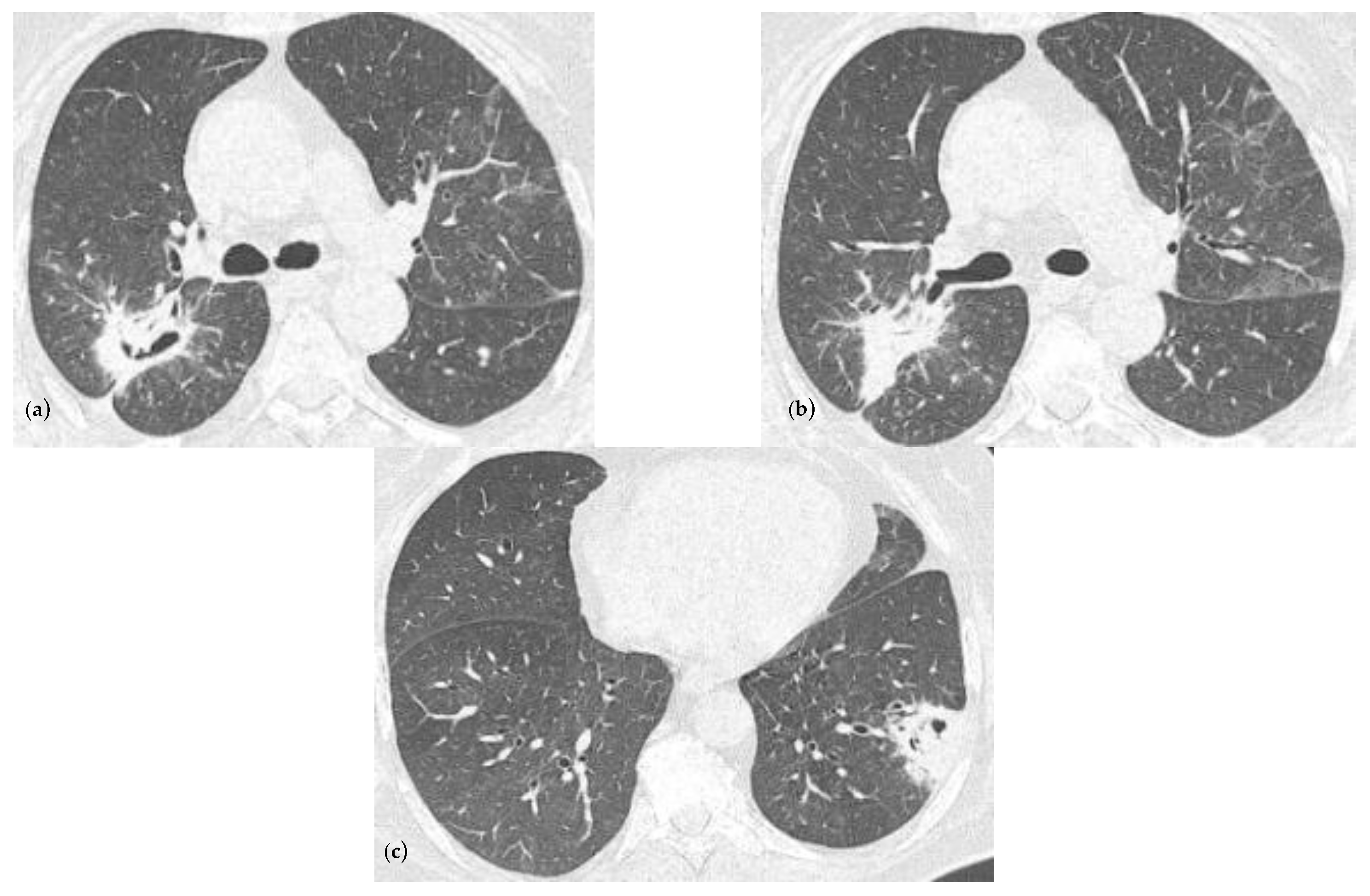
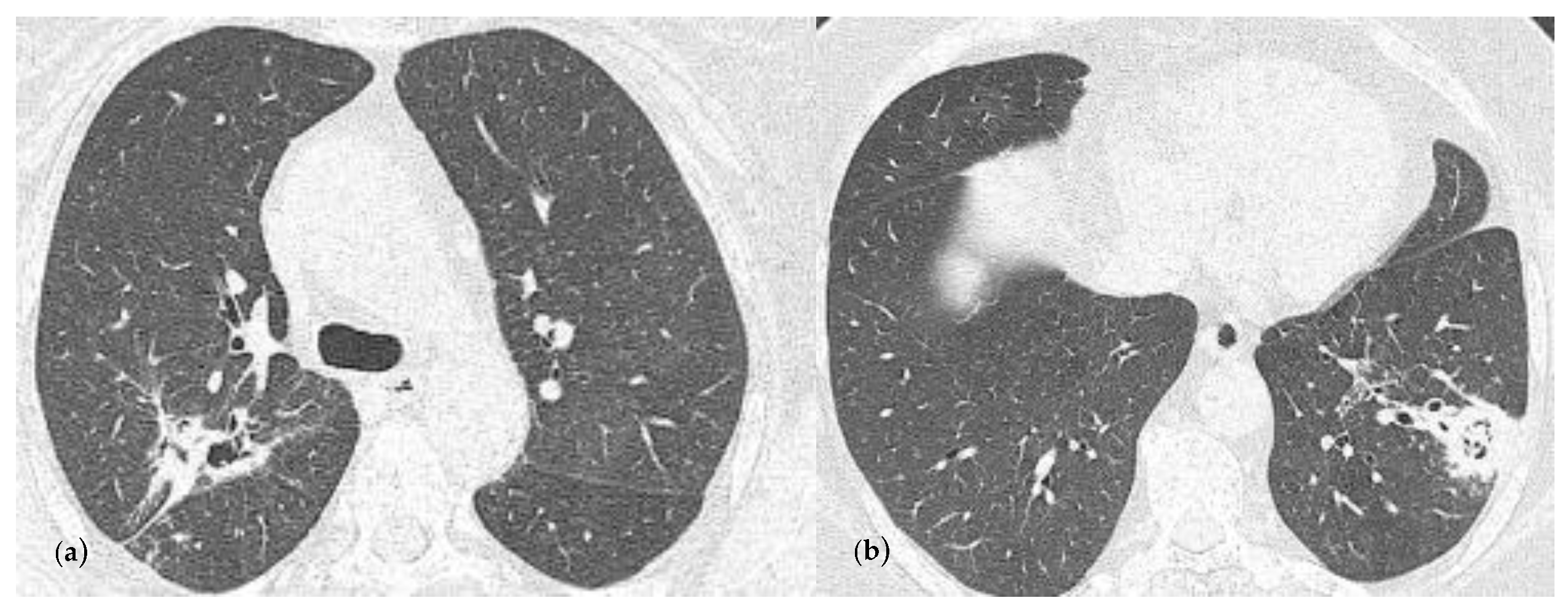
2.4. Follow-Ups
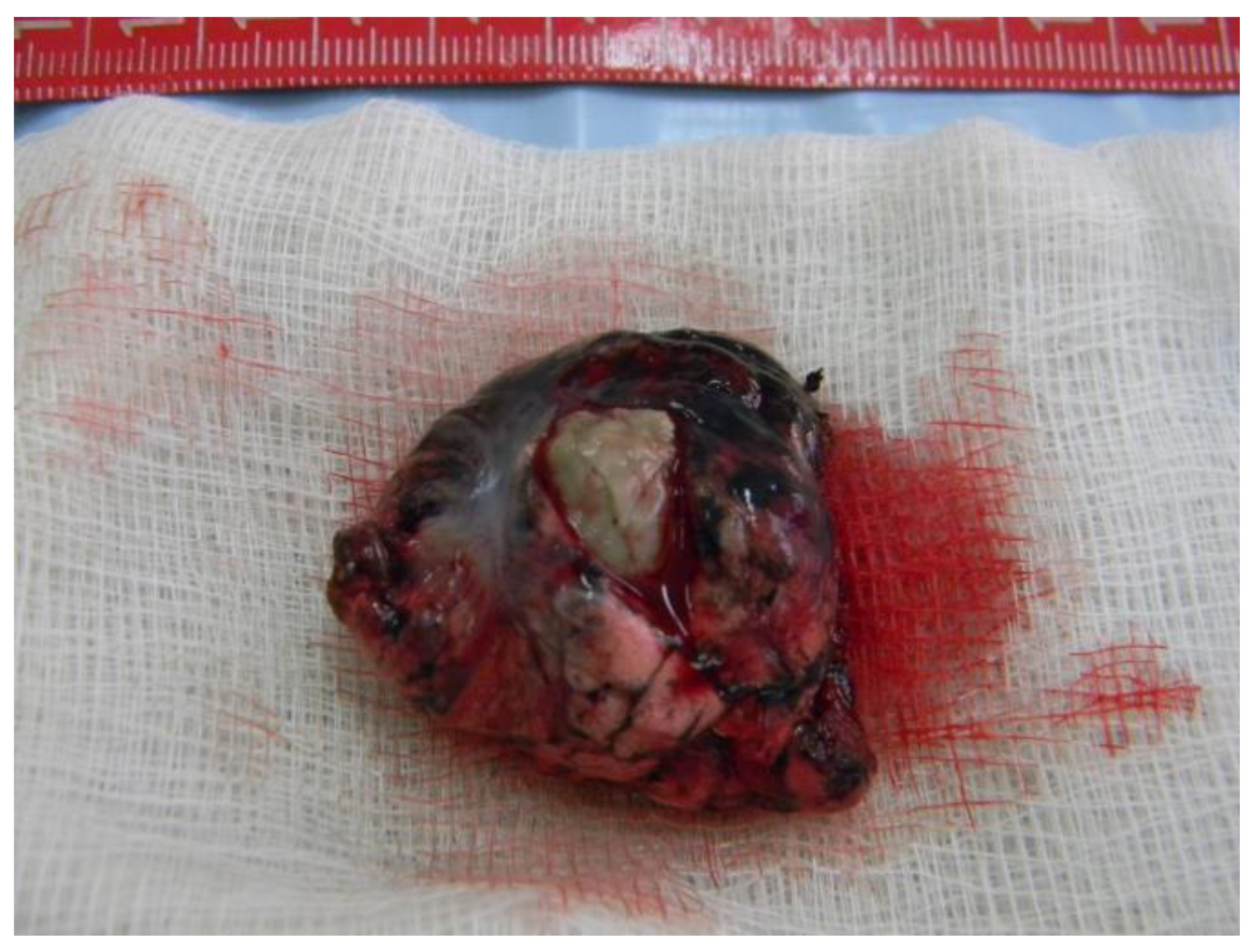
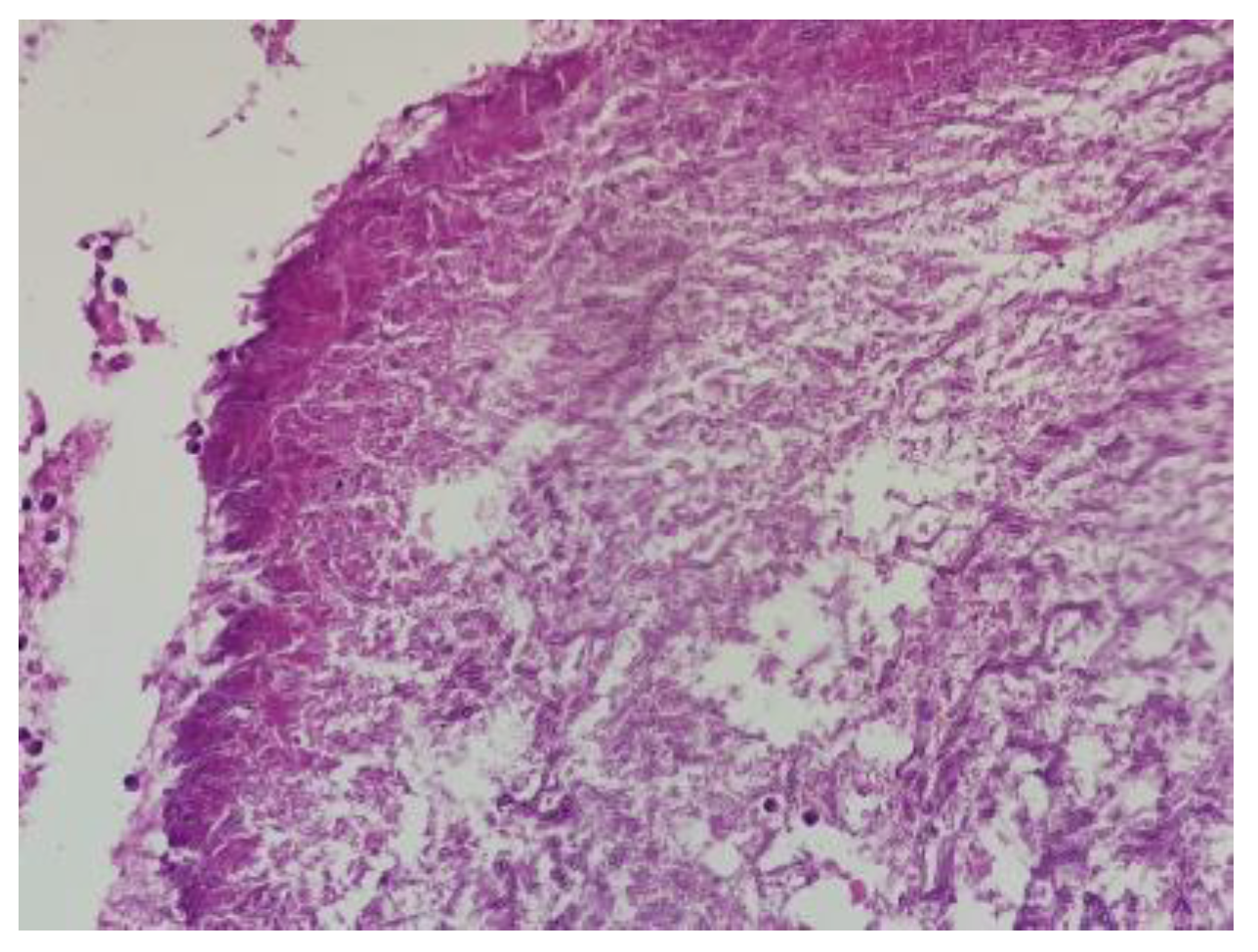
2.5. Pathology Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, Y.; Klein, S.L. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef]
- Salazar, F.; Bignell, E.; Brown, G.D.; Cook, P.C.; Warris, A. Pathogenesis of Respiratory Viral and Fungal Coinfections. Clin. Microbiol. Rev. 2022, 35, e00094-21. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021, 21, 149–162. [Google Scholar] [CrossRef]
- El-Baba, F.; Gao, Y. Pulmonary Aspergillosis: What the Generalist Needs to Know. Am. J. Med. 2020, 133, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Montrucchio, G.; Lupia, T. Risk factors for invasive aspergillosis in ICU patients with COVID-19: Current insights and new key elements. Ann. Intensive Care. 2021, 11, 136. [Google Scholar] [CrossRef]
- El-Shabasy, R.M.; Nayel, M. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar] [CrossRef]
- Araf, Y.; Akter, F. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence (NICE): London, UK, 2020.
- Horiuchi, H.; Utada, S. Chronic Pulmonary Aspergillosis During Convalescence from Severe COVID-19 Treated with Oral Itraconazole: A Report of Two Cases. Cureus 2022, 14, e27281. [Google Scholar] [PubMed]
- Permpalung, N.; Chiang, T.P. Coronavirus Disease 2019-Associated Pulmonary Aspergillosis in Mechanically Ventilated Patients. Clin Infect Dis. 2022, 74, 83–91. [Google Scholar] [CrossRef]
- Gangneux, J.P.; Dannaoui, E. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Xu, J.; Yang, X. Risk Factors for Invasive Aspergillosis in Patients Admitted to the Intensive Care Unit with Coronavirus Disease 2019: A Multicenter Retrospective Study. Front. Med. 2021, 8, 753659. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ruigómez, M.; Fernández-Ruiz, M. Long-Term Follow-Up of Patients Diagnosed with COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Fungi. 2022, 8, 840. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.Y.; Li, P.C. Diagnostic performance of serum galactomannan and β-D-glucan for invasive aspergillosis in suspected patients: A meta-analysis. Medicine 2024, 103, e37067. [Google Scholar] [CrossRef] [PubMed]
- Fosses Vuong, M.; Waymack, J.R. Aspergillosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chippa, V.; Aleem, A. Post Acute Coronavirus (COVID-19) Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- El Hammoumi, M.M.; Slaoui, O. Lung resection in pulmonary aspergilloma: Experience of a Moroccan center. BMC Surg. 2015, 15, 114. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.K.; Jiang, G.N. Surgical treatment for pulmonary aspergilloma: A 35-year experience in the Chinese population. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Gregoire, E.; Pirotte, B.F. Incidence and Risk Factors of COVID-19-Associated Pulmonary Aspergillosis in Intensive Care Unit-A Monocentric Retrospective Observational Study. Pathogens 2021, 10, 1370. [Google Scholar] [CrossRef] [PubMed]
- Anka, A.U.; Tahir, M.I. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand J. Immunol. 2021, 93, e12998. [Google Scholar] [CrossRef]
- Wang, J.; Yang, Q. Clinical characteristics of invasive pulmonary aspergillosis in patients with COVID-19 in Zhejiang, China: A retrospective case series. Crit. Care. 2020, 24, 299. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef]
- Bruscoli, S.; Puzzovio, P.G. Glucocorticoids and COVID-19. Pharmacol. Res. 2022, 185, 106511. [Google Scholar] [CrossRef]
- Cârstea, A.P.; Mită, A. How Dexamethasone Used in Anti-COVID-19 Therapy Influenced Antihypertensive Treatment in Patients with SARS-CoV-2. Healthcare 2023, 11, 1399. [Google Scholar] [CrossRef]
- Wagner, C.; Griesel, M. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst Rev. 2021, 8, CD014963. [Google Scholar]
- Dellière, S.; Dudoignon, E. Risk factors associated with COVID-19-associated pulmonary aspergillosis in ICU patients: A French multicentric retrospective cohort. Clin. Microbiol. Infect. 2020, 27, 790.e1–790.e5. [Google Scholar] [CrossRef]
- Bienvenu, A.L.; Bleyzac, N. No time for pending confirmation of invasive fungal disease in critically ill COVID-19 patients-think empirical treatment. Crit. Care. 2020, 24, 588. [Google Scholar] [CrossRef] [PubMed]
- Rovina, N.; Koukaki, E. Fungal Infections in Critically Ill COVID-19 Patients: Inevitabile Malum. J. Clin. Med. 2022, 11, 2017. [Google Scholar] [CrossRef] [PubMed]
- Bhopalwala, H.; Mishra, V. COVID-19 Infection and Late Manifestation of Pulmonary Aspergillosis. J. Investig. Med. High. Impact Case Rep. 2022, 10, 23247096211063332. [Google Scholar] [CrossRef]
- Ledoux, M.P.; Herbrecht, R. Invasive Pulmonary Aspergillosis. J. Fungi 2023, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.; Valerio, M. COVID-19 Study Group. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef]
- Seidel, D.; Simon, M. Results from a national survey on COVID-19-associated mucormycosis in Germany: 13 patients from six tertiary hospitals. Mycoses 2022, 65, 103–109. [Google Scholar] [CrossRef]
- Cocoş, R.; Mahler, B. Risk of Death in Comorbidity Subgroups of Hospitalized COVID-19 Patients Inferred by Routine Laboratory Markers of Systemic Inflammation on Admission: A Retrospective Study. Viruses 2022, 14, 1201. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S. The possible association between COVID-19 and postural tachycardia syndrome. Heart Rhythm. 2021, 18, 508–509. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Misra, A. Post COVID-19 Syndrome (“Long COVID”) and Diabetes: Challenges in Diagnosis and Management. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102235. [Google Scholar] [CrossRef] [PubMed]
- Thieben, M.J.; Sandroni, P. Postural orthostatic tachycardia syndrome: The Mayo clinic experience. Mayo Clin. Proc. 2007, 82, 308–313. [Google Scholar] [CrossRef]
- Shaw, B.H.; Stiles, L.E. The face of postural tachycardia syndrome-insights from a large cross-sectional online community-based survey. J. Intern. Med. 2019, 286, 438–448. [Google Scholar] [CrossRef]
- Miglis, M.G.; Prieto, T. A case report of postural tachycardia syndrome after COVID-19. Clin. Auton. Res. 2020, 30, 449–451. [Google Scholar] [CrossRef]
- Segrelles-Calvo, G.; de SAraújo, G.R.; Llopis-Pastor, E.; Carrillo, J.; Hernández-Hernández, M.; Rey, L.; Melean, N.R.; Escribano, I.; Antón, E.; Zamarro, C.; et al. Candida spp. co-infection in COVID-19 patients with severe pneumonia: Prevalence study and associated risk factors. Respir. Med. 2021, 188, 106619. [Google Scholar] [CrossRef]
- Golli, A.L.; Nitu, F.M. Bacterial Isolates from Endotracheal Aspirates and their Antimicrobial Resistance Pattern in Patients from Intensive Care Unit. Rev. Chim. 2019, 70, 3299–3304. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A. COVID-19-Associated Candidiasis (CAC): An Underestimated Complication in the Absence of Immunological Predispositions? J. Fungi 2020, 6, 211. [Google Scholar] [CrossRef]
- Mahler, B.; Parliteanu, O.A. Mucormycosis in a Patient with Severe COVID-19 Disease-The First Case Report in Romania and a Literature Review. Medicina 2023, 59, 555. [Google Scholar] [CrossRef]
- Kumar, M.; Sarma, D.K. Mucormycosis in COVID-19 pandemic: Risk factors and linkages. Curr. Res. Microb. Sci. 2021, 2, 100057. [Google Scholar] [CrossRef] [PubMed]
- Koukaki, E.; Rovina, N. Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients. J. Fungi 2022, 8, 881. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Values | Normal Range | |
|---|---|---|
| Blood Glucose | 233 md/dL | 74–106 mg/dL |
| Alanine Aminotransferase | 55 U/L | 0–35 U/L |
| Aspartate Aminotrasferase | 95 U/L | 0–35 U/L |
| Potassium | 3.07 mmoL/L | 3.5–5.5 mmol/L |
| Hemoglobin | 9.7 g/dL | 11.9–14.6 g/dL |
| D-Dimers | 671 ng/mL | 0–243 ng/mL |
| Erythrocyte Sedimentation Rate | 41 mm/h | 2–30 mm/h |
| Vital Capacity | Gas Transfer Factor | |
|---|---|---|
| Values | 73.6% | 20.1% |
| Drug | Dose | Administration |
|---|---|---|
| Gentamicin | 40 mg/12 h | Intravenous |
| Tigecycline | 50 mg/12 h | Intravenous |
| Gentamicin + Ipratropium + Physiological Serum | 20 mg + 0.5 mg + 1 mL | Aerosols |
| Voriconazole | 200 mg/12 h | Oral |
| Fragmin | 5000 UI/12 h | Subcutaneous |
| Acetylcysteine | 200 mg/8 h | Oral |
| Seebri Breezehaler | 44 mcg/12 h | Inhaler |
| Metoprolol | 50 mg/12 h | Oral |
| Ivabradine | 5 mg/12 h | Oral |
| Humulin R | Depending on glycemic values | Subcutaneous |
| Physiological Serum | 500 mL/12 h | Intravenous |
| Glucose 5% | 500 mL/12 h | Intravenous |
| Hepiflor | 1 tablet/12 h | Oral |
| 1 Month | 3 Months | 7 Months | 1 Year | |
|---|---|---|---|---|
| Blood Glucose | 153 mg/dL | 130 mg/dL | Not performed | 156 mg/dL |
| Hemoglobin | 10.3 g/dL | 11.7 g/dL | Not performed | 11.7 g/dL |
| Erytrocyte Sedimentation Rate | 108 mm/h | 57 mm/h | Not performed | 56 mm/h |
| Spirometry | Normal values | Normal values | Normal values | Normal values |
| Gas Transfer Factor | 53% | 67.9% | Not performed | 60% |
| 6 Mwt (6 Minute Walk Test) | 82.8% of predicted + moderate dyspnea at the end of the test | 98.38% + slight fatigue at the end of the test | Not performed | Not performed |
| Treatment | Voriconazole | Voriconazole | Thoracic surgery | No treatment |
| Study Name | Study Type | Study Duration, Country | Description | Steroid Treatment | Capa Treatment | Conclusions |
|---|---|---|---|---|---|---|
| Case report | Not mentioned | 49-year-old woman, diabetes mellitus, hypertension, hyperuricemia, obesity (BMI 33.8) | methylprednisolone (mPSL) puls | Itraconazole | Patient was transferred to a long-term care facility |
| Retrospective cohort | March 2020–August 2020, Maryland | 39 patients (17 female patients), mean age 66 (55–70), 15 patients had diabetes mellitus, 29 patients had hypertension | 26/39; the CAPA patients and the controls statistically significantly differed from one another for hydrocortisone alone (38.5% vs. 12%, respectively; p < 0.001). | 19/39 | 17 patients survived |
| Retrospective, prospective, observational multicentre cohort. | February–July 2020, France | 76 patients (14 female patients), 26 had diabetes, 36 had hypertension, mean age 76; 76/128 had CAPA. | 34/76 received steroids treatment. | Voriconazole was given to 44 (76%) patients, liposomal amphotericin B to 20, caspofungin to 16, isavuconazole to 11 (19%), fluconazole to 30 (52%), and other antifungal medications (not specified) to 5 (9%) patients, either separately or in combination. | In addition, 45.8% (95% CI 25.6–67.2) was noted in the 24 patients who had a suitable clinical setting of aspergillosis and non-bronchoalveolar lavage or bronchial or tracheal aspiration positive for Aspergillus spp. |
| Retrospective cohort | December 2019–April 2020, China | 78 patients (29 female patients), mean age 64.3 ± 13.6, 16 had diabetes, 38 had hypertension. | Compared to patients without CAPA, those with CAPA had a significantly higher likelihood of using a higher daily dose (≥40 mg) of methylprednisolone (53.9 vs. 34.2%, p = 0.002). | considerably more likely than individuals without CAPA to use methylprednisolone at a higher daily dose (≥40 mg). | 37 survived; those with CAPA had a greater ICU death rate (52.6 vs. 28.4%, p < 0.001) than those without CAPA. |
| Retrospective, observational, single-centre cohort | January 2020–January 2021, Spain | 12 patients (3 female patients), mean age 65 ± 10. | All patients received steroid treatment. | Voriconazole was given to 5/12, liposomal amphotericin B to 1/12, and isavuconazol to 2/12 (42.1%). The serum galactomannan test was run in 66.7% (18/27), and 11.1% (2/18) of the results were positive. | It was found that five of the twelve survivors (41.6%) were ultimately diagnosed as colonization, and that either no antifungal treatment was administered or it was stopped in less than 48 h. Ultimately, it was decided that the remaining seven individuals were CAPA-confirmed cases. Upon follow-up, all seven patients were deemed cured and did not exhibit a clinical relapse. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosteanu, I.-M.; Mahler, B.; Parliteanu, O.-A.; Stoichita, A.; Matache, R.-S.; Marghescu, A.-S.; Filip, P.-V.; Mota, E.; Vladu, M.I.; Mota, M. Wedge Resection and Optimal Solutions for Invasive Pulmonary Fungal Infection and Long COVID Syndrome—A Case Report and Brief Literature Review. Reports 2024, 7, 25. https://doi.org/10.3390/reports7020025
Mosteanu I-M, Mahler B, Parliteanu O-A, Stoichita A, Matache R-S, Marghescu A-S, Filip P-V, Mota E, Vladu MI, Mota M. Wedge Resection and Optimal Solutions for Invasive Pulmonary Fungal Infection and Long COVID Syndrome—A Case Report and Brief Literature Review. Reports. 2024; 7(2):25. https://doi.org/10.3390/reports7020025
Chicago/Turabian StyleMosteanu, Ioana-Madalina, Beatrice Mahler, Oana-Andreea Parliteanu, Alexandru Stoichita, Radu-Serban Matache, Angela-Stefania Marghescu, Petruta-Violeta Filip, Eugen Mota, Mihaela Ionela Vladu, and Maria Mota. 2024. "Wedge Resection and Optimal Solutions for Invasive Pulmonary Fungal Infection and Long COVID Syndrome—A Case Report and Brief Literature Review" Reports 7, no. 2: 25. https://doi.org/10.3390/reports7020025
APA StyleMosteanu, I.-M., Mahler, B., Parliteanu, O.-A., Stoichita, A., Matache, R.-S., Marghescu, A.-S., Filip, P.-V., Mota, E., Vladu, M. I., & Mota, M. (2024). Wedge Resection and Optimal Solutions for Invasive Pulmonary Fungal Infection and Long COVID Syndrome—A Case Report and Brief Literature Review. Reports, 7(2), 25. https://doi.org/10.3390/reports7020025