
Comparative Analysis of the Six-Strand Hamstring and Peroneus Longus in Sports Medicine and Rehabilitation


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
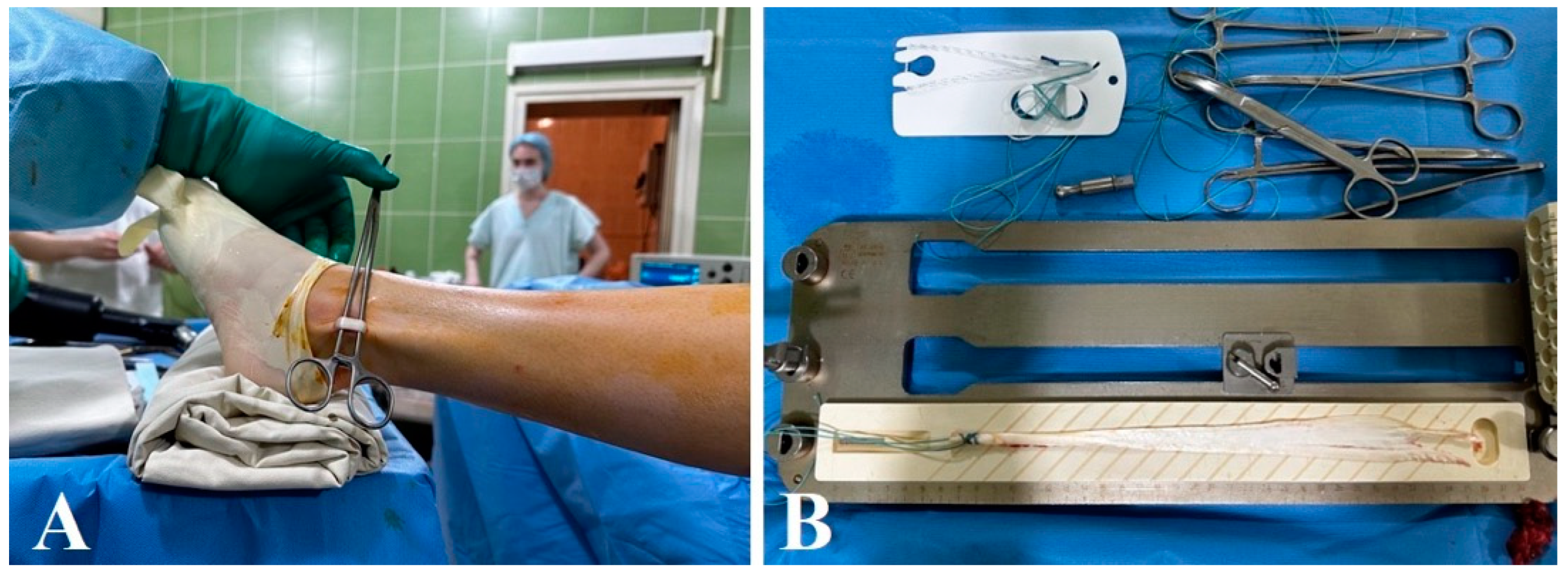
2.2. Surgical Technique
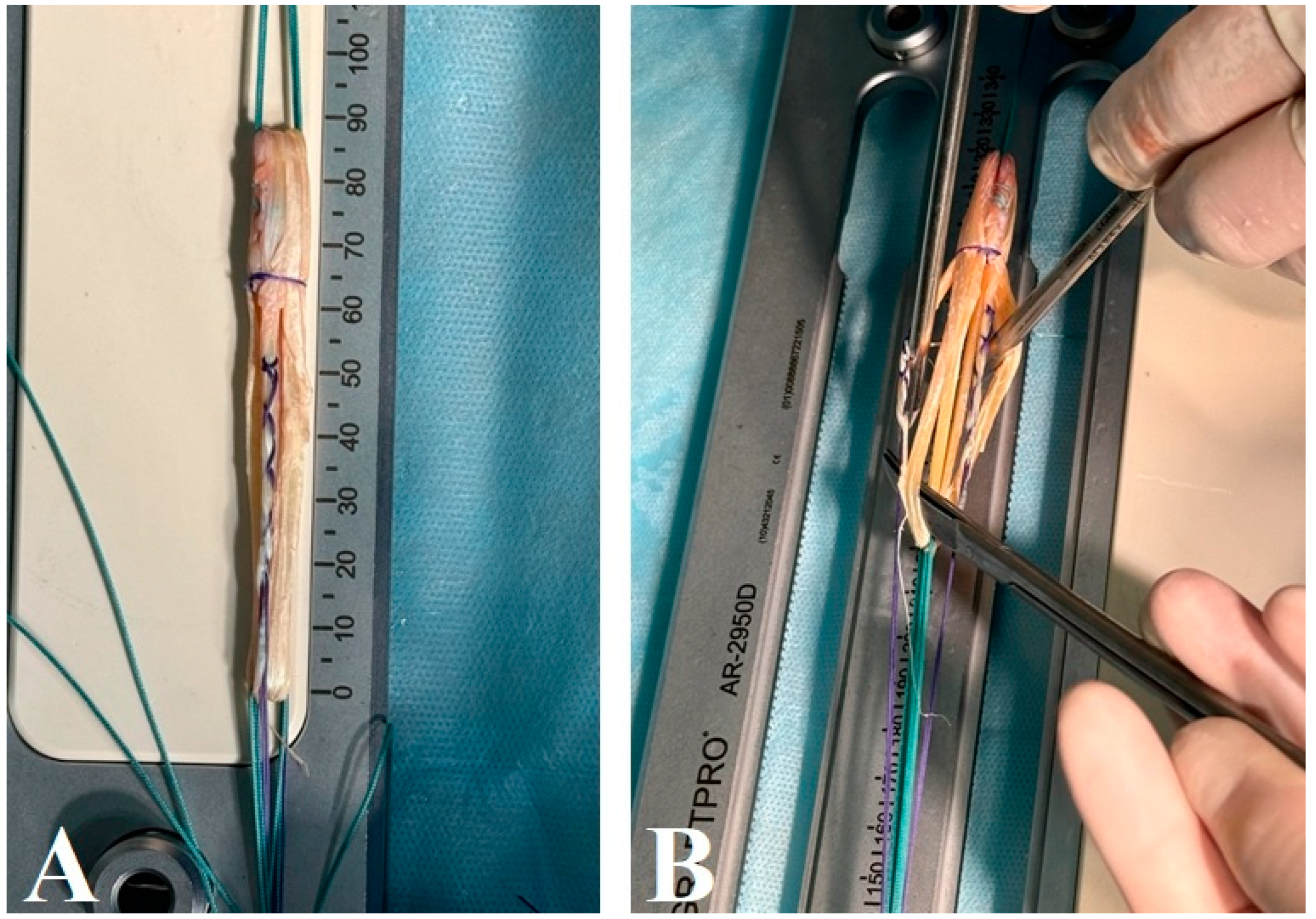
2.3. Hamstring Graft
2.4. Postoperative Care and Rehabilitation
- Early mobilization: Patients were encouraged to begin weight-bearing and knee flexion exercises starting the day after surgery. The goal was to achieve a minimum knee flexion angle of 90 degrees by the sixth week postoperatively.
- Rehabilitation program: A structured rehabilitation program was implemented for all patients. This program focused on quadriceps and hamstring strengthening exercises, stationary cycling, and a gradual return to sports activities. The exercises were tailored to enhance muscle strength, improve joint flexibility, and support the overall recovery process.
- Physical therapy: Patients were advised to avoid activities that could place undue strain on the graft, such as sharp turns or high-impact sports, until their recovery was sufficiently advanced. The rehabilitation plans included specific exercises to restore their full range of motion and strength while protecting the surgical site.
- Return to sports: A cautious return to sports activities was recommended around six months postoperatively, once full recovery of muscle strength and knee stability had been achieved. For high-impact activities, knee band support was advised for up to one year to provide additional protection.
2.5. Functional Assessment
2.6. Statistical Analysis
2.7. Rehabilitation
3. Results
4. Discussion
4.1. Clinical Outcomes and Functional Assessments
4.2. Anterior Drawer Test and Lachman’s Test
4.3. Surgical and Rehabilitation Protocols
4.4. Complications and Donor Site Morbidity
4.5. Biomechanical Efficacy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Graft Type | Advantages | Disadvantages |
|---|---|---|
| Six-strand hamstring tendon [1,17,29,47] |
|
|
| Peroneus longus tendon [5,7,34,48] |
|
|
| Bone-patellar tendon-bone (BPTB) [1,24,29] |
|
|
| Quadriceps tendon [22,38,49] |
|
|
| Allografts (donor tissue) [23,28,52] |
|
|
4.6. Future Directions
4.7. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goncharov, E.N.; Koval, O.A.; Bezuglov, E.N.; Vetoshkin, A.A.; Goncharov, N.G.; Ramirez, M.E.; Nurmukhametov, R.; Montemurro, N. Outcome of Primary Anterior Cruciate Ligament Reconstruction with Peroneus Longus and Bone–Patellar Tendon–Bone Autografts: A Clinical Comparative Study. Surgeries 2023, 4, 434–445. [Google Scholar] [CrossRef]
- Evans, J.; Nielson, J.L. Anterior Cruciate Ligament Knee Injuries. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Volume 2, p. 1. [Google Scholar]
- Ingram, J.G.; Fields, S.K.; Yard, E.E.; Comstock, R.D. Epidemiology of knee injuries among boys and girls in us high school athletics. Am. J. Sports Med. 2008, 36, 1116–1122. [Google Scholar] [CrossRef]
- Powell, J.W.; Barber-Foss, K.D. Injury patterns in selected high school sports: A review of the 1995–1997 seasons. J. Athl. Train. 1999, 34, 277–284. [Google Scholar]
- Risberg, M.A.; Lewek, M.; Snyder-Mackler, L. A systematic review of evidence for anterior cruciate ligament rehabilitation: How much and what type? Phys. Ther. Sport 2004, 5, 125–145. [Google Scholar] [CrossRef]
- Teitz, C.C.; Hu, S.S.; Arendt, E.A. The female athlete: Evaluation and treatment of sports-related problems. J. Am. Acad. Orthop. Surg. 1997, 5, 87–96. [Google Scholar] [CrossRef]
- Nicolini, A.; Teixeira De Carvalho, R.; Matsuda, M. Common injuries in athletes’ knee: Experience of a specialised centre. Acta Ortop. Bras. 2014, 22, 127–131. [Google Scholar] [CrossRef]
- Salmon, L.; Russell, V.; Musgrove, T.; Pinczewski, L.; Refshauge, K. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 948–957. [Google Scholar] [CrossRef]
- Oiestad, B.; Engebretsen, L.; Storheim, K.; Risberg, M.A. Knee osteoarthritis after anterior cruciate ligament injury: A systematic re-view. Am. J. Sports Med. 2009, 37, 1434–1443. [Google Scholar] [PubMed]
- Roos, H.; Adalberth, T.; Dahlberg, L.; Lohmander, L.S. Osteoarthritis of the knee after injury to the anterior cruciate ligament or meniscus: The influence of time and age. Osteoarthr. Cartil. 1995, 3, 261–267. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Preventing Injuries in Sports, Recreation and Exercise; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2006; Volume 2, p. 1. [Google Scholar]
- Hartnett, N.; Tregonning, R.J. Delay in diagnosis of anterior cruciate ligament injury in sport. N. Z. Med. J. 2001, 114, 11–13. [Google Scholar]
- Khan, T.; Alvand, A.; Prieto-Alhambra, D.; Culliford, D.J.; Judge, A.; Jackson, W.F.; Scammell, B.E.; Arden, N.K.; Price, A.J. ACL and meniscal injuries increase the risk of primary total knee replacement for osteoarthritis: A matched case–control study using the Clinical Practice Re-search Datalink (CPRD). Br. J. Sports Med. 2019, 53, 965–968. [Google Scholar] [CrossRef]
- Eggerding, V.; Reijman, M.; Meufels, D.E.; van Es, E.; van Arkel, E.; van den Brand, I.; van Linge, J.; Zijl, J.; Bierma-Zeinstra, S.M.; Koopmanschap, M. ACL reconstruction for all is not cost-efective after acute ACL rupture. Br. J. Sports Med. 2021, 1, 1. [Google Scholar]
- Ardern, C.L.; Kvist, J.; Webster, K.E. Psychological aspects of anterior cruciate ligament injuries. Oper. Technol. Sports Med. 2016, 24, 77–83. [Google Scholar] [CrossRef]
- Kumar, R.; Singh, B.; Gautam, A. Single Bundle ACL Reconstruction with Peroneus Longus Tendon Autograft: A Short-Term Study. Available online: http://ejmcm.com/uploads/paper/c615b9004c2996925882b832ca439e2b.pdf (accessed on 1 April 2024).
- Rhatomy, S.; Asikin, A.I.Z.; Wardani, A.E.; Rukmoyo, T.; Lumban-Gaol, I.; Budhiparama, N.C. Peroneus longus autograft can be rec-ommended as a superior graft to hamstring tendon in single-bundle ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3552–3559. [Google Scholar] [CrossRef] [PubMed]
- Rudy, M.E.; Phatama, K.Y. Tensile strength comparison between peroneus longus and hamstring tendons: A biomechanical study. Int. J. Surg. Open 2017, 9, 41–44. [Google Scholar] [CrossRef]
- Laoruengthana, A.; Pattayakorn, S.; Chotanaputhi, T.; Kosiyatrakul, A. Clinical comparison between six-strand hamstring tendon and patellar tendon autograft in arthroscopic anterior cruciate ligament reconstruction: A prospective, randomized clinical trial. J. Med. Assoc. Thail. 2009, 92, 491–497. [Google Scholar]
- Migliorini, F.; Torsiello, E.; Trivellas, A.; Eschweiler, J.; Hildebrand, F.; Maffulli, N. Bone-patellar tendon-bone versus two- and four-strand hamstring tendon auto-grafts for ACL reconstruction in young adults: A Bayesian network meta-analysis. Sci. Rep. 2023, 13, 6883. [Google Scholar] [CrossRef]
- Urchek, R.; Karas, S. Biomechanical Comparison of Quadriceps and 6-Strand Hamstring Tendon Grafts in Anterior Cruciate Ligament Reconstruction. Orthop. J. Sports Med. 2019, 7, 2325967119879113. [Google Scholar] [CrossRef]
- Grassi, A.; Agostinone, P.; Di Paolo, S.; Altovino, E.; Gallese, A.; Akbaba, D.; Bonanzinga, T.; Marcacci, M.; Zaffagnini, S. Donor age has no relevant role in biomechanical properties of allografts used in anterior cruciate ligament (ACL) reconstruction: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2024, 32, 1123–1142. [Google Scholar] [CrossRef]
- DeFazio, M.W.; Curry, E.J.; Gustin, M.J.; Sing, D.C.; Abdul-Rassoul, H.; Ma, R.; Fu, F.; Li, X. Return to Sport After ACL Reconstruction With a BTB Versus Hamstring Tendon Autograft: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2020, 8, 2325967120964919. [Google Scholar] [CrossRef]
- Lin, K.M.; Boyle, C.B.; Marom, N.; Marx, R.G. Graft Selection in Anterior Cruciate Ligament Reconstruction. Sports Med. Arthrosc. Rev. 2020, 28, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Avasthi, S.; Aggarwal, P.; Mahapatra, S.; Nishat, N.; Mishra, M.; Aslam, A. Diagnostic accuracy of lever sign test in acute and chronic acl injuries. J. Clin. Orthop. Trauma 2024, 52, 102427. [Google Scholar] [CrossRef] [PubMed]
- Nazari, G.; Barton, K.I.; Bryant, D.; Getgood, A.; Brown, C.H. Five- and six-strand hamstring grafts consistently produce appropriate graft diameters for anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2020, 29, 2940–2947. [Google Scholar] [CrossRef]
- Attia, A.K.; Nasef, H.; ElSweify, K.H.; Adam, M.A.; AbuShaaban, F.; Arun, K. Failure Rates of 5-Strand and 6-Strand vs Quadrupled Hamstring Autograft ACL Reconstruction: A Comparative Study of 413 Patients with a Minimum 2-Year Follow-up. Orthop. J. Sports Med. 2020, 8, 2325967120946326. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Kwaees, T.A.; Thomas, T.; Pydisetty, R. Cohort study of short-term outcomes after ACL-reconstruction using au-tograft with internal brace reinforcement versus isolated autograft demonstrating no significant difference. J. Orthop. 2023, 43, 115–120. [Google Scholar] [CrossRef]
- Hardy, A.; Casabianca, L.; Andrieu, K.; Baverel, L.; Noailles, T.; Junior French Arthroscopy Society. Complications following har-vesting of patellar tendon or hamstring tendon grafts for anterior cruciate ligament reconstruction: Systematic review of literature. Orthop. Traumatol. Surg. Res. 2017, 103, S245–S248. [Google Scholar] [CrossRef]
- Noyes, F.R.; Huser, L.E.; Ashman, B.; Palmer, M. Anterior Cruciate Ligament Graft Conditioning Required to Prevent an Ab-normal Lachman and Pivot Shift After ACL Reconstruction: A Robotic Study of 3 ACL Graft Constructs. Am. J. Sports Med. 2019, 47, 1376–1384. [Google Scholar] [CrossRef]
- Dietvorst, M.; van der Steen, M.C.M.; Besselaar, M.v.D.; Janssen, R.P. Height is a predictor of hamstring tendon length and ACL graft characteristics in adolescents. BMC Musculoskelet. Disord. 2023, 24, 563. [Google Scholar] [CrossRef]
- Bourgeault-Gagnon, Y.; Leang, A.K.; Bédard, S.; Lebel, K.; Balg, F.; Vézina, F. Estimated diameter increase from a 4S to a 6S hamstring graft configuration—A cadaveric study. SICOT-J 2023, 9, 34. [Google Scholar] [CrossRef]
- Tutkus, V.; Kluonaitis, K.; Silove, S.; Tutkuviene, J. ACL reconstruction using 5- or 6-strand hamstring autograft provides graft’s diameter bigger than 8 mm. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1349–1356. [Google Scholar] [CrossRef]
- Park, J.Y.; Fernandes, A.; Park, S.Y.; Lim, H.; Sayudo, I.F.; Leibovitch, L.; Machinski, E.; Ha, J. Comparative effectiveness of peroneus longus tendon (PLT) autografts versus hamstring tendon (HT) autografts in anterior cruciate ligament reconstruction: A comprehensive systematic review and meta analysis. Eur. J. Orthop. Surg. Traumatol. 2024, 34, 2691–2699. [Google Scholar] [CrossRef]
- Zhang, S.; Cai, G.; Ge, Z. The Efficacy of Anterior Cruciate Ligament Reconstruction with Peroneus Longus Tendon and its Impact on Ankle Joint Function. Orthop. Surg. 2024, 16, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Abudaqqa, R.Y.; Elsheoibi, A.M.; Al Mas, A.J.; Arun, K.P.; Shaaban, F.A.; Aliessa, K.A. The Correlation Between Graft Size and Graft Failure in Hamstring Autograft Anterior Cruciate Ligament Reconstruction. Cureus 2024, 16, e55069. [Google Scholar] [CrossRef] [PubMed]
- Dwidmuthe, S.; Roy, M.; Bhikshavarthi Math, S.A.; Sah, S.; Bhavani, P.; Sadar, A. Functional Outcome of Single-Bundle Arthro-scopic Anterior Cruciate Ligament Reconstruction using Peroneus Longus Graft and Hamstring Graft: An Open-Label, Randomized, Comparative Study. Cureus 2024, 16, e60239. [Google Scholar] [PubMed]
- Coffey, R.; Bordoni, B. Lachman Test. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024; Volume 1, p. 32119302. [Google Scholar]
- Zhao, L.; Lu, M.; Deng, M.; Xing, J.; He, L.; Wang, C. Outcome of bone-patellar tendon-bone vs hamstring tendon autograft for anterior cruciate ligament reconstruction: A meta-analysis of randomized controlled trials with a 5-year minimum follow-up. Medicine 2020, 99, e23476. [Google Scholar] [CrossRef]
- Kaya, S.; Unal, Y.C.; Guven, N.; Ozcan, C.; Dundar, A.; Turkozu, T.; Ozkan, S.; Adanas, C.; Gokalp, M.A. The impact of early weight-bearing on results following anterior cruciate ligament reconstruction. BMC Musculoskelet. Disord. 2024, 25, 395. [Google Scholar] [CrossRef]
- Vari, N.; Cavaignac, E.; Cavaignac, M.; Bérard, É.; Marot, V. Outcomes of hamstring graft with preserved tibial insertion for ACL reconstruction: Systematic review and meta-analysis. Eur. J. Orthop. Surg. Traumatol. 2023, 34, 67–73. [Google Scholar] [CrossRef]
- Kawanishi, Y.; Kobayashi, M.; Yasuma, S.; Fukushima, H.; Kato, J.; Murase, A.; Takenaga, T.; Yoshida, M.; Kuroyanagi, G.; Kawaguchi, Y.; et al. Factors Associated with Residual Pivot Shift After ACL Reconstruction: A Quantitative Evaluation of the Pivot-Shift Test Preoperatively and at Minimum 12-Month Follow-up. Orthop. J. Sports Med. 2024, 12, 23259671241230967. [Google Scholar] [CrossRef]
- Mascarenhas, R.; Tranovich, M.J.; Kropf, E.J.; Fu, F.H.; Harner, C.D. Bone-patellar tendon-bone autograft versus hamstring autograft anterior cruciate ligament reconstruction in the young athlete: A retrospective matched analysis with 2–10 year follow-up. Knee Surg Sports Traumatol. Arthrosc. 2012, 20, 1520–1527. [Google Scholar] [CrossRef]
- Lima, L.H.P.; Gomes, J.L.E. Must a Knee with Anterior Cruciate Ligament Deficiency and High-grade Pivot Shift Test Present an Increase in Internal Rotation? Rev. Bras Ortop. 2024, 59, e82–e87. [Google Scholar]
- Rezansoff, A.; Firth, A.D.; Bryant, D.M.; Litchfield, R.; McCormack, R.G.; Heard, M.; MacDonald, P.B.; Spalding, T.; Verdonk, P.C.M.; Peterson, D.; et al. Anterior Cruciate Ligament Reconstruction Plus Lateral Ex-tra-articular Tenodesis Has a Similar Return-to-Sport Rate to Anterior Cruciate Ligament Reconstruction Alone but a Lower Failure Rate. Arthroscopy 2024, 40, 384–396.e1. [Google Scholar] [CrossRef]
- Vyacheslavovich, O.A.; Vladimirovna, N.A.; Bekzhan, D.; Ayanovich, K.K.; Goncharov, E.; Koval, O.; Bezuglov, E.; Ramirez, M.D.J.E.; Montemurro, N. Evaluating the Efficacy of Reconstruction: Systematic Review of Six-Strand Hamstring Autografts for Anterior Cruciate Ligament Reconstruction: Biomechanical and Clinical Outcomes. Surgeries 2024, 5, 449–464. [Google Scholar] [CrossRef]
- Dai, C.; Wang, F.; Wang, X.; Wang, R.; Wang, S.; Tang, S. Arthroscopic single-bundle anterior cruciate ligament reconstruction with six-strand hamstring tendon allograft versus bone-patellar tendon-bone allograft. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 2915–2922. [Google Scholar] [CrossRef] [PubMed]
- Punnoose, D.J.; Varghese, J.; Theruvil, B.; Thomas, A.B. Peroneus Longus Tendon Autografts have Better Graft Diameter, Less Morbidity, and Enhanced Muscle Recuperation than Hamstring Tendon in ACL Reconstruction. Indian J. Orthop. 2024, 58, 979–986. [Google Scholar] [CrossRef]
- Ertilav, D.; Ertilav, E.; Dirlik, G.N.; Barut, K. Donor Site Morbidity after Removal of Full-Thickness Peroneus Longus Tendon Graft for Anterior Cruciate Ligament (ACL) Reconstruction: 4-Year Follow-up. Acta Chir. Orthop. Traumatol. Cechoslov. 2024, 91, 170–174. [Google Scholar] [CrossRef]
- Holmgren, D.; Noory, S.; Moström, E.; Grindem, H.; Stålman, A.; Wörner, T. Weaker Quadriceps Muscle Strength with a Quadriceps Tendon Graft Compared With a Patellar or Hamstring Tendon Graft at 7 Months After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2024, 52, 69–76. [Google Scholar] [CrossRef]
- Li, X.; Cao, W.; Zhou, H.; Ji, R.; Xiao, J.; Zhao, C. The healing effect of the all inside technique is superior to the traditional technique in the reconstruction of the anterior cruciate ligament. Eur. J. Transl. Myol. 2024, 34, 11970. [Google Scholar] [CrossRef] [PubMed]
- Goncharov, E.N.; Koval, O.A.; Nikolaevich Bezuglov, E.; Encarnacion Ramirez, M.d.J.; Engelgard, M.; Igorevich, E.I.; Saporiti, A.; Valentinovich Kotenko, K.; Montemurro, N. Stromal Vascular Fraction Therapy for Knee Osteoarthritis: A Systematic Review. Medicina 2023, 59, 2090. [Google Scholar] [CrossRef]
- Goncharov, E.N.; Koval, O.A.; Nikolaevich Bezuglov, E.; Engelgard, M.; Igorevich, E.I.; Velentinovich Kotenko, K.; Encarnacion Ramirez, M.D.J.; Montemurro, N. Comparative Analysis of Stromal Vascular Fraction and Alternative Mechanisms in Bone Fracture Stimulation to Bridge the Gap between Nature and Technological Advancement: A Systematic Review. Biomedicines 2024, 12, 342. [Google Scholar] [CrossRef]
- Torres, C.S.O.; Mora, A.E.; Campero, A.; Cherian, I.; Sufianov, A.; Sanchez, E.F.; Ramirez, M.E.; Pena, I.R.; Nurmukhametov, R.; Beltrán, M.A.; et al. Enhancing microsurgical skills in neurosurgery residents of low-income countries: A comprehensive guide. Surg. Neurol. Int. 2023, 14, 437. [Google Scholar] [CrossRef] [PubMed]
- Cheykin, A.; Goncharov, E.N.; Koval, O.A.; Goncharov, N.; Bezuglov, E.; Vetoshkin, A.; Ramirez, M.D.J.E.; Montemurro, N. Postoperative Multimodal Approach to Pain Control in Anterior Cruciate Ligament Autograft Surgery: A Single-Center Series. Surgeries 2024, 5, 660–673. [Google Scholar] [CrossRef]
- Ramirez, M.D.J.E.; Montemurro, N.; Musa, G.; Chmutin, G.E.; Nurmukhametov, R.; Rosario, A.R.; Barza, J.L.; Kaprovoy, S.; Konovalov, N.; Kudriavtsev, D.; et al. On the balance beam: Facing the challenges of neurosurgical education in the third millennium. Surg. Neurol. Int. 2024, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Pierozzi, E.; Inchingolo, A.M.; Pahwa, B.; De Carlo, A.; Palermo, A.; Scarola, R.; Dipalma, G.; Corsalini, M.; Inchingolo, A.D.; et al. New biograft solution, growth factors and bone regenerative approaches in neurosurgery, dentistry, and orthopedics: A review. Rev. Med. Pharmacol. Sci. 2023, 16, 7653–7664. [Google Scholar] [CrossRef]
- Zou, J.; Yang, W.; Cui, W.; Li, C.; Ma, C.; Ji, X.; Hong, J.; Qu, Z.; Chen, J.; Liu, A.; et al. Therapeutic potential and mechanisms of mesenchymal stem cell-derived exosomes as bio-active materials in tendon-bone healing. J. Nanobiotechnology 2023, 21, 14. [Google Scholar] [CrossRef]
- Jang, K.-M.; Lim, H.; Bae, J. Mesenchymal Stem Cells for Enhancing Biologic Healing after Anterior Cruciate Ligament Injuries. Curr. Stem Cell Res. Ther. 2015, 10, 535–547. [Google Scholar] [CrossRef]
- Jin, Y.; Xu, M.; Zhu, H.; Dong, C.; Ji, J.; Liu, Y.; Deng, A.; Gu, Z. Therapeutic effects of bone marrow mesenchymal stem cells-derived exosomes on osteo-arthritis. J. Cell. Mol. Med. 2021, 25, 9281–9294. [Google Scholar] [CrossRef]
- Montemurro, N.; Ortenzi, V.; Naccarato, G.A.; Perrini, P. Angioleiomyoma of the knee: An uncommon cause of leg pain. A systematic review of the literature. Interdiscip. Neurosurg. 2020, 22, 100877. [Google Scholar] [CrossRef]
- Reynoso, J.P.; Encarnacion, M.D.J.; Nurmukhametov, R.; Melchenko, D.; Efe, I.E.; Goncharov, E.; Taveras, A.A.; Pena, I.J.R.; Montemurro, N. Anatomical Variations of the Sciatic Nerve Exit from the Pelvis and Its Relationship with the Piriformis Muscle: A Cadaveric Study. Neurol. Int. 2022, 14, 894–902. [Google Scholar] [CrossRef]
- McRobb, J.; Kamil, K.H.; Ahmed, I.; Dhaif, F.; Metcalfe, A. Influence of platelet-rich plasma (PRP) analogues on healing and clinical outcomes following anterior cruciate ligament (ACL) reconstructive surgery: A systematic review. Eur. J. Orthop. Surg. Traumatol. 2022, 33, 225–253. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, Q.; Cui, L.; Wu, L.; Gao, S. Kartogenin Combined Platelet-Rich Plasma (PRP) Promoted Tendon-Bone Healing for Anterior Cruciate Ligament (ACL) Reconstruction by Suppressing Inflammatory Response Via targeting AKT/PI3K/NF-κB. Appl. Biochem. Biotechnol. 2023, 195, 1284–1296. [Google Scholar] [CrossRef] [PubMed]

| Time Point Post-Surgery | Clinical Examination | Functional Assessment |
|---|---|---|
| 3 months | Lachman test, wound inspection, anterior drawer | IKDC-2000, Lysholm score, range of motion |
| 6 months | Lachman test, wound inspection, pivot-shift test, anterior drawer test | IKDC-2000, Lysholm score |
| 12 months | Lachman test, pivot-shift test, anterior drawer test | IKDC-2000, Lysholm score |
| 24 months | Lachman test, pivot-shift test, anterior drawer test | IKDC-2000, Lysholm score |
| Group H (Hamstring Tendon) | Group P (P. Longus Tendon) | |
|---|---|---|
| Total patients | 55 | 55 |
| Sex | ||
| Male | 41 | 38 |
| Female | 14 | 17 |
| Side involved | ||
| Left side | 13 (23.64%) | 8 (14.55%) |
| Right side | 42 (76.36%) | 47 (85.45%) |
| Mean age (years) | 33.10 ± 4.17 | 32.90 ± 6.98 |
| Mean height | 178.00 ± 5.05 cm | 180.95 ± 4.53 cm |
| Mean weight | 83.40 ± 2.56 kg | 87.25 ± 3.34 kg |
| Average graft diameter | 8.3 ± 0.47 mm | 8.4 ± 0.35 mm |
| Time Period | Group H (Mean ± SD) | Group P (Mean ± SD) |
|---|---|---|
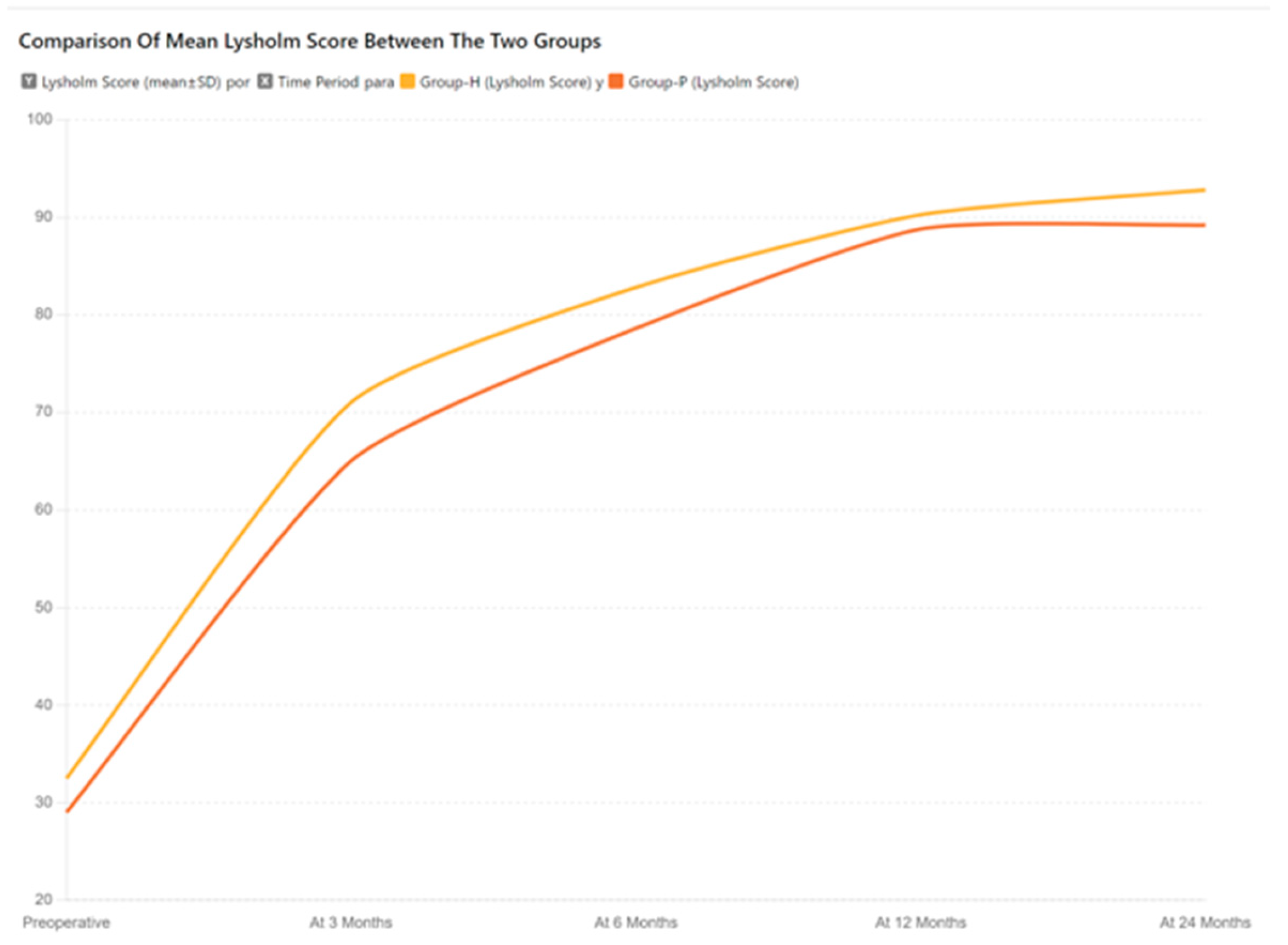
| Preoperative | 32.50 ± 4.35 | 29.00 ± 2.05 |
| At 3 months | 71.00 ± 2.60 | 65.00 ± 3.40 |
| At 6 months | 82.80 ± 3.45 | 78.60 ± 3.45 |
| At 12 months | 90.26 ± 1.30 | 88.80 ± 1.00 |
| At 24 months | 92.80 ± 2.91 | 89.20 ± 2.40 |
| Time Period | Group H (Mean ± SD) | Group P (Mean ± SD) | ‘t’ Value, df | p Value |
|---|---|---|---|---|
| Preoperative | 36.27 ± 2.31 | 38.77 ± 1.84 | −6.26 = 108 | <0.0001 |
| At 3 months | 68.70 ± 3.55 | 70.00 ± 2.80 | −2.19, df = 108 | 0.031 |
| At 6 months | 77.48 ± 5.24 | 75.77 ± 1.30 | 2.40, df = 108 | 0.018 |
| At 12 months | 92.00 ± 2.00 | 90.84 ± 1.30 | 3.50, df = 108 | 0.001 |
| At 24 months | 94.43 ± 1.59 | 90.84 ± 2.44 | 9.14 = 108 | <0.0001 |
| Time Point | Grade | Hamstring (Group H) Pre-Operative | Hamstring (Group H) 3 Months Follow-Up | Hamstring (Group H) 6 Months Follow-Up | Hamstring (Group H) 1 Year Follow-Up | Hamstring (Group H) 2 Years Follow-Up | Peroneus Longus (Group P) Pre-Operative | Peroneus Longus (Group P) 3 Months Follow-Up | Peroneus Longus (Group P) 6 Months Follow-Up | Peroneus Longus (Group P) 1 Year Follow-Up | Peroneus Longus (Group P) 2 Years Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anterior drawer test (ADT) | Grade 0 (1–2 mm) | 0 | 6 | 10 | 14 | 15 | 0 | 7 | 12 | 17 | 18 |
| Grade I (3–5 mm) | 0 | 8 | 5 | 7 | 6 | 0 | 8 | 6 | 6 | 5 | |
| Grade II (6–10 mm) | 12 | 10 | 6 | 1 | 1 | 12 | 10 | 7 | 0 | 0 | |
| Grade III (>10 mm) | 10 | 1 | 0 | 0 | 0 | 11 | 2 | 0 | 0 | 0 |
| Time Point | Grade | Hamstring (Group H) Pre-Operative | Hamstring (Group H) 3 Months Follow-Up | Hamstring (Group H) 6 Months Follow-Up | Hamstring (Group H) 1 Year Follow-Up | Hamstring (Group H) 2 Years Follow-Up | Peroneus Longus (Group P) Pre-Operative | Peroneus Longus (Group P) 3 Months Follow-Up | Peroneus Longus (Group P) 6 Months Follow-Up | Peroneus Longus (Group P) 1 Year Follow-Up | Peroneus Longus (Group P) 2 Years Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lachman’s test (LT) | Grade 0 (1–2 mm) | 0 | 5 | 10 | 13 | 14 | 0 | 6 | 15 | 18 | 19 |
| Grade I (3–5 mm) | 0 | 6 | 5 | 8 | 7 | 0 | 6 | 7 | 5 | 4 | |
| Grade II (6–10 mm) | 14 | 10 | 4 | 1 | 1 | 10 | 8 | 4 | 0 | 0 | |
| Grade III (>10 mm) | 8 | 4 | 0 | 0 | 0 | 13 | 6 | 0 | 0 | 0 |
| Time Point | Grade | Hamstrings Pre-Operative | Hamstrings 6 Months Follow-Up | Hamstrings 1 Year Follow-Up | Hamstrings 2 Years Follow-Up | Peroneus Longus Pre-Operative | Peroneus Longus 6 Months Follow-Up | Peroneus Longus 1 Year Follow-Up | Peroneus Longus 2 Years Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| Pivot shift test (PST) | Equal | 5 | 12 | 16 | 18 | 6 | 14 | 18 | 20 |
| Glide I | 7 | 9 | 6 | 4 | 4 | 6 | 5 | 3 | |
| Clunk II | 6 | 3 | 0 | 0 | 8 | 3 | 0 | 0 | |
| Gross III | 3 | 0 | 0 | 0 | 6 | 0 | 0 | 0 |
| Postoperative Complications | Group H | Group P |
|---|---|---|
| Knee stiffness | 0 | 2 |
| Infection requiring arthroscopic debridement | 0 | 0 |
| Case of cyclops syndrome | 1 | 1 |
| Case of permanent hemarthrosis | 1 | 0 |
| Case of permanent synovitis | 1 | 0 |
| Case of severe contracture of knee joint | 1 | 1 |
| Case of instability | 1 | 2 |
| Outcome Measure | Group H (Six-Strand Hamstring) | Group P (Peroneus Longus) | Effect Size (Cohen’s d) |
|---|---|---|---|
| Lysholm score | 92.80 ± 2.91 | 89.20 ± 2.40 | 0.55 |
| IKDC score | 94.43 ± 1.59 | 90.84 ± 2.44 | 0.65 |
| Anterior drawer test (Grade 0) | 15 | 12 | 0.25 |
| Lachman’s test (Grade 0) | 14 | 12 | 0.20 |
| Pivot shift test (Grade 0) | 18 | 20 | −0.10 |
| Complications (Total) | 5 | 6 | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vyacheslavovich, O.A.; Vladimirovna, N.A.; Bekzhan, D.; Ivanovich, K.K.; Goncharov, E.; Koval, O.; Bezuglov, E.; Ramirez, M.D.J.E.; Montemurro, N. Comparative Analysis of the Six-Strand Hamstring and Peroneus Longus in Sports Medicine and Rehabilitation. Surgeries 2024, 5, 778-798. https://doi.org/10.3390/surgeries5030063
Vyacheslavovich OA, Vladimirovna NA, Bekzhan D, Ivanovich KK, Goncharov E, Koval O, Bezuglov E, Ramirez MDJE, Montemurro N. Comparative Analysis of the Six-Strand Hamstring and Peroneus Longus in Sports Medicine and Rehabilitation. Surgeries. 2024; 5(3):778-798. https://doi.org/10.3390/surgeries5030063
Chicago/Turabian StyleVyacheslavovich, Ondar Artysh, Nikonova Alina Vladimirovna, Dzhunusov Bekzhan, Khaizhok Konstantin Ivanovich, Evgeniy Goncharov, Oleg Koval, Eduard Bezuglov, Manuel De Jesus Encarnacion Ramirez, and Nicola Montemurro. 2024. "Comparative Analysis of the Six-Strand Hamstring and Peroneus Longus in Sports Medicine and Rehabilitation" Surgeries 5, no. 3: 778-798. https://doi.org/10.3390/surgeries5030063