Abstract
The present study is a Dance Movement Psychotherapy (DMP) pilot intervention designed to address the psychological challenges faced by Greek breast cancer patients, after surgery and around radiotherapy treatment. It was designed as a 12 weeks’ project, involving patients of diverse age and educational level, mostly living in rural areas. The personality and psychopathology inventory Symptoms’ Check List-90 (SCL-90), the therapist’s records and video self-observation were used in a mixed method approach. Thirteen subjects initiated the study, but they were gradually reduced and only four completed it. Statistical analysis was performed using SPSS-25 addressing this fact. Positive results of qualitative interpretation of the therapist’s data and SCL-90, as well as changes in movement patterns and self-perception evaluated via video self-observation, showed that the intervention was beneficial for the patients who completed it. However, the fact that not all the participants were able to finish the program, implies that although DMT intervention at an early stage can help some patients deal with strong emotions, careful evaluation of eligible individuals should precede. Besides the patients’ medical condition, demographic and personality characteristics should be considered in the design of future similar studies.
1. Cancer and Psychopathology
A serious illness affects the psychological well-being of a person. Being diagnosed with cancer one recognizes that the world is less controllable than one thought. Depending on how one perceives and evaluates the threat of the disease to one’s life, emotions are influenced. One-third of cancer patients in acute care experience mental disorders [1] which in general might include depression, anxiety, grief, reduced self-esteem, and lower quality of life with feelings of inferiority, fear of rejection, and self-blame [2,3].
Breast cancer has been regarded as a particularly traumatic experience [4,5] and women diagnosed with early-stage breast cancer indicate high rates of psychological disturbances or psychiatric problems [6]. Nearly 50% of them have been found with depression, anxiety, or both in the year after diagnosis, that in some of the cases is the recurrence of previously existing illness [7,8,9]. Parallel breast cancer patients are particularly concerned with existential issues, changes in everyday activities, and the impact on social life, as well as bodily physical changes and their female identity [10]. Their body image, that is, their perception of their body in connection to feelings sensations and ideas, changes negatively [11,12].
Culture plays an important role in how the illness is perceived by the patient and her environment. Early researchers noted that having cancer was considered as a mark of disgrace [13]. The psychopathological profile of Greek women with breast cancer also shows high scores on somatization, depression, phobic anxiety, and general psychopathology. In Greek society, having cancer is still considered sordid and something like a punishment, often a self-punishment, while talking about cancer is still a taboo [14]. Guilt, mixed with lack of information, creates stereotypes that make patients feel afraid not only of the illness but also of what is connected to it, and diffuses what a person feels. This diffusion of feelings is similar to the initial effect of paralysis after hearing the news of having cancer. Those blurred feelings, also called “aporetic”, are experienced as hazy, conflicted, and confusing [15].
Since as early as 1989 [16], researchers have agreed that treatment for breast cancer [6,17,18] or cancer in general [19], must include appropriate psychotherapeutic intervention, focusing attention on quality of life, which is especially underlined in breast cancer patients [1] and female cancer patients independent of their diagnosis [20].
Dance movement therapy (DMT) or dance movement psychotherapy (DMP) (we will use here the term dance movement psychotherapy (DMP) which is used in the UK, whereas the term dance movement therapy (DMT) is used in America) is an expressive arts therapy. Arts therapies involve using the arts in a therapeutic environment with a trained therapist. The different types of arts therapies include music, visual art, dance, and drama. DMP is a combination of the art of dance with psychology and psychopathology, utilizing a variety of theoretical orientations, philosophies, and techniques, towards different directions of need. The American Dance Therapy Association (ADTA) defines it as the psychotherapeutic use of movement to promote cognitive, emotional, social, and physical integration of the individual. Believing that the mind is not in the brain but in the whole body, in other words, our neurocognitive system exists through our bodily existence [21], DMP addresses the body and creates a safe environment where one can practice non-verbal communication and self-expression. This can be especially useful to individuals who have difficulty verbalizing thoughts and emotions. Studies have showed short and long-term DMP to be effective in improving quality of life, managing stress, and reducing psychological distress [22,23]. Concerning stress, one study has also shown DMP to have a beneficial effect on stress-related hormones [24]. Medical dance movement psychotherapy adapts knowledge from medical science and develops clinical methods addressing needs of medical patients [3]. DMP can increase quality of life, decrease clinical symptoms such as depression and anxiety, and can promote positive mood, affect, and body image in those patients [25,26].
DMP work with cancer patients facilitates coping with this chronic, life threatening illness through learning to accept and altering their awareness towards their bodies, building higher self-confidence, reinforcing self-expression, addressing feelings of isolation, anger, and fear, as well as strengthening personal resources and increasing their sense of hope [3,26,27,28,29,30,31]. To our knowledge, only one DMP study has addressed cancer patients in the initial state of treatment, conducted with Chinese patients. In this study, [32] found that psychological and physical relief that came from the DMP intervention helped breast cancer patients, during and after radiotherapy, to cope with radiation treatments and physical symptoms, improve mental well-being and general functioning, reconnect with life, and participate in shared positive experiences. Concerning DMP in cancer, Bradt et al. [33], suggest that the overall quality of the evidence is low, as it consists of a limited number of studies, mostly small and with little statistical power. However, a recent review [34] suggests that many qualitatively perceived benefits and improvements in quality of life were not seized by the statistical analyses.
The purpose of this pilot study was exploratory, in order to investigate the efficacy of a DMT intervention designed to address the psychological challenges faced by breast cancer patients in the initial state of treatment (during, right before, or right after radiotherapy). To our knowledge, in this country, only two studies with oncologic patients used dance as exercise and in the form of Greek traditional dances, in order to manage anxiety and stress and to improve quality of life with positive results [35,36]. Our hypothesis is that the expressive aspects of DMP can be beneficial to the patients in this early stage of illness, taking also in consideration characteristics of their ethnic idiosyncrasy and the perception of cancer in this country. To our knowledge, this is the first DMP study conducted with a Greek oncologic population.
2. Materials and Methods
The study was based on a 12-week DMP work group conducted by the Psychiatric Department and took place in the Radiotherapy Department of a University General Hospital in Greece. The work group involved 13 women, aged from 40 to 74 years, with a mean of 58.4 years and a standard deviation of 9.2. Most of them were living in nearby rural areas. All of them had been surgically treated for breast cancer and were undergoing the process of radiotherapy. The sessions took place in the Radiotherapy Department.
3. Data Collection
3.1. SCL-90
Symptoms’ Checklist-90 (SCL-90) [37] was used as a descriptive measure of the patients’ psychopathology before and after the DMP program. It is a self-report questionnaire designed for use as a psychiatric screening instrument and a measure of global symptom severity, measuring symptom intensity on nine different subscales. Participants were asked to complete the questionnaires at baseline, at the beginning of the first DMP session, and at the end, immediately after the last session.
3.2. Video
Patients were individually videotaped during the DMT session in the 2nd and 11th week of the study. Video observation and qualitative interpretation, conducted together by the patients and the therapist, took place as part of the last (12th) session in order to evaluate changes in movement patterns and self-perception. Nine patients participated in the initial video and four patients participated in the final.
3.3. Observation–Therapist’s Records
Data of a mainly process-oriented qualitative character were gathered using participant observation during the 12 DMT sessions and were documented in the therapist’s journals.
4. Session Design
A 60-min DMP session was held once a week for 12 consecutive weeks. The structure of the sessions was: warm-up, process, and closure, as has previously been suggested in the literature [30,38]. Warm-up focused on awareness of (a) the body, (b) breathing, (c) the room, and (d) the group. Process was based on thematic movement and was developed according to the progress and dynamics of the group, involving mostly emotional processing of psychological struggles associated with breast cancer diagnosis. Closure included relaxation exercises and a movement ritual initially given by the therapist and later developed mainly by the patients. Verbalization was used for self-reflection at the end of the process part of the session and before the closure ritual, or parallel to the movement experience, allowing the patient to give meaning and significance to this experience. The patients had the freedom to choose not to participate in any part of the session.
5. DMP Intervention
The intervention was based on the group’s process focused on specific factors associated with the therapeutic experience and chosen for the needs of this specific population: instillation of hope, universality of feelings, and solidarity/information sharing [39]. The main focus was in response to the groups’ needs and was associated with improvement in motility/vitality, work on body image, and emotional release and externalization. Schmais’ [40] notion that the kernel of dance therapy is to keep the group in motion, remained central in this study. A circle formation was mainly used in the beginning and at the end of every session, integrating group participants and therapist in equal democratic positions. The emotional repertoire of patients’ movements was mirrored by the therapist in order to establish empathic connections and build empathic reflection, namely kinesthetic empathy as recommended by Sandel [41] and Levy [42]. Rhythmic group activity was used in a non-directive way, while individuality was strongly supported, allowing each participant to find their own personal rhythm and the group to find synchronization in its own pace. Images, suggested by the therapist or patients, became movement material and were processed verbally during the dance and at the end of each session.
6. Results
None of the women participating in our study had major psychopathology at baseline according to the SCL-90 questionnaire.
Of the 13 women who were invited to attend the total twelve sessions of the dance therapy program, 4 women responded to one or two sessions, 5 to four to seven sessions, and 4 to nine to twelve sessions.
7. Description of the Intervention
The women were encouraged to bring into each session issues connected to their illness. The exploration of those themes was done mainly through dance and movement in the circle. In this formation women alternated in taking the leadership in movement and the rest of the group followed. The “group leader” was encouraged to “follow her need” and the rest of the group to follow her movement, if they felt like. A further proposition was to step in the center of the circle and dance “how I feel today”. We agreed on the freedom of choosing not to step in the center if not feeling ready for it, but even if not entering, the patients stayed active dancing and witnessing on spot in the circle.
In the 2nd session, the individual videos were shot. The camera held by the therapist focused on one person at a time, while everyone danced on the spot in the circle formation.
Expression of emotions and releasing physical and emotional energy came naturally to some patients even in the first sessions. At a very early phase (3rd session), the issue of their illness became central and the confrontation with their personal situation became already critical. In the 4th session, themes emerged concerning body, freedom, truth, communication, and release. In the 6th session, the group felt really comfortable together. The image of a ball, which had been introduced at baseline, through the study took various symbolic forms. We used this image working on the individuals’ perception of kinesphere and her use of space in order to communicate. Soon this initially big ball became one that could be held in the hands. The 8th session was a very important one, as the imaginary ball became their cancer. When one decided to “throw the ball to Mount Olympus” (the highest mountain of Greece, overlooking the city), they all followed. In the 9th session the group consisted of 4 patients. The group agreed that this was probably because “things came up”. The group was at this point delighted to meet each other and it was difficult to keep them from talking constantly. They also agreed that the less people in the group, the deeper work was being done. At this point the circle formed and dissolved itself naturally, with the therapist being a part of it, intervening only to raise awareness mainly towards neglected body parts, and reminding them to stay connected to their needs. In the 11th session, the second videos were shot. It was initially planned to be in the circle as at baseline, but they very soon started to dance free in space and became interactive with each other. In the final session, a retrospective video review took place, where they talked about each other’s movement, their personal experience, and changes they noticed in others and themselves. Finally, they were all throwing balls of all colors and sizes filled with emotional weight.
8. Effects of the DMT Intervention
Generally, at baseline the group seemed confused, did not know what was expected from them, and worked hard as if obeying medical instructions. This hard work was mainly manifested in arm movements, like digging and kneading, or repetitive opening and raising of the arms. Patients very soon started to connect to each other, metaphors were discussed, and they agreed on common facts such as saying “yes” more often than “no” in their everyday lives. While they became comfortable in forming a circle, it took courage to step in the middle of it and deal with what initially seemed hazy, and obviously overwhelming emotions. Rhythmic synchrony of the group connected and supported this courage, building a sense of solidarity. Women who were disconnected from themselves and others began to connect. Images and movement metaphors that manifested themselves almost constantly, were processed verbally mostly during the dance, and gave us knowledge about their inner reality and the quality of their experience [43]. Verbalization was an important part of the session. It emerged spontaneously early in the study, mostly as a need in the form of exchanging information and experience about their illness, what Yalom [39] calls solidarity/information sharing. Later, directed by the therapist, verbalization focused on the imagery symbols that they used in-session and the expression of associated feelings. The imaginary “throwing of a ball” became a group ritual, through repetition it became an important act of tension release, and it seemed that as an action, it brought hope.
An important moment was during the 9th session, when a woman, that had just finished chemotherapy and had to start radiation therapy, stated that she felt like having been “at the bottom of a deep well” and was now resurfacing towards the light. “The light will soon be too strong and I need protection”, she confessed.
At the end of the study their overall movement stayed mainly peripheral, but the flow was remarkably freer. The use of personal space was much bigger and there was a lot of locomotion. It was by then considerably easier to take initiative and express oneself. The circle was easily dissolved, and couples were dancing and conversing casually with each other. There was fun and laughter and a sense of conspiracy that connected all, patients and therapist.
Through the collective video review, they had a chance to look at themselves, an experience that none of them had before. They were surprised over how they looked, observed, and talked about each other. They recognized a common lack of action in the trunk that remained through the study, which they believed was due to shame and lack of similar movement experience. They also noticed that the arms were constantly very active and agreed that due to their illness this body area carries strong emotions. They recognized the fun they had and positive changes in themselves and others. Finally, they talked about their limits, new facts, and life roles. Decisions were made mostly concerning changes in values and priorities, including doing less hard work (saying “no” more often) and adding movement in their everyday life.
According to the SCL-90, the patients that remained and completed the study showed a shift from the medium (2) or extremes on the right side of the scale (3, 4) that they had on different intensities at baseline, to a much more subtle attitude with numbers almost exclusively from the left side of the scale (0, 1, and a few 2) present. The biggest shifts were about being less nervous, less tired, much less lonely, less angry, gaining better self-esteem, sleeping better, having less death thoughts, getting less easily hurt, and having much more hope.
9. Statistical Analysis
A statistical analysis was done in order to investigate the tendency to subgrouping and presence interruptions, as we believed had a connection to patients’ age and the distance they had to travel to be able to participate in the study (Table 1).

Table 1.
Characteristics of the patients (age/distance).
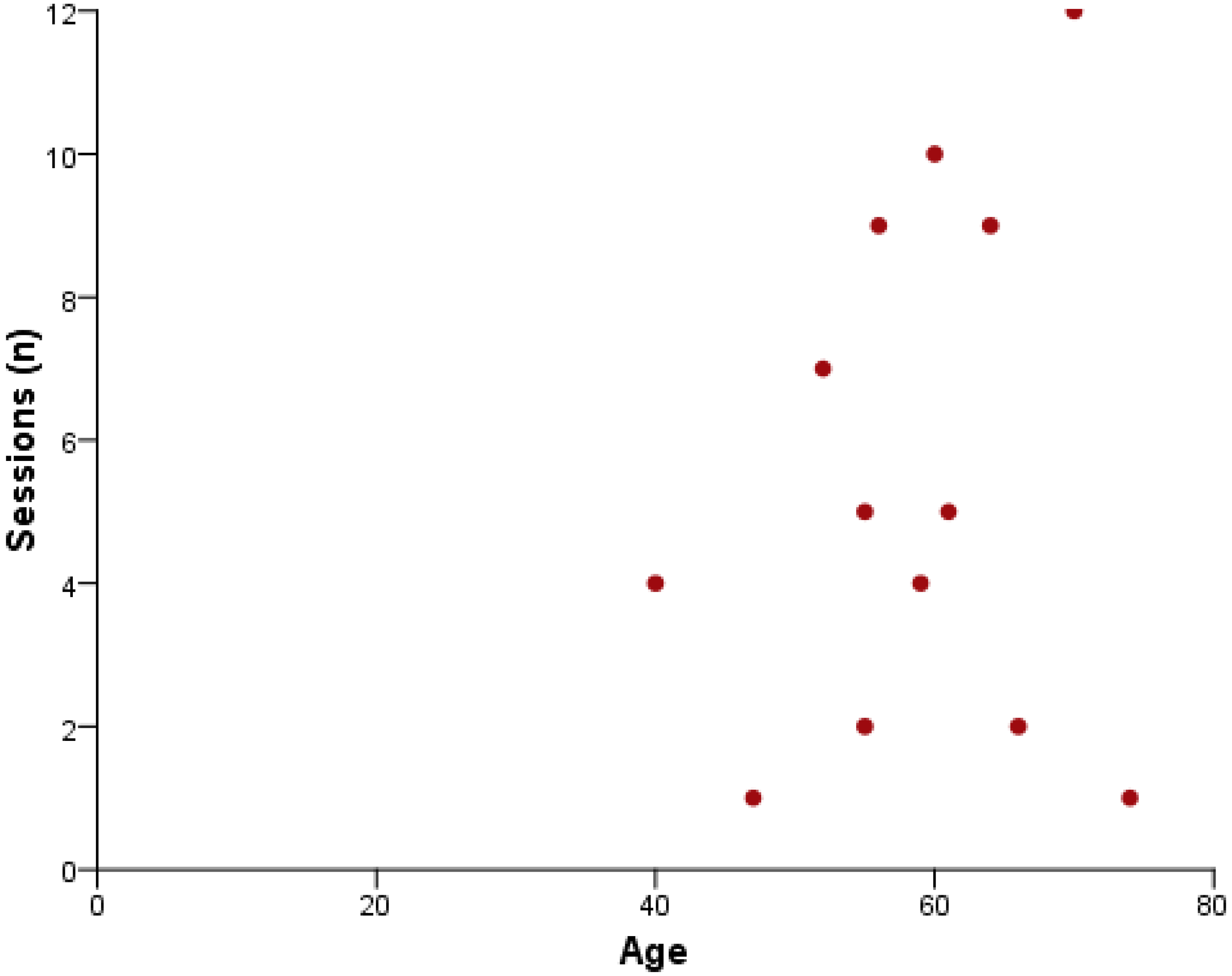
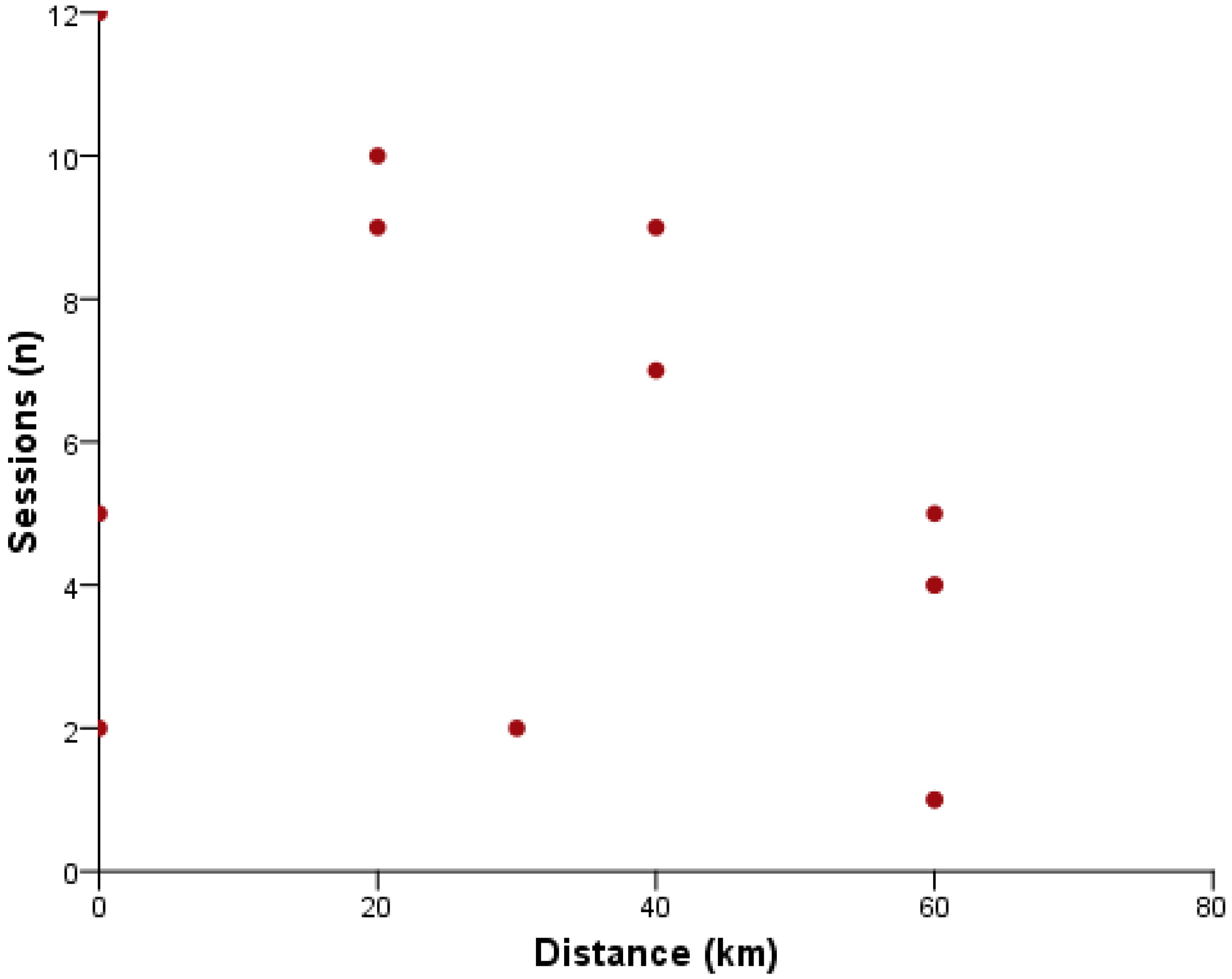
Linear bivariate correlation was used to investigate the relationship between the total number of sessions attended by each participant and the age and distance of the patient’s home from the intervention site. Statistical analysis was performed using SPSS-25. The minimum value of the level of statistical significance, p-value, was set at 5%. The normality assumption of the data was tested by the Shapiro–Wilk test, due to the small sample size (n = 13). It was found that the variable “Distance” does not follow the normal distribution (p = 0.002), while the “Age” (p = 0.998) and “Sessions” (p = 0.318) variables are normally distributed. Therefore, Pearson’s coefficient was used to investigate the relationship between the “Sessions” and “Age” variables, and Spearman’s coefficient for “Sessions” and “Distance” variables.
The analysis did not show statistically significant associations between the total number of sessions attended by the participants and neither age (rp (13) = 0.193, p = 0.527) nor distance (rs (13) = −0.442, p = 0.130). However, the trend implied that older women, who live closer to the area where the intervention program took place, were more likely to participate (Figure 1 and Figure 2 near here).
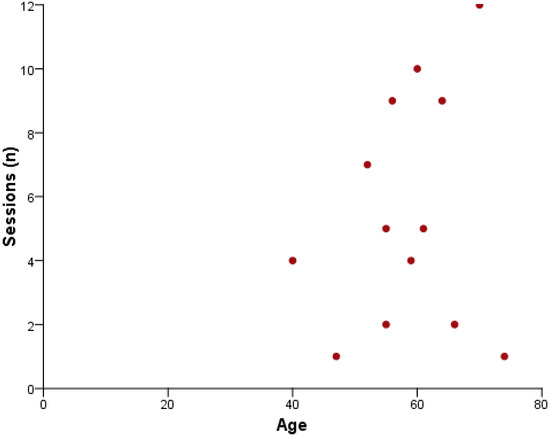
Figure 1.
Scatter plot of Age vs. Sessions.
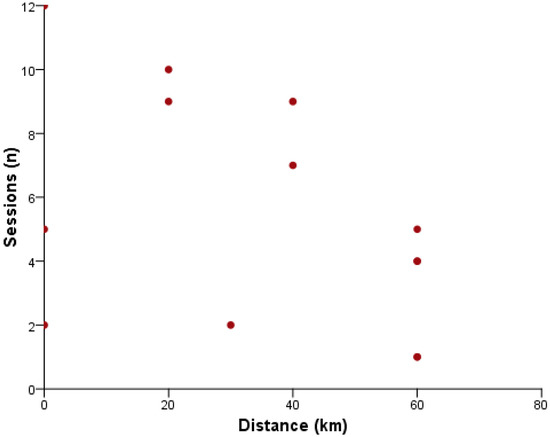
Figure 2.
Scatter plot of Distance vs. Sessions.
10. Discussion
Our clinical impression at baseline was that emotional distress was strongly present, yet this was not revealed in our psychometric screening. However, as has previously been suggested, psychopathology may often be unrecognized or may not emerge until after treatment has ended [18].
While the initial intention was to use the Symptoms’ Checklist-90 (SCL-90) quantitatively, it was finally used descriptively and qualitatively, due to the small number of participants that completed the study. This actually limits the mixed method approach of the study and stresses the qualitative aspects of it. However, as stated by Goodill [34], and already mentioned earlier, many qualitatively perceived benefits and improvements in quality of life due to the intervention, may not be seized quantitatively.
DMP is a very new modality of psychotherapy for most Greek people, and a totally unknown one for Greek cancer patients. It is generally well documented that physical exercise enhances the quality of life of cancer patients [44] and has positive effects on physiology, body composition, physical functions, and psychology after breast cancer treatment [45]. Similar positive effects had a recent study with Greek traditional dances used as aerobic exercise together with upper body training on cancer survivors and is suggested as an alternative choice of physical activity [46].
Traditional Greek dance as exercise intervention was also used in order to reduce stress and anxiety levels in patients diagnosed with cancer of any type [35] and in order to improve the quality of life in breast cancer patients [36] and had positive results. Traditional Greek dances involve specific music, specific rhythm and steps, specific usually circular united structure, specific leadership by the first dancer and obedient following by the rest of the dancers. In simple words, they provide an absolutely stable structure ensuring minimum personal exposure. That is, minimum emotional risk-taking similar to physical exercise.
Dance, though, goes beyond physical exercise involving the emotions, emphasizing the expressive aspects of movement and enhancing communication. Moreover, in DMP, it is not the learnt movement that leads to change, but the freely improvised one. Through this free movement, letting oneself follow his/her needs and expressing them through body action and through the therapeutic intervention, positive changes occur. The communication of emotions through symbols and metaphors in a non-verbal level makes them less threatening. In cancer, metaphors can become an escape from the rationality that the patient’s condition demands and can open a door to their inner world. This play and symbolism can create a positive atmosphere and promote expression and communication in the group, especially between those individuals connected already with a common strong experience, such as cancer. The act of creating symbols for emotions, especially suppressed emotions coming from negative life events, brings them to the surface and helps the patient deal with them. This may stimulate the healing processes. In this study, imagery initiated by our ball image became “a bird” that one let free from a cage, “a necklace” that one wore and danced with in the party, a “child toy ball” the group played with. The most characteristic symbolic image often used by the group was the “throwing of the ball” recognized as cancer, high and far away (as far and high as Mount Olympus).
“The image reveals the quality of the experience and, at the same time, it triggers a potential experience.”[43]
However, is every patient emotionally ready to deal with such a potential experience? Our patients had absolutely no previous exposure to similar suggestions and no familiarity with DMP. Most of them were coming from rural isolated areas and had to travel long distances to receive treatment and access the sessions, and mostly had a relative driving them. Their independence and freedom were limited.
As they mentioned, when they heard the word dance they were expecting the well-known to them safe structure of traditional Greek dancing. When exposed to a different, less structured modality, they had to face the fact that “things come up…”. Thus, the initially larger number of patients was spontaneously divided in smaller inter-changing groups (4–8 participants). However, despite the reasons for subgrouping and presence interruptions in this study, it was indeed evident that, as the number of the patients that participated in every session decreased, the work became deeper therapeutically.
Potentially, if a division was done by the researchers from the beginning of the study, based on a thorough individual psychiatric interview addressing demographic and personality issues, the number of patients completing the 12-week program might have been larger. Apparently, although a major health issue on its own, cancer alone is not enough to ensure a group’s eligibility for DMP. Personality and demographic issues are likely more important in what is practically a form of psychodynamic therapy, and as such smaller working groups may have been more effective.
Furthermore, the overall timing of the intervention in association to the illness might have been an important factor for presence interruptions. All of the patients had been more or less under the initial shock, with aporetic feelings, manifesting in great confusion. The DMP intervention itself, so early after their diagnosis, might as well have temporally increased the feeling of sadness. This could have been too threatening against a possibly active denial used in order to cover their fear about the illness. Goodil [3] suggests that one can deal better with denial when moving further in treatment and rehabilitation. Furthermore, there is also a notion that a constant positive attitude is necessary for the healing of cancer, connected to the fear that the experience and expression of negative or painful feelings might somehow meddle with this healing, and may even progress the illness [31]. When this fake positive attitude came against the truth of the body, the strong emotions that emerged might have become a good reason for some to protect themselves by absence, or even run away.
11. Limitations and Recommendations for Further Studies
As the treatment intervention was led by the researcher, this inevitably introduced bias into some data. Therefore, the researcher was supervised throughout the study, in order to eliminate those biases. Finally, the small number of participants that completed the study, as well as the absence of a control group, limit the generalizability of it. Aspects of the study though, may have the potential for wider application, and provide the rationale for a larger study. Further research needs a more rigorous design, including possibly a group, or groups of a smaller size, and a follow-up period in order to assess DMT’s lasting effects on participants.
12. Conclusions
What seems to be the conclusion out of the results of the present pilot study, is that for the most suitable individuals, DMP did provide a safe therapeutic environment and they benefited highly from this, initially non-verbal and later also verbal, opportunity to release emotions. Powerful feelings came out in the open as part of the dance and expressing those feelings was experienced as positive and this way less terrifying. Sharing positive experiences through DMP fostered the group’s cohesiveness [39,40]. The group became a good source of emotional support, while the common action and repetition in different levels of intensity reduced fear and anxiety [29,32]. Verbal processing of the movement material allowed the patients to actively give meaning and significance to the experience, and video-collective review helped them reflect on non-verbal somatic signals and symptoms.
The study confirmed well-established findings on the positive influence of dance movement psychotherapy on the psychological wellbeing of suitable cancer patients. The non-verbal level of dance and the creative symbolic action became the container of our patients’ experience. By reflecting on them, the given fact of their illness could be seen from a new perspective. This new perspective enabled the patients to overcome their boundaries, open themselves up and express their feelings and emotions. This enabled them to gain new perception about themselves and develop relationships with each other. As it is well documented that psychological disturbances are to be expected among cancer patients, DMP intervention at some point can be preventive and help patients understand that strong emotions are normal, and that even a cancer experience could guide a path to positive personal growth.
Author Contributions
Conceptualization, S.K.; Formal analysis, S.K. and M.T.; Funding acquisition, S.K.; Investigation S.K.; Methodology, S.K.; Project administration, P.D.F.; Resources, M.T. and A.P.; Supervision, M.N.P.; Validation, M.N.P. and K.B.; Visualization, S.K. and M.N.P.; Writing—original draft; S.K.; Writing—review & editing, M.N.P. and K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Singer, S.; Das-Munshi, J.; Brähler, E. Prevalence of mental health conditions in cancer patients in acute care—A meta-analysis. Ann. Oncol. 2010, 21, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.L.; Lopez, A.M.; Schwartz, G.E.; Bootzin, R.; Figueredo, A.J.; Braden, C.J.; Kurker, S.F. Quality of life and breast cancer: Relationship to psychosocial variables. J. Clin. Psychol. 2001, 57, 501–519. [Google Scholar] [CrossRef] [PubMed]
- Goodill, S. An Introduction to Medical Dance/Movement Therapy: Health Care in Motion; Jessica Kingsley Publishers: London, UK; Philadelphia, PA, USA, 2005. [Google Scholar]
- Van den Berg, S.W.; Van Amstel, F.K.P.; Ottevanger, P.B.; Gielissen, M.F.; Prins, J.B. The cancer empowerment questionnaire: Psychological empowerment in breast cancer survivors. J. Psychosoc. Oncol. 2013, 31, 565–583. [Google Scholar] [CrossRef] [PubMed]
- Chilton, J.A.; Downing, C.; Lofton, M.; Hernandez, M.; Allen, B.W.; Hajek, R.A.; Gor, B. Circle of sisters: Raising awareness of Native American women to breast cancer. J. Health Care Poor Underserved 2013, 24, 1167–1179. [Google Scholar] [CrossRef]
- Kissane, D.W.; Ildn, J.; Bloch, S.; Vitetta, L.; Clarke, D.M.; Smith, G.C.; McKenzie, D.P. Psychological morbidity and quality of life in Australian women with early-stage breast cancer: A cross-sectional survey. Med. J. Aust. 1998, 169, 192–196. [Google Scholar] [CrossRef]
- Burgess, C.; Cornelius, V.; Love, S.; Graham, J.; Richards, M.; Ramirez, A. Depression and anxiety in women with early breast cancer: Five year observational cohort study. BMJ 2005, 330, 702. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.; Holcombe, C.; Clark, L.; Boothby, M.R.K.; Hincks, A.; Fisher, J.; Salmon, P. Predictors of onset of depression and anxiety in the year after diagnosis of breast cancer. Psychol. Med. 2011, 41, 1429–1436. [Google Scholar] [CrossRef]
- Klikovac, T.; Djurdjevic, A. Psychological aspects of the cancer patients’ education: Thoughts, feelings, behavior and body reactions of patients faced with diagnosis of cancer. J. BU ON Off. J. Balk. Union Oncol. 2010, 15, 153–156. [Google Scholar]
- Landmark, B.T.; Wahl, A. Living with newly diagnosed breast cancer: A qualitative study of 10 women with newly diagnosed breast cancer. J. Adv. Nurs. 2002, 40, 112–121. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Giovannini, L.; Muzzatti, B. Assessing the body image: Relevance, application and instruments for oncological settings. Support. Care Cancer 2012, 20, 901–907. [Google Scholar] [CrossRef]
- Przezdziecki, A.; Sherman, K.A.; Baillie, A.; Taylor, A.; Foley, E.; Stalgis-Bilinski, K. My changed body: Breast cancer, body image, distress and self-compassion. Psycho-Oncology 2013, 22, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Abrams, R.D.; Finesinger, J.E. Guilt reactions in patients with cancer. Cancer 1953, 6, 474–482. [Google Scholar] [CrossRef]
- Fafouti, M.; Paparrigopoulos, T.; Zervas, Y.; Rabavilas, A.; Malamos, N.; Liappas, I.; Tzavara, C. Depression, anxiety and general psychopathology in breast cancer patients: A cross-sectional control study. In Vivo 2010, 24, 803–810. [Google Scholar]
- Jurist, E.L. Mentalized affectivity. Psychoanal. Psychol. 2005, 22, 426. [Google Scholar] [CrossRef]
- Spiegel, D.; Kraemer, H.; Bloom, J.; Gottheil, E. Effect of psychosocial treatment on survival of patients with metastatic breast cancer. Lancet 1989, 334, 888–891. [Google Scholar] [CrossRef]
- Leszcz, M.; Goodwin, P.J. The Rationale and Foundations of Group Psychotherapy for Women with Metastatic Breast Cancer. Int. J. Group Psychother. 1998, 48, 245–273. [Google Scholar] [CrossRef]
- Sellick, S.M.; Crooks, D.L. Depression and cancer: An appraisal of the literature for prevalence, detection, and practice guideline development for psychological interventions. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 1999, 8, 315–333. [Google Scholar] [CrossRef]
- Singh, U.; Verma, N. Psychopathology among female breast cancer patients. J. Indian Acad. Appl. Psychol. 2007, 33, 61–71. [Google Scholar]
- Greimel, E.; Thiel, I.; Peintinger, F.; Cegnar, I.; Pongratz, E. Prospective assessment of quality of life of female cancer patients. Gynecol. Oncol. 2002, 85, 140–147. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, T.; Schlimme, J.E. Embodiment and psychopathology: A phenomenological perspective. Curr. Opin. Psychiatry 2009, 22, 570–575. [Google Scholar] [CrossRef]
- Bräuninger, I. The efficacy of dance movement therapy group on improvement of quality of life: A randomized controlled trial. Arts Psychother. 2012, 39, 296–303. [Google Scholar] [CrossRef]
- Bräuninger, I. Dance movement therapy group intervention in stress treatment: A randomized controlled trial (RCT). Arts Psychother. 2012, 39, 443–450. [Google Scholar] [CrossRef]
- Horwitz, E.B.; Theorell, T.; Anderberg, U.M. Fibromyalgia patients’ own experiences of video self-interpretation: A phenomenological-hermeneutic study. Scand. J. Caring Sci. 2003, 17, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.; Kunz, T.; Lykou, S.; Cruz, R. Effects of dance movement therapy and dance on health-related psychological outcomes: A meta-analysis. Arts Psychother. 2014, 41, 46–64. [Google Scholar] [CrossRef]
- Sharma, D.K.B. Dance/Movement Therapy (DMT) for Cancer Survivors and Caregivers in Fairbanks, Alaska; University of Alaska Fairbanks: Ann Arbor, MI, USA, 2016. [Google Scholar]
- Cohen, S.O.; Walco, G.A. Dance/movement therapy for children and adolescents with cancer. Cancer Pract. 1999, 7, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Dibbell-Hope, S. The use of dance/movement therapy in psychological adaptation to breast cancer. Arts Psychother. 2000, 27, 51–68. [Google Scholar] [CrossRef]
- Ho, R.T. Effects of dance movement therapy on Chinese cancer patients: A pilot study in Hong Kong. Arts Psychother. 2005, 32, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Sandel, S.L.; Judge, J.O.; Landry, N.; Faria, L.; Ouellette, R.; Majczak, M. Dance and movement program improves quality-of-life measures in breast cancer survivors. Cancer Nurs. 2005, 28, 301–309. [Google Scholar] [CrossRef]
- Serlin, I.A.; Classen, C.; Frances, B.; Angell, K. Symposium: Support groups for women with breast cancer: Traditional and alternative expressive approaches. Arts Psychother. 2000, 27, 123–138. [Google Scholar] [CrossRef]
- Ho, R.T.; Lo, P.H.; Luk, M.Y. A good time to dance? A mixed-methods approach of the effects of dance movement therapy for breast cancer patients during and after radiotherapy. Cancer Nurs. 2016, 39, 32–41. [Google Scholar] [CrossRef]
- Bradt, J.; Shim, M.; Goodill, S.W. Dance/movement therapy for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2015, 2015, CD007103. [Google Scholar]
- Goodill, S.W. Accumulating evidence for dance/movement therapy in cancer care. Front. Psychol. 2018, 9, 1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karathanou, I.; Bebetsos, E.; Filippou, F.; Psirri, A.; Konas, I. Greek Traditional Dance as a Practice for Managing Stress and Anxiety in Cancer Patients. J. Cancer Educ. 2021, 36, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Filippou, F.; Rokka, S.; Sivvas, G.; Pitsi, A.; Bebetsos, E.; Koupani, A.; Samara, E. Greek Traditional Dance Teaching Programs: Effects on the Quality of Life of Women who Survived Breast Cancer. Nosileftiki 2020, 59, 78–85. [Google Scholar]
- Derogatis, L.R. Symptom Checklist-90-Revised, Brief Symptom Inventory, and BSI-18. In Handbook of Psychological Assessment in Primary Care Settings; Taylor and Francis: Abingdon, UK, 2017. [Google Scholar]
- Chaiklin, S.; Schmais, C. The Chace approach to dance therapy. In Theoretical Approaches in Dance-Movement Therapy; Lewis, P., Ed.; Kendall/Hunt: Dubuque, IA, USA, 1986; Volume 1, pp. 17–36. [Google Scholar]
- Yalom, I.D. The Theory and Practice of Group Psychotherapy, 4th ed.; BasicBooks: New York, NY, USA, 1995. [Google Scholar]
- Schmais, C. Healing processes in group dance therapy. Am. J. Danc. Ther. 1985, 8, 17–36. [Google Scholar] [CrossRef]
- Sandel, S.; Chaiklin, S.; Lohn, A. Foundations of dance/movement therapy: The life and work of marian chace. Am. J. Danc. Ther. 1994, 16, 127–131. [Google Scholar]
- Levy, F.J. Dance/Movement Therapy: A Healing Art. 2nd Revised Edition 2005. Am. J. Danc. Ther. 2008, 30, 50–52. [Google Scholar]
- Samaritter, R. The use of metaphors in dance movement therapy. Body Mov. Danc. Psychother. 2009, 4, 33–43. [Google Scholar] [CrossRef]
- Bicego, D.; Brown, K.; Ruddick, M.; Storey, D.; Wong, C.; Harris, S.R. Effects of exercise on quality of life in women living with breast cancer: A systematic review. Breast J. 2009, 15, 45–51. [Google Scholar] [CrossRef]
- Fong, D.Y.; Ho, J.W.; Hui, B.P.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.; Cerin, E.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Physical activity for cancer survivors: Meta-analysis of randomised controlled trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef] [Green Version]
- Kaltsatou, A.; Mameletzi, D.; Douka, S. Physical and psychological benefits of a 24-week traditional dance program in breast cancer survivors. J. Bodyw. Mov. Ther. 2011, 15, 162–167. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).