
Identifying the Predictors of Pediatric Vaccine Uptake during the COVID-19 Pandemic

1
Division of Natural Sciences and Engineering, University of South Carolina Upstate, Spartanburg, SC 29303, USA
2
Department of Psychology, University of South Carolina Upstate, Spartanburg, SC 29303, USA
*
Author to whom correspondence should be addressed.
COVID 2024, 4(4), 495-505; https://doi.org/10.3390/covid4040033
Submission received: 5 March 2024
/
Revised: 12 April 2024
/
Accepted: 14 April 2024
/
Published: 16 April 2024
Abstract
:Identifying determinants of vaccination uptake is critical for public and community health. The population became divided in regard to preventative measures and vaccinations during the COVID-19 pandemic. In addition, there are varying opinions on decisions to vaccinate children against childhood diseases and COVID-19. Recent findings suggest that the COVID-19 pandemic has exacerbated existing vaccine hesitancy. Here, we assess vaccine hesitancy in parents by identifying predictors of vaccine acceptance by parents during the COVID-19 pandemic using a survey given to parents in South Carolina. Knowledge about COVID-19 and vaccinations affects vaccination intentions. Age, education, gender, and politics were also found to predict parents’ decisions about vaccinating their kids. Understanding potential barriers to vaccine acceptance will aid healthcare providers and public health entities to better reach the community.
1. Introduction
On 11 March 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) a pandemic [1]. By 30 November 2022, the respiratory disease had caused over 1 million deaths in the United States, and in total, the country had seen 98 million cases [2]. During the early onset of the disease, preventative measures such as mask-wearing and social distancing were implemented, but not without opposition. A previous study found that age and gender contributed to the practice of COVID-19 preventative behaviors, with females and older individuals more likely to wear masks. Urban residents were also found to be more likely to practice preventative measures compared with rural residents [3].
On 11 December 2020, the U.S. Food and Drug Administration (FDA) authorized the emergency use of the Pfizer-BioNTech COVID-19 vaccine. Pfizer’s vaccine was fully approved on 23 August 2021 for individuals aged 16 and older [4]. On 27 February 2021, Johnson & Johnson’s (J&J) COVID-19 vaccine was approved for emergency use [5]. J&J’s vaccine has not received full approval by the FDA in the United States but received full approval in Canada on 24 November 2021 [6]. The FDA authorized the emergency use of Moderna’s COVID-19 vaccine on 17 December 2021 [7]. Moderna’s COVID-19 vaccine was fully approved on 31 January 2022 for adults aged 18 and older [8]. On 10 May 2021, the emergency use of the Pfizer-BioNTech vaccine was approved for children between the ages of 12–15 [9]. The FDA approved the emergency use of the Pfizer-BioNTech vaccine for children ages 5–11 on 29 October 2021 [10]. At the time of this study, all age groups are eligible for the first and second doses of the COVID-19 vaccines provided by Pfizer-BioNTech. As of 3 December 2022, only 53.7% of all eligible South Carolinians had completed the primary vaccine series [11]. Specifically examining the pediatric data, only 19.3% of children 5–11 and 1.8% of children under age 5 in South Carolina had completed the primary vaccine series [11]. Travis et al.’s study, conducted prior to any COVID-19 vaccine approval, found that trust in science was responsible for nearly half of all the variance explained in the model examining vaccination intentions. Gender, age, education level, and political identification also contributed to vaccine intentions. The same study revealed that COVID-19 knowledge, age, trust in science, political ideology, party identification, and voting behavior were also important factors in the adherence to COVID-19 prevention measures [3]. A 2021 report by Schneider et al. revealed that the main causes of hesitancy among the unvaccinated population in the United States were concerns about the vaccine development process, their peers’ vaccination status, and distrust in the vaccine [12].
The less than adequate COVID-19 vaccination rate is not the only concern. A 2020 survey revealed that childhood measles, mumps, and rubella (MMR) and diphtheria, tetanus, and pertussis (DTaP) vaccination rates have decreased compared with pre-pandemic times [13]. Additionally, vaccine risk perception by parents increased during the pandemic [14]. South Carolina has a lower childhood vaccination rate when compared to other states. The South Carolina Department of Health and Environmental Control (SC DHEC) reported that in 2018, compared with the national average, South Carolina had lower coverage rates for all adolescent vaccines recommended by the Advisory Committee on Immunization Practices except for DTaP. The rates of religious exemptions for vaccines required from school rose from 1.18% in 2017–2018 to 1.99% in 2021–2022 [15]. The SC DHEC reported that during the 2018–2019 flu season, 46.8% of eligible South Carolinians were vaccinated against the flu [15]. A positive correlation has been found between flu vaccination status and COVID-19 vaccination status among pregnant women [16]. It is important to improve parental trust in childhood vaccines and to increase vaccination rates not only for childhood vaccines but also for the COVID-19 vaccine. Parental hesitation toward vaccination can potentially allow for dormant diseases to resurface and allow increased COVID-19 transmission, which can lead to new variants of the virus. The purpose of our study is to identify the contributors to parents’ decisions to vaccinate their children and to identify how the COVID-19 pandemic has affected parents’ attitudes toward vaccinations. This research can help guide public health officials when providing resources and education to improve vaccination rates.
2. Methods
2.1. Participants and Procedures
All of our data collection procedures were approved by the Institutional Review Board (IRB) at the University of South Carolina. Participants (n = 1765) were obtained by Qualtrics and recruited through online methods. We aimed to obtain a sample representative of South Carolina adults. The only criteria to participate were being a South Carolina resident and at least 18 years of age. All participants provided informed consent electronically by clicking “I agree.” Of the total participants responding to the survey, 204 expectant parents reported childhood vaccine intentions, and 517 parents of children 17 and under reported childhood COVID-19 vaccine intentions. Parents’ and expectant parents’ survey responses were used in this study. Participants were recruited using traditional, double-opt-in research panels.
Data collection began in October 2021 and ended in December 2021. Qualtrics compensated participants for their contributions. Participants averaged 45 years old within the entire data set and 35.9 years old for parents and expectant parents, with 71.5% reporting as female and 95.3% reporting a high school education or higher. The counties most represented were Greenville, Spartanburg, Charleston, Horry, and Richland, which are the largest counties in South Carolina.
2.2. Measures
COVID-19 Knowledge Test. We assessed COVID-19 knowledge through an embedded 11-question quiz on the transmission, infection, and treatment of the disease. The quiz was administered in a multi-choice format. The correct option had a numerical value of 1 and the incorrect options had a numerical value of 0. Scores ranged from 0 to 11.
COVID-19-Vaccine Knowledge Test. We measured COVID-19-vaccine knowledge with an 11-question quiz pertaining to the mechanism and protection provided by the COVID-19 vaccine. The quiz was administered in a true or false format, with correct responses receiving a value of 1 and incorrect responses a value of 0. Scores ranged from 2 to 11.
General Vaccine Knowledge Test. We assessed general vaccine knowledge through an embedded 4-question quiz pertaining to the mechanism and protection provided in general by vaccines. The quiz was administered in a true or false format. The correct option had a numerical value of 1 and the incorrect options had a numerical value of 0. Scores ranged from 1 to 4.
Vaccine Intentions. We asked parental participants about their intentions to vaccinate their children against COVID-19 and expectant parents’ intentions for their children to receive general childhood vaccines. Three responses were available: yes, no, and not sure.
Political Affiliation. Participants were asked to choose a political identity they most aligned with. The options were: Democrat, Republican or independent.
Race. Participants were asked to indicate which racial group they identified as. The options were White, African American, Asian/Pacific Islander, Hispanic/Latino, or American Indian/Alaskan Native. Other than reporting descriptive statistics, all non-white categories were collapsed into a single category for regression analyses.
Gender. Participants were asked, “What is your gender”, with response options of “male”, “female”, “Other (please specify)”, and “prefer not to say”. Since fewer than 1% of responses were neither “male” or “female,” all analyses were conducted using these two groups.
Financial Status. We assess participants’ financial status by asking them to choose which range most accurately reflected their annual income. The options were <USD 25,000, USD 25,000–USD 49,999, USD 50,000–USD 75,999, USD 75,000–USD 99,000, >USD 100,000.
Education. We assessed education by asking participants to indicate their highest attained degree. Available education options were high school diploma, associate’s degree, bachelor’s degree, or postgraduate degree. Participants in-between degrees had options such as <high school or some college.
3. Results
3.1. Descriptive Results
A total of 58% of expectant parents planned to give their child the recommended childhood vaccines but only 33% of expectant parents were planning to vaccinate their child against COVID-19. A total of 65.5% of parents reported that COVID-19 had not affected their decisions or opinions about childhood vaccines. Approximately 83% of respondents reported that COVID-19 did not interrupt their child’s regular childhood vaccination schedule. The data showed that 66.7% of parents expecting their first child planned to vaccinate their child with routine childhood vaccines, while 81.8% of expectant parents who already had 4 or more children planned to vaccinate their child with routine childhood vaccines.
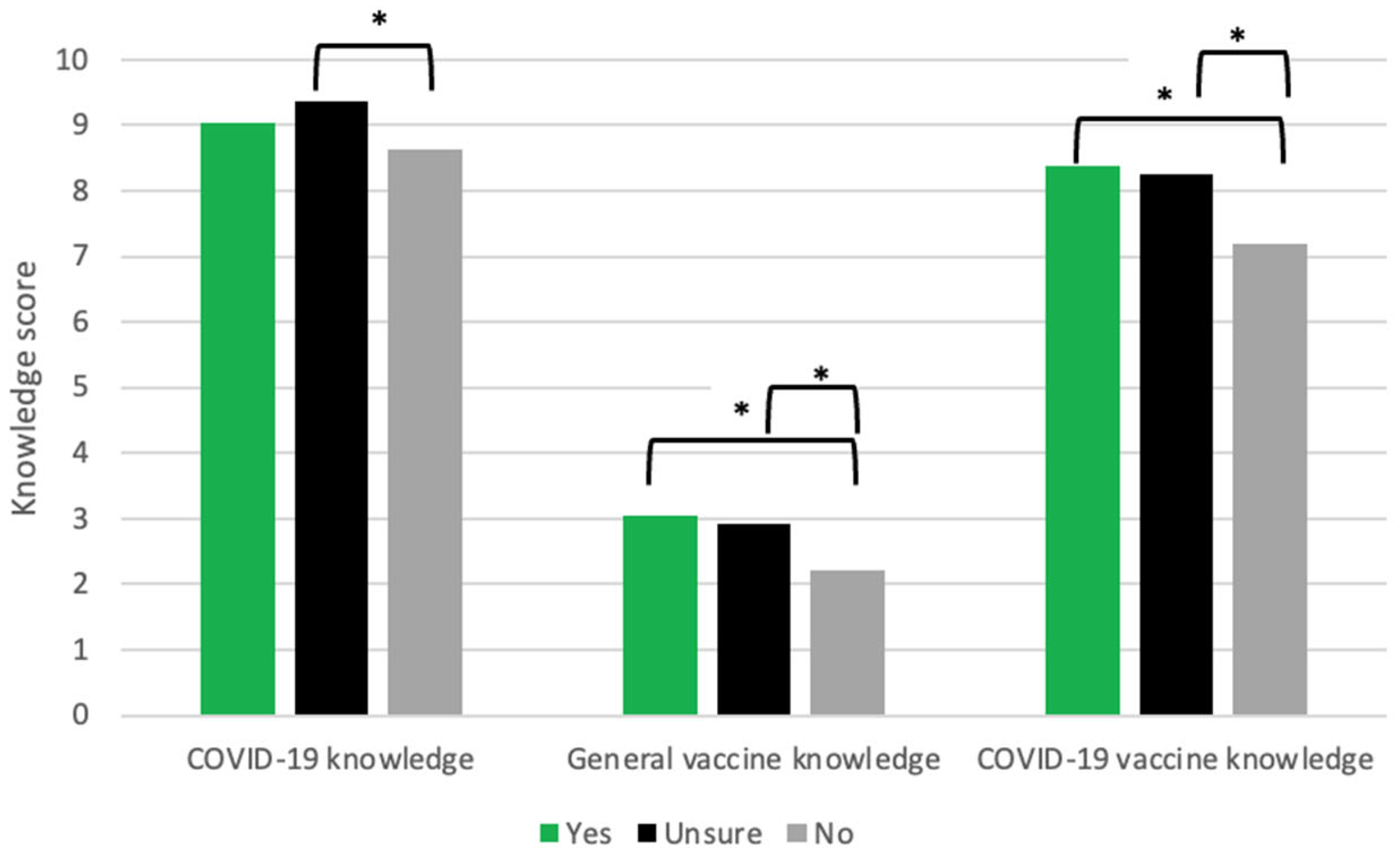
3.2. COVID-19-Vaccine, General Vaccine, and COVID-19 Knowledge for Parents of Children 17 and Under
COVID-19-vaccine knowledge, COVID-19 knowledge, and general vaccine knowledge varied among all parental groups: those who planned to vaccinate their children, those who did not, and those who were unsure. We interpreted the unsure category as an indication of uncertain vaccination plans. We assumed that parents choosing the unsure option had not yet determined their vaccination intentions. Results from an analysis of variance (ANOVA) indicated there are significant differences in each of the three knowledge scores (COVID-19 knowledge, general vaccine knowledge, and COVID-19-vaccine knowledge respectively) across groups; however, post hoc analyses using Games–Howell correction revealed where the group means were significantly different (Figure 1). For COVID-19 knowledge, only parents not planning to vaccinate their children (M = 8.62) and parents that were unsure (M = 9.36) were significantly different (p < 0.01). For general vaccine knowledge, parents not planning to vaccinate their children (M = 2.22) scored significantly lower than parents that did plan to vaccinate (M = 3.06, p < 0.01) and parents that were unsure (M = 2.93, p < 0.01). Lastly, for COVID-19-vaccine knowledge, parents not planning to vaccinate their children (M = 7.19) scored significantly lower than parents that did plan to vaccinate (M = 8.39, p < 0.01) and parents that were unsure (M = 8.24, p < 0.01).
3.3. Education vs. COVID-19 Vaccination
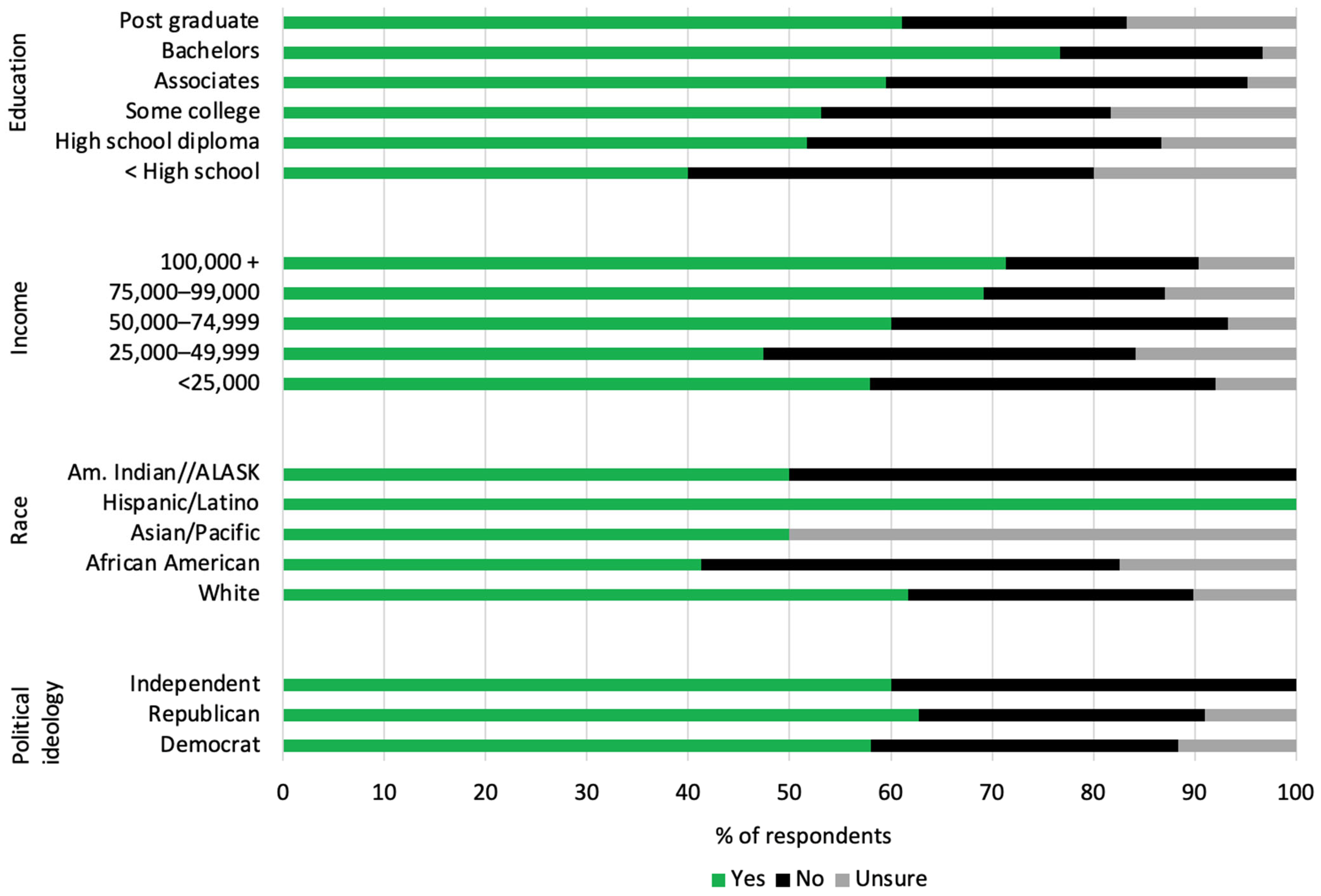
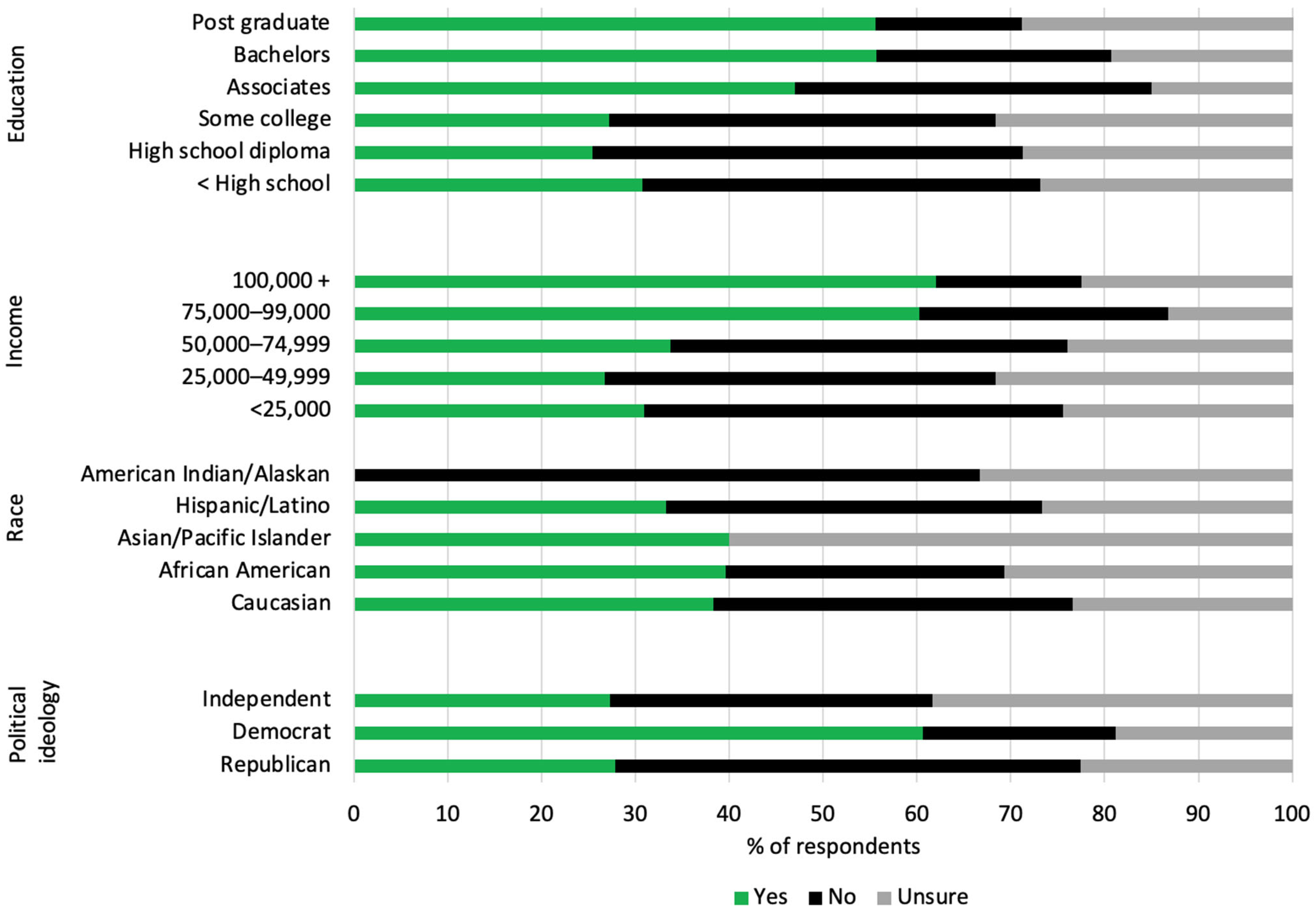
Higher educational attainment was positively associated with intentions to vaccinate one’s child against COVID-19. The majority of expectant parents with at least a bachelor’s degree planned on their children receiving the recommended childhood vaccines (Figure 2). Around 40% of parents of children 17 and under with an associate degree had plans to vaccinate their children against COVID-19 (Figure 3). Parents with a bachelor’s degree were less hesitant about COVID-19 vaccination, with 51.5% indicating that they would vaccinate their children against COVID-19 (Figure 3). Similar results were seen in expectant parents’ intentions for typical childhood vaccinations (Figure 2).
3.4. Political Affiliation vs. COVID-19 Vaccination
The role of political affiliation on vaccine intentions was different between expectant parents’ plans to vaccinate with routine childhood vaccinations and parents’ plans to vaccinate against COVID-19. The majority of expectant parents planned for their children to receive the recommended childhood vaccines, regardless of their political affiliation (Figure 2). However, Figure 3 shows that Republican or Independent parents of children 17 and under were less likely to vaccinate their children against COVID-19, with intentions of 27.9% and 27.3%, respectively, compared with Democrat parents, who were more likely to report intentions to vaccinate their children against COVID-19, with 60.6% reporting intentions to vaccinate (Figure 3).
3.5. Race vs. COVID-19 Vaccination
American Indians and Alaskan Natives were split evenly in their intentions to vaccinate with the typical childhood vaccines. On the other hand, 50% of Asian parents reported being unsure about childhood vaccinations, while the other half of Asian parents were supportive of childhood vaccinations. Around 60% of white parents had intentions to vaccinate their children with the typical vaccines. Equal proportions of African American parents indicated plans to vaccinate their children or had no plans for childhood vaccination. All Latino parents expressed positive intentions for their children to receive the regular childhood vaccines (Figure 2).
American Indians/Alaskan Natives were the only parental racial group that had a majority indicating no plans to vaccine their children against COVID-19. Latinos and African Americans had equal proportions of parents indicating plans to or no plans to vaccinate their children against COVID-19. About 60% of Asian parents were unsure about their plans to vaccinate their children against COVID-19, while 40% of Asians parents had plans to vaccinate their children against COVID-19. Approximately 39% of white parents reported no plans to vaccinate their children against COVID-19, and 37% of white parents reported positive plans (Figure 3).
3.6. Predictors of Routine Childhood Vaccination Acceptance by Expectant Parents
A regression analysis revealed several predictors of routine childhood vaccination acceptance by expectant parents. Factors found to be statistically significant were age, gender, and COVID-19 knowledge (Table 1). Parents who are younger, male, or had higher COVID-19 knowledge scores were more likely to accept routine childhood vaccinations for their child(ren) when comparing parents who said yes to no to vaccine acceptance. Beta coefficients and odds ratios indicated that the relationships between gender and COVID-19 knowledge were much larger than the relationship between age and childhood vaccination acceptance. There were no significant predictors found when comparing parents who said yes to parents who reported as being unsure.
3.7. Predictors of COVID-19 Vaccine Acceptance for Parents of Children 17 and Under
Our survey evaluated how knowledge, education, political affiliation, and race affected vaccination intentions. Regression analysis of our data showed that political affiliation, gender, age, education, and general and COVID-19 vaccine knowledge were statistically significant predictors of vaccine acceptance compared with vaccine refusal (Table 2). Compared with those indicating “yes” to vaccinating their children for COVID-19, those reporting “no” were more likely to have a lower education level, less COVID-19 and general vaccine knowledge, be female, and identify as Republican. Compared with those indicating “yes”, those reporting “unsure” were more likely to have less education, be female, identify as a Republican, and have more COVID-19 knowledge.
4. Discussion
Our results showed a notable decrease in childhood vaccination intentions, with 58% of expectant parents reporting intentions to vaccinate their children with routine childhood vaccinations. SCDHEC reports that over 90.3 percent of kindergarten children were up to date with their vaccinations for the 2020–2021 school year [15]. During the 2018–2019 flu season, 46.8 percent of eligible South Carolinians aged 6 months and older were vaccinated against the flu, and 59.7 percent of children aged 6 months–17 years were vaccinated against the flu [15]. The discrepancy seen in our survey could be due to hesitancy caused by increased accessibility to false information. A study by Rocha et al. found that an overload of misinformation can interfere with behavior surrounding health and generate distrust in health professionals [17]. He et al. found that childhood vaccine hesitancy increased during the COVID-19 pandemic due to increased risk perception [14]. However, these changes did not significantly affect plans for routine childhood vaccinations or flu vaccinations. Their literature review showed that 34 to 47% of flu-vaccine-hesitant parents still vaccinated their kids. A 2021 survey by Teasdale et al. revealed that 49.4% of parents of children ≤12 years of age reported plans to vaccinate their children against COVID-19. Safety concerns and lower risk perception were the primary factors for the vaccine hesitancy [18]. In addition, the discrepancy between the vaccine intentions reported in our survey to actual vaccine rates may simply be due to expectant parents being unsure of their upcoming decisions and their lack of experience with pediatrician recommendations. This is supported by our data showing that first-time parents report lower rates of vaccine acceptance. It is especially important to examine the factors leading parents to report that they are “unsure” about their child(ren) receiving vaccines as this is a group of individuals who have not made their decision, and they may benefit from additional information and discussion.
Our survey found that higher education levels of parents correlate with increased intentions to vaccinate children against COVID-19. Similar results were seen regarding attitudes toward general childhood vaccinations. This result is comparable to Khairat et al.’s study showing that lower education contributes to higher COVID-19 vaccine hesitancy [19]. Female respondents were less likely to accept COVID-19 and routine vaccinations for their child(ren) compared with male-parent respondents. Interestingly, 71% of respondents to the survey were female. Studies show that females are generally more likely to respond to online surveys [20]. In addition, research shows that females are more likely to be health-care decision makers for their household, with an estimation that females make 80% of health-care decisions for their families [21]. Studies have examined how mothers’ see themselves as experts of their children and have dedication to making health-care decisions for their child(ren) [22]. In addition, females have been shown to express more vaccine hesitancy, potentially due to being less likely to take risks. The novelty of the COVID-19 vaccines may be interpreted as a higher risk [3,23,24].
Political affiliation did not appear to be a major contributor to routine childhood vaccination intentions. However, COVID-19 vaccination attitudes varied based on political ideologies. Democrats had higher intentions to vaccinate their children against COVID-19, compared with Republicans, who were less likely to have intentions to vaccinate their children against COVID-19. This result emulates a model proposed by BMC Public Health. The model showed that Republican counties were more likely to have lower COVID-19 vaccination rates [25].
Our survey showed mixed results regarding race and vaccination. White parents were the only racial group with a clear majority supporting general childhood vaccines. All Latino parents involved in the survey reported positive attitudes toward childhood vaccination. However, this result is skewed, as only four Latino parents were participants in our survey. The results pertaining to general childhood vaccination correlate with previous studies of low vaccination among people of color due to medical distrust. Bagasra et al. found that racial groups who have been subjected to “higher perceived discrimination” were more likely to have higher medical distrust resulting in the under-utilization of healthcare services, a low adherence to medical advice, and reduced compliance with recommended health behaviors [26]. The unclear results regarding childhood COVID-19 vaccination may be due to the racial disparities in COVID-19 infection and deaths. American Indian, Alaskan Native, Latino, and African American people are at greater risk for COVID-19 infection, hospitalization, and death [27].
Our data suggest that parents reported more hesitation toward the COVID-19 vaccine compared with general childhood vaccines. Some demographic factors that affected COVID-19 vaccine acceptance had no effect on routine childhood vaccinations. Education level, political affiliation, COVID-19-vaccine knowledge, and general vaccine knowledge all had an effect on COVID-19 vaccine decisions by parents but not on parents’ decisions about routine childhood vaccinations. This is most likely a result of the rapid production of the COVID-19 vaccine and the significant politicization and polarization surrounding the COVID-19 pandemic [28]. This may have led to more hesitancy toward the COVID-19 vaccine compared with routine childhood vaccinations. Respondents reported that the pandemic did not act as a major deterrent or disturbance to normal childhood vaccination schedules, with 69.8% of parents reporting that COVID-19 did not affect childhood vaccine opinions. However, the results of our survey show there was a decrease in childhood vaccination intentions compared with the pre-pandemic years. This discrepancy could be due to a response bias [29]. Response bias refers to extraneous factors that could influence a survey response. The parents may have had subconscious cognitive biases toward their actions during the pandemic. Parents believed that the pandemic did not affect their vaccine decision-making despite their contradictory behavior; in this case, not vaccinating their children during the pandemic. Parents held onto their denial of vaccination disruption because of COVID-19, thus resulting in contradictory survey responses. The decline in plans for childhood vaccination seen in our study aligns with vaccination rate changes seen by the CDC. An April 2022 study revealed a one percent drop among kindergarteners in the United States [30].
The significant difference in knowledge scores within the three groups (COVID-19, COVID-19 vaccine, and general vaccine) shows that there is still an outreach gap in spreading accurate information about these topics. There has been a constant flood of information the past few years surrounding COVID-19 and COVID-19 vaccines. However, there is a need for greater advocation of general vaccine knowledge to hopefully improve the childhood vaccination rate in South Carolina. Our survey shows that COVID-19 vaccine knowledge plays a significant role in determining COVID-19 vaccine acceptance. Additionally, our results reveal that, in general, parents with greater knowledge are more accepting of vaccines.
How do we increase general vaccine knowledge? Liang et al. specifically studied the spread of Ebola information. They suggested spreading information to cohesive sub-communities and employing a cascading one-to-many model. Additionally, their study found that social media influencers were more effective in spreading information than formal health organizations [31]. Building upon this finding, we could use social media to fill in the knowledge gaps present in our community, especially the general vaccine knowledge gaps evident from our survey results. Our study shows that greater vaccination knowledge leads to greater vaccine acceptance. Additionally, our study revealed that political affiliation was a significant factor in determining vaccine acceptance. Using the one-to-many model proposed by Liang et al. we could begin building public-health campaigns centered around common values present on both ends of the political spectrum to bridge the gap in vaccination opinions. By starting at a common middle ground, we would be able to spread vaccination education in a bilateral cascade. COVID-19 has disrupted countless lives not only in South Carolina but around the world. It is important to identify the factors contributing to increased vaccine hesitancy in order to build public-health campaigns to best support the health of local communities.
Author Contributions
Conceptualization, G.W. and J.T.; methodology, G.W., J.T., C.P. and B.M.; formal analysis, G.W. and J.T.; investigation, G.W., J.T., C.P. and B.M.; data curation, J.T.; writing—original draft preparation, C.P.; writing—review and editing, G.W. and J.T.; project administration, G.W. and J.T.; funding acquisition, G.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by SC INBRE and the National Institute of General Medical Sciences of the NIH (PG0GM103499-20), the University of South Carolina Upstate’s Office of Sponsored Awards and Research Support, and the University of South Carolina’s Office of the Vice President for Research.
Institutional Review Board Statement
The study was approved by the Institutional Review Board of the University of South Carolina (Pro00110195, 22 April 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Who Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 13 April 2022).
- Centers for Disease Control and Prevention. COVID-19 Data Tracker. 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 6 December 2022).
- Travis, J.; Harris, S.; Fadel, T.; Webb, G. Identifying the determinants of COVID-19 preventative behaviors and vaccine intentions among South Carolina residents. PLoS ONE 2021, 16, e0256178. [Google Scholar] [CrossRef] [PubMed]
- Pfizer. BioNTech COVID-19 Vaccine COMIRNATY® Receives Full U.S. FDA Approval for Individuals 16 Years and Older. 2021. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-biontech-covid-19-vaccine-comirnatyr-receives-full (accessed on 6 December 2022).
- Johnson, J. Johnson & Johnson COVID-19 Vaccine Authorized by U.S. FDA For Emergency Use—First Single-Shot Vaccine in Fight Against Global Pandemic. 2021. Available online: https://www.jnj.com/media-center/press-releases/johnson-johnson-covid-19-vaccine-authorized-by-u-s-fda-for-emergency-usefirst-single-shot-vaccine-in-fight-against-global-pandemic#:~:text=NEW%20BRUNSWICK%2C%20N.J.%2C%20February%2027,of%20Johnson%20%26%20Johnson%2C%20to%20prevent (accessed on 6 December 2022).
- Johnson, J. Johnson & Johnson COVID-19 Vaccine Fully Approved by Health Canada to Prevent COVID-19 in Individuals 18 Years and Older Vaccine Demonstrates p. Johnson & Johnson. 2021. Available online: https://www.jnj.com/media-center/press-releases/johnson-johnson-covid-19-vaccine-fully-approved-by-health-canada-to-prevent-covid-19-in-individuals-18-years-and-older (accessed on 6 December 2022).
- Ledford, H. Moderna COVID vaccine becomes second to get US authorization. Nature, 2020; online ahead of print. [Google Scholar] [CrossRef]
- Wallace, M. The Advisory Committee on Immunization Practices’ Recommendation for Use of Moderna COVID-19 Vaccine in Adults Aged ≥18 Years and Considerations for Extended Intervals for Administration of Primary Series Doses of mRNA COVID-19 Vaccines—United States, February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 416–421. [Google Scholar] [PubMed]
- United States Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-Biontech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight against Pandemic; United States Food and Drug Administration: Silver Spring, MD, USA, 2021. [Google Scholar]
- United States Food and Drug Administration. FDA Authorizes Pfizer-Biontech COVID-19 Vaccine for Emergency Use in Children 5 through 11 Years of Age. 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use-children-5-through-11-years-age#:~:text=Years%20of%20Age-,FDA%20Authorizes%20Pfizer%2DBioNTech%20COVID%2D19%20Vaccine%20for%20Emergency%20Use,through%2011%20Years%20of%20Age&text=Today%2C%20the%20U.S.%20Food%20and,through%2011%20years%20of%20age (accessed on 6 December 2022).
- South Carolina Department of Health and Environmental Control. Coronavirus Disease 2019. 2022. Available online: https://scdhec.gov/covid19/covid-19-data/#viz1651519321236 (accessed on 6 December 2022).
- Schneider, K.E.; Dayton, L.; Rouhani, S.; Latkin, C.A. Implications of attitudes and beliefs about COVID-19 vaccines for vaccination campaigns in the United States: A latent class analysis. Prev. Med. Rep. 2021, 24, 101584. [Google Scholar] [CrossRef] [PubMed]
- Chanchlani, N.; Buchanan, F.; Gill, P.J. Addressing the indirect effects of COVID-19 on the health of children and young people. CMAJ 2020, 192, E921–E927. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Mack, W.J.; Neely, M.; Lewis, L.; Anand, V. Parental Perspectives on Immunizations: Impact of the COVID-19 Pandemic on Childhood Vaccine Hesitancy. J. Community Health 2022, 47, 39–52. [Google Scholar] [CrossRef] [PubMed]
- South Carolina Department of Health and Environmental Control. South Carolina Immunization Data. 2022. Available online: https://scdhec.gov/health/vaccinations/sc-immunization-data (accessed on 6 December 2022).
- Sznajder, K.K.; Kjerulff, K.H.; Wang, M.; Hwang, W.; Ramirez, S.I.; Gandhi, C.K. COVID-19 vaccine acceptance and associated factors among pregnant women in Pennsylvania 2020. Prev. Med. Rep. 2022, 26, 101713. [Google Scholar] [CrossRef] [PubMed]
- Rocha, Y.M.; de Moura, G.A.; Desidério, G.A.; de Oliveira, C.H.; Lourenço, F.D.; de Figueiredo Nicolete, L.D. The impact of fake news on social media and its influence on health during the COVID-19 pandemic: A systematic review. J. Public Health 2021, 31, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, C.A.; Borrell, L.N.; Kimball, S.; Rinke, M.L.; Rane, M.; Fleary, S.A.; Nash, D. Plans to Vaccinate Children for Coronavirus Disease 2019: A Survey of United States Parents. J. Pediatr. 2021, 237, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Khairat, S.; Zou, B.; Adler-Milstein, J. Factors and reasons associated with low COVID-19 vaccine uptake among highly hesitant communities in the US. Am. J. Infect. Control 2022, 50, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Smith, W. Does Gender Influence Online Survey Participation? A Record-Linkage Analysis of University Faculty Online Survey Response Behavior. Online Submission. 2008. Available online: https://eric.ed.gov/?id=ED501717 (accessed on 6 December 2022).
- Matoff-Stepp, S.; Applebaum, B.; Pooler, J.; Kavanagh, E. Women as health care decision-makers: Implications for health care coverage in the United States. J. Health Care Poor Underserved 2014, 25, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Reich, J.A. Neoliberal Mothering and Vaccine Refusal: Imagined Gated Communities and the Privilege of Choice. Gend. Soc. 2014, 28, 679–704. [Google Scholar] [CrossRef]
- McElfish, P.A.; Willis, D.E.; Shah, S.K.; Bryant-Moore, K.; Rojo, M.O.; Selig, J.P. Sociodemographic Determinants of COVID-19 Vaccine Hesitancy, Fear of Infection, and Protection Self-Efficacy. J. Prim. Care Community Health 2021, 12, 21501327211040746. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine Hesitancy and Its Associated Factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, D. Vaccination, politics and COVID-19 impacts. BMC Public Health 2022, 22, 96. [Google Scholar] [CrossRef] [PubMed]
- Bagasra, A.B.; Doan, S.; Allen, C.T. Racial differences in institutional trust and COVID-19 vaccine hesitancy and refusal. BMC Public Health 2021, 21, 2104. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.; Artiga, S. COVID-19 Cases and Deaths by Race/Ethnicity: Current Data and Changes over Time. 2022. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/covid-19-cases-and-deaths-by-race-ethnicity-current-data-and-changes-over-time/ (accessed on 9 May 2022).
- Stroebe, W.; Vandellen, M.R.; Abakoumkin, G.; Lemay, E.P., Jr.; Schiavone, W.M.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Reitsema, A.M.; et al. Politicization of COVID-19 health-protective behaviors in the United States: Longitudinal and cross-national evidence. PLoS ONE 2021, 16, e0256740. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics. What Is Response Bias and How Can You Avoid It? Qualtrics: Seattle, WA, USA, 2022; Available online: https://www.qualtrics.com/experience-management/research/response-bias/ (accessed on 6 June 2022).
- Seither, R. Vaccination Coverage with Selected Vaccines and Exemption Rates among Children in Kindergarten—United States, 2020–2021 School Year. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Fung, I.C.; Tse, Z.T.; Yin, J.; Chan, C.H.; Pechta, L.E.; Smith, B.J.; Marquez-Lameda, R.D.; Meltzer, M.I.; Lubell, K.M.; et al. How did Ebola information spread on twitter: Broadcasting or viral spreading? BMC Public Health 2019, 19, 438. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The role of COVID-19 and vaccine knowledge in parental intentions to vaccinate children against COVID-19. Knowledge scores varied significantly between parents who answered yes, no, or unsure in response to plans to vaccinate their child(ren); n = 517, * p < 0.01.
Figure 1.
The role of COVID-19 and vaccine knowledge in parental intentions to vaccinate children against COVID-19. Knowledge scores varied significantly between parents who answered yes, no, or unsure in response to plans to vaccinate their child(ren); n = 517, * p < 0.01.

Figure 2.
Parental intentions to vaccinate children with general recommended childhood vaccines vs. demographic factors. Summary of the reported demographics of expectant parents who responded to the survey based on their intentions for their child(ren) to receive the recommended childhood vaccinations; n = 204.
Figure 2.
Parental intentions to vaccinate children with general recommended childhood vaccines vs. demographic factors. Summary of the reported demographics of expectant parents who responded to the survey based on their intentions for their child(ren) to receive the recommended childhood vaccinations; n = 204.

Figure 3.
Parental intentions to vaccinate children against COVID-19 vs. demographic factors. Summary of the reported demographics of parents with children 17 or under who responded to the survey based on their intentions for their child(ren) to receiving the COVID-19 vaccine (n = 517). Education level: < high school (n = 26), high school diploma (n = 122), some college (n = 136), associate’s degree (n = 100), bachelor’s degree (n = 88), postgraduate degree (n = 45). Household income: < USD 24,999 (n = 94), USD 25,000–USD 49,999 (n = 180), USD 50,000–USD 74,999 (n = 104), USD 75,000–USD 99,000 (n = 68), >USD 100,000 (n = 71). Racial identity: White (n = 389), African American (n = 101), Asian/Pacific Islander (n = 5), Hispanic/Latino (n = 15), American Indian or Alaskan Native (n = 3), and Other (n = 4). Political affiliation: Democrat (n = 165), Republican (n = 190), Independent (n = 128), Apolitical (n = 23), and Other (n = 11).
Figure 3.
Parental intentions to vaccinate children against COVID-19 vs. demographic factors. Summary of the reported demographics of parents with children 17 or under who responded to the survey based on their intentions for their child(ren) to receiving the COVID-19 vaccine (n = 517). Education level: < high school (n = 26), high school diploma (n = 122), some college (n = 136), associate’s degree (n = 100), bachelor’s degree (n = 88), postgraduate degree (n = 45). Household income: < USD 24,999 (n = 94), USD 25,000–USD 49,999 (n = 180), USD 50,000–USD 74,999 (n = 104), USD 75,000–USD 99,000 (n = 68), >USD 100,000 (n = 71). Racial identity: White (n = 389), African American (n = 101), Asian/Pacific Islander (n = 5), Hispanic/Latino (n = 15), American Indian or Alaskan Native (n = 3), and Other (n = 4). Political affiliation: Democrat (n = 165), Republican (n = 190), Independent (n = 128), Apolitical (n = 23), and Other (n = 11).


{kind=link}
{kind=link}
{kind=link}
Table 1.
Multinomial regression results on intentions of expectant parents to vaccinate their children with routine childhood vaccines (n = 146).
Table 1.
Multinomial regression results on intentions of expectant parents to vaccinate their children with routine childhood vaccines (n = 146).
| B | SE | p | Odds Ratio | 95% Confidence Interval for Odds Ratio | |||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| No | Intercept | −0.186 | 1.353 | 0.890 | |||
| Age | 0.062 | 0.026 | 0.020 | 1.064 | 1.010 | 1.120 | |
| Education Level | −0.264 | 0.190 | 0.164 | 0.768 | 0.529 | 1.114 | |
| COVID-19-Vaccine Knowledge | 0.101 | 0.142 | 0.478 | 1.106 | 0.837 | 1.461 | |
| General Vaccine Knowledge | −0.060 | 0.218 | 0.784 | 0.942 | 0.614 | 1.445 | |
| COVID-19 Knowledge | −0.246 | 0.114 | 0.030 | 0.782 | 0.626 | 0.977 | |
| Race (White) | −0.110 | 0.546 | 0.840 | 0.896 | 0.307 | 2.609 | |
| Gender (Male) | −0.941 | 0.478 | 0.049 | 0.390 | 0.153 | 0.997 | |
| Political Affiliation (Democrat) | 0.193 | 0.498 | 0.699 | 1.213 | 0.457 | 3.221 | |
| Unsure | Intercept | −1.786 | 2.064 | 0.387 | |||
| Age | 0.013 | 0.038 | 0.733 | 1.013 | 0.940 | 1.092 | |
| Education Level | −0.019 | 0.256 | 0.941 | 0.981 | 0.594 | 1.622 | |
| COVID-19-Vaccine Knowledge | 0.039 | 0.194 | 0.842 | 1.040 | 0.710 | 1.522 | |
| General Vaccine Knowledge | 0.017 | 0.325 | 0.959 | 1.017 | 0.538 | 1.921 | |
| COVID-19 Knowledge | 0.060 | 0.175 | 0.734 | 1.061 | 0.753 | 1.496 | |
| Race (White) | −0.941 | 0.729 | 0.197 | 0.390 | 0.093 | 1.628 | |
| Gender (Male) | −1.511 | 0.866 | 0.081 | 0.221 | 0.040 | 1.206 | |
| Political Affiliation (Democrat) | −0.234 | 0.723 | 0.746 | 0.791 | 0.192 | 3.261 | |
The reference category for the dependent variable is “Yes”. SE = standard error.
Table 2.
Multinomial regression results on intentions to vaccinate children for COVID-19 among parents of children 17 and under (n = 353).
Table 2.
Multinomial regression results on intentions to vaccinate children for COVID-19 among parents of children 17 and under (n = 353).
| B | SE | p | Odds Ratio | 95% Confidence Interval for Odds Ratio | |||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| No | Intercept | 6.67 | 1.12 | <0.001 | |||
| Age | −0.04 | 0.02 | 0.022 | 0.96 | 0.93 | 0.99 | |
| Education Level | −0.288 | 0.12 | 0.016 | 0.75 | 0.59 | 0.95 | |
| COVID-19-Vaccine Knowledge | −0.37 | 0.11 | <0.001 | 0.69 | 0.56 | 0.85 | |
| General Vaccine Knowledge | −0.716 | 0.18 | <0.001 | 0.49 | 0.34 | 0.70 | |
| COVID-19 Knowledge | 0.166 | 0.09 | 0.061 | 1.18 | 0.99 | 1.41 | |
| Race (White) | 0.217 | 0.42 | 0.602 | 1.24 | 0.55 | 2.81 | |
| Gender (Male) | −1.709 | 0.39 | <0.001 | 0.18 | 0.09 | 0.39 | |
| Political Affiliation (Democrat) | −1.507 | 0.36 | <0.001 | 0.22 | 0.11 | 0.45 | |
| Unsure | Intercept | 2.317 | 1.21 | 0.056 | |||
| Age | −0.012 | 0.02 | 0.473 | 0.99 | 0.96 | 1.02 | |
| Education Level | −0.361 | 0.13 | 0.004 | 0.70 | 0.54 | 0.89 | |
| COVID-19-Vaccine Knowledge | −0.192 | 0.11 | 0.083 | 0.83 | 0.66 | 1.03 | |
| General Vaccine Knowledge | −0.215 | 0.20 | 0.277 | 0.81 | 0.55 | 1.19 | |
| COVID-19 Knowledge | 0.281 | 0.10 | 0.006 | 1.32 | 1.08 | 1.62 | |
| Race (White) | −0.744 | 0.42 | 0.074 | 0.48 | 0.21 | 1.08 | |
| Gender (Male) | −1.096 | 0.39 | 0.005 | 0.33 | 0.16 | 0.72 | |
| Political Affiliation (Democrat) | −1.469 | 0.39 | <0.001 | 0.23 | 0.11 | 0.49 | |
The reference category for the dependent variable is “Yes”. SE = standard error.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Phan, C.; Mercado, B.; Travis, J.; Webb, G. Identifying the Predictors of Pediatric Vaccine Uptake during the COVID-19 Pandemic. COVID 2024, 4, 495-505. https://doi.org/10.3390/covid4040033
AMA Style
Phan C, Mercado B, Travis J, Webb G. Identifying the Predictors of Pediatric Vaccine Uptake during the COVID-19 Pandemic. COVID. 2024; 4(4):495-505. https://doi.org/10.3390/covid4040033
Chicago/Turabian StylePhan, Colleen, Brandon Mercado, Justin Travis, and Ginny Webb. 2024. "Identifying the Predictors of Pediatric Vaccine Uptake during the COVID-19 Pandemic" COVID 4, no. 4: 495-505. https://doi.org/10.3390/covid4040033