
Three-Dimensional Finite Element Analysis on Mandibular Biomechanics Simulation under Normal and Traumatic Conditions


 ,
,
Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
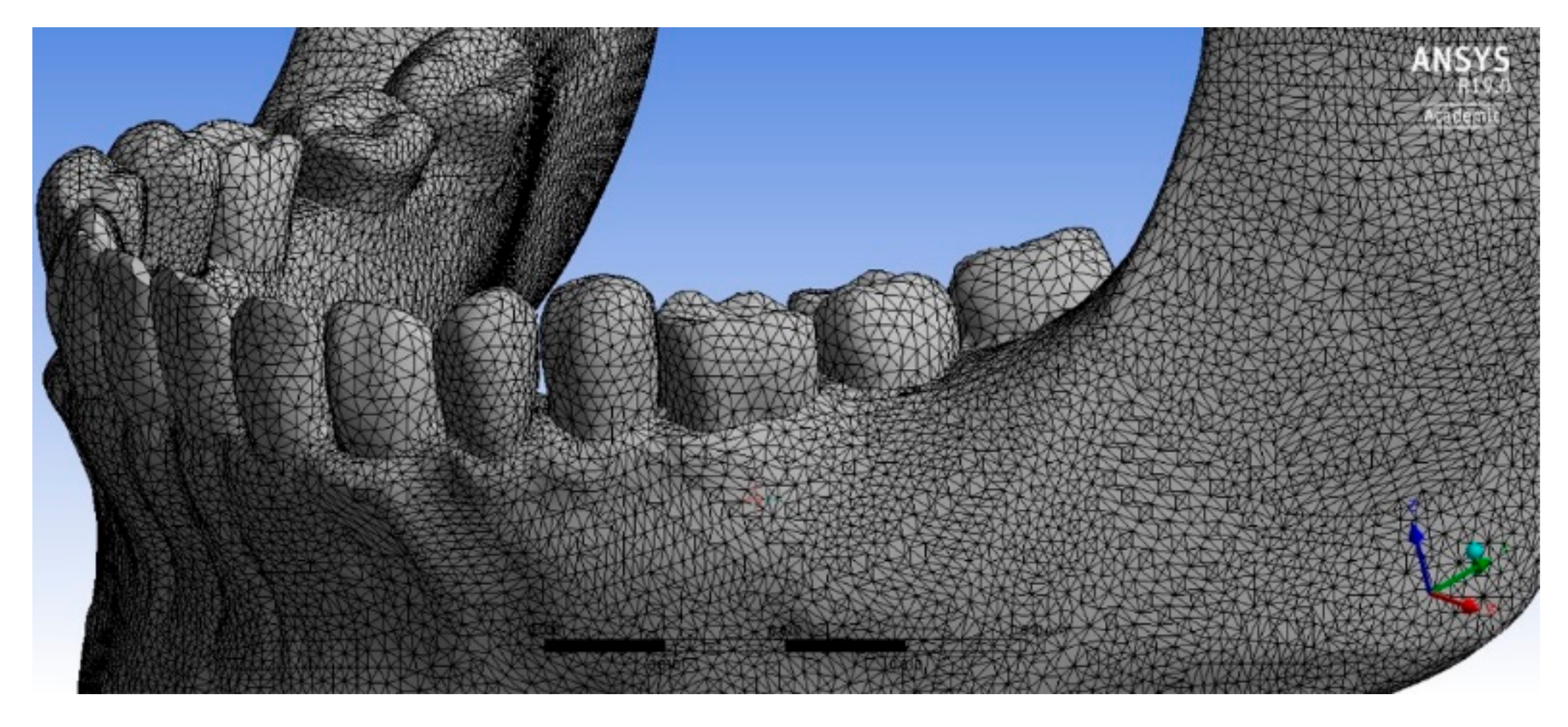
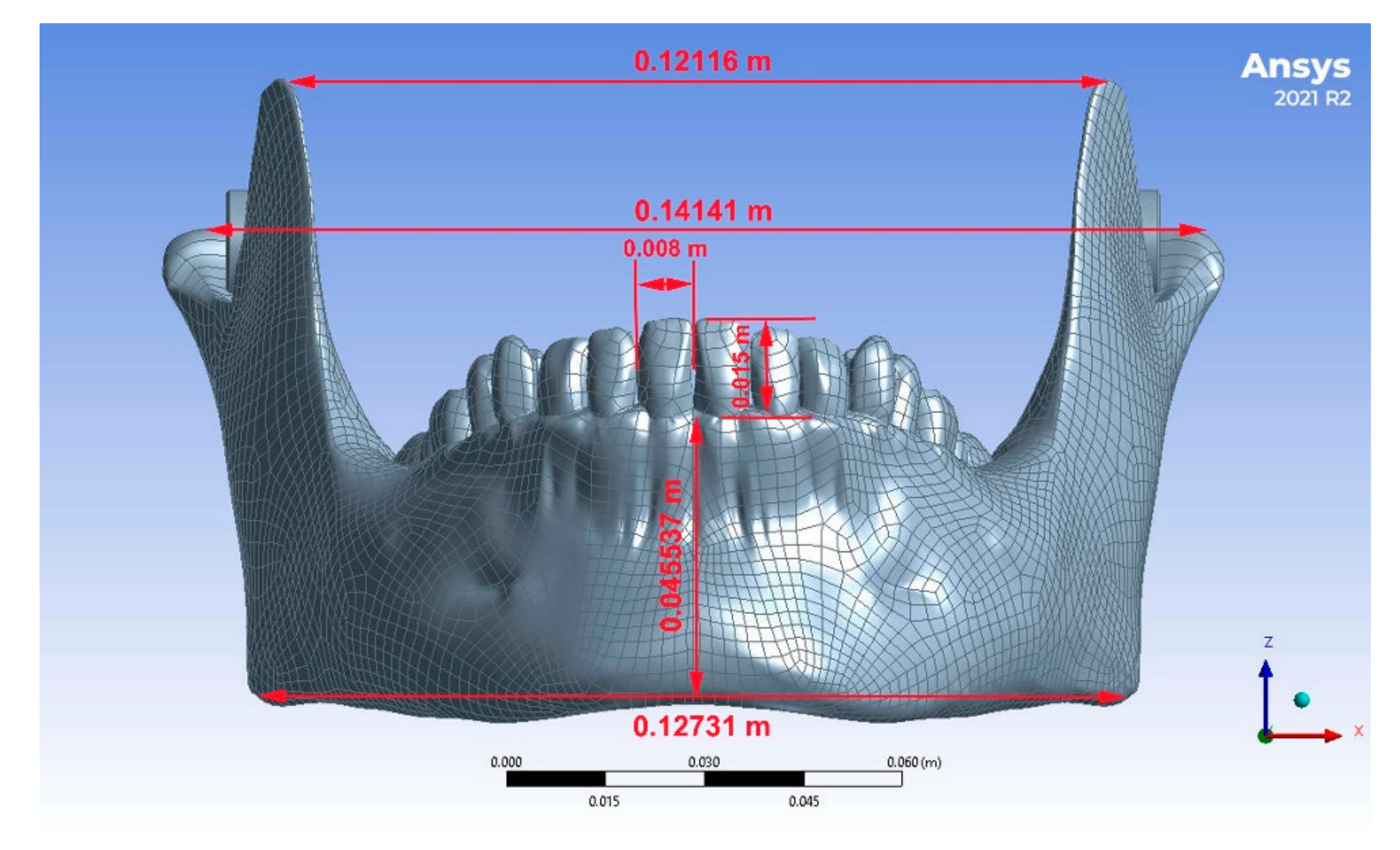
2.1. Virtual Models for Mandibular Bone
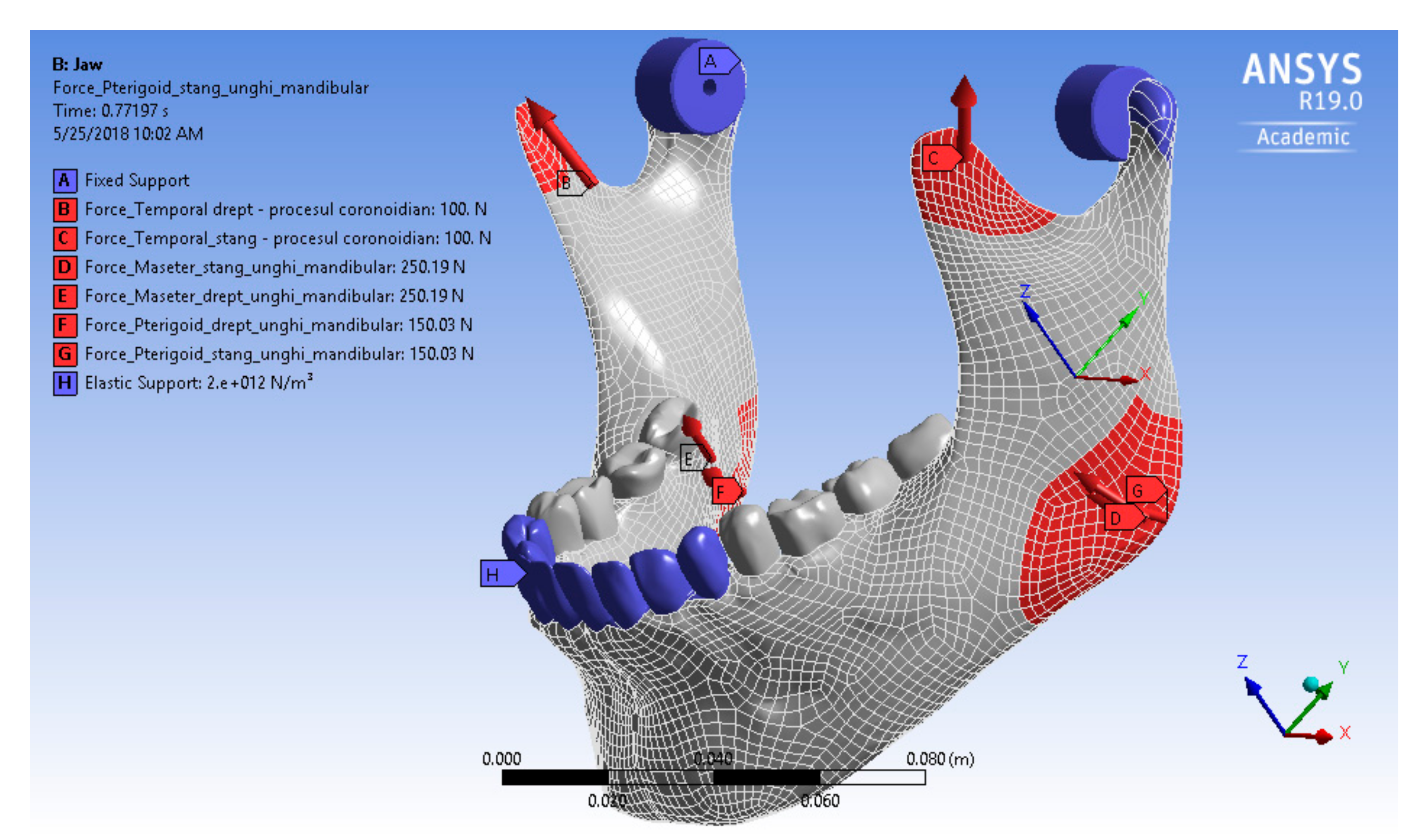
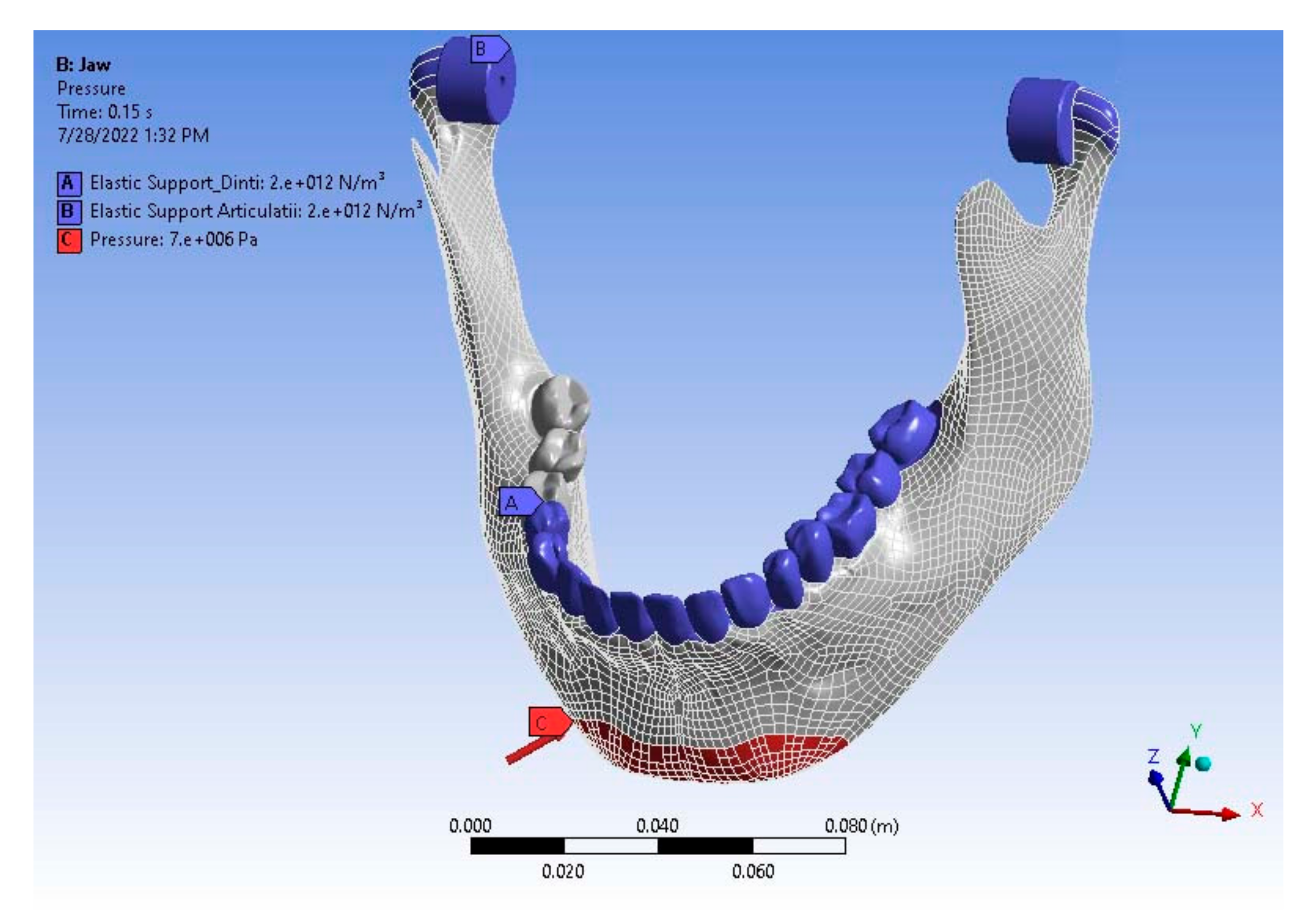
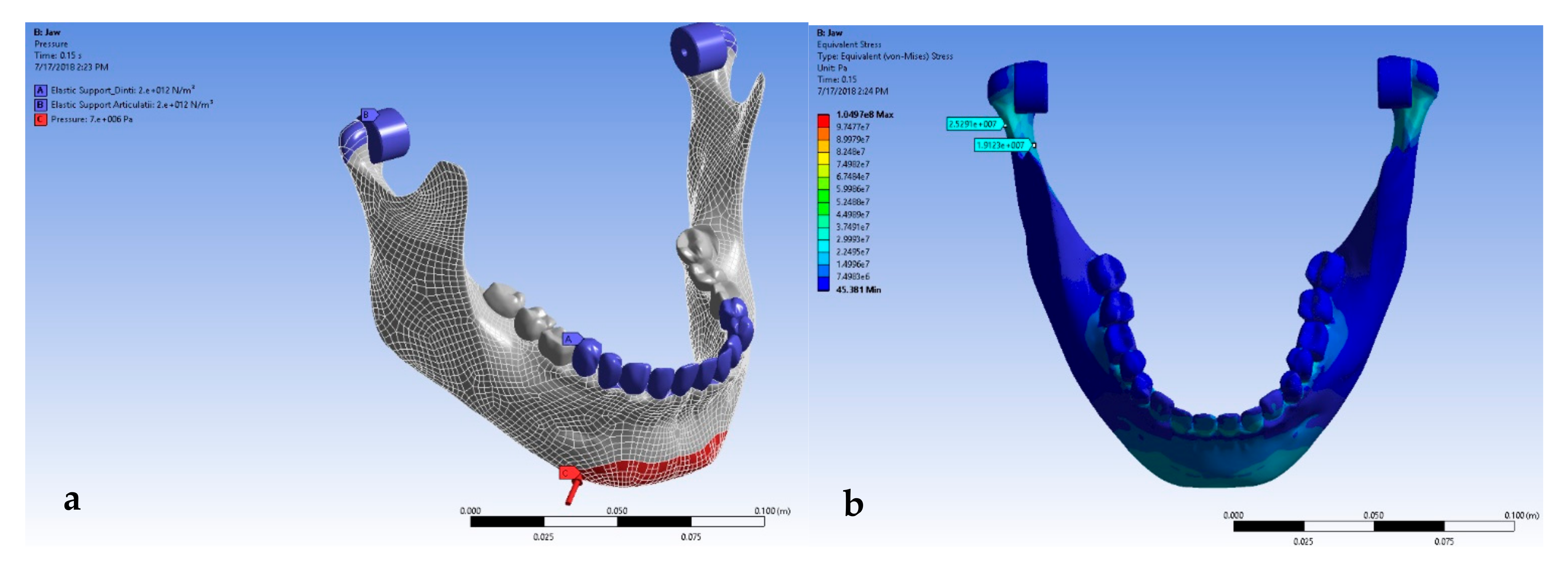
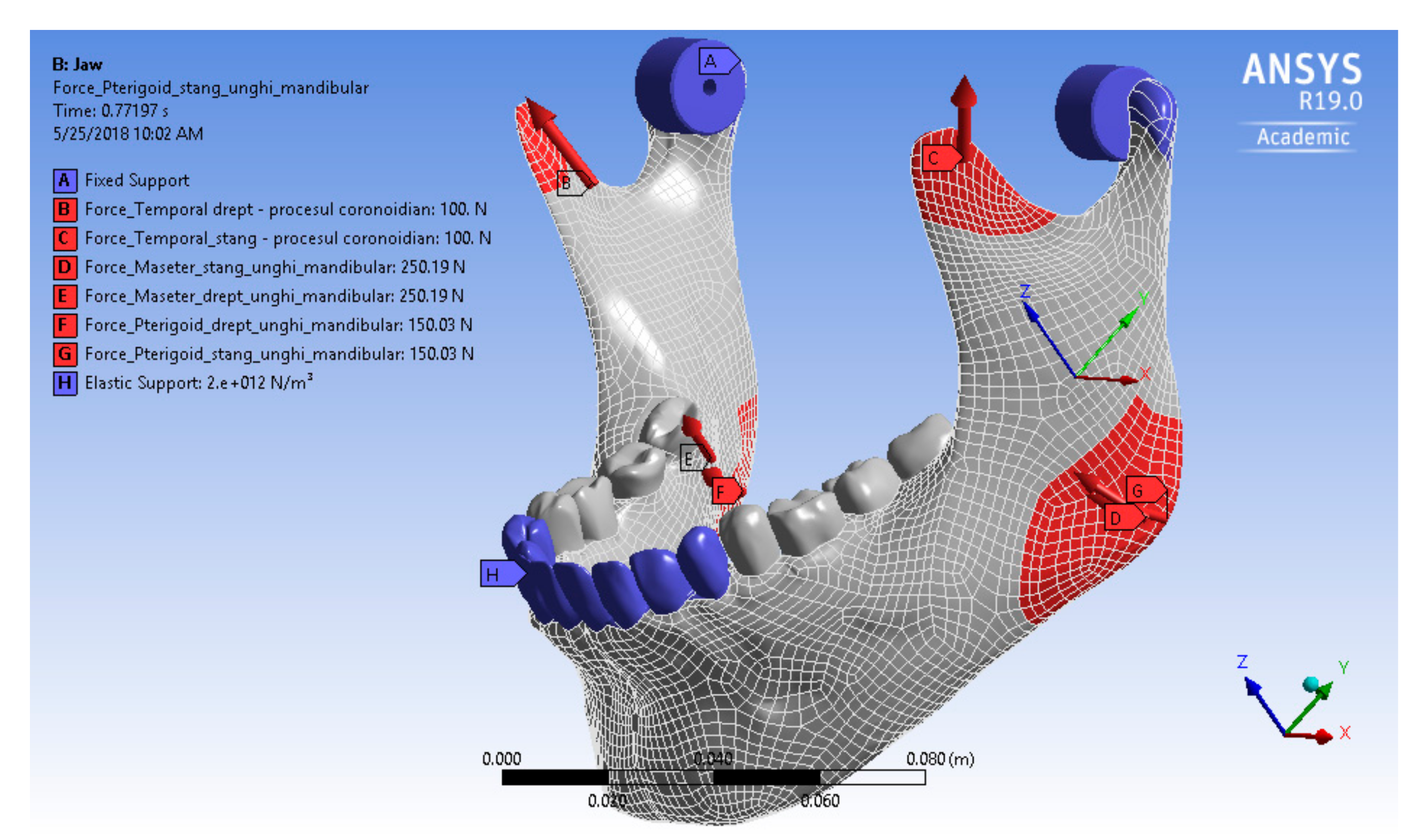
2.2. Mechanical Stress Simulation
3. Results
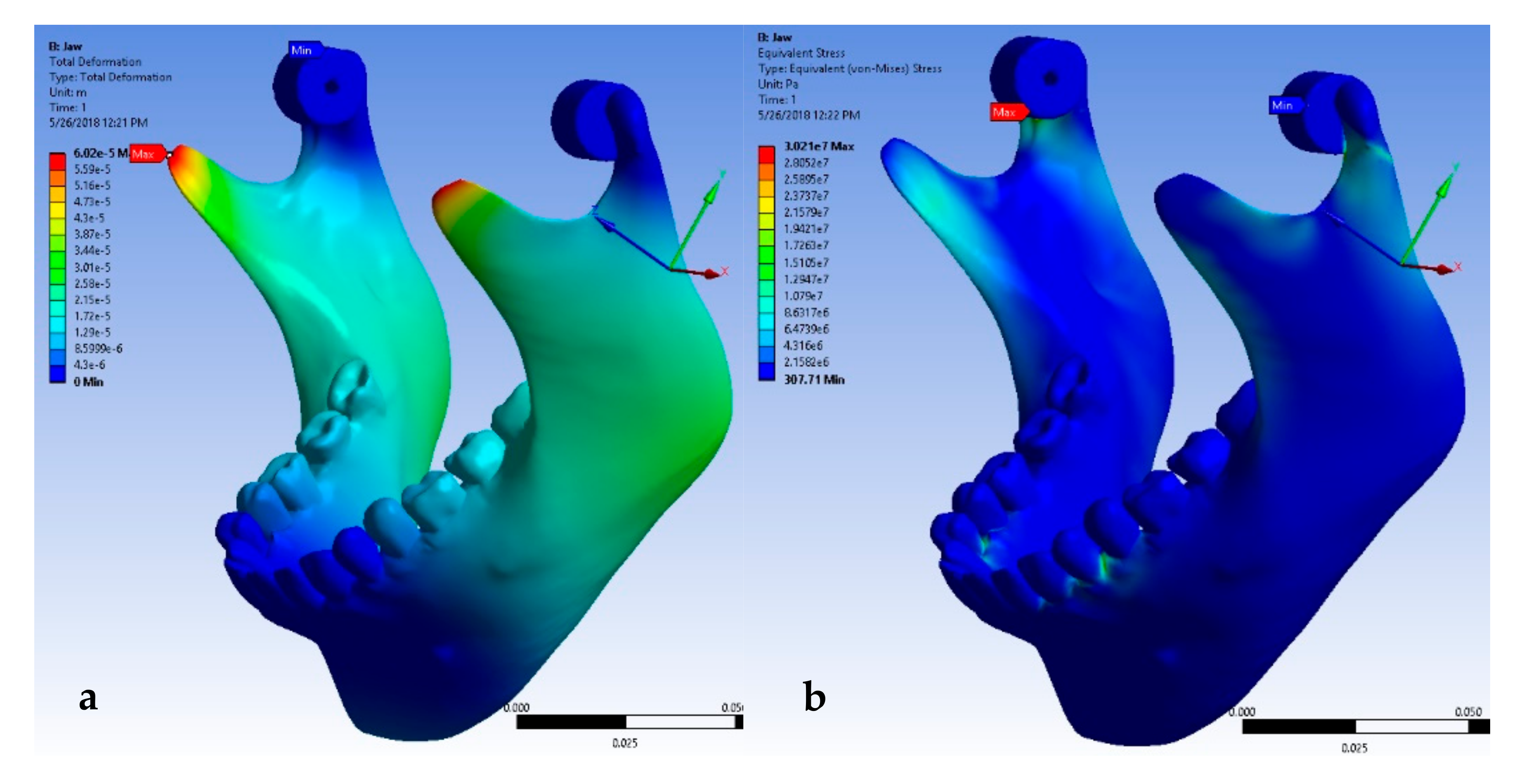
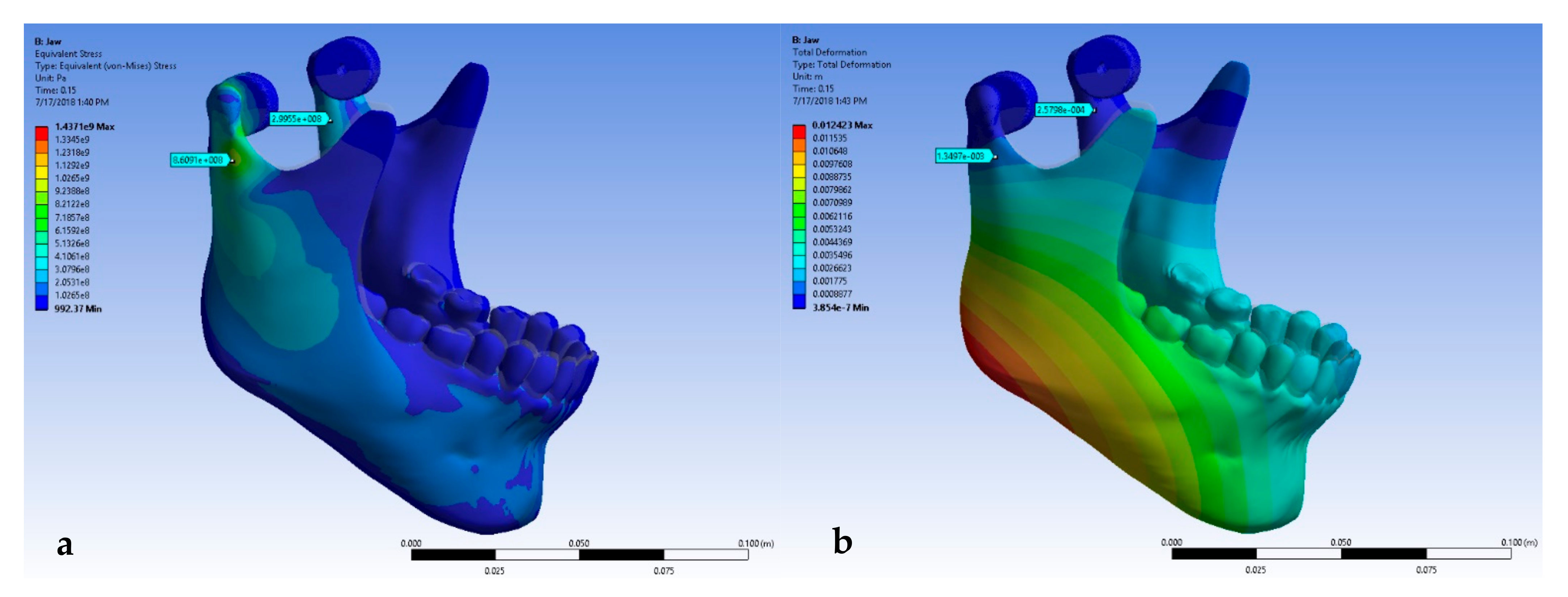
3.1. Normal Bite
3.2. Impact Response
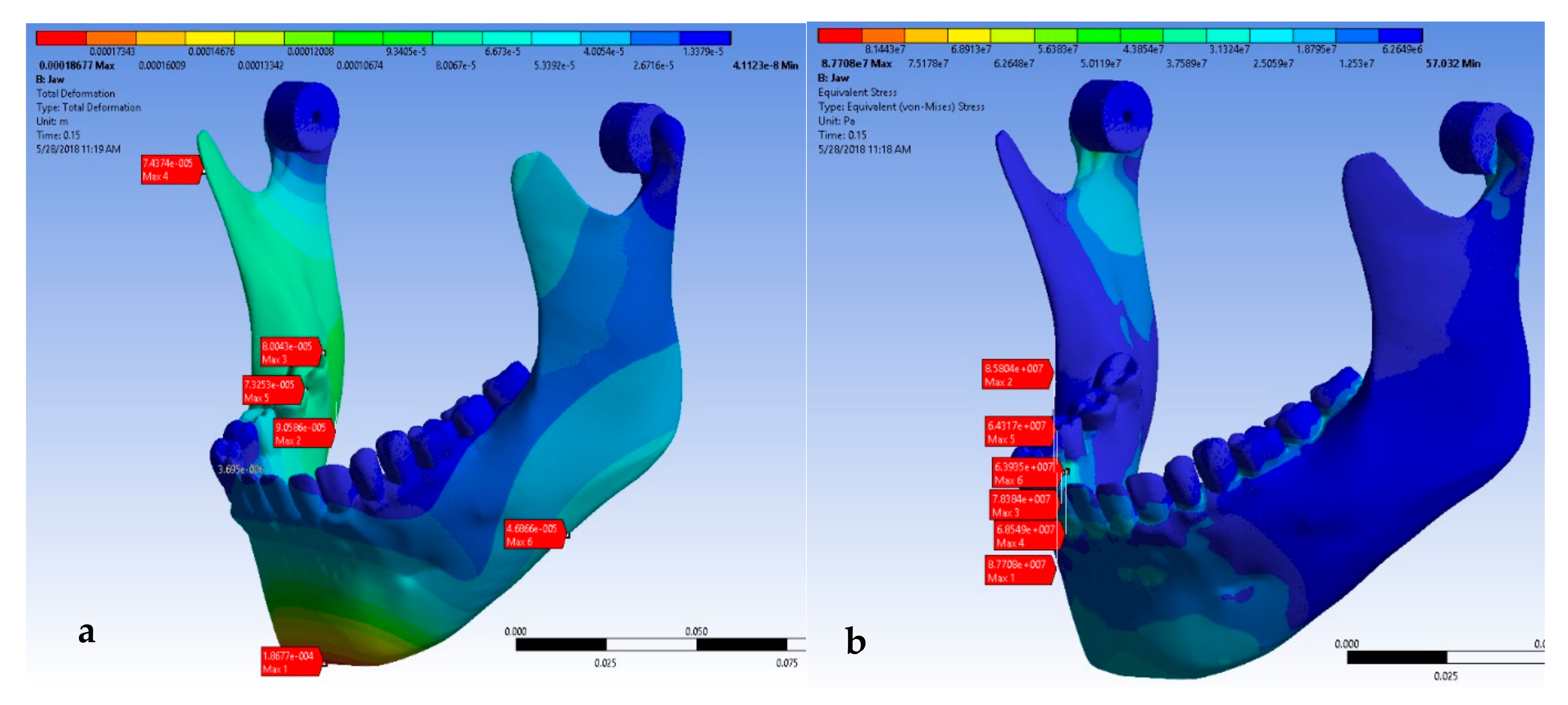
3.2.1. Impact on the Chin Region
Impact on the Chin with Mandibular Complete Dentition
Impact in the Chin Region of the Jaw with Missing Mandibular Molars
Impact in the Chin Region of the Jaw with Missing Third Molar, First and Second Premolars
Impact in the Chin Region of the Jaw with Missing Canine, Third Molar, First and Second Premolars
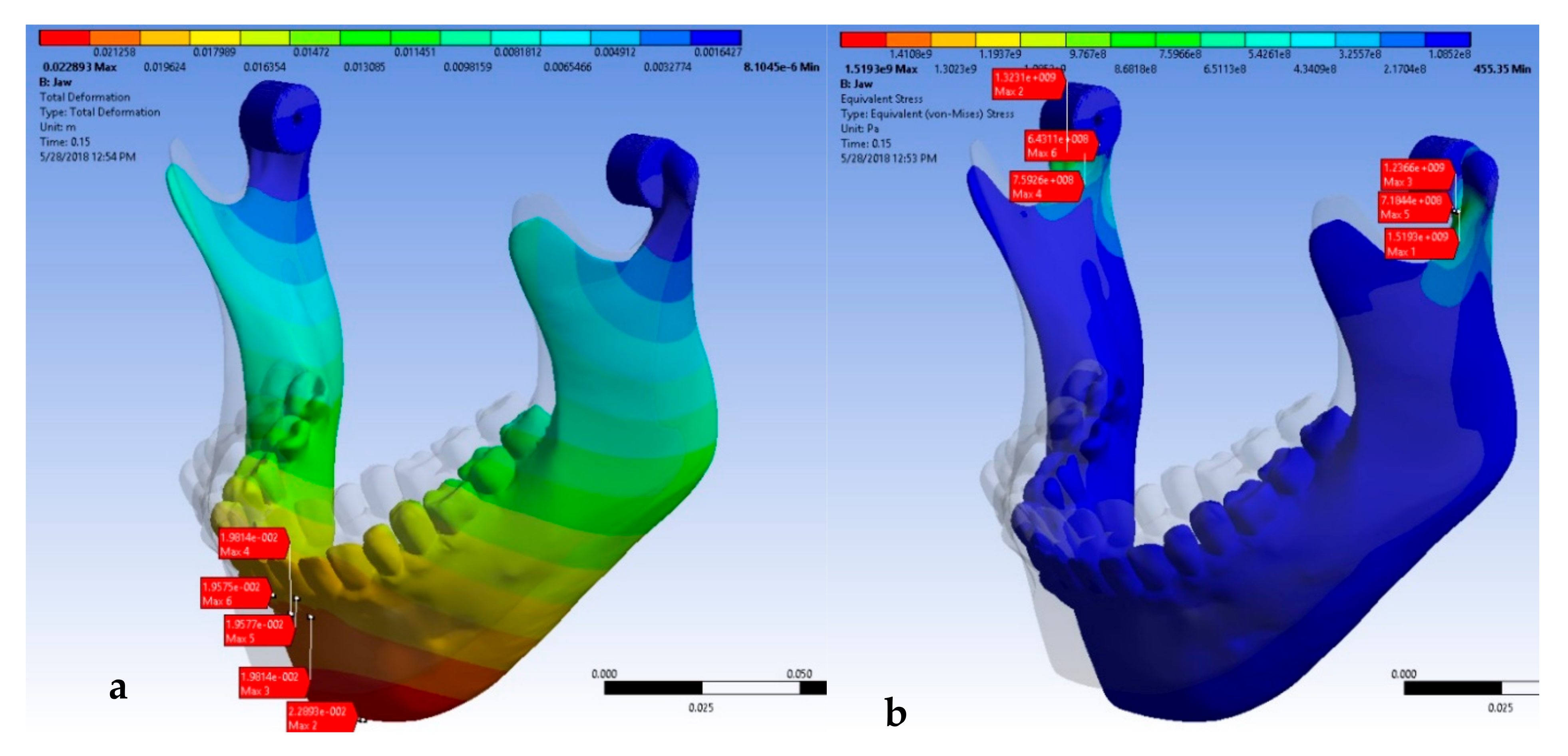
Impact in the Chin Region of Mandible with Complete Edentation
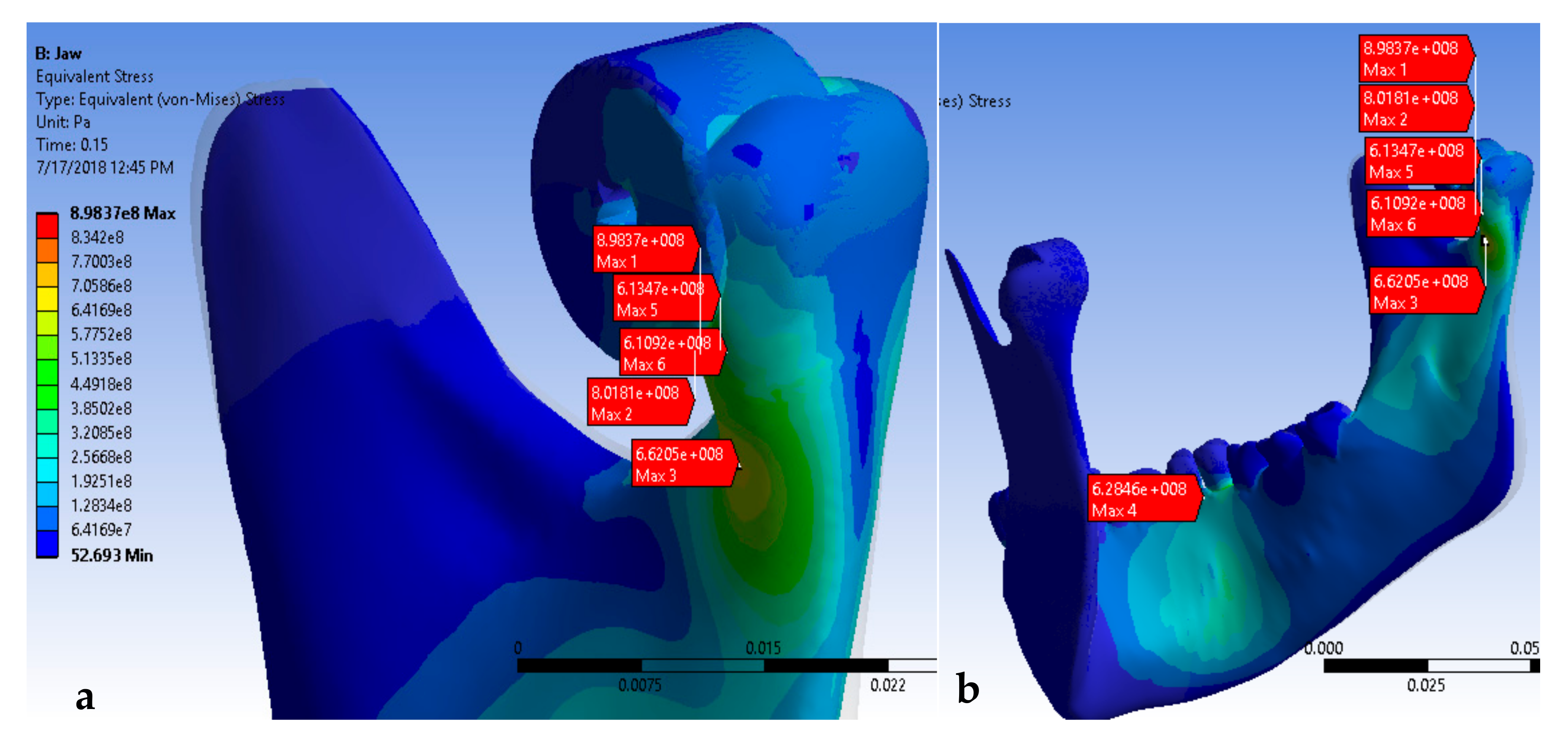
3.2.2. Impact on the Lateral Area of the Mandible
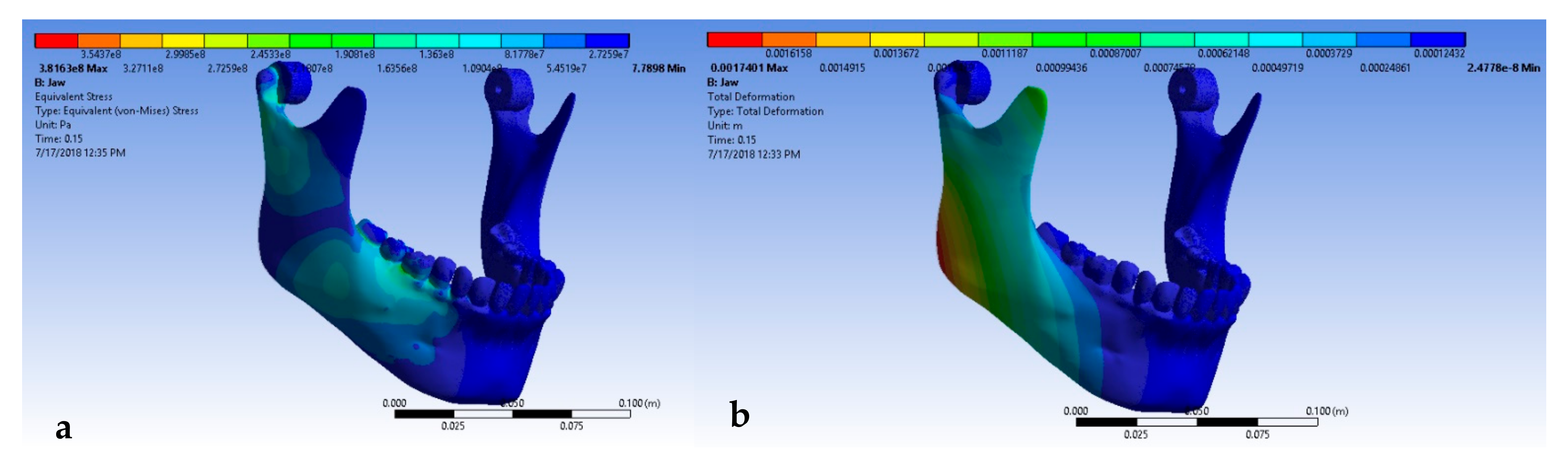
Lateral Impact on the Mandible in the Jaw with Complete Dentition
Lateral Impact on Mandible with Missing First, Second and Third Lower Molar
Lateral Impact on Mandible with Missing Third Molar, First and Second Premolars
Lateral Impact on Mandible with Missing the Third Molar, First and Second Premolars, and Canine
Lateral Impact on Mandible with Complete Edentation
3.3. Impact Stress with Edentation on Both Hemiarches
3.3.1. Impact on the Chin in the Mandible with Bilateral Edentation on the Molar Region
3.3.2. Impact on the Chin in the Mandible with Bilateral Edentation on the Molar, Premolar Region, and Canine
3.3.3. Lateral Impact on the Mandible with First, Second, and Third Molars Missing on Both Hemiarches
3.4. Lateral Impact on the Mandible with the Third Molar, First and Second Premolars, and Canine Absence on Both Hemiarches
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
References
- Farzan, R.; Farzan, A.; Farzan, A.; Karimpour, M.; Tolouie, M. A 6-Year Epidemiological Study of Mandibular Fractures in Traumatic Patients in North of Iran: Review of 463 Patients. World J. Plast. Surg. 2021, 10, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, A.G. Trends and Outcomes of Management of Mandibular Fractures. J. Craniofacial Surg. 2019, 30, 1245–1251. [Google Scholar] [CrossRef]
- Dreizin, D.; Nam, A.J.; Tirada, N.; Levin, M.D.; Stein, D.M.; Bodanapally, U.K.; Mirvis, S.E.; Munera, F. Multidetector CT of Mandibular Fractures, Reductions, and Complications: A Clinically Relevant Primer for the Radiologist. Radiographics 2016, 36, 1539–1564. [Google Scholar] [CrossRef]
- Algan, S.; Kara, M.; Cakmak, M.A.; Tan, O.; Cinal, H.; Barin, E.Z.; Inaloz, A. Experiences with a Modified Preauricular Mini Incision with Subdermally Dissection in Condylar and Subcondylar Fractures of the Mandible. J. Cranio-Maxillofac. Surg. 2018, 46, 588–593. [Google Scholar] [CrossRef]
- Bertin, E.; Louvrier, A.; Meyer, C.; Weber, E.; Barrabé, A. Pons An Epidemiologic Retrospective Study of Maxillofacial Traumatology in the Elderly. J. Stomatol. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Abukhder, M.; Mobarak, D. A Retrospective Cohort Study on the Aetiology and Characteristics of Maxillofacial Fractures Presenting to a Tertiary Centre in the UK. Ann. Med. Surg. 2022, 77, 103622. [Google Scholar] [CrossRef]
- Pickrell, B.; Serebrakian, A.; Maricevich, R. Mandible Fractures. Semin. Plast. Surg. 2017, 31, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Gillani, S.R.R.; Erkin, M.; Khan, M.; Abbas, M.; Khurshid khattak, N. Role of Environmental and Occupational Factors in Fall-related Maxillofacial Fractures. Clin. Exp. Dent. Res. 2022, 8, 737–774. [Google Scholar] [CrossRef] [PubMed]
- Sorenson, T.J.; Borad, V.; Schubert, W. A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma. Craniomaxillofac. Trauma Reconstr. 2022, 15, 28–33. [Google Scholar] [CrossRef]
- Diab, J.; Moore, M.H. Patterns and Characteristics of Maxillofacial Fractures in Women. Oral Maxillofac. Surg. 2022, 1–10. [Google Scholar] [CrossRef]
- Li, J.; Jiao, J.; Luo, T.; Wu, W. Biomechanical Evaluation of Various Internal Fixation Patterns for Unilateral Mandibular Condylar Base Fractures: A Three-Dimensional Finite Element Analysis. J. Mech. Behav. Biomed. Mater. 2022, 133, 105354. [Google Scholar] [CrossRef]
- Avci, T.; Omezli, M.M.; Torul, D. Investigation of the Biomechanical Stability of Cfr-PEEK in the Treatment of Mandibular Angulus Fractures by Finite Element Analysis. J. Stomatol. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Graillon, N.; Guyot, L.; Thollon, L.; Godio-Raboutet, Y.; Roux, M.-K.L.; Foletti, J.-M. Do Mandibular Titanium Miniplates Affect the Biomechanical Behaviour of the Mandible? A Preliminary Experimental Study. J. Stomatol. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Torreira, M.G.; Fernández, J.R. A Three-Dimensional Computer Model of the Human Mandible in Two Simulated Standard Trauma Situations. J. Cranio-Maxillofac. Surg. 2004, 32, 303–307. [Google Scholar] [CrossRef]
- Gomez, M.A.; Nahum, A.M. Biomechanics of Bone. In Accidental Injury; Nahum, A.M., Melvin, J.W., Eds.; Springer: New York, NY, USA, 2002; pp. 206–227. ISBN 978-1-4419-3168-9. [Google Scholar]
- Carter, D.R.; Spengler, D.M. Mechanical Properties and Composition of Cortical Bone. Clin. Orthop. 1978, 135, 192–217. [Google Scholar] [CrossRef]
- Burstein, A.H.; Reilly, D.T.; Martens, M. Aging of Bone Tissue: Mechanical Properties. J. Bone Jt. Surg. Am. 1976, 58, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Gregolin, R.F.; de Carvalho Zavaglia, C.A.; Tokimatsu, R.C.; Pereira, J.A. Biomechanical Stress and Strain Analysis of Mandibular Human Region from Computed Tomography to Custom Implant Development. Adv. Mater. Sci. Eng. 2017, 2017, 7525897. [Google Scholar] [CrossRef]
- Turner, C.H.; Burr, D.B. Basic Biomechanical Measurements of Bone: A Tutorial. Bone 1993, 14, 595–608. [Google Scholar] [CrossRef]
- Kimsal, J.; Baack, B.; Candelaria, L.; Khraishi, T.; Lovald, S. Biomechanical Analysis of Mandibular Angle Fractures. J. Oral Maxillofac. Surg. 2011, 69, 3010–3014. [Google Scholar] [CrossRef]
- Jung, B.T.; Kim, W.H.; Park, B.; Lee, J.-H.; Kim, B.; Lee, J.-H. Biomechanical Evaluation of Unilateral Subcondylar Fracture of the Mandible on the Varying Materials: A Finite Element Analysis. PLoS ONE 2020, 15, e0240352. [Google Scholar] [CrossRef]
- Syed, I.; Joshi, A.; Desai, A.K.; Anehosur, V. Occlusal Analysis Using T-Scan in Patients with Condylar Fractures When Managed by Closed Method. J. Craniofac. Surg. 2020, 31, e451–e459. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.J.; Chung, Y.H.; Cho, J.Y.; Burm, J.S. The Use of Microplates for Internal Fixation of Comminuted Mandibular Fractures. Ann. Plast. Surg. 2019, 82, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Datarkar, A.; Tayal, S.; Thote, A.; Galie, M. An In-Vitro Evaluation of a Novel Design of Miniplate for Fixation of Fracture Segments in the Transition Zone of Parasymphysis-Body Region of Mandible Using Finite Element Analysis. J. Cranio-Maxillo-fac. Surg. 2019, 47, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Singleton, C.; Manchella, S.; Nastri, A.; Bordbar, P. Mandibular Fractures—What a Difference 30 Years Has Made. Br. J. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, A.C.; Kaing, T.-L. Point-of-Care Computer-Assisted Design and Manufacturing Technology and Its Utility in Post-Traumatic Mandibular Reconstruction: An Australian Public Hospital Experience. SAGE Open Med. Case Rep. 2022, 10, 2050313X221103733. [Google Scholar] [CrossRef]
- Huang, C.-M.; Chan, M.-Y.; Hsu, J.-T.; Su, K.-C. Biomechanical Analysis of Subcondylar Fracture Fixation Using Miniplates at Different Positions and of Different Lengths. BMC Oral Health 2021, 21, 543. [Google Scholar] [CrossRef]
- Costa, F.W.G.; Bezerra, M.F.; Ribeiro, T.R.; Pouchain, E.C.; Sabóia, V.D.P.A.; Soares, E.C.S. Biomechanical Analysis of Titanium Plate Systems in Mandibular Condyle Fractures: A Systematized Literature Review. Acta Cir. Bras. 2012, 27, 424–429. [Google Scholar] [CrossRef]
- Mańkowski, J.; Piękoś, J.; Dominiak, K.; Klukowski, P.; Fotek, M.; Zawisza, M.; Żach, P. A Mandible with the Temporomandibular Joint-A New FEM Model Dedicated to Strength and Fatigue Calculations of Bonding Elements Used in Fracture and Defect Surgery. Materials 2021, 14, 5031. [Google Scholar] [CrossRef] [PubMed]
- WĄdoŁowski, P.; KrzesiŃski, G.; Gutowski, P. Finite Element Analysis of Mini-Plate Stabilization of Human Mandible Angle Fracture—A Comparative Study. Acta Bioeng. Biomech. 2020, 22, 105–116. [Google Scholar] [CrossRef]
- Joshi, U.; Kurakar, M. Assessment of Lingual Stability in Mandible Fracture: Monocortical Versus Bicortical Fixation Using FEM Analysis. J. Maxillofac. Oral Surg. 2018, 17, 514–519. [Google Scholar] [CrossRef]
- 3-Parts Anatomical Skull Model|3D CAD Model Library|GrabCAD. Available online: https://grabcad.com/library/3-parts-anatomical-skull-model (accessed on 18 June 2022).
- GrabCAD Making Additive Manufacturing at Scale Possible. Available online: https://grabcad.com/ (accessed on 18 June 2022).
- Hart, N.H.; Nimphius, S.; Rantalainen, T.; Ireland, A.; Siafarikas, A.; Newton, R.U. Mechanical Basis of Bone Strength: Influence of Bone Material, Bone Structure and Muscle Action. J. Musculoskelet. Neuronal Interact. 2017, 17, 114–139. [Google Scholar]
- ANSYS Products V19.0 Free Download {Full Version} for PC Windows. Available online: https://www.getintopces.com/ansys-products-v19-0-free-download/ (accessed on 18 June 2022).
- Madruga, C.F.L.; Ramos, G.F.; Borges, A.L.S.; Saavedra, G.D.S.F.A.; Souza, R.O.; Marinho, R.M.D.M.; Penteado, M.M. Stress Distribution in Modified Veneer Crowns: 3D Finite Element Analysis. Oral 2021, 1, 272–280. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.D.O.; da Silva-Concílio, L.R.; Ausiello, P.; Kalman, L. Influence of Implant-Abutment Contact Surfaces and Prosthetic Screw Tightening on the Stress Concentration, Fatigue Life and Microgap Formation: A Finite Element Analysis. Oral 2021, 1, 88–101. [Google Scholar] [CrossRef]
- Campaner, L.M.; Alves Pinto, A.B.; Demachkia, A.M.; Paes-Junior, T.J.D.A.; Pagani, C.; Borges, A.L.S. Influence of Cement Thickness on the Polymerization Shrinkage Stress of Adhesively Cemented Composite Inlays: Photoelastic and Finite Element Analysis. Oral 2021, 1, 168–180. [Google Scholar] [CrossRef]
- Dragulescu, D. Studierea Dinamicii Mandibulei si Modelarea de Implante Pentru Corectarea Prin Interventii Chirurgicale a Ruperilor Sale Accidentale. Available online: https://www.yumpu.com/en/document/view/53136953/studierea-dinamicii-mandibulei-si-modelarea-de-implante-pentru- (accessed on 19 June 2022).
- Hart, R.T.; Hennebel, V.V.; Thongpreda, N.; Van Buskirk, W.C.; Anderson, R.C. Modeling the Biomechanics of the Mandible: A Three-Dimensional Finite Element Study. J. Biomech. 1992, 25, 261–286. [Google Scholar] [CrossRef]
- Szucs, A.; Bujtar, P.; Sándor, G.; Barabás, J. Finite Element Analysis of the Human Mandible to Assess the Effect of Removing an Impacted Third Molar. J. Can. Dent. Assoc. 2010, 76, a72. [Google Scholar]
- Tanaka, E.; Tanne, K.; Sakuda, M. A Three-Dimensional Finite Element Model of the Mandible Including the TMJ and Its Application to Stress Analysis in the TMJ during Clenching. Med. Eng. Phys. 1994, 16, 316–322. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Gabryelczak, I. The Osteosynthesis of the Mandibular Head, Does the Way the Screws Are Positioned Matter? J. Clin. Med. 2022, 11, 2031. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Zieliński, R.; Konieczny, B.; Krasowski, M.; Okulski, J. Open Rigid Internal Fixation of Low-Neck Condylar Fractures of the Mandible: Mechanical Comparison of 16 Plate Designs. Materials 2020, 13, 1953. [Google Scholar] [CrossRef]
- d’Apuzzo, F.; Minervini, G.; Grassia, V.; Rotolo, R.P.; Perillo, L.; Nucci, L. Mandibular Coronoid Process Hypertrophy: Diagnosis and 20-Year Follow-Up with CBCT, MRI and EMG Evaluations. Appl. Sci. 2021, 11, 4504. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible. Cranio J. Craniomandib. Pract. 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. BioMed Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Scenario | Deformation [mm] | Stress [MPa] |
|---|---|---|---|
| Normal bite | Complete dentition | 0.02 | 4.3 |
| Impact on the anterior region, in the chin area | Complete dentition | 0.01 | 9.6 |
| Missing first, second and third molars | 0.02 | 25 | |
| Missing third molar and first and second premolars | 0.01 | 13.4 | |
| Missing third molar, first and second premolars, and canine | 0.01 | 13.65 | |
| Complete edentation | 1.6 | 1300 (>180) |
| Case | Scenario | Deformation [mm] | Stress [MPa] |
|---|---|---|---|
| Normal bite | Complete dentition | 0.24 | 109.04 |
| Impact on the lateral region, at the level of the gonion and the ascending ramus | Complete dentition | 1.3 | 662 |
| Missing first, second and third molars | 0.7 | 240 | |
| Missing third molar and first and second premolars | 0.7 | 241.5 | |
| Missing third molar, first and second premolars, and canine | 1.35 | 860 | |
| Complete edentation | 0.24 | 109.04 |
| Scenario | Impact on the Anterior Side, in the Chin Region | Impact on the Lateral Side, on the Angle of the Mandible | ||
|---|---|---|---|---|
| Edentation on One Hemiarch | Symmetrical Edentation | Edentation on One Hemiarch | Symmetrical Edentation | |
| Missing first, second and third molars | 25 | 25.29 | 662 | 659 |
| Missing third molar, first and second premolars, and canine | 13.65 | 13.51 | 241.5 | 241.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hedeșiu, M.; Pavel, D.G.; Almășan, O.; Pavel, S.G.; Hedeșiu, H.; Rafiroiu, D. Three-Dimensional Finite Element Analysis on Mandibular Biomechanics Simulation under Normal and Traumatic Conditions. Oral 2022, 2, 221-237. https://doi.org/10.3390/oral2030021
Hedeșiu M, Pavel DG, Almășan O, Pavel SG, Hedeșiu H, Rafiroiu D. Three-Dimensional Finite Element Analysis on Mandibular Biomechanics Simulation under Normal and Traumatic Conditions. Oral. 2022; 2(3):221-237. https://doi.org/10.3390/oral2030021
Chicago/Turabian StyleHedeșiu, Mihaela, Dan George Pavel, Oana Almășan, Sorin Gheorghe Pavel, Horia Hedeșiu, and Dan Rafiroiu. 2022. "Three-Dimensional Finite Element Analysis on Mandibular Biomechanics Simulation under Normal and Traumatic Conditions" Oral 2, no. 3: 221-237. https://doi.org/10.3390/oral2030021
APA StyleHedeșiu, M., Pavel, D. G., Almășan, O., Pavel, S. G., Hedeșiu, H., & Rafiroiu, D. (2022). Three-Dimensional Finite Element Analysis on Mandibular Biomechanics Simulation under Normal and Traumatic Conditions. Oral, 2(3), 221-237. https://doi.org/10.3390/oral2030021