Abstract
Background: This study focused on the widely used Body Image subscale, a dimension of the Body Investment Scale developed by Orbach and Mikulincer in 1998. Specifically, we explored its psychometric properties and potential use for health promotion research among young Spanish university students. Method: A sample of 793 participants (75.28% female) aged 18–26 years (M = 20.68; SD = 2.13) completed the questionnaire and related variables. Results: A unidimensional structure was confirmed with a good fit, demonstrating gender- and age-invariance, along with robust internal consistency. The scale exhibited a significant association with self-esteem, life satisfaction, a sense of coherence, and psychological distress. Conclusions: The Body Image subscale can be considered unidimensional. The obtained factor solution provides a reliable, valid, and invariant measure across gender and age for assessing body feelings in Spanish university students. Therefore, the instrument can effectively investigate the relationship between body image and health-related behaviors. Additionally, it can serve as a valuable tool in designing effective health interventions for university students to prevent mental health conditions, such as eating disorders or suicidal behaviors.
1. Introduction
In the late 1990s, Orbach and Mikulincer [1] broadened the understanding of body image to include emotions, attitudes, and satisfaction related to the body, as well as factors such as comfort with physical touch, protection from harm, and overall care for the body. This conceptualization gave rise to the development of the body investment concept, theorized to be linked with self-preservation, reflecting an attraction to life, and involving proactive measures for the care and protection of the body.
This expansion prompted extensive studies on this construct in relation to mental health issues. Previous research has established connections between body investment factors and suicide risk, distinguishing between suicidal and non-suicidal individuals [2,3,4], the onset of depressive symptoms [5], non-suicidal self-injury behaviors [6], and acting as a mediator between emotion dysregulation and gender dysphoria in adolescents [7]. Additionally, it has been associated with physical health conditions; studies post-surgery have indicated that wound dehiscence negatively impacts body investment [8].
To measure this construct, Orbach and Mikulincer [1] developed the Body Investment Scale (BIS), which is composed of four subscales, including body image feelings and attitude and body care (simplified as body image), body touch, body care, and body protection. However, this seminal work used an orthogonal rotation and a factorial structure, which has only been partially supported in posterior validation studies [2] and adaptations to other languages, such as Portuguese [9,10] or Spanish [11], where the factors were altered and correlated (oblique rotation), and some items covaried in models with the best fit. Moreover, other empirical studies used modified versions of the instrument with different structures of the subscales [8,12], whereas others have adapted the instrument to different languages based on their own translation-back-translation process [13,14,15] without exploring any psychometric properties of the adaptation. These factors make the obtained results opaque and difficult to compare with the results of other populations.
As a solution, some authors have used just the first subscale of the instrument, the Body Image (I-BIS), also called Body Feelings or Body Satisfaction, which measures the feelings that individuals experience regarding their own body and is closely related to body satisfaction.
The construct of body image has been shown to be a key mediator between physical activity and quality of life [16]. Moreover, an adverse perception of one’s body is indicative of reduced physical activity [17], poor dietary habits [18,19], and correlates with engaging in unsafe sexual practices [20] and smoking [21,22], among other factors. Consequently, addressing negative body image becomes imperative for health promotion efforts.
Conversely, a negative perception of one’s body has also been associated with the emergence and perpetuation of body dysmorphic disorder and eating disorders [23,24], alongside diminished self-esteem [25] and depressive symptoms [26,27], among others mental health issues.
Regarding the I-BIS instrument, Brausch and Muehlenkamp [28] found that scores of the I-BIS alone contributed substantially to the prediction of suicide-related behaviors. Thus, it does appear that the items on this particular scale tap into a useful construct, especially for making broad discriminations between suicidal and non-suicidal adolescents [2]. Furthermore, this subscale has demonstrated stable external validity and is the dimension with the highest reliability in the English, Portuguese, and Spanish versions [2,9,11]. The I-BIS has been utilized to explore the association between body image and eating disorder symptomatology in adolescents [13] and female athletes [29], the level of physical activity achieved among male and female adolescents [15], the probability of following a diet to lose weight [30], and to analyze its role as a mediator between patients with diabetic foot ulcers and their quality of life [12]. Nevertheless, there are no studies that support the validity, invariance, and reliability of this subscale for different populations and contexts.
Therefore, the present study aimed to analyze the psychometric properties of the I-BIS in a sample of young Spanish university students. This study provides evidence of its validity, including its factor solution, structural invariance, and relationships with other variables. Additionally, we estimated its reliability based on internal consistency.
2. Materials and Methods
2.1. Study Design and Participants
This study is a component of the Health Behavior in University (HBU) project, employing a cross-sectional survey approach. The data analyzed in this study were collected in the academic year 2018/2019. This project serves as a pilot study, aiming to comprehensively assess the lifestyles and various dimensions of health and human behavior among young Spanish university students.
The HBU study followed the core ethical principles set forth in the Declaration of Helsinki. Approval was granted by the Research Ethics Committee of Huelva Centers (CEI) of the Junta de Andalucía (0846-N-19/P1027/19), and the participants provided explicit permission through informed consent for the confidential and anonymous use and handling of their data. The research team was responsible for storing the data.
To enroll participants, a method of stratified random cluster sampling was utilized. Stratification, employing proportional allocation, was determined by area of study. Clusters of students from the first and third years were randomly chosen until the predetermined quota was reached for each area of study. The inclusion criteria mandated enrollment in a degree program at the University of Huelva and explicit consent for data processing. The exclusion criteria applied to international students (Erasmus) and individuals under the age of 18 years. Furthermore, students who had already participated were informed not to complete the survey again. This usually occurred when a student was enrolled in multiple courses that were selected for surveying. In cases of duplication due to this reason, these records were excluded from subsequent analysis to avoid redundancy. The study included almost 1000 students who consented to take part. After excluding those who did not complete the consent form, minors, age outliers within the university population, and participants/questionnaires with missing values, the final study sample consisted of 793 students. Among them, 75.28% identified as female and 24.72% as male, falling within the age range of 18 to 26 years (M = 20.68; SD = 2.13). The participants in the current study were distributed across various fields of study, including arts and humanities (6.05% of the sample), engineering and architecture (1.77%), natural sciences (2.27%), health sciences (42.12%), and, lastly, social and legal sciences, which constituted nearly half of the sample (47.79%).
Using R [31] to create random samples with quotas based on gender and age groups, approximately 50% of the cases were divided into two groups. The first group underwent Exploratory Factor Analysis (EFA), whereas the second group underwent Confirmatory Factor Analysis (CFA). Sub-sample 1 consisted of 394 participants and Sub-sample 2 consisted of 399 participants, with no statistically significant differences between the groups in terms of gender (χ2(1) < 0.001, p = 1) or age (t(790.72) = −0.3097, p = 0.757). Therefore, this data split ensured cross-validation of the results through two different methodological perspectives.
2.2. Instruments
The items comprising the subscale were chosen, along with other relevant variables pertinent to this research:
Body Image was measured using the Body Image (I-BIS) instrument extracted from the BIS [1]. The Spanish translation of this instrument was taken from the HBSC study in Spain [32]. This subscale consisted of 6 items with 5 Likert-type response options, where 1 represented “completely agree” and 5 represented “completely disagree”. The overall score consisted of the sum of each item, generating a range from 6 to 30 points, where a high score indicated more positive feelings about the body.
Self-esteem was assessed using Rosenberg’s Self-Esteem Scale (RSES), adapted to Spanish [33,34], focusing on overall self-esteem encompassing feelings of worthiness, adequacy, and self-respect. The scale used in this study consisted of 10 items rated on a 5-point Likert scale (1 = strongly agree to 5 = strongly disagree), with scores ranging from 10 to 50. This version has demonstrated adequate psychometric properties [35,36]. Higher scores indicated higher self-esteem. The reliability of the scale, measured via Cronbach’s Alpha, was α = 0.87.
Life satisfaction was evaluated using the Satisfaction with Life Scale (SWLS) [37] in Spanish [38], comprising five items rated on a scale from 1 to 5 (1 = “totally disagree” to 5 = “totally agree”). This scale has demonstrated adequate psychometric properties among Spanish university students [39], with a reliability coefficient of α = 0.84.
Sense of coherence was measured using the Spanish version of the Sense of Coherence Scale (SOC-13) developed by Antonovsky [40,41], which was obtained from the HBSC study [32]. This version consisted of 13 items rated on a 7-point Likert scale, assessing the frequency of certain experiences. Total scores range from 13 to 91 and can be analyzed as a single dimension. The reliability of the full scale, determined by Cronbach’s Alpha, was α = 0.80.
Psychological distress was assessed using the 12-item version of the General Health Questionnaire (GHQ-12) [42], adapted to Spanish [43,44]. The responses ranged from 0 = “No, not at all” to 3 = “Much more than usual”. Each item received a score of 0 (if options 1 or 2 were chosen) or 1 (if options 3 or 4 were chosen), resulting in a total score ranging from 0 to 12. The reliability of the instrument, as measured by Cronbach’s Alpha, was α = 0.86.
2.3. Statistical Analysis
First, descriptive analyses were conducted to determine the mean, standard deviation, range, skewness, and kurtosis of the instrument and its items. Additionally, ceiling and floor effects (when ≥15% of participants scored at the extremes of the scale) were assessed for the total scale score [45,46]. An analysis of the univariate and multivariate normality of the data was conducted to select the most adequate correlation matrix for the posterior analysis.
Then, Sub-sample 1 underwent exploratory factor analysis (EFA), preceded by the Kaiser–Meyer–Olkin (KMO) test for sample adequacy, Bartlett’s test of sphericity, and assessment of the determinant of the matrix. Subsequently, communalities were examined, and the most concise and reliable factorial solution was assessed using Optimal Coordinates, Acceleration Factor, Parallel Analysis, and Eigenvalues (Kaiser criterion).
To confirm the obtained solution, Sub-sample 2 underwent confirmatory factor analysis (CFA), evaluating fit measures, including the chi-square ratio (χ2/df), the comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). Threshold criteria were applied as follows: χ2/df ratio ≤ 3; CFI and TLI ≥ 0.90; and RMSEA and SRMR ≤ 0.08 [47].
A factor invariance analysis was conducted across gender and age groups on the entire sample. Invariance indicators were evaluated based on a −0.01 change in CFI, along with changes in RMSEA of +0.015 concerning the least restrictive model [48]. Progressive invariance was assessed across four models (configural, metric, scalar, and strict).
Internal consistency analyses were conducted using Ordinal alpha, Guttman split-half, and McDonald’s omega, and correlations between item scores and total subscale scores were analyzed for the overall sample, as well as for gender and age groups. Percent attenuation, due to the application of Cronbach’s alpha, was calculated for the subscale [49], enabling assessment of the degree to which the theoretical reliability of the underlying variable was underestimated.
Finally, to examine the external validity of evidence regarding the association of the subscale score with other variables, the Pearson correlation coefficient was utilized to describe the relationship between the I-BIS score and SOC-13, RSES, SWLS, and GHQ-12.
Data processing and analyses were conducted using R (Version 4.1.3) and the following packages were implemented: psycho (Version 0.6.1), psych (Version 2.2.3), MVN (Version 5.9), semPlot (Version 1.1.5), psychometric (Version 2.3), lavaan (Version 0.6.11.1676), and semTools (Version 0.5.6).
3. Results
3.1. Descriptive Analysis
Table 1 presents the means, standard deviations, minimum, maximum, skewness, and kurtosis of the six-item subscale. The original items and their Spanish translations can be found in Appendix A. Item 3 and Item 5 showed skewness and kurtosis outside the range of −1 and +1, whereas Item 1 exceeded the range only in kurtosis. Furthermore, the tests of multivariate skewness (z = 30.359, p < 0.001) and multivariate kurtosis (χ2(56) = 809.678, p < 0.001) were both statistically significant, indicating that the data did not follow univariate and multivariate normal distribution. Only 1.01% of participants scored at the lower extreme of the global score, and 6.68% scored at the upper extreme. Therefore, no floor or ceiling effect was identified.

Table 1.
Descriptive statistics of the I-BIS items.
3.2. Evidence of Validity Based on Factor Analysis
An EFA was conducted using the Unweighted Least Squares extraction method on a polychoric correlation matrix obtained from Sub-sample 1.
The appropriateness of the dataset to perform a factor analysis was verified using the KMO measure of sampling adequacy (0.88), sphericity Bartlett’s test (χ2 = 2608.022, p < 0.001), and a determinant equal to 0.001. The application of factor extraction methods revealed a one-factor structure, accounting for 78% of the variance. This model indicated that all factor loadings were ≥0.80, ranging from 0.84 (Item 6) to 0.91 (Item 3 and Item 5), and communality was equal to or higher than 0.70 for all the cases (Table 2).
Table 2.
Pattern matrix based on the polychoric matrix using Unweighted Least Squares.
In order to confirm the structure obtained using the EFA, a CFA was performed using Sub-sample 2. The unidimensional model showed adequate goodness of fit regarding its indexes (χ2/df = 1.588; CFI = 0.998, TLI = 0.997; RMSEA = 0.038, 90% CI [0, 0.074]; SRMR = 0.041). The standardized weights for both models are shown in Figure 1.
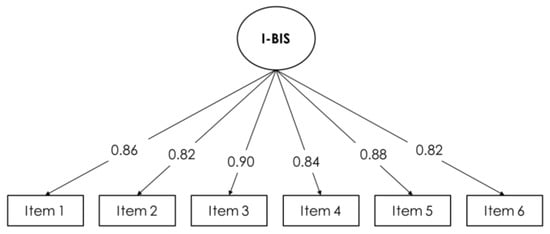
Figure 1.
Path diagram for the one-dimensional model in the confirmatory factor analysis. Standardized weights are provided.
The full sample was utilized to examine gender and age group invariance. As shown in Table 3, no reductions in CFI exceeding −0.01 and no increases in RMSEA beyond 0.015 were observed. Consequently, measurement invariance was confirmed across all the sub-samples. Hence, a strict level of invariance was established for the tested model, irrespective of gender and age differences.
Table 3.
Goodness of fit indexes for the different steps of the factorial invariance analysis.
3.3. Evidence of Reliability Based on Internal Consistency
All items have corrected Item Total correlations, ranging from 0.86 (Item 6) to 0.91 (Item 3 and Item 5).
The 6-item subscale exhibited an ordinal alpha of 0.95 (95% confidence interval: 0.84–0.99), whereas Cronbach’s alpha for the same items was 0.92, indicating an attenuation effect of −2.97. A McDonald’s omega value of 0.95 and an average Guttman Coefficient value of 0.95 (min = 0.92; max= 0.96) were observed. The removal of any of the items did not improve either the Item Total correlations or the internal consistency of the subscale.
Additionally, the subscale exhibited a robust internal consistency across gender and age groups (Table 4). There were no statistically significant differences in ordinal alpha, and the removal of any item did not result in an improvement in any of the sub-samples.
Table 4.
Internal consistency coefficient by gender and age group.
3.4. Evidence of External Validity Based on the Relationship with Other Constructs
External validity was assessed by examining the correlation between the total I-BIS score and the other constructs of theoretical relevance. The correlation matrix, displayed in Table 5, reveals positive and significant relationships (p < 0.001) between the instrument’s total score and RSES, SWLS, and SOC-13 scores, whereas a negative relationship was observed with the GHQ-12 score.
Table 5.
Correlations between I-BIS subscale scores and other constructs.
4. Discussion
The present study aimed to evaluate the psychometric properties of the Spanish version of the I-BIS, a subscale of the BIS developed by Orbach and Mikulincer [1]. The I-BIS assesses individuals’ feelings and attitudes towards their own bodies, reflecting their satisfaction with their bodies. This research provides evidence of the scale’s validity and estimates the reliability of the Spanish version of the I-BIS in a sample of university students.
Concerning the instrument’s validity, the items of the original subscale underwent reduction through exploratory factor analysis (EFA), revealing a resulting scale with a unidimensional structure. Cross-validation of these initial results was obtained through a confirmatory factor analysis (CFA), which supported the existence of this structure. It was found to be invariant across gender and age. These findings enable the comparison of scores with outcomes from non-clinical populations, addressing the gap left by the study conducted by Marco et al. [11], which focused solely on females with eating disorders and employed a 7-item I-BIS. Even with three reverse-scored items included in the total score computation, no wording effects were detected. This suggests that the scale effectively captured changes in body satisfaction within the same continuum. Additionally, this unidimensional factorial solution demonstrated invariance across gender and age. Thus, the current study supports the notion that gender differences in body image, where females tended to have a more negative perception of their bodies compared to males [16,50], and its association with adherence to weight loss diets, as found by Ramos et al. [30], are attributed to sample variations rather than issues with the instrument. Hence, employing this tool could be beneficial in upcoming research endeavors for identifying unhealthy attitudes, such as bulimia and anorexia, stemming from discontent with self-image, particularly concerning aspects related to body weight, as observed in previous studies involving women [51].
The instrument also exhibited good reliability, as evidenced by its internal consistency indexes (Cronbach’s Alpha, McDonald’s Omega, and split-half Gutman coefficients in their ordinal version, calculated based on the polychoric correlation of the items) across the entire sample and in subsequent sub-samples stratified by gender and age. These findings align with results from prior studies involving both clinical and non-clinical samples [2,9,11].
Furthermore, meaningful correlations with relevant constructs related to well-being and health were identified. The robust positive correlation with SOC and SWLS aligns with the hypothesis that the instrument can be valuable in exploring the role of bodily experiences in self-enhancement, health-promoting behavior, and coping with physical illness, as proposed by Orbach and Mikulincer [1]. These results are in line with previous studies indicating that developing a perception of body image is essential to improve the quality of life of the population [16]. Simultaneously, the strong positive association with self-esteem and the negative association with psychological distress support the proposition that dissatisfaction with one’s appearance may serve as a symptom of a more severe disorder. This dissatisfaction could potentially lead to a decline in overall self-esteem, contributing to feelings of alienation, depression, engagement in risky behavior, and the development of eating disorders [15].
The I-BIS may be useful not only in assessing the effectiveness of interventions for improving body image [52], but also in evaluating interventions and technologies aimed at promoting physical exercise [53], given its strong relationship with a more positive body image [16]. Additionally, it could be valuable in developing new methodologies to understand the mechanisms underlying body image disturbances and subsequently designing innovative and effective interventions [54].
This study has several limitations that should be acknowledged. Firstly, all data were collected using self-administered instruments in a cross-sectional design. Although efforts were made to mitigate potential biases through voluntary participation and ensuring that the participants were informed in advance about data confidentiality, additional longitudinal studies would be valuable to observe the test–retest reliability of the instrument and to explore differences between body image as a state and as a trend.
It is important to highlight that the results stem from a sample of Spanish university students without clinical backgrounds. The applicability of these findings to other groups, including children, high school students, or employed adults, cannot be assured. Hence, additional research involving these demographics is warranted.
On the other hand, to the best of our knowledge, this is the first study to assess the psychometric properties, including factorial structure, gender- and age-invariance, and reliability, of the I-BIS extracted from the BIS developed by Orbach and Mikulincer [1]. The results demonstrate that the instrument maintains invariance across gender and age differences, confirming its stability and applicability within the university community. Moreover, the instrument’s specificity and brevity enable its integration into more complex research, facilitating the close monitoring of mental health issues or serving as a focal point for interventions in health promotion programs.
Future research should adopt a network analysis perspective to understand the role of body feelings in connection with other psychological constructs and health behaviors, addressing the complexity of these interactions within more comprehensive models.
5. Conclusions
In conclusion, the findings demonstrate that the Spanish version of the Body Image dimension in the Body Investment Scale (I-BIS) is a valid and invariant measure across gender and age, exhibiting reliability for use among Spanish university students. Consequently, this instrument effectively investigates the relationship between body image and health-related behaviors connected to psychological constructs, such as psychological distress, a sense of coherence, self-esteem, or satisfaction with life. Additionally, it can serve as a valuable tool in designing effective health interventions for university students to prevent mental health conditions, such as eating disorders or suicidal behaviors, among others. Body image has been shown to be a key factor in the physical and mental health of the population, which makes its adequate assessment essential to build a better understanding of its role in public health.
Author Contributions
Conceptualization, D.D.-M.; methodology, D.D.-M. and P.J.P.-M.; formal analysis, D.D.-M.; investigation, D.D.-M. and P.J.P.-M.; data curation, D.D.-M.; writing—original draft preparation, D.D.-M.; writing—review and editing, D.D.-M., C.S.V., M.A.-V., A.S.-B. and P.J.P.-M.; supervision, C.S.V., M.A.-V. and P.J.P.-M.; funding acquisition, M.A.-V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the EPIT 2020 project (University of Huelva, Spain) under Grant UHU-6272020.
Institutional Review Board Statement
This research adhered to the principles outlined in the Declaration of Helsinki and received approval from the Ethics Committee of Huelva Centers (CEI) of the Junta de Andalucía (protocol code 0846-N-19/P1027/19) on the 24 September 2019.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors have no competing interests to declare. The funders played no part in designing the study, collecting, analyzing, or interpreting data, writing the manuscript, or deciding to publish the findings.
Appendix A
Table A1.
Definition of I-BIS items in Spanish and English.
Table A1.
Definition of I-BIS items in Spanish and English.
| Item | Spanish | English |
|---|---|---|
| 1 | Me siento frustrado/a con mi apariencia física | I am frustrated with my physical appearance |
| 2 | Estoy satisfecho/a con mi apariencia | I am satisfied with my appearance |
| 3 | Odio mi cuerpo | I hate my body |
| 4 | Me siento cómodo/a con mi cuerpo | I feel comfortable with my body |
| 5 | Desprecio mi cuerpo | I feel anger toward my body |
| 6 | Me gusta mi apariencia a pesar de mis defectos | I like my appearance in spite of its imperfections |
References
- Orbach, I.; Mikulincer, M. The Body Investment Scale: Construction and Validation of a Body Experience Scale. Psychol. Assess. 1998, 10, 415–425. [Google Scholar] [CrossRef]
- Osman, A.; Gutierrez, P.M.; Schweers, R.; Fang, Q.; Holguin-Mills, R.L.; Cashin, M. Psychometric Evaluation of the Body Investment Scale for Use with Adolescents. J. Clin. Psychol. 2010, 66, 259–276. [Google Scholar] [CrossRef]
- Orbach, I.; Gilboa-Schechtman, E.; Sheffer, A.; Meged, S.; Har-Even, D.; Stein, D. Negative Bodily Self in Suicide Attempters. Suicide Life-Threat. Behav. 2006, 36, 136–153. [Google Scholar] [CrossRef]
- Brausch, A.M.; Nichols, P.M.; Laves, E.H.; Clapham, R.B. Body Investment as a Protective Factor in the Relationship Between Acquired Capability for Suicide and Suicide Attempts. Behav. Ther. 2021, 52, 1114–1122. [Google Scholar] [CrossRef]
- Lamis, D.A.; Malone, P.S.; Langhinrichsen-Rohling, J.; Ellis, T.E. Body Investment, Depression, and Alcohol Use as Risk Factors for Suicide Proneness in College Students. Crisis 2010, 31, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Muehlenkamp, J.J.; Brausch, A.M. Body Image as a Mediator of Non-Suicidal Self-Injury in Adolescents. J. Adolesc. 2012, 35, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Petruzzelli, M.G.; Margari, L.; Furente, F.; Marzulli, L.; Piarulli, F.M.; Margari, A.; Ivagnes, S.; Lavorato, E.; Matera, E. Body Emotional Investment and Emotion Dysregulation in a Sample of Adolescents with Gender Dysphoria Seeking Sex Reassignment. J. Clin. Med. 2022, 11, 3314. [Google Scholar] [CrossRef] [PubMed]
- De Lima, E.L.; De Brito, M.J.A.; Da Cunha, J.B.; Duarte, M.F.P.; Correâ, N.F.M.H.; De Carvalho Resende, M.M.; Ferreira, L.M. The Impact of Surgical Wound Dehiscence on Body Image. Adv. Ski. Wound Care 2018, 31, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.I.; Fernandes, J.; Machado, P.P.P.; Gonçalves, S. The Portuguese Version of the Body Investment Scale: Psychometric Properties and Relationships with Disordered Eating and Emotion Dysregulation. J. Eat. Disord. 2020, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, V.V.; Santos, C.A.; Gouveia, R.S.V.; Santos, W.; Pronk, S.L. Escala de Investimento Corporal (BIS)—Evidencias de Sua Validade Fatorial e Consistência Interna. Avaliação Psicológica 2008, 7, 57–66. [Google Scholar]
- Marco, J.H.; Cañabate, M.; García-Alandete, J.; Llorca, G.; Real-López, M.; Beltrán, M.; Pérez, S. Body Image and Nonsuicidal Self-Injury: Validation of the Body Investment Scale in Participants with Eating Disorders. Clin. Psychol. Psychother. 2018, 25, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Putri, N.M.M.E.; Yasmara, D.; Yen, M.F.; Pan, S.C.; Fang, S.Y. Body Image as a Mediator Between Gender and Quality of Life Among Patients with Diabetic Foot Ulcers in Indonesia. J. Transcult. Nurs. 2021, 32, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Palmeroni, N.; Luyckx, K.; Verschueren, M.; Claes, L. Body Dissatisfaction as a Mediator between Identity Formation and Eating Disorder Symptomatology in Adolescents and Emerging Adults. Psychol. Belg. 2020, 60, 328–346. [Google Scholar] [CrossRef] [PubMed]
- García-Alandete, J.; Ros, M.C.; Salvador, J.H.M.; Rodríguez, S.P. Psychometric Properties of the Purpose-In-Life Test and Age-Related Differences among Women Diagnosed with Eating Disorders. Psychiatry Res. 2018, 261, 161–167. [Google Scholar] [CrossRef]
- Kołoło, H.; Guszkowska, M.; Mazur, J.; Dzielska, A. Self-Efficacy, Self-Esteem and Body Image as Psychological Determinants of 15-Year-Old Adolescents’ Physical Activity Levels. Hum. Mov. 2012, 13, 264–270. [Google Scholar] [CrossRef]
- Nayir, T.; Uskun, E.; Yürekli, M.V.; Devran, H.; Çelik, A.; Okyay, R.A. Does Body Image Affect Quality of Life?: A Population Based Study. PLoS ONE 2016, 11, e0163290. [Google Scholar] [CrossRef]
- Moreno-Díaz, M.I.; Vaquero-Solís, M.; Tapia-Serrano, M.Á.; Sánchez-Miguel, P.A. Physical Activity, Body Composition, Physical Fitness, and Body Dissatisfaction in Physical Education of Extremadura Adolescents: An Exploratory Study. Children 2024, 11, 83. [Google Scholar] [CrossRef]
- Zhang, T.; Wang, K.; Gu, T.; Zhang, Y.; Zhang, X. Body Dissatisfaction and Restricted Diet in Chinese Adolescents: A Longitudinal Analysis. Psychol. Res. Behav. Manag. 2023, 16, 4003–4013. [Google Scholar] [CrossRef]
- Łebek, E.; Knapik, A. Body Image and Physical Activity and the Diet of Polish Youth Aged 15–18. Int. J. Environ. Res. Public Health 2023, 20, 3213. [Google Scholar] [CrossRef]
- Schooler, D. Early Adolescent Body Image Predicts Subsequent Condom Use Behavior among Girls. Sex. Res. Soc. Policy 2013, 10, 52–61. [Google Scholar] [CrossRef]
- Coniglio, K.A.; Rosen, R.; Burr, E.K.; Farris, S.G. Adherence to Low-Calorie and Low-Sugar Diets Is Uniquely Associated with Distinct Facets of Appearance/Weight-Related Smoking Motivations. J. Behav. Med. 2020, 43, 487–492. [Google Scholar] [CrossRef]
- Gonçalves, L.; Zanlorenci, S.; Borges, L.L.; de Lima, T.R.; Silva, D.A.S. Body Weight Dissatisfaction and Health Risk Behaviors in Adolescents. Percept. Mot. Skills 2023, 130, 340–363. [Google Scholar] [CrossRef]
- Cornelissen, P.L.; Tovée, M.J. Targeting Body Image in Eating Disorders. Curr. Opin. Psychol. 2021, 41, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Mölbert, S.C.; Klein, L.; Thaler, A.; Mohler, B.J.; Brozzo, C.; Martus, P.; Karnath, H.O.; Zipfel, S.; Giel, K.E. Depictive and Metric Body Size Estimation in Anorexia Nervosa and Bulimia Nervosa: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2017, 57, 21–31. [Google Scholar] [CrossRef]
- De Coen, J.; Verbeken, S.; Goossens, L. Body Dissatisfaction and Low Self-Esteem in Elementary School-Aged Children: The Role of Media Pressure and Trust in Parent–Child Relationships. Front. Psychol. 2023, 14, 1228860. [Google Scholar] [CrossRef]
- Wang, X.; Lu, C.; Niu, L. Body Image Construction and Mental Health Levels among College Students: A Data Survey of Chinese University Students. Front. Public Health 2023, 11, 1268775. [Google Scholar] [CrossRef] [PubMed]
- Paxton, S.J.; Neumark-Sztainer, D.; Hannan, P.J.; Eisenberg, M.E. Body Dissatisfaction Prospectively Predicts Depressive Mood and Low Self-Esteem in Adolescent Girls and Boys. J. Clin. Child Adolesc. Psychol. 2006, 35, 539–549. [Google Scholar] [CrossRef]
- Brausch, A.M.; Muehlenkamp, J.J. Body Image and Suicidal Ideation in Adolescents. Body Image 2007, 4, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Borowiec, J.; Banio-Krajnik, A.; Malchrowicz-Mośko, E.; Kantanista, A. Eating Disorder Risk in Adolescent and Adult Female Athletes: The Role of Body Satisfaction, Sport Type, BMI, Level of Competition, and Training Background. BMC Sports Sci. Med. Rehabil. 2023, 15, 91. [Google Scholar] [CrossRef]
- Ramos, P.; Rivera, F.; Pérez, R.S.; Lara, L.; Moreno, C. Diferencias de Género En La Imagen Corporal y Su Importancia En El Control de Peso. Escritos Psicol. Psychol. Writ. 2016, 9, 42–50. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. Available online: https://www.r-project.org/ (accessed on 6 May 2019).
- Moreno, C.; Ramos, P.; Rivera, F.; Jiménez-Iglesias, A.; García-Moya, I.; Sánchez-Queija, I.; Moreno-Maldonado, C.; Paniagua, C.; Villafuerte-Díaz, A.; Ciria-Barreiro, E.; et al. Informe Técnico de Los Resultados Obtenidos Por El Estudio Health Behaviour in School-Aged Children (HBSC) 2018 En España; Ministerio de Sanidad: Madrid, Spain, 2020. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image. Soc. Forces 1965, 44, 255–256. [Google Scholar] [CrossRef]
- Martín-Albo, J.; Núñez, J.L.; Navarro, J.G.; Grijalvo, F. The Rosenberg Self-Esteem Scale: Translation and Validation in University Students. Span. J. Psychol. 2007, 10, 458–467. [Google Scholar] [CrossRef]
- Leung, S.-O. A Comparison of Psychometric Properties and Normality in 4-, 5-, 6-, and 11-Point Likert Scales. J. Soc. Serv. Res. 2011, 37, 412–421. [Google Scholar] [CrossRef]
- Dobson, C.; Goudy, W.J.; Keith, P.M.; Powers, E. Further Analysis of Rosenberg’s Self-Esteem Scale. Psychol. Rep. 1979, 44, 639–641. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Atienza, F.L.; Pons, D.; Balaguer, I.; García-Merita, M. Propiedades Psicométricas de La Escala de Satisfacción Con La Vida En Adolescentes. Psicothema 2000, 12, 314–319. [Google Scholar]
- Diaz-Milanes, D.; Salado, V.; Santín Vilariño, C.; Andrés-Villas, M.; Pérez-Moreno, P.J. A Network Analysis Study on the Structure and Gender Invariance of the Satisfaction with Life Scale among Spanish University Students. Healthcare 2024, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Antonovsky, A. The Structure and Properties of the Sense of Coherence Scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Sánchez-López, M.d.P.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Reliability, External Validity and Factor Structure in the Spanish Population. Psicothema 2008, 20, 839–843. [Google Scholar] [PubMed]
- Rocha, K.B.; Pérez, K.; Rodríguez-Sanz, M.; Borrell, C.; Obiols, J.E. Propiedades Psicométricas y Valores Normativos Del General Health Questionnaire (GHQ-12) En Población General Española. Int. J. Clin. Health Psychol. 2011, 11, 125–139. [Google Scholar]
- McHorney, C.A.; Tarlov, A.R. Individual-Patient Monitoring in Clinical Practice: Are Available Health Status Surveys Adequate? Qual. Life Res. 1995, 4, 293–307. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Gadermann, A.M.; Guhn, M.; Zumbo, B.D. Estimating Ordinal Reliability for Likert-Type and Ordinal Item Response Data: A Conceptual, Empirical, and Practical Guide. Pract. Assess. Res. Eval. 2012, 17, 3. [Google Scholar]
- Unterhalter, G.; Farrell, S.; Mohr, C. Selective Memory Biases for Words Reflecting Sex-Specific Body Image Concerns. Eat. Behav. 2007, 8, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Porto, D.B.; de Azevedo, B.G.; de Melo, D.G.; Christofaro, D.G.D.; Codogno, J.S.; da Silva, C.B.; Fernandes, R.A. Fatores Associados à Autoavaliação Do Peso Corporal Em Mulheres Praticantes de Academia. Rev. Bras. Cineantropometria Desempenho Hum. 2015, 17, 175. [Google Scholar] [CrossRef]
- Alleva, J.M.; Sheeran, P.; Webb, T.L.; Martijn, C.; Miles, E. A Meta-Analytic Review of Stand-Alone Interventions to Improve Body Image. PLoS ONE 2015, 10, e0139177. [Google Scholar] [CrossRef]
- Rick, P.; Sánchez-Martín, M.; Singh, A.; Navas-León, S.; Borda-Mas, M.; Bianchi-Berthouze, N.; Tajadura-Jiménez, A. Investigating Psychological Variables for Technologies Promoting Physical Activity. Digit. Health 2022, 8, 20552076221116559. [Google Scholar]
- Navas-León, S.; Morales Márquez, L.; Sánchez-Martín, M.; Crucianelli, L.; Bianchi-Berthouze, N.; Borda-Mas, M.; Tajadura-Jiménez, A. Exploring Multisensory Integration of Non-Naturalistic Sounds on Body Perception in Young Females with Eating Disorders Symptomatology: A Study Protocol. J. Eat. Disord. 2023, 11, 28. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).