
Prediction of Recovery from Traumatic Brain Injury with EEG Power Spectrum in Combination of Independent Component Analysis and RUSBoost Model

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcome Assessment
2.2. TBI Patients
2.3. EEG Recordings
2.4. EEG Data Preprocessing
2.5. Data Preparation
2.6. EEG Feature Extraction
2.7. RUSBoost Prediction Model
| Algorithm 1 RUSBoost Algorithm. |
Input: Given a set R of examples , , ⋯, with minority class . Weak learner (decision trees), WeakLearn. Number of iteration, T Desired percentage of total examples to be represented by the minority class, N
Output: The final hypothesis: |
2.8. Evaluation in Imbalanced Dataset
- The sensitivity, often referred to as the True Positive Rate, , is expressed in terms of:indicates the ability of a classifier to identify a positive class correctly. It ranges from 0 to 1, with 1 being the perfect score.
- The specificity, alternatively referred to as the True Negative Rate, , is determined as;denotes the ability of a classifier to identify a negative class correctly. The perfect score is 1, and 0 is the worst measure.
- G-mean (geometric mean), is denoted as;G-Mean introduced by [53] quantifies the ability of a classifier to balance classification accuracy between positive and negative classes. By combining the G-Means of and , a low G-Mean score indicates a highly discriminative classifier toward one class and vice versa.
- F1 score describes the trade-off between precision and recall in the positive class. This well-known metric is perfectly suitable for skewed dataset problem that is determined as;It is a numeric value between 0 and 1, with 1 representing the perfect value.
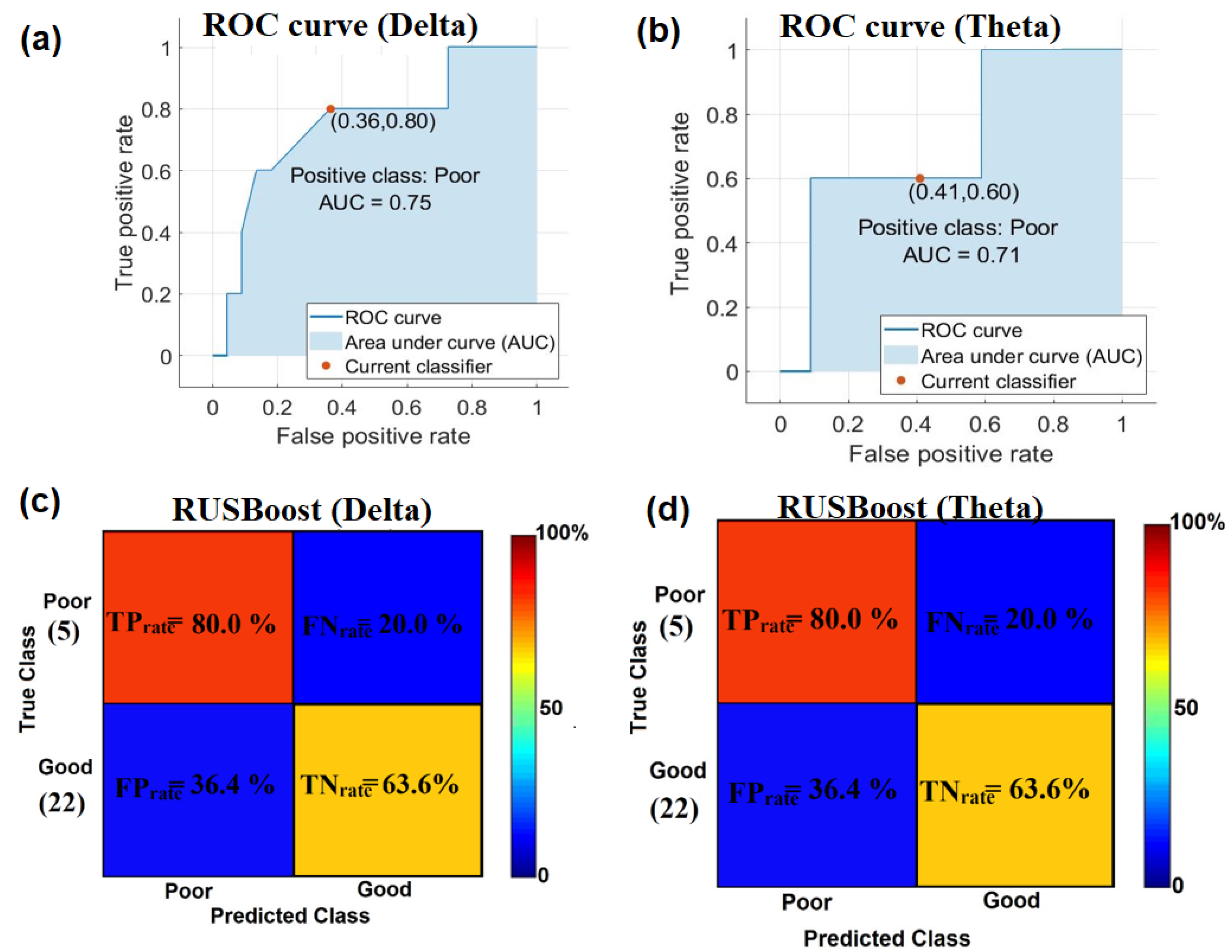
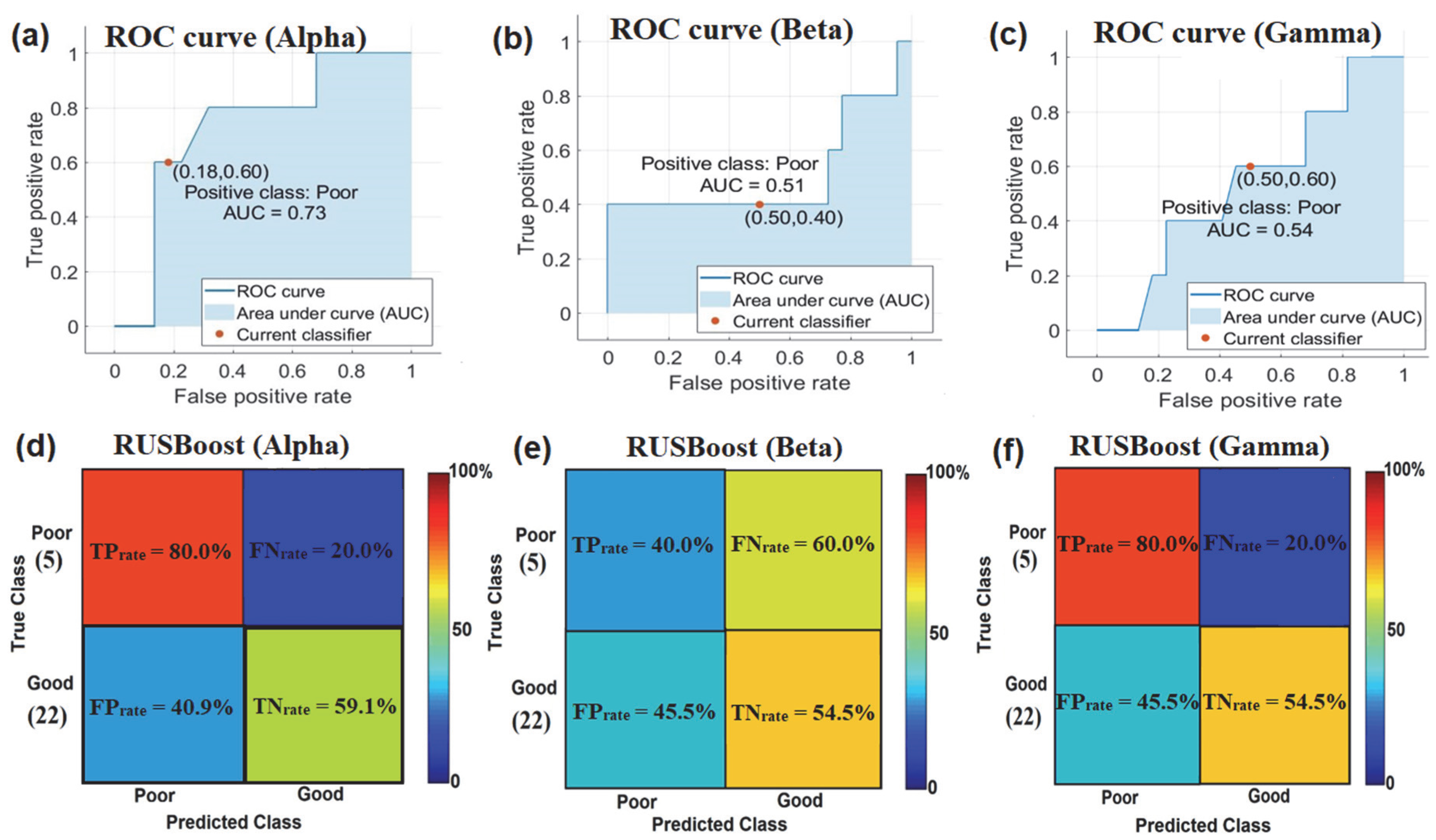
- Area Under Curve (AUC) is a popular overall model performance evaluation, especially for rating binary classifiers in the presence of class imbalance. Receiver operating characteristic (ROC) equals to AUC. To generate the ROC curve, we plotted the against the false positive rate , which is calculated as follows:It should be noted that higher AUC values imply a better ROC curve and, thus resulting in better performance.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Moppett, I.K. Traumatic brain injury: Assessment, resuscitation and early management. Br. J. Anesth. 2007, 99, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MRC CRASH Trial Collaborators. Predicting outcome after traumatic brain injury: Practical prognostic models based on large cohort of international patients. BMJ 2008, 336, 425–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noor, N.S.E.M.; Ibrahim, H. Predicting outcomes in patients with traumatic brain injury using machine learning models. In Proceedings of the Intelligent Manufacturing and Mechatronics, Melaka, Malaysia, 8 July 2019; Jamaludin, Z., Mokhtar, M.N.A., Eds.; Springer: Singapore, 2019; pp. 12–20. [Google Scholar]
- Lee, H.; Mizrahi, M.A.; Hartings, J.A.; Sharma, S.; Pahren, L.; Ngwenya, L.B.; Moseley, B.D.; Privitera, M.; Tortella, F.C.; Foreman, B. Continuous electroencephalography after moderate to severe traumatic brain injury. Crit. Care Med. 2019, 47, 574–582. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Marmarou, A.; Murray, G.D.; Teasdale, S.G.M.; Steyerberg, E.W. Prognosis and clinical trial design in traumatic brain injury: The IMPACT study. J. Neurotrauma 2007, 24, 232–238. [Google Scholar] [CrossRef]
- Fidali, B.C.; Stevens, R.D.; Claassen, J. Novel approaches to prediction in severe brain injury. Curr. Opin. Neurol. 2020, 33, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Emami, P.; Czorlich, P.; Fritzsche, F.S.; Westphal, M.; Rueger, J.M.; Lefering, R.; Hoffmann, M. Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: A retrospective, multicenter cohort study. J. Neurosurg. 2017, 126, 760–767. [Google Scholar] [CrossRef]
- Duncan, C.C.; Summers, A.C.; Perla, E.J.; Coburn, K.L.; Mirsky, A.F. Evaluation of traumatic brain injury: Brain potentials in diagnosis, function, and prognosis. Int. J. Psychophysiol. 2011, 82, 24–40. [Google Scholar] [CrossRef]
- Haveman, M.E.; Putten, M.J.A.M.V.; Hom, H.W.; Eertman-Meyer, C.J.; Beishuizen, A.; Tjepkema-Cloostermans, M.C. Predicting outcome in patients with moderate to severe traumatic brain injury using electroencephalography. Crit. Care 2019, 23, 401. [Google Scholar] [CrossRef] [Green Version]
- Mikola, A.; Ratsep, I.; Sarkela, M.; Lipping, T. Prediction of outcome in traumatic brain injury patients using long-term qEEG features. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Milan, Italy, 25–29 August 2015; pp. 1532–1535. [Google Scholar]
- Stefan, S.; Schorr, B.; Lopez-Rolon, A.; Kolassa, I.-T.; Shock, J.P.; Rosenfelder, M.; Heck, S.; Bender, A. Consciousness indexing and outcome prediction with resting-state EEG in severe disorders of consciousness. Brain Topogr. 2018, 31, 848–862. [Google Scholar] [CrossRef]
- McNerney, M.W.; Hobday, T.; Cole, B.; Ganong, R.; Winans, N.; Matthews, D.; Hood, J.; Lane, S. Objective classification of mTBI using machine learning on a combination of frontopolar electroencephalography measurements and self-reported symptoms. Sports Med. Open 2019, 5, 14. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.Q.; Abdullah, M.Z.; Abdullah, J.M.; Azman, A.; Ibrahim, H. Screening of Moderate Traumatic Brain Injury from Power Feature of Resting-State Electroencephalography using Support Vector Machine. In Proceedings of the 2nd International Conference on Electronics and Electrical Engineering Technology, Penang, Malaysia, 25–27 September 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 99–103. [Google Scholar]
- Lai, C.Q.; Abdullah, M.Z.; Hamid, A.A.; Abdullah, J.M.; Azman, A.; Ibrahim, H. Moderate Traumatic Brain Injury Identification from Power Spectral Density of Electroencephalography’s Frequency Bands using Support Vector Machine. In Proceedings of the IEEE International Circuits and Systems Symposium (ICSyS), Kuantan, Malaysia, 18–19 September 2019; pp. 1–4. [Google Scholar]
- Lai, C.Q.; Ibrahim, H.; Hamid, A.I.A.; Abdullah, J.M. Classification of Non-Severe Traumatic Brain Injury from Resting-State EEG Signal Using LSTM Network with ECOC-SVM. Sensors 2020, 20, 5234. [Google Scholar] [CrossRef]
- Lai, C.Q.; Ibrahim, H.; Abdullah, M.Z.; Azman, A.; Abdullah, J.M. Detection of moderate traumatic brain injury from resting-state eye-closed electroencephalography. Comput. Intell. Neurosci. 2020, 2020, 8923906. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.Q.; Ibrahim, H.; Abdullah, J.M.; Azman, A.; Abdullah, M.Z. Convolutional Neural Network Utilizing Error-Correcting Output Codes Support Vector Machine for Classification of Non-Severe Traumatic Brain Injury From Electroencephalogram Signal. IEEE Access 2021, 9, 24946. [Google Scholar] [CrossRef]
- Brink, R.L.V.; Nieuwenhuis, S.; Boxtel, G.J.M.V.; Luijtelaar, G.V.; Eilander, H.J.; Wijnen, V.J.M. Task-free spectral EEG dynamics track and predict patient recovery from severe acquired brain injury. Neuroimage Clin. 2018, 17, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Al-Fahoum, A.S.; Al-Fraihat, A.A. Methods of EEG signal features extraction using linear analysis in frequency and time-frequency domains. ISRN Neurosci. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushkudiani, N.A.; Hukkelhoven, C.W.P.M.; Hernández, A.V.; Murray, G.D.; Choi, S.C.; Maas, A.I.R.; Steyerberg, E.W. A systematic review finds methodological improvements necessary for prognostic models in determining traumatic brain injury outcomes. J. Clin. Epidemiol. 2008, 61, 331–343. [Google Scholar] [CrossRef]
- Rapp, P.E.; Keyser, D.O.; Albano, A.; Hernandez, R.; Gibson, D.B.; Zambon, R.A.; Hairston, W.D.; Hughes, J.D.; Krystal, A.; Nichols, A.S. Traumatic brain injury detection using electrophysiological methods. Front. Hum. Neurosci. 2015, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Pauli, R.; O’Donnell, A.; Cruse, D. Resting-State Electroencephalography for Prognosis in Disorders of Consciousness Following Traumatic Brain Injury. Front. Neurol. 2020, 11, 586945. [Google Scholar] [CrossRef]
- Noor, N.S.E.M.; Ibrahim, H. Machine learning algorithms and quantitative electroencephalography predictors for outcome prediction in traumatic brain injury: A systematic review. IEEE Access 2020, 8, 102075–102092. [Google Scholar] [CrossRef]
- Ramos-Lima, L.F.; Waikamp, V.; Salgado, T.A.; Passos, I.C.; Freitas, L.H.M. The use of machine learning techniques in trauma-related disorders: A systematic review. J. Psychiatr. Res. 2020, 121, 159–172. [Google Scholar] [CrossRef]
- Subasi, A. Practical Guide for Biomedical Signals Analysis Using Machine Learning Techniques: A MATLAB Based Approach, 1st ed.; Academic Press: Cambridge, MA, USA, 2019; p. 456. [Google Scholar]
- Sakai, K.; Yamada, K. Machine learning studies on major brain diseases: 5-year trends of 2014–2018. J. Jpn. Rad. 2019, 37, 34–72. [Google Scholar] [CrossRef]
- Feng, J.-Z.; Wang, Y.; Peng, J.; Sun, M.-W.; Zeng, J.; Jiang, H. Comparison between logistic regression and machine learning algorithms on survival prediction of traumatic brain injuries. J. Crit. Care 2019, 54, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Senders, J.T.; Staples, P.C.; Karhade, A.V.; Zaki, M.M.; Gormley, W.B.; Broekman, M.L.D.; Smith, T.R.; Arnaout, O. Machine Learning and neurosurgical outcome prediction: A systematic review. World Neurosurg. 2018, 109, 476–486.e1. [Google Scholar] [CrossRef]
- Celtikci, E. A systematic review on machine learning in neurosurgery: The future of decision-making in patient care. Turk. Neurosurg. Soc. 2018, 28, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, N.T.; Salinas, J. Machine learning for predicting outcomes in trauma. Turk. Neurosurg. Soc. 2017, 48, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Saeidi, M.; Karwowski, W.; Farahani, F.V.; Fiok, K.; Taiar, R.; Hancock, P.A.; Al-Juaid, A. Neural Decoding of EEG Signals with Machine Learning: A Systematic Review. Brain Sci. 2021, 11, 1525. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Bian, G.-B.; Tian, Z. Removal of Artifacts from EEG Signals: A Review. Brain Sci. 2019, 19, 987. [Google Scholar] [CrossRef] [Green Version]
- Radüntz, T.; Scouten, J.; Hochmuth, O.; Meffert, B. EEG artifact elimination by extraction of ICA-component features using image processing algorithms. J. Neurosci. Methods 2015, 243, 84–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoshnevis, S.A.; Sankar, R. Classification of the stages of Parkinson’s disease using novel higher-order statistical features of EEG signals. Neural Comput. Appl. 2021, 33, 7615–7627. [Google Scholar] [CrossRef]
- Barros, A.K.; Vigário, R.; Jousmaki, V.; Ohnishi, N. Extraction of event-related signals from multichannel bioelectrical measurements. IEEE Trans. Biomed. Eng. 2000, 47, 583–588. [Google Scholar] [CrossRef]
- Lee, S.; Zhao, X.; Davis, K.A.; Topjian, A.A.; Litt, B.; Abend, N.S. Quantitative EEG predicts outcomes in children after cardiac arrest. Neurology 2019, 92, e2329–e2338. [Google Scholar] [CrossRef]
- Vigário, R.N. Extraction of ocular artefacts from EEG using independent component analysis. Electroencephalogr. Clin. Neurophysiol. 1997, 103, 395–404. [Google Scholar] [CrossRef]
- Vigário, R.; Sarela, J.; Jousmiki, V.; Hamalainen, M.; Oja, E. Independent component approach to the analysis of EEG and MEG recordings. IEEE Trans. Biomed. Eng. 2000, 47, 589–593. [Google Scholar] [CrossRef] [Green Version]
- Romero, S.; Mananas, M.; Clos, S.; Gimenez, S.; Barbanoj, M. Reduction of EEG artifacts by ICA in different sleep stages. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, IEEE Cat. No. 03CH37439, Cancun, Mexico, 17–21 September 2003; pp. 675–2678. [Google Scholar]
- Noor, N.S.E.M.; Ibrahim, H.; Lah, M.H.C.; Abdullah, J.M. Improving Outcome Prediction for Traumatic Brain Injury From Imbalanced Datasets Using RUSBoosted Trees on Electroencephalography Spectral Power. IEEE Access 2021, 9, 121608–121631. [Google Scholar] [CrossRef]
- Jennett, B.; Snoek, J.; Bond, M.R.; Brooks, N. Disability after severe head injury: Observations on the use of the glasgow outcome scale. J. Neurol. Neurosurg. Psychiatry 1981, 44, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Jennett, B.; Snoek, J.; Bond, M.R.; Brooks, N. Assessment of outcome after severe brain damage: A practical scale. J. Neurol. Neurosurg. 1975, 305, 480–484. [Google Scholar] [CrossRef]
- Lai, C.Q.; Ibrahim, H.; Abdullah, M.Z.; Abdullah, J.M.; Suandi, S.A.; Azman, A. Arrangements of Resting State Electroencephalography as the Input to Convolutional Neural Network for Biometric Identification. Comput. Intell. Neurosci. 2019, 2019, 7895924. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Mullen, T.; Kothe, C.; Acar, Z.A.; Bigdely-shamlo, N.; Vankov, A.; Makeig, S. EEGLAB, SIFT, NFT, BCILAB, and ERICA: New Tools for Advanced EEG Processing. Comput. Intell. Neurosci. 2011, 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Winkler, I.; Haufe, S.; Tangermann, M. Automatic Classification of Artifactual ICA-Components for Artifact Removal in EEG Signals. Behav. Brain Funct. 2011, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Winkler, I.; Brandl, S.; Horn, F.; Waldburger, E.; Allefeld, C.; Tangermann, M. Robust artifactual independent component classification for BCI practitioners. J. Neural Eng. 2014, 11, 035013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haresign, I.M.; Phillips, E.; Whitehorn, M.; Noreika, V.; Jones, E.J.H.; Leong, V.; Wass, S.V. Automatic classification of ICA components from infant EEG using MARA. Dev. Cogn. Neurosci. 2021, 52, 1–43. [Google Scholar]
- Alam, R.-U.; Zhao, H.; Goodwin, A.; Kavehei, O.; McEwan, A. Differences in Power Spectral Densities and Phase Quantities Due to Processing of EEG Signals. Sensors 2020, 20, 6285. [Google Scholar] [CrossRef]
- Seiffert, C.; Khoshgoftaar, T.M.; Hulse, J.V.; Napolitano, A. RUSBoost: A hybrid approach to alleviating class imbalance. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 2010, 40, 185–197. [Google Scholar] [CrossRef]
- Seiffert, C.; Khoshgoftaar, T.M.; Hulse, J.V.; Napolitano, A. RUSBoost: Improving classification performance when training data is skewed. In Proceedings of the 19th International Conference on Pattern Recognition, Tampa, FL, USA, 8–11 December 2008; pp. 185–197. [Google Scholar]
- Ahlawat, K.; Chug, A.; Singh, A.P. Benchmarking framework for class imbalance problem using novel sampling approach for big data. Int. J. Syst. Assur. Eng. Manag. 2019, 10, 824–835. [Google Scholar] [CrossRef]
- Powers, D.M. Evaluation: From precision, recall and F-measure to ROC, informedness, markedness and correlation. J. Mach. Learn. Technol. 2011, 2, 63. [Google Scholar]
- Chen, W.; Liu, G.; Su, Y.; Zhang, Y.; Lin, Y.; Jiang, M.; Huang, H.; Ren, G.; Yan, J. EEG signal varies with different outcomes in comatose patients: A quantitative method of electroencephalography reactivity. J. Neurosci. Methods 2020, 342, 108812. [Google Scholar] [CrossRef] [PubMed]
- Tanha, J.; Abdi, Y.; Samadi, N.; Razzaghi, N.; Asadpour, M. Boosting methods for multi-class imbalanced data classification: An experimental review. J. Big Data 2020, 7, 1–47. [Google Scholar] [CrossRef]
- Ali, A.; Shamsuddin, S.M.; Ralescu, A.L. Classification with class imbalance problem: A review. Int. J. Soft Comput. Appl. 2015, 7, 1–30. [Google Scholar]
- Freund, Y.; Schapire, R.E. Experiments with a new boosting algorithm. In Proceedings of the International Conference of Machine Learning, Bari, Italy, 22 January 1996; pp. 148–156. [Google Scholar]
- Galar, M.; Fernandez, A.; Barrenechea, E.; Bustince, H.; Herrera, F. A review on ensembles for the class imbalance problem: Bagging-, boosting-, and hybrid-based approaches. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2011, 42, 463–484. [Google Scholar] [CrossRef]
- Kinoshita, T.; Fujiwara, K.; Kano, M.; Ogawa, K.; Sumi, Y.; Matsuo, M.; Kadotani, H. Sleep Spindle detection using RUSBoost and synchrosqueezed wavelet transform. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Bhuiyan, M.I.H.; Hassan, A.R. Sleep stage classification using single-channel EOG. Comput. Biol. Med. 2018, 102, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Bhuiyan, M.I.H.; Hassan, A.R. Automated identification of sleep states from EEG signals by means of ensemble empirical mode decomposition and random under sampling boosting. Comput. Methods Programs Biomed. 2017, 140, 201–210. [Google Scholar]
- Tahir, M.A.U.H.; Asghar, S.; Manzoor, A.; Noor, M.A. A classification model for class imbalance dataset using genetic programming. IEEE Access 2019, 7, 71013–71037. [Google Scholar] [CrossRef]
- Tahir, M.A.U.H.; Asghar, S.; Manzoor, A.; Noor, M.A. ADJUST: An automatic EEG artifact detector based on the joint use of spatial and temporal features. Psychophysiology 2011, 48, 229–240. [Google Scholar]
- Li, Y.; Wang, P.T.; Vaidya, M.P.; Liu, Y.C.; Slutzky, M.W.; Do, A.H. A novel algorithm for removing artifacts from EEG data. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 229–240. [Google Scholar]
- Urigüen, J.A.; Garcia-Zapirain, B. EEG artifact removal—State-of-the-art and guidelines. J. Neural Eng. 2015, 12, 031001. [Google Scholar] [CrossRef]
- Zhang, C.; Tong, L.; Zeng, Y.; Jiang, J.; Bu, H.; Yan, B.; Li, J. Automatic Artifact Removal from Electroencephalogram Data Based on A Priori Artifact Information. BioMed Res. Int. 2015, 2015, 720450. [Google Scholar] [CrossRef] [Green Version]
- Bilal, M.; Rizwan, M.; Saleem, S.; Khan, M.M.; Alkatheir, M.S.; Alqarni, M. Automatic seizure detection using multi-resolution dynamic mode decomposition. IEEE Access 2019, 7, 61180–61194. [Google Scholar] [CrossRef]
- Pedroni, A.; Bahreini, A.; Langer, N. Automagic: Standardized preprocessing of big EEG data. NeuroImage 2019, 200, 460–473. [Google Scholar] [CrossRef] [Green Version]
- Trigui, O.; Daoud, S.; Ghorbel, M.; Dammak, M.; Mhiri, C.; Hamida, A.B. Removal of eye blink artifacts from EEG signal using morphological modeling and orthogonal projection. Signal Image Video Processing 2021, 14, 1–9. [Google Scholar] [CrossRef]
- Song, S.; Nordin, A.D. Mobile Electroencephalography for Studying Neural Control of Human Locomotion. Front. Hum. Neurosci. 2021, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chennu, S.; Annen, J.; Wannez, S.; Thibaut, A.; Chatelle, C.; Cassol, H.; Martens, G.; Schnakers, C.; Gosseries, O.; Menon, D. Brain networks predict metabolism, diagnosis and prognosis at the bedside in disorders of consciousness. Brain 2017, 140, 2120–2132. [Google Scholar] [CrossRef] [PubMed]
- Tolonen, A.; Särkelä, M.O.K.; Takala, R.S.K.; Katila, A.; Frantzén, J.; Posti, J.P.; Müller, M.; van Gils, M.; Tenovuo, O. Quantitative EEG parameters for prediction of outcome in severe traumatic brain injury: Development study. Clin. EEG Neurosci. 2018, 49, 248–257. [Google Scholar] [CrossRef]
- Chennu, S.; Finoia, P.; Kamau, E.; Allanson, J.; Williams, G.B.; Monti, M.M.; Noreika, V.; Arnatkeviciute, A.; Canales-Johnson, A.; Olivares, F.; et al. Spectral Signatures of Reorganised Brain Networks in Disorders of Consciousness. PLoS Comput. Biol. 2014, 10, e1003887. [Google Scholar] [CrossRef] [PubMed]
- Sharova, E.V.; Chelyapina, M.V.; Korobkova, E.V.; Kulikov, M.A.; Zaitsev, O.S. EEG-correlates of consciousness recovery after traumatic brain injury. Zh. Vopr. Neirokhir. Im. N. N. Burdenko 2014, 78, 14–25. [Google Scholar]
- Edlow, B.L.; Chatelle, C.; Spencer, C.A.; Chu, C.J.; Bodien, Y.G.; O’Connor, K.L.; Hirschberg, R.E.; Hochberg, L.R.; Giacino, J.T.; Rosenthal, E.S. Early detection of consciousness in patients with acute severe traumatic brain injury. Brain 2017, 140, 2399–2414. [Google Scholar] [CrossRef]
- Schorr, B.; Schlee, W.; Arndt, M.; Bender, A. Coherence in resting-state EEG as a predictor for the recovery from unresponsive wakefulness syndrome. J. Neurol. 2017, 263, 937–953. [Google Scholar] [CrossRef] [PubMed]
- Hebb, M.O.; McArthur, D.L.; Alger, J.; Etchepare, M.; Glenn, T.C.; Bergsneider, M.; Martin, N.; Vespa, P.M. Impaired percent alpha variability on continuous electroencephalography is associated with thalamic injury and predicts poor long-term outcome after human traumatic brain injury. J. Neurotrauma 2007, 24, 579–590. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GOS Score | Clinical Meaning | Outcome |
|---|---|---|
| 1 | Death | Poor |
| 2 | Persistent vegetative state | Poor |
| 3 | Severe disability | Poor |
| 4 | Moderate disability | Poor |
| 5 | Mild or no disability | Good |
| EEG Dataset ID | Gender (F/M) | Age | Date of Accident | CT Brain Characteristic on Emergency Admission | GCS | GOS from 4-Weeks to 12-Months | |
|---|---|---|---|---|---|---|---|
| GOS 1–4 | GOS 5 | ||||||
| B1 | Male | 53 | 27 January 2017 | No parenchyma, | 9 | ✓ | |
| Subarachnoid hemorrhage over L-F, P cortex, | ✓ | ||||||
| B2 | Male | 18 | 18 October 2017 | Two-way subdural hematoma, No parenchyma | 11 | ✓ | |
| B3 | Male | 19 | 14 February 2018 | L-extradural hematoma, two-way T-bruise | 10 | ✓ | |
| B4 | Male | 22 | 13 April 2018 | L-T extradural hematoma | 10 | ✓ | |
| B5 | Male | 53 | 15 May 2018 | L-P bruise, severe subarachnoid hemorrhage | 9 | ✓ | |
| B6 | Male | 19 | 06 August 2018 | R-F small extradural hematoma | 11 | ✓ | |
| B7 | Male | 45 | 12 September 2018 | Top extradural hematoma | 10 | ✓ | |
| B8 | Male | 62 | 30 September 2018 | F-bruise hemorrhage | 9 | ✓ | |
| B9 | Male | 54 | 30 October 2018 | L-T bruise | 11 | ✓ | |
| B10 | Male | 22 | 28 October 2018 | R-F bruise | 11 | ✓ | |
| B11 | Male | 39 | 30 April 2019 | L-P bruise, L-FTP severe subdural hematoma | 11 | ✓ | |
| B12 | Male | 18 | 22 November 2017 | L-F bruise, mild R-T bruise | 11 | ✓ | |
| B13 | Male | 19 | 22 February 2017 | L-extradural hematoma | 11 | ✓ | |
| B14 | Male | 53 | 27 February 2017 | No parenchyma, | 9 | ✓ | |
| Subarachnoid hemorrhage over L-F, P cortex, | |||||||
| B15 | Male | 18 | 18 October 2017 | Two-way subdural hematoma, No parenchyma | 11 | ✓ | |
| B16 | Male | 19 | 14 February 2018 | L-extradural hematoma, two-way T-bruise | 10 | ✓ | |
| B17 | Male | 22 | 13 April 2018 | L-T extradural hematoma | 10 | ✓ | |
| B18 | Male | 53 | 15 May 2018 | L-P bruise, severe subarachnoid hemorrhage | 9 | ✓ | |
| B19 | Male | 19 | 06 August 2018 | R-F thin extradural hematoma | 11 | ✓ | |
| B20 | Male | 22 | 28 October 2018 | R-F small extradural hematoma | 11 | ✓ | |
| B21 | Male | 62 | 30 September 2018 | F-bruise hemorrhage | 9 | ✓ | |
| B22 | Male | 54 | 30 October 2018 | L-T bruise | 11 | ✓ | |
| B23 | Male | 22 | 28 October 2018 | R-F bruise | 11 | ✓ | |
| B24 | Male | 39 | 30 April 2019 | L-P bruise, L-FTP severe subdural hematoma, | 11 | ✓ | |
| B25 | Male | 19 | 14 February 2018 | L-extradural hematoma, bilateral T-contusions | 10 | ✓ | |
| B26 | Male | 53 | 15 May 2018 | L-P contusion, severe subdural hematoma | 9 | ✓ | |
| B27 | Male | 19 | 06 August 2018 | R-F small extradural hematoma | 11 | ✓ | |
| Ground Truth | Prediction | |
|---|---|---|
| Positive | Negative | |
| (Poor Outcome) | (Good Outcome) | |
| Positive (Poor Outcome) | TP | FN |
| Negative (Good Outcome) | FP | TN |
| Absolute PSD | TP | FN | TN | FP | AUC | G-Mean (%) | F1 Score | ||
|---|---|---|---|---|---|---|---|---|---|
| 4 | 1 | 14 | 8 | 80.0 | 63.6 | 0.75 | 71.33 | 0.5 | |
| 4 | 1 | 14 | 8 | 80.0 | 63.6 | 0.71 | 71.33 | 0.5 | |
| 4 | 1 | 13 | 9 | 80.0 | 59.1 | 0.73 | 68.76 | 0.4 | |
| 2 | 3 | 12 | 10 | 40.0 | 54.5 | 0.51 | 46.69 | 0.2 | |
| 4 | 1 | 12 | 10 | 80.0 | 54.5 | 0.54 | 66.33 | 0.4 |
| Freq.Bands | (%) | (%) | G-Mean (%) | F1 Score | AUC |
|---|---|---|---|---|---|
| 20.0 | 77.3 | 39.3 | 0.1 | 0.49 | |
| 20.0 | 81.8 | 40.45 | 0.1 | 0.53 | |
| 0.0 | 68.2 | 0.0 | 0.0 | 0.30 | |
| 20.0 | 81.8 | 40.45 | 0.1 | 0.70 | |
| 20.0 | 72.7 | 38.13 | 0.1 | 0.55 |
| Freq.Bands | (%) | (%) | G-Mean (%) | F1 Score | AUC |
|---|---|---|---|---|---|
| 20.0 | 63.6 | 35.7 | 0.1 | 0.38 | |
| 20.0 | 59.1 | 34.4 | 0.1 | 0.41 | |
| 0.0 | 86.36 | 0.0 | 0.0 | 0.42 | |
| 0.0 | 77.3 | 0.0 | 0.0 | 0.30 | |
| 20.0 | 68.2 | 36.9 | 0.1 | 0.57 |
| Freq.Bands | (%) | (%) | G-Mean (%) | F1 Score | AUC |
|---|---|---|---|---|---|
| 40.0 | 77.3 | 55.6 | 0.2 | 0.59 | |
| 40.0 | 72.7 | 53.9 | 0.2 | 0.56 | |
| 40.0 | 77.3 | 55.6 | 0.2 | 0.59 | |
| 40.0 | 81.8 | 57.2 | 0.2 | 0.61 | |
| 40.0 | 86.4 | 58.7 | 0.2 | 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohd Noor, N.S.E.; Ibrahim, H.; Che Lah, M.H.; Abdullah, J.M. Prediction of Recovery from Traumatic Brain Injury with EEG Power Spectrum in Combination of Independent Component Analysis and RUSBoost Model. BioMedInformatics 2022, 2, 106-123. https://doi.org/10.3390/biomedinformatics2010007
Mohd Noor NSE, Ibrahim H, Che Lah MH, Abdullah JM. Prediction of Recovery from Traumatic Brain Injury with EEG Power Spectrum in Combination of Independent Component Analysis and RUSBoost Model. BioMedInformatics. 2022; 2(1):106-123. https://doi.org/10.3390/biomedinformatics2010007
Chicago/Turabian StyleMohd Noor, Nor Safira Elaina, Haidi Ibrahim, Muhammad Hanif Che Lah, and Jafri Malin Abdullah. 2022. "Prediction of Recovery from Traumatic Brain Injury with EEG Power Spectrum in Combination of Independent Component Analysis and RUSBoost Model" BioMedInformatics 2, no. 1: 106-123. https://doi.org/10.3390/biomedinformatics2010007
APA StyleMohd Noor, N. S. E., Ibrahim, H., Che Lah, M. H., & Abdullah, J. M. (2022). Prediction of Recovery from Traumatic Brain Injury with EEG Power Spectrum in Combination of Independent Component Analysis and RUSBoost Model. BioMedInformatics, 2(1), 106-123. https://doi.org/10.3390/biomedinformatics2010007