

Treating Preeclampsia in the COVID-19 Era: Is Allopurinol Useful as an Adjuvant Therapy? A Case Report and Review of the Literature

 ,
,  ,
, 
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, S.L.; Wallace, E.M.; Walker, D.W. Antioxidant therapies: A potential role in perinatal medicine. Neuroendocrinology 2012, 96, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Nunes, P.R.; Romao-Veiga, M.; Serrao Peracoli, M.T.; Peracoli, J.C.; Sandrim, V.C. Potential role of uric acid to activate NLRP3 inflammasome triggering endothelial dysfunction in preeclampsia. Clin. Immunol. Commun. 2022, 2, 69–75. [Google Scholar] [CrossRef]
- Komiya, T.; Sato, T. Long-term follow-up study of anti-acetylcholine receptor antibody titers and clinical symptoms in patients with myasthenia gravis. Rinsho Shinkeigaku 1988, 28, 727–734. [Google Scholar] [PubMed]
- Zuabidi, A.L.; Mezaal, Z.F. The Role of Uric Acid in Predicting Preeclampsia Women. J. Chem. Pharm. Res. 2016, 8, 1175–1179. [Google Scholar]
- Michalczyk, M.; Celewicz, A.; Celewicz, M.; Woźniakowska-Gondek, P.; Rzepka, R. The Role of Inflammation in the Pathogenesis of Preeclampsia. Mediat. Inflamm 2020, 2020, 3864941. [Google Scholar] [CrossRef]
- Ryu, A.; Cho, N.J.; Kim, Y.S.; Lee, E.Y. Predictive value of serum uric acid levels for adverse perinatal outcomes in preeclampsia. Medicine 2019, 98, e15462. [Google Scholar] [CrossRef] [PubMed]
- Bellos, I.; Pergialiotis, V.; Loutradis, D.; Daskalakis, G. The prognostic role of serum uric acid levels in preeclampsia: A meta-analysis. J. Clin. Hypertens. 2020, 22, 826–834. [Google Scholar] [CrossRef]
- Hassen, F.S.; Malik, T.; Dejenie, T.A. Evaluation of serum uric acid and liver function tests among pregnant women with and without preeclampsia at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. PLoS ONE 2022, 17, e0272165. [Google Scholar] [CrossRef]
- Negi, M.; Mulla, M.J.; Han, C.S.; Abrahams, V.M. Allopurinol inhibits excess glucose-induced trophoblast IL-1β and ROS production. Reproduction 2020, 159, 73–80. [Google Scholar] [CrossRef]
- Moreno Santillan, A.A.; Briones Garduño, J.C.; Diaz de Leon Ponce, M.A. Uric Acid in Pregnancy: New Concepts. Contrib. Nephrol. 2018, 192, 110–115. [Google Scholar] [CrossRef]
- Bainbridge, S.A.; Roberts, J.M. Uric acid as a pathogenic factor in preeclampsia. Placenta 2008, 29 (Suppl. A), 67–72. [Google Scholar] [CrossRef] [PubMed]
- Sudjai, D.; Satho, P. Relationship between maternal serum uric acid level and preeclampsia with or without severe features. J. Obs. Gynaecol. 2022, 2704–2708. [Google Scholar] [CrossRef] [PubMed]
- Nana, M.; Nelson-Piercy, C. COVID-19 in pregnancy. Clin. Med. 2021, 21, e446–e450. [Google Scholar] [CrossRef]
- Mullin, A.M.; Handley, S.C.; Lundsberg, L.; Elovitz, M.A.; Lorch, S.A.; McComb, E.J.; Montoya-Williams, D.; Yang, N.; Dysart, K.; Son, M.; et al. Changes in preterm birth during the COVID-19 pandemic by duration of exposure and race and ethnicity. J. Perinatol. 2022, 42, 1346–1352. [Google Scholar] [CrossRef]
- Ayed, A.; Embaireeg, A.; Benawadh, A.; Al-Fouzan, W.; Hammoud, M.; Al-Hathal, M.; Alzaydai, A.; Ahmad, A.; Ayed, M. Maternal and perinatal characteristics and outcomes of pregnancies complicated with COVID-19 in Kuwait. BMC Pregnancy Childbirth 2020, 20, 754. [Google Scholar] [CrossRef]
- Novoa, R.H.; Quintana, W.; Llancarí, P.; Urbina-Quispe, K.; Guevara-Ríos, E.; Ventura, W. Maternal clinical characteristics and perinatal outcomes among pregnant women with coronavirus disease 2019. A systematic review. Travel Med. Infect. Dis. 2021, 39, 101919. [Google Scholar] [CrossRef]
- Gabrieli, D.; Cahen-Peretz, A.; Shimonovitz, T.; Marks-Garber, K.; Amsalem, H.; Kalish, Y.; Lavy, Y.; Walfisch, A. Thromboembolic events in pregnant and puerperal women after COVID-19 lockdowns: A retrospective cohort study. Int. J. Gynaecol. Obstet. 2021, 155, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Mirbeyk, M.; Saghazadeh, A.; Rezaei, N. A systematic review of pregnant women with COVID-19 and their neonates. Arch. Gynecol. Obstet. 2021, 304, 5–38. [Google Scholar] [CrossRef] [PubMed]
- Zitiello, A.; Grant, G.E.; Ben Ali, N.; Feki, A. Thrombocytopaenia in pregnancy: The importance of differential diagnosis during the COVID-19 pandemic. J. Matern. Fetal Neonatal. Med. 2022, 35, 2414–2416. [Google Scholar] [CrossRef]
- Moses, M.L.; Kazzi, N.G.; Lee, L. Severe Thrombocytopenia in a Pregnant Patient with Asymptomatic COVID-19 Infection: A Case Report. Cureus 2021, 13, e12990. [Google Scholar] [CrossRef]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Kadir, R.A.; Kobayashi, T.; Iba, T.; Erez, O.; Thachil, J.; Kazi, S.; Malinowski, A.K.; Othman, M. COVID-19 coagulopathy in pregnancy: Critical review, preliminary recommendations, and ISTH registry-Communication from the ISTH SSC for Women’s Health. J. Thromb. Haemost. 2020, 18, 3086–3098. [Google Scholar] [CrossRef] [PubMed]
- Mullins, E.; Evans, D.; Viner, R.M.; O’Brien, P.; Morris, E. Coronavirus in pregnancy and delivery: Rapid review. Ultrasound Obstet. Gynecol. 2020, 55, 586–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller-Deile, J.; Schiffer, M. Preeclampsia from a renal point of view: Insides into disease models, biomarkers and therapy. World J. Nephrol. 2014, 3, 169–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Veen, T.R.; Haeri, S. Gout in pregnancy: A case report and review of the literature. Gynecol. Obstet. Investig. 2015, 79, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Aljelehawy, Q.A.H.; Almonem Alftlawy, R.A.M.; Alavi, H. The role of hyperuricemia in the pathophysiology of preeclampsia. Cent. Asian J. Med. Pharm. Sci. Innov. 2022, 2, 37–45. [Google Scholar]
- Tálosi, G.; Németh, I.; Pintér, S. Inhibitory effects of methylxanthines on the pre-eclamptic-like symptoms in ewes. Eur. J. Obs. Gynecol. Reprod. Biol. 2001, 99, 25–32. [Google Scholar] [CrossRef]
- Wang, I.K.; Chen, J.H.; Muo, C.H.; Chou, C.Y.; Liu, Y.L.; Lin, S.Y.; Liang, C.C.; Yen, T.H.; Sung, F.C. Subsequent risk of gout for women with hypertensive disorders in pregnancy: A retrospective cohort study. J. Hypertens. 2016, 34, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, T.; McGuire, W. Allopurinol for preventing mortality and morbidity in newborn infants with hypoxic-ischaemic encephalopathy. Cochrane Database Syst. Rev. 2012, 7, CD006817. [Google Scholar] [CrossRef]
- Fontana, R.J.; Li, Y.J.; Phillips, E.; Saeed, N.; Barnhart, H.; Kleiner, D.; Hoofnagle, J. Allopurinol hepatotoxicity is associated with human leukocyte antigen Class I alleles. Liver Int. 2021, 41, 1884–1893. [Google Scholar] [CrossRef]
- Kaandorp, J.J.; Benders, M.J.; Schuit, E.; Rademaker, C.M.; Oudijk, M.A.; Porath, M.M.; Oetomo, S.B.; Wouters, M.G.; van Elburg, R.M.; Franssen, M.T.; et al. Maternal allopurinol administration during suspected fetal hypoxia: A novel neuroprotective intervention? A multicentre randomised placebo controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F216–F223. [Google Scholar] [CrossRef]
- Kebria, M.M.; Milan, P.B.; Peyravian, N.; Kiani, J.; Khatibi, S.; Mozafari, M. Stem cell therapy for COVID-19 pneumonia. Mol. Biomed. 2022, 3, 6. [Google Scholar] [CrossRef]
- Alem, M.M. Allopurinol and endothelial function: A systematic review with meta-analysis of randomized controlled trials. Cardiovasc. Ther. 2018, 36, e12432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panickar, R.; Wo, W.K.; Ali, N.M.; Tang, M.M.; Ramanathan, G.R.L.; Kamarulzaman, A.; Aziz, Z. Allopurinol-induced severe cutaneous adverse drug reactions: Risk minimization measures in Malaysia. Pharm. Drug Saf. 2020, 29, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Stegeman, R.; Nijman, M.; Breur, J.M.P.J.; Groenendaal, F.; Haas, F.; Derks, J.B.; Nijman, J.; van Beynum, I.M.; Taverne, Y.J.H.J.; Bogers, A.J.J.C.; et al. CeRebrUm and CardIac Protection with ALlopurinol in Neonates with Critical Congenital Heart Disease Requiring Cardiac Surgery with Cardiopulmonary Bypass (CRUCIAL): Study protocol of a phase III, randomized, quadruple-blinded, placebo-controlled, Dutch multicenter trial. Trials 2022, 23, 174. [Google Scholar] [CrossRef] [PubMed]
- Castro, V.M.F.; Melo, A.C.; Belo, V.S.; Chaves, V.E. Effect of allopurinol and uric acid normalization on serum lipids hyperuricemic subjects: A systematic review with meta-analysis. Clin. Biochem. 2017, 50, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Stamp, L.K.; Barclay, M.L. How to prevent allopurinol hypersensitivity reactions. Rheumatology 2018, 57, i35–i41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, P.; Tao, M.; Zhao, H.; Sheng, Y.; Qiu, J.; Xu, Y.; Li, H.; Wang, H.; Cao, G.; Ronco, C.; et al. Successful Treatment of Allopurinol-Induced Severe Skin Reactions with Double Filtration Plasmapheresis: A Case Report. Blood Purif. 2020, 49, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Yun, J.; Kang, D.Y.; Park, J.W.; Koh, Y.I.; Kim, S.; Kim, S.H.; Nam, Y.H.; Jeong, Y.Y.; Kim, C.W.; et al. Unique Clinical Characteristics and Prognosis of Allopurinol-Induced Severe Cutaneous Adverse Reactions. J. Allergy Clin. Immunol. Pract. 2019, 7, 2739–2749.e3. [Google Scholar] [CrossRef]
- Simsek, M.; Opperman, R.C.M.; Mulder, C.J.J.; Lambalk, C.B.; de Boer, N.K.H. The teratogenicity of allopurinol: A comprehensive review of animal and human studies. Reprod. Toxicol. 2018, 81, 180–187. [Google Scholar] [CrossRef]
- Hoeltzenbein, M.; Stieler, K.; Panse, M.; Wacker, E.; Schaefer, C. Allopurinol Use during Pregnancy—Outcome of 31 Prospectively Ascertained Cases and a Phenotype Possibly Indicative for Teratogenicity. PLoS ONE 2013, 8, e66637. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Results During Period of Admission Mother | Blood Results Newborn | |||||||
|---|---|---|---|---|---|---|---|---|
| Tests | Normal Value | 13 July 2022 | 14 July 2022 | 15 July 2022 | 22 July 2022 | 26 July 2022 | 27 July 2022 | 26 July 2022 |
| Leukocytes (WBC) | 4.00–10.00 × 109/L | 14.10 × 109/L | 10.82 × 109/L | 12.5 × 109/L | 24.7 × 109/L | |||
| Lymphocytes (Lymphs) | 1.0–4.1 × 109/L | 1.2 × 109/L | 2.27 × 109/L | 2.05 × 109/L | 23.0 × 109/L | |||
| Hemoglobin (HGB) | 11.5–16 g/dL | 9.9 g/dL | 10.5 g/dL | 10.9 g/dL | 14.2 g/dL | |||
| Hematocrit (HCT) | 35–48% | 32.4% | 34.50% | 35.8% | 44.8% | |||
| Platelets (PLT) | 150–450 × 109/L | 280 × 109/L | 360 × 109/L | 400 × 109/L | 213 × 109/L | |||
| INR | 0.8–1.2 | 0.87 | 0.94 | |||||
| APTT | 25–38 s | 29.9 s | 25.9 s | |||||
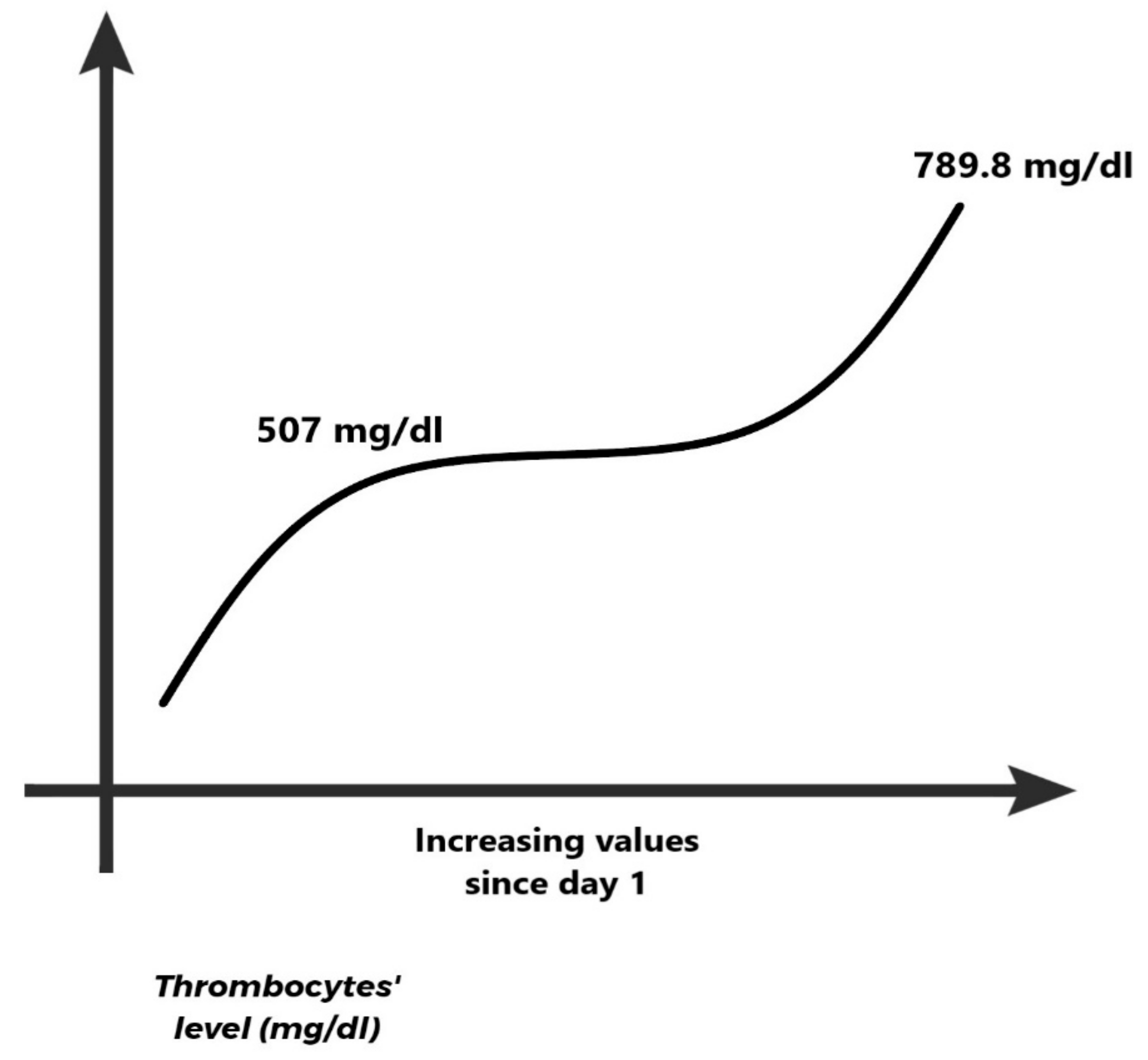
| Fibrinogen | 180–450 mg/dL | 507.4 mg/dL | 789.8 mg/dL | |||||
| Creatinine | 0.50–0.90 mg/dL | 0.70 mg/dL | 0.53 mg/dL | |||||
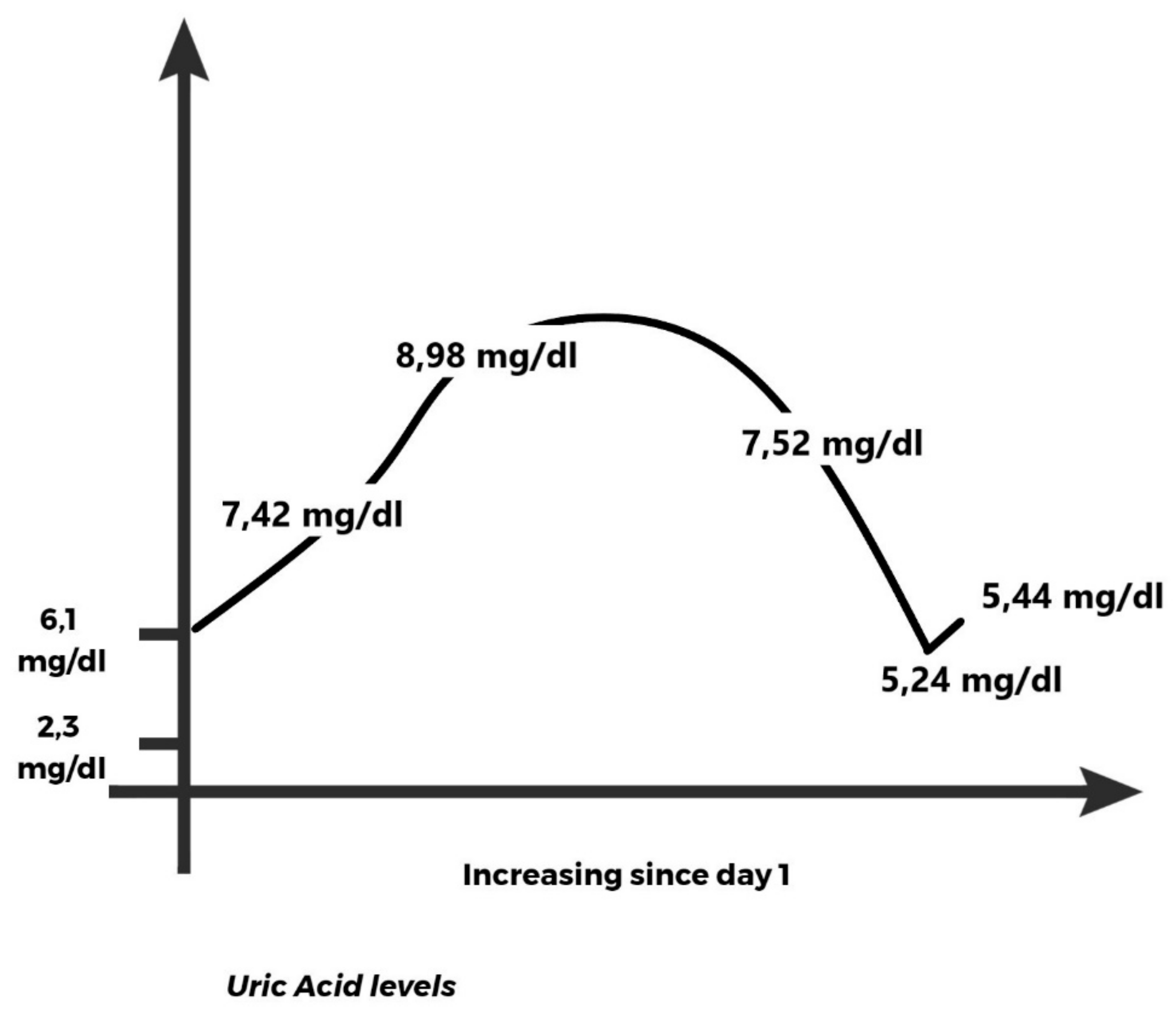
| Uric acid | 2.3–6.10 mg/dL | 7.42 mg/dL | 8.98 mg/dL | 7.52 mg/dL | 5.24 mg/dL | 5.44 mg/dL | ||
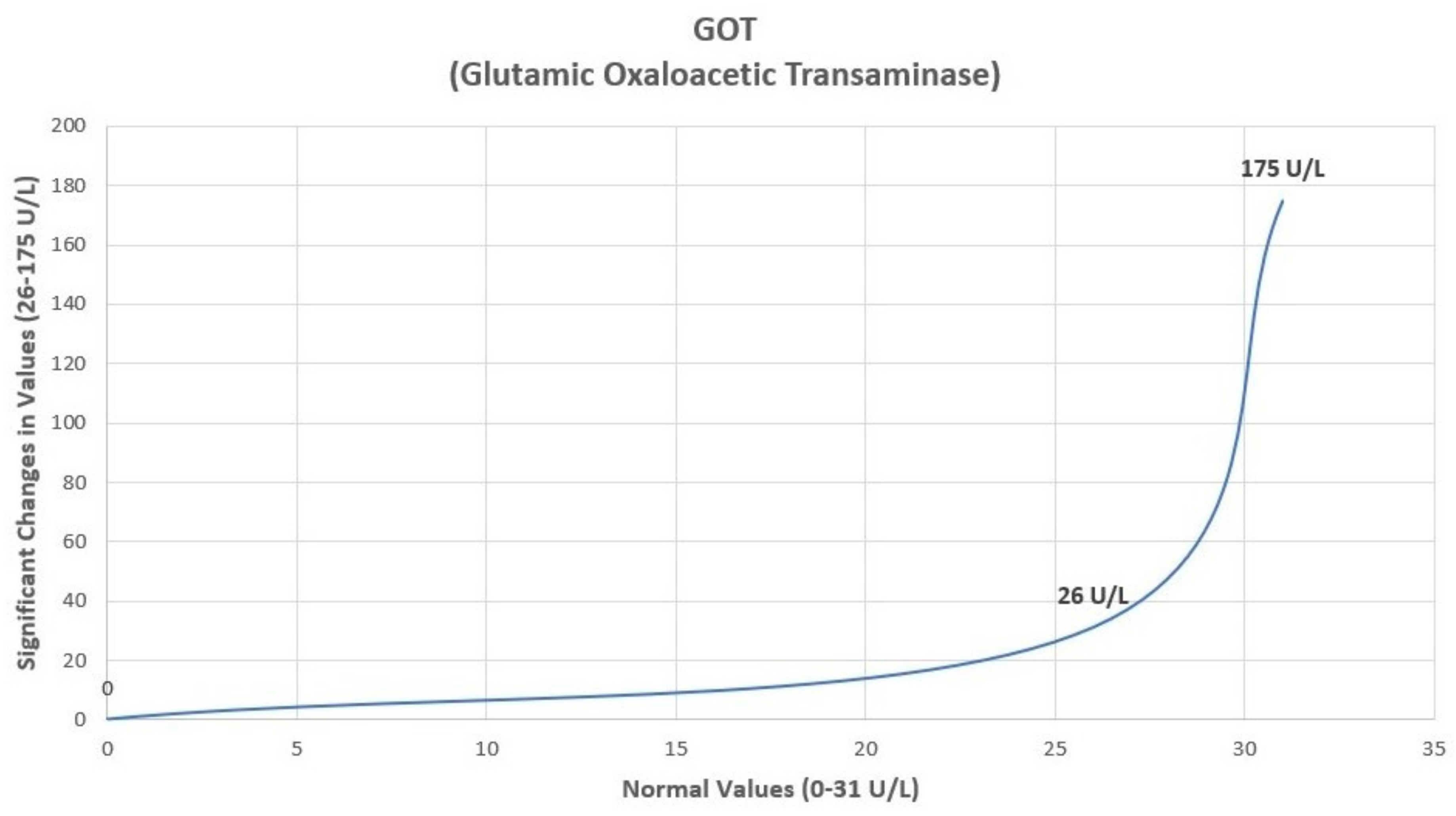
| GOT/ALT | 0.00–31.00 U/I | 26 U/I | 175 U/I | 62 U/I | 53 U/I | |||
| GPT/AST | 0.00–34.00 U/I | 21 U/I | 388 U/I | 171 U/I | 15 U/I | |||
| C Reactive Protein | 0.00–5.00 mg/L | 51.3 mg/L | 103.83 mg/L | 108.8 mg/L | 1.68 mg/L | |||
| Proteinuria | <150 mg/24 h | 400 mg/24 h | ||||||
| COVID-19 (PCR) | SARS-CoV-2 infection was positive by PCR testing. | Negative by PCR testing | ||||||
| Cultures | All cultures were negative | All cultures were negative | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitranovici, M.-I.; Chiorean, D.M.; Mureșan, M.C.; Buicu, C.-F.; Moraru, R.; Moraru, L.; Cotoi, T.C.; Cotoi, O.S.; Toru, H.S.; Apostol, A.; et al. Treating Preeclampsia in the COVID-19 Era: Is Allopurinol Useful as an Adjuvant Therapy? A Case Report and Review of the Literature. Stresses 2023, 3, 125-135. https://doi.org/10.3390/stresses3010010
Mitranovici M-I, Chiorean DM, Mureșan MC, Buicu C-F, Moraru R, Moraru L, Cotoi TC, Cotoi OS, Toru HS, Apostol A, et al. Treating Preeclampsia in the COVID-19 Era: Is Allopurinol Useful as an Adjuvant Therapy? A Case Report and Review of the Literature. Stresses. 2023; 3(1):125-135. https://doi.org/10.3390/stresses3010010
Chicago/Turabian StyleMitranovici, Melinda-Ildiko, Diana Maria Chiorean, Maria Cezara Mureșan, Corneliu-Florin Buicu, Raluca Moraru, Liviu Moraru, Titiana Cornelia Cotoi, Ovidiu Simion Cotoi, Havva Serap Toru, Adrian Apostol, and et al. 2023. "Treating Preeclampsia in the COVID-19 Era: Is Allopurinol Useful as an Adjuvant Therapy? A Case Report and Review of the Literature" Stresses 3, no. 1: 125-135. https://doi.org/10.3390/stresses3010010
APA StyleMitranovici, M. -I., Chiorean, D. M., Mureșan, M. C., Buicu, C. -F., Moraru, R., Moraru, L., Cotoi, T. C., Cotoi, O. S., Toru, H. S., Apostol, A., Turdean, S. G., Petre, I., Mărginean, C., Oală, I. E., Ivan, V., & Pușcașiu, L. (2023). Treating Preeclampsia in the COVID-19 Era: Is Allopurinol Useful as an Adjuvant Therapy? A Case Report and Review of the Literature. Stresses, 3(1), 125-135. https://doi.org/10.3390/stresses3010010