Abstract
The successful operation of medical tourism mobile applications primarily depends on the extent to which users are fully motivated to adopt their use. Therefore, the primary purpose of this study was to investigate the factors influencing medical tourism mobile application usage intentions. This study applied the unified theory of acceptance and use of technology (UTAUT2) to build a comprehensive model that explains users’ intentions to use medical tourism mobile apps. Our research findings confirm the validity of the UTAUT2 in explaining users’ intentions to use medical tourism mobile apps in the context of medical tourism mobile services. Additionally, the results focus on the enhancement in the role of the other rather that contextual attributes of the IT/IS environment (i.e., personal involvement and personal innovativeness). This study can confirm the importance of the UTAUT2 constructs in the setting of medical tourism mobile app usage. By conducting surveys, medical tourism mobile app designers can know that personal involvement and personal innovativeness lead to influences on the effectiveness of corporate marketing efforts relating to using mobile medical apps.
1. Introduction
With the rapid development of information technology and the improvement of health awareness, online medical services dedicated to linking artificial intelligence (AI) and providing efficient and convenient health services are increasingly emerging. Additionally, innovation in digital health applications is accelerating. Combined with the big data database, data analysis is applied to medical diagnosis and treatment and it is promoted to be implemented in local clinics so that local and rural medical care can also have enough resources to use it. Furthermore, with the increasing adoption of mobile applications (apps) in the healthcare industry, the opportunity for health apps is vast.
Many companies have introduced their own medical apps as these apps are important platforms for future marketing. With the purpose of better serving medical tourism mobile app users, the company (such as Dr. Advice in Taiwan) introduced the medical tourism mobile app to integrate medical information (e.g., strengths of participating hospitals, news on medical services, and information on app platforms). There are also numerous potential benefits afforded by mobile apps, particularly in healthcare [1].
The previous literature has focused on a single form of online medical services (e.g., discussing the application of online medical services from the perspective of developers) [2,3]. Few studies have considered mobile medical apps from the perspective of users. To fill the research gaps, this study develops and empirically validates a model that explicates mobile users’ intentions to use mobile medical apps. More specifically, this investigation revisits a popular contemporary adoption theory (i.e., the unified theory of adoption and use of technology (UTAUT2)) [4] by augmenting it to better capture mobile medical application environments.
Recently, Stocchi et al. [5] added a personal involvement construct to the UTAUT2 in a branded mobile applications context. Agarwal and Prasad [6] also effectively introduced an innovation-related construct, personal innovativeness, which influences users to adopt technology. Thus, these two constructs are especially relevant when identifying users’ characteristics regarding the adoption of IT: personal involvement and personal innovativeness [7].
Hence, this study augments the application of the UTAUT2 and adds two individual factors (i.e., personal involvement and personal innovativeness) to explain users’ intentions regarding medical tourism mobile applications. Therefore, the primary purpose of this study was to combine the UTAUT2 and the two specific factors to improve the IT adoption model and better explain users’ intentions with respect to medical tourism mobile applications.
2. Literature Review
2.1. Medical Tourism Mobile Applications
Mobile applications (apps) can help people better understand their own health and wellness, promote healthy living, and gain access to useful information when and where they need it. These tools are being adopted almost as quickly as they are being developed. There are now over 318,000 health apps obtainable from the top app stores worldwide, which is approximately double the number of apps that were available in 2015, with more than 200 apps being added each day [8]. As such, the effort to use digital health tools in clinical practice has significantly progressed. These users include health care professionals, consumers, patients, and potential patients.
Furthermore, medical tourism is gaining heights due to the technological advancements that aid it. Technological advancements make this industry unique. Web 2.0, cloud computing, mobile technology, etc., are going deep into the field of medical research. Medical tourism mobile apps are medical devices that meet the definition of a medical device. They are also an accessory to a controlled medical device and can transform a mobile platform into a regulated medical device. Medical tourism mobile apps can be used to manage a person’s own health and wellness and monitor their caloric intake for healthy weight care. Many countries in Asia have launched their own medical tourism apps. To better serve medical tourists, the Taiwan government has launched the TMT App, which integrates medical tourism information, such as the strength of participating hospitals, medical tourism service information, and local scenic spot information (Chang et al., 2016) [9]. Taking Taiwan’s TMT App as an example, the information on medical institutions is complete and rich. In addition to the introduction of the institutions and medical features, there are map downloads and immediate contact numbers, providing convenient and real-time medical tourism information for the global public. Taiwan’s rich and unique tourism resources, coupled with high-quality medical technology and services, have become a strong force in promoting Taiwan’s international medical care. Now through the TMT App for smart mobile devices, the dissemination of this information can be wider and more convenient.
2.2. Revisiting the Primary UTAUT2 Model
The UTAUT2 [4] is an academic model based on the UTAUT [10], which aims to provide a rough framework specifically designed to explain technology adoption. Whereas the original UTAUT was mainly designed for organizational contexts, the extended unified theory of acceptance and use of technology (UTAUT2) was specifically proposed to clarify technology acceptance from the customer’s perspective [4].
This theoretical framework introduces three main aspects regarding its predecessor: (1) redefining the four explanatory variables included in the original UTAUT (i.e., performance expectancy, effort expectancy, social influence, and facilitating conditions) to adapt them to the consumption context, (2) identifying three additional key constructs from the prior research on both the general adoption and use of technologies and consumer adoption and use of technologies, and (3) altering some of the existing relationships in the original formulation of the UTAUT and introducing new relationships.
The main constructs in the UTAUT2 (i.e., performance expectancy (PE), effort expectancy (EE), social influence (SI), facilitating conditions (FC), hedonistic motivation (HM), price value (PV), and habit (HB)) were proposed as direct determinants of customers’ intentions to adopt medical mobile apps. Despite its recent adoption in the literature, the UTAUT2 has already been tested in some studies that have confirmed its validity to explain technology adoption in consumption contexts, including the mobile application industry [9].
2.3. Intention to Use
Intention to use refers to the degree to which a person consciously plans to perform or not perform some specific future behavior [11]. In addition, Venkatesh et al. [10] pointed out that usage intent is the main indicator of the effectiveness of information systems. The usage intent of medical tourism mobile applications is also a form that information systems take.
2.4. Performance Expectancy
Performance expectancy refers to an individual’s perception that an IS facilitates the completion of a task [4,10]. That is, the degree to which users perceive that using mobile medical apps enables them to achieve improved health management. Performance expectancy is of direct significance to the use of mobile apps for medical management. This is because users rely on the use of mobile apps to access adequate information.
2.5. Effort Expectancy
Effort expectancy is an individual’s evaluation of the effort necessary to complete a task using a given IS [4,10]. Venkatesh et al. [10] viewed effort expectancy as the degree of ease associated with the use of an information system. Effort expectancy is also based on the idea that there are relationships between the effort put forth at work, the performance achieved from that effort, and the rewards received from the effort [12].
2.6. Social Influences
Social influences refer to how an individual perceives the degree of approval of a certain behavior from important referents [4,10]. Social influences have a strong origin in attitudinal-behavioral theories (e.g., theory of reasoned action; [13]), although it was not present in the preceding theories of IS adoption (e.g., TAM; [14]).
Taylor and Todd [15] indicated that peer influence from friends and classmates, as well as superior influence from professors, indirectly influences behavioral intentions through the mediator of the subjecting norms. Use of the medical mobile app would be affected by superior or important people’s influences.
2.7. Facilitating Conditions
Facilitating conditions refer to the degree to which an individual believes that a technical infrastructure exists to support technology use [16]. In commercial settings, facilitating conditions represent the extent to which a consumer believes that resources exist. They facilitate the task completion using the IT/IS. This construct was introduced more recently in the IS adoption literature to overcome the narrower focus of the previous research, which almost exclusively focused on a user’s internal belief system [17].
2.8. Hedonic Motivation
Hedonic motivation refers to internal incentives (e.g., fun, enjoyment, and pleasure) derived from using technology. It also represents the extent to which consumers believe that using an IS system is entertaining [4]. Initially, when most consumers were primarily task-oriented, the adoption focus was on internal beliefs and utilitarian factors [18].
2.9. Perceived Value
Perceived value is treated as a multi-dimensional construct in the context of consumer value [19]. Customers could cognitively care about the utility and financial cost of using these new systems. They also see that using technology should be perceived as more advantageous and useful than the monetary cost paid (Venkatesh et al. [4]). More importantly, the facilities and resources required (e.g., 4G services, smart phones, and Wi-Fi) to perform mobile medical apps could result in a further financial cost, thus enhancing the important role of price value in the conceptual model.
2.10. Habit
Habit is commonly understood as the learned sequences of acts that become automatic responses to specific situations, which may be functional in obtaining certain goals or end states [20]. It indicates the extent to which people tend to perform behaviors automatically because of learning [4]. In addition, Limayem et al. [21] indicated that habit has been included in certain continuance intentions models to explain IT use behavior, because consumers frequently use those IT devices and the behavior becomes automatic.
2.11. Personal Involvement
Involvement is generally understood as referring to the individual’s personal relevance or the importance of an object or activity. Involvement is a motivational factor that determines the attitude strength and the probability of the consistent behavior [22]. Gabbott and Hogg [23] further defined involvement as “a motivational variable reflecting the extent of personal relevance to the individual in terms of basic goals, values and self-concept” (p. 160).
Almost all consumers, it seems, are particularly involved with one or more product categories that he or she finds highly relevant and attractive. Compared to uninvolved consumers, involved consumers feel that these product categories are especially relevant to their lives [23]. Therefore, in this study, we expected that a higher level of personal involvement would lead to a higher level of intentions to use mobile applications. In addition, TAM theorizes that external variables (e.g., personal involvement) [24] are fully mediated by perceived enjoyment, perceived usefulness, and perceived ease of use.
2.12. Personal Innovativeness
Rogers [25] indicated that innovators are people who are willing to take risks in relation to trying new technologies. Furthermore, personal innovativeness refers to an individual’s willingness to try out new information technologies [6]. Personal innovativeness influences the adoption of new technology to an excessive extent [7]; thus, it is appropriate to examine how personal innovativeness influences users’ intentions to use medical tourism mobile applications.
2.13. Hypothesis Development
According to the literature review, the research hypotheses were as follows:
H1.
Performance expectancy has a positive influence on users’ intentions to use medical tourism mobile apps.
H2.
Effort expectancy has a positive influence on users’ intentions to use medical tourism mobile apps.
H3.
Social influences have a positive influence on users’ intentions to use medical tourism mobile apps.
H4.
Facilitating conditions have a positive influence on users’ intentions to use medical tourism mobile apps.
H5.
Hedonic motivation has a positive influence on users’ intentions to use medical.
H6.
Perceived value has a positive influence on users’ intentions to use medical tourism mobile apps.
H7.
Habit has a positive influence on users’ intentions to use medical tourism mobile apps.
H8.
Personal involvement has a positive influence on users’ intentions to use medical tourism mobile apps.
H9.
Personal innovativeness has a positive influence on users’ intentions to use medical tourism mobile apps.
3. Methodological Aspects
3.1. Research Model
The research model is presented in Figure 1. It illustrates the main effect of the constructs of the UTAUT2. This study focuses on examining the individual’s factors (i.e., personal involvement and personal innovativeness) because these factors are a direct reflection of users’ responses to medical tourism mobile app services.
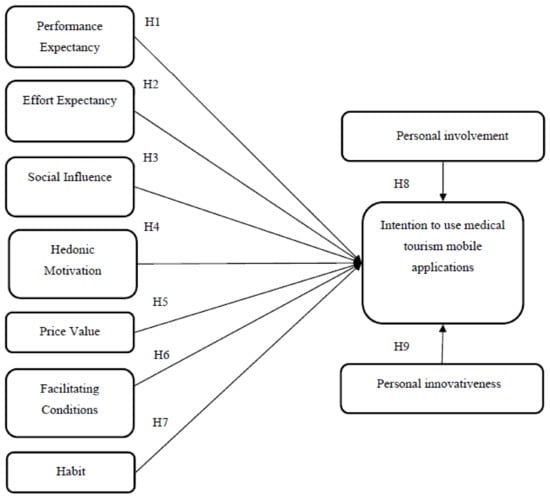
Figure 1.
Research model.
3.2. Instrument Development
Data were collected via a self-administered online survey. Measurement scales for all construct items were taken from the existing scales in the prior work, with modified wordings to adapt the items to the topic area. During the pretest phase, the questionnaire was reviewed by a small group of management faculty and management students; the scales were modified as a result of their suggestions. The questionnaire was then tested with a sample of medical and business school students and personnel. This resulted in further modifications to the questions. The purpose of these pretests was to confirm that relevant aspects were included and to enhance the clarity and readability of the questionnaire.
3.3. Measurements
To ensure the content validity of the scales used, the selected items must represent the concept around which the generalizations are to be made. Therefore, the items selected for the constructs were largely adapted from the prior studies to ensure content validity. In this study, the constructs of the UTAUT2 were taken from Alalwan et al. [26] and Venkatesh et al. [4] and were modified to reflect the utility of medical tourism mobile apps. The personal involvement and personal innovativeness constructs were driven by the work of [7,22].
The participants were instructed to rate each item of these dependent variables on a 5-point Likert scale, where 1 is “strongly disagree” and 5 is “strongly agree”.
3.4. Procedures and Participants
To comply with the background of this sampling project, an electronic survey was posted through an online survey platform to obtain a sample from the mass population of online mobile users. The web link was posted on Facebook, a popular social networking site. After clicking on the link and entering the questionnaire’s website, participants were asked whether they were medical tourism mobile app users or potential users. The degree of personal involvement and personal innovativeness is mainly measured by the scale of the questionnaire in this study.
3.5. Data Collection Process and Participants
An online self-administrated survey is an appropriate instrument to use to obtain medical tourism mobile app users’ information. All questions were measured on a 5-point Likert scale, where 1 is ‘strongly disagree’ and 5 is ‘strongly agree’. The time required to complete the questionnaire was estimated to be 3–5 min. All respondents voluntarily participated in the study during 20 July–20 August 2018. There was a total of 392 participants, comprised of 202 males and 190 females. Most of the participants (69%) stated that they were familiar with the term mobile medical app prior to completing the survey.
4. Results
Based on the two-step approach recommended in Anderson and Gerbing [27], this study first analyzed the measurement model to test the reliability and validity of the instrument and then analyzed the structural model to test the research hypotheses.
4.1. Measurement Model Analysis
To examine the reliability of each item, this study checked the significance and magnitude of its loadings. All items significantly loaded on their respective latent factors; they all achieved standardized loadings of at least 0.60. Two measures were used to assess the internal consistency of the constructs: the composite reliability (CR) and the average variance extracted (AVE). The CR results were between 0.81 and 0.88, while the AVE results were between 0.74 and 0.89. These results were above the recommended cut-off levels of 0.70 and 0.50, respectively, and revealed adequate internal consistency.
In the validity analysis, the convergent validity was examined through a composite reliability. The composite reliability for both constructs is above the recommended guideline of 0.70. In addition, Fornell and Larcker [28] suggested that discriminant validity be established if the square root of the AVE for an individual construct is greater than the correlation of that construct with the other constructs.
Table 1 and Table 2 illustrate that this condition is met for all cases. The measurement indications of this model fit with the experts’ recommendations. The statistics of the fit indications are acceptable when compared to the ideal level.

Table 1.
Loadings and composite reliability.
Table 2.
Correlations between constructs (diagonal elements are square roots of average variance extracted).
Each factor loading of the observed variables onto their respective latent variables was in the anticipated direction. They were also significantly different from zero at the 0.01 level. These results corroborate the existence of convergent validity (Table 1).
Checks were then conducted to determine whether or not the correlations among the latent variables were significantly less than 1. The 95% confidence intervals for each correlation coefficient were all less than 1, indicating discriminant validity. Chi-squared difference tests were also applied to freely estimate the correlations between all possible pairs of constructs; these values were constrained to 1. Checks were conducted to determine whether or not the constraint caused a significant degradation in fit. This series of tests also revealed discriminant validity.
The diagonal elements, which represent the square roots of the AVE for each construct, were found to be higher than the loadings of the items designed to measure the other constructs. Similarly, the item loadings were found to be considerably higher for their corresponding constructs than for the other constructs. These results illustrate that all of the construct measures in our model achieved discriminant validity. Consequently, the testing for validity and reliability showed that the data were robust and provided us with a high degree of confidence in the scale items used in the study.
4.2. Structural Model Analysis
In a structural model, it is important to determine the significance and association of each hypothesized path and the variance explained ( value). The values represent the amount of variance explained by the independent variables. Together, the values and path coefficients indicated how well the data supported the hypothesized model.
Model testing involves two steps. The first step in the model testing process is to estimate the goodness-of-fit, which is typically conducted using a test. That being said, such tests are sensitive to sample sizes and the probability of rejecting any model increases as the sample size increases, even when the model is minimally false. Bentler and Bonett [29] suggested the ratio (: degrees of freedom) as a more appropriate measure of model fit. This ratio, which should not exceed 5.0 for models with good fit [30], was estimated at a value of 2.92 in the hypothesized model (, ).
Table 3 lists the recommended and actual values of the fit indices of the goodness-of-fit (GFI), the adjusted goodness-of-fit (AGFI), the normalized fit index (NFI), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA). For all indices, the actual values were found to be better than the recommended values. Therefore, the model has good fit [30] (Bentler, 1989).
Table 3.
Fit statistics.
The second step in the model testing process is to examine the path significance of each hypothesis. Figure 2 illustrates the results of the tests performed using AMOS 22.0 software. As predicted in H1, the performance expectancy is positively and significantly related to users’ behavioral intentions to use medical tourism mobile apps, with standardized coefficients of 0.43 (). Similarly, the results reveal a positive relationship between the effort expectancy and users’ behavioral intentions to use medical tourism mobile apps () in support of H2.
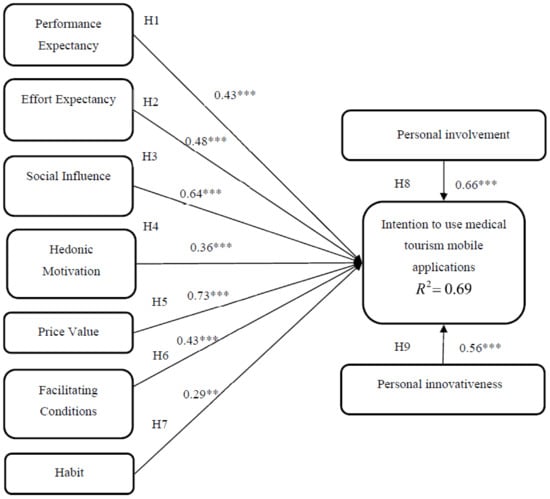
Figure 2.
Results of testing model. ** p < 0.01; *** p < 0.001.
The direct influence of the social influence has a significant impact on users’ intentions to use medical tourism mobile apps () and the hedonic motivation also has positive effects on users’ behavioral intentions to use medical tourism mobile apps (), validating H3 and H4, respectively. In addition, the price value has a positive effect on users’ behavioral intentions to use medical tourism mobile apps (), supporting H5. The facilitating conditions and habit have a positive effect on users’ intentions to use medical tourism mobile apps (). Therefore, H6 and H7 were supported.
All UTAUT2 constructs were fit to the setting of medical tourism mobile app usage. This study can confirm the importance of the UTAUT2 constructs in the setting of medical tourism mobile app usage as has been demonstrated in [32] in the e-commerce context. As for the other main predictors of users’ intentions to use medical tourism mobile apps, both personal involvement () and personal innovativeness () were proven to have a significant influence on users’ intentions to use medical tourism mobile apps, confirming H8 and H9.
5. Discussion and Implications
This study extends the UTAUT2 model in the mobile environment by adding personal factors as external variables. The study has provided some valuable insight into users’ intentions to use a medical tourism mobile application from the perspectives of users. In addition, this study tested the descriptive validity of the UTAUT2 in the domain of the mobile context. Based on the results presented herein, several implications can be made.
The results reveal that the model being examined in the current study has been able to reach an accepted level in terms of the predictive power of the endogenous factor: users’ intentions to use medical tourism mobile apps (Figure 2). That is, by including personal innovativeness and personal involvement, along with the UTAUT2 factor, the value extracted in users’ intentions to use medical tourism mobile apps reached 69% (Figure 2). This result supports personal innovativeness and personal involvement as external factors in the conceptual model. That is, departing from the literature view of system performance as the central critical predictor of adoption [17] (Venkatesh and Bala, 2008), the results focus on the enhancement in the role of the other rather than contextual attributes of the IT/IS environment (i.e., personal involvement and personal innovativeness). These findings confirm the validity of the UTAUT2 in explaining users’ intentions to use medical tourism mobile apps in the context of mobile medical services. Consequently, several theoretical and practical contributions can be made.
5.1. Theoretical Implications
After the analyses were complete, the perceived value was found to have more positive effects than those of others on users’ intentions to use medical tourism mobile apps. That is, healthcare users’ use of a mobile medical app to find hospital and healthcare-related information reflects their concern regarding their own health and the value of the services.
In addition, this study found that social influences with the strongest effect determine the predisposition to use medical tourism mobile apps, as previous studies found. In addition to the perceived value and social influences, the UTAUT2 has endorsed that all constructs are significant predictors of users’ intentions to use medical tourism mobile apps. That is, the UTAUT2 is one of the extensively used models for testing the acceptance and use of various technologies in a number of different studies [4] (Venkatesh et al., 2012).
Finally, this study has to highlight the positive effect of personal involvement and personal innovativeness on users’ intentions to use medical tourism mobile apps, as obtained in the research of Sørebø et al. [7] (2008). Personal factors have positive effects on users’ intentions to use mobile medical apps. This is part of what many scholars have not discussed in the past. Specific factors also affect users’ intentions to use medical tourism mobile apps.
5.2. Practical Implications
The constructs of the UTAUT2 may influence users’ intentions to use mobile medical apps. More specifically, the performance expectancy that represents the utilitarian features is the third driver of users’ intentions to use medical tourism mobile apps. For this reason, service providers should offer utilitarian features to satisfy user needs. On the other hand, the UTAUT2 included discussing psychological factors. In this study, social influences were found to lead to users’ intentions to use medical tourism mobile apps. Indeed, predicting the usage intentions in the medical tourism mobile app market space is more complex, because the usage intentions can also be influenced by friends rather than by services. Thus, service providers can apply some promotion strategies to enhance users’ usage motivation and determine more data on users’ usage motivation. Regardless, personal communication was found to be the best way to persuade potential users that using a medical tourism mobile app service is more useful and advantageous than traditional services [32].
Personal involvement and personal innovativeness have played important roles in explaining users’ intentions to use medical tourism mobile apps. By conducting surveys, medical tourism mobile app designers can know that personal involvement and personal innovativeness lead to influences on the effectiveness of corporate marketing efforts related to using medical tourism mobile apps.
Finally, the results reveal that habit has fewer positive effects than the other factors of the UTAUT2. Hence, this study suggests that mobile medical app designers must include practical functions after medical services (e.g., individual medical checkup analysis and follow-up medical consulting) to allow users to develop habits.
6. Limitations and Future Research
This study has opened up new avenues for a further examination or replication of similar studies in different settings to explore the role of individual factors in the acceptance and use of technology. However, as the research sample is somewhat diversified (i.e., respondents’ ages ranged from 31–66), the findings may not apply to people who are significantly older. Hence, it is recommended that future research focuses on testing the UTAUT2 with different sample structures. In addition, this study is limited to convenience sampling. For convenience sampling, research questionnaires were distributed on Facebook. As a result, when measuring personal innovativeness, because the sample itself has used social media, it is inherently innovative. Measurement may introduce measurement error. Another possible streak of future research may be to validate the UTAUT2 model in other types of IT/IS in view of the respondents’ different behavioral intentions.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declare no conflict of interest.
References
- Aungst, T.D.; Clauson, K.A.; Mistra, S.; Lewis, T.L.; Husain, I. Utilization of smartphone applications by Anesthesia providers. Anesthesiol. Res. Pract. 2018, 2018, 8694357. [Google Scholar] [CrossRef]
- Hsiao, C.-H.; Chang, J.-J.; Tang, K.-Y. Exploring the influential factors in continuance usage of mobile social Apps: Satisfaction, habit, and customer value perspectives. Telemat. Inform. 2016, 33, 342–355. [Google Scholar] [CrossRef]
- Kao, H.-Y.; Wei, C.-W.; Yu, M.-C.; Liang, T.-Y.; Wu, W.-H.; Wu, Y.J. Integrating a mobile health applications for self-management to enhance Telecare system. Telemat. Inform. 2018, 35, 815–825. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong JY, L.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef]
- Stocchi, L.; Michaelidou, N.; Pourazad, N.; Micevski, M. The rules of engagement: How to motivate consumers to engage with branded mobile apps. J. Mark. Manag. 2018, 34, 1196–1226. [Google Scholar] [CrossRef]
- Agarwal, R.; Prasad, J. A conceptual and operational definition of personal innovativeness in the domain of information technology. Inf. Syst. Res. 1998, 9, 204–224. [Google Scholar] [CrossRef]
- Sørebø, A.M.; Sørebø, Ø.; Sein, M.K. The influence of user involvement and personal innovativeness on user behavior. Int. J. Hum. Soc. Sci. 2008, 3, 326–331. [Google Scholar]
- IQVIA. The Growing Value of Digital Health Evidence and Impact on Human Health and the Healthcare System. 2017. Available online: https://www.iqvia.com/institute/reports/the-growing-value-of-digital-health (accessed on 7 November 2017).
- Chang, I.C.; Chou, P.C.; Yeh RJ, K.; Tseng, H.T. Factors influencing Chinese tourists’ intentions to use the Taiwan Medical Travel App. Telemat. Inform. 2016, 33, 401–409. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Ghalandari, K. The effect of performance expectancy, effort expectancy, social influence and facilitating conditions on acceptance of e-banking services in Iran: The moderating role of age and gender. Middle East J. Sci. Res. 2012, 12, 801–807. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Taylor, S.; Todd, P.A. Understanding information technology usage: A test of competing models. Inf. Syst. Res. 1995, 6, 144–176. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Venkatesh, V.; Bala, H. Technology acceptance model 3 and a research agenda on interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef]
- Thong, J.Y.L.; Hong, S.J.; Tam, K.Y. The effects of post-adoption beliefs on the expectation-confirmationmodel for information technology continuance. Int. J. Hum. Comput. Stud. 2006, 64, 799–810. [Google Scholar] [CrossRef]
- Sweeney, J.; Soutar, G.N. Consumer perceived value: The development of a multiple item scale. J. Retail. 2001, 77, 203–220. [Google Scholar] [CrossRef]
- Verplanken, B.; Wood, W. Interventions to break and create consumer habits. J. Public Policy Mark. 2006, 25, 90–103. [Google Scholar] [CrossRef]
- Zaichkowsky, J.L. Measuring the involvement construct. J. Consum. Behav. Res. 1985, 12, 341–352. [Google Scholar] [CrossRef]
- Limayem, M.; Hirt, S.G.; Cheung, M.K. How habit limits the predictive power of intention: The case of information systems continuance. MIS Q. 2007, 31, 705–737. [Google Scholar] [CrossRef]
- Gabbott, M.; Hogg, G. The role of non-verbal communication in service encounters: A conceptual framework. J. Mark. Manag. 2001, 17. [Google Scholar] [CrossRef]
- Rouibah, K.; Hamdy, H. Effect of management support, training, and user involvement on system usage and satisfaction in Kuwait. Ind. Manag. Data Syst. 2009, 109, 338–356. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 3rd ed.; Free Press: New York, NY, USA, 1983. [Google Scholar]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Brown, M.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Eysenbach, G. There’s an app for that: Content analysis of paid health and fitness apps. J. Med. Internet Res. 2012, 14, e72. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).