Abstract
Background: A number of corticosteroids are commonly used to treat COVID-19 infection. The aim of this retrospective study was to compare various hospital outcomes among mechanically ventilated COVID-19 patients in an ICU, who were administered either dexamethasone or methylprednisolone. Methods: A total of 121 mechanically ventilated COVID-19 patients from the ICU were included in the analysis, of which 43.8% (n = 53) received methylprednisolone, while 56.2% (n = 68) received dexamethasone. Results: In-hospital mortality (p = 0.381) and hospital length of stay (p = 0.307) were lower among the methylprednisolone group, compared to the dexamethasone group, though not significantly. Survival analysis showed that there were no significant differences between the methylprednisolone and dexamethasone groups (p = 0.978). A Cox proportional regression analysis showed that in-hospital mortality was lower among COVID-19 patients receiving methylprednisolone, compared to the dexamethasone group, though not significantly (hazard ratio (HR), 0.64; 95% CI: 0.35–3.17). Conclusion: Our study showed that in-hospital mortality was lower and hospital length of stay was higher among COVID-19 patients receiving methylprednisolone, compared to dexamethasone. These findings could have been due to the small sample size and limited scope of the study. Therefore, future large-scale studies should evaluate and confirm the findings in this study.
1. Introduction
Coronavirus disease (COVID-19) has infected more than 487 million people, causing nearly 6.1 million deaths worldwide [1]. This disease has substantially affected numerous aspects of the healthcare system due to increased pressure on healthcare resources and personnel [2]. In addition, the management of COVID-19 has been affected due to a lack of concrete guidelines. This has also adversely affected the management of other health conditions due to the prioritization of resources for COVID-19 and, conversely, patients not seeking treatments due to fear of contracting the disease [3]. Several factors, such as extreme infectivity, severe lung involvement, variable disease presentation, and lack of definitive treatments, make managing COVID-19 a significant challenge. Though many studies have furthered our understanding of the disease in terms of pathogenesis and newer therapeutic options such as antiviral medications, traditional medications, and vaccines, the effectiveness of these therapeutic options has not yet been thoroughly proven [4,5,6].
Numerous studies have shown that cytokine storm constitutes the primary pathogenic mechanism for organ dysfunction and critical deterioration in this disease [7]. Therefore, interventions such as administering corticosteroids and other immunosuppressive medications could be an effective management option among patients progressing to severe forms of the disease, as previously documented in other similar conditions such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) [8,9]. Corticosteroids such as dexamethasone and methylprednisolone have been extensively used among severely affected COVID-19 patients requiring ventilation and supplemental oxygen therapy. For example, dexamethasone treatment significantly decreased 28-day mortality among patients receiving respiratory support, such as mechanical ventilation and oxygen therapy [10]. Similarly, another study that compared dexamethasone and methylprednisolone showed that both medications significantly decreased 28-day all-cause mortality among patients requiring respiratory support [11]. In addition, a study that compared dexamethasone and methylprednisolone showed that methylprednisolone demonstrated significantly better clinical status, hospital length of stay, and need for a ventilator [12]. However, not many studies compared the efficacy of dexamethasone versus methylprednisolone. This retrospective study aimed to compare various hospital outcomes among mechanically ventilated COVID-19 patients in the Intensive Care Unit (ICU), who were administered either dexamethasone or methylprednisolone.
2. Materials and Methods
2.1. Study Design and Data Source
The current study was a retrospective analysis of data from COVID-19 patients admitted to the ICU at a community hospital in South Miami between April 2020 and December 2020. The COVID-19 (SARS-CoV-2) infection was confirmed using a real-time PCR method. These patients were 18 years or older, mechanically ventilated, and were administered either dexamethasone or methylprednisolone. Patients who were administered both steroids were excluded from the analysis.
2.2. Demographic, Clinical and Laboratory Characteristics
Demographic characteristics included age, sex, and racial distribution. Clinical characteristics included body mass index (BMI), Charlson comorbidity index, APS score, APACHE III score, days on steroids, administration of hydroxychloroquine or tocilizumab, the interval between hospital admission and steroid administration, the interval between hospital admission and ICU admission, the interval between steroid administration and death, frailty levels, and disposition status. Laboratory variables included random blood sugar (RBS), insulin, C-reactive protein (CRP), ferritin, d-dimer, lactic acid, PO2, O2 saturation, bicarbonate, hematocrit, hemoglobin, white blood cell (WBC), neutrophil to lymphocyte ratio (NLR), platelet count, sodium, potassium, calcium, chloride, creatinine, bilirubin, total protein, albumin to globulin ratio (AGR), alkaline phosphate, serum glutamic pyruvic transaminase (SGPT).
2.3. Outcome Variables
Outcome variables included in-hospital mortality and hospital length of stay.
2.4. Ethical Consideration
The study was reviewed by the Baptist Health South Florida’s Institutional Review Board (IRB), which exempted the study from IRB approval and waived the requirement for informed consent because it uses previously collected deidentified data stored in electronic health records. Informed consent was not required since this study involved stored data and did not contain any identifiable information that could be linked to any specific participant.
2.5. Statistical Analysis
Differences in demographic, clinical, and laboratory characteristics were shown using the Chi-square test (or Fischer’s exact when appropriate) for categorical variables, and the t-Test (or Kruskal–Wallis test where applicable) for continuous variables. Prior to any further analysis, multiple imputations were performed to account for missing data in variables such as the interval between hospital admission and ICU admission, CRP, and D-dimer. We conducted survival analysis using the Kaplan–Meier method to compare differences in mortality between dexamethasone and methylprednisolone groups. Cox proportional hazard models were used to find associations between steroids and mortality. Variables with p < 0.10 in the bivariate analysis were included in the final model. Multivariate linear regression analysis was used to find associations between steroids and hospital length of stay. Similar to hazard models, variables with p < 0.10 in the bivariate analysis were included in the final model. For both analyses, the covariates included in the model were demographic, clinical, laboratory characteristics, and medication group. Statistical significance was set at p < 0.05, and all tests were two-sided. All statistical tests were performed using SAS software version 9.4 (Cary, NC, USA).
The study was approved by the institutional review board at Baptist Health South Florida, assuring compliance with all regulatory requirements. Since this study was a retrospective analysis of deidentified data, the requirement for informed consent was waived. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline to ensure the quality of this study [13].
3. Results
A total of 121 mechanically ventilated patients from the ICU were included in the analysis, of which 43.8% (n = 53) received methylprednisolone, while 56.2% (n = 68) received dexamethasone. The Median (IQR) age of the sample was 71.0 (59.0, 78.0) years. There were more males compared to females (70.2% vs. 29.8%), and the majority were of Hispanic ethnicity (79.3%). Demographic characteristics did not differ significantly between those receiving methylprednisolone or dexamethasone (Table 1).

Table 1.
Comparison of demographic, clinical, and laboratory characteristics between patients administered methylprednisolone and dexamethasone.
The total number of days on steroids was significantly higher among patients receiving dexamethasone as compared to methylprednisolone (15.5 days vs. 9.0 days, p < 0.001). Sixteen patients in the methylprednisolone group received hydroxychloroquine, while none of the patients in the dexamethasone group were administered hydroxychloroquine. Eleven patients in the methylprednisolone group received tocilizumab, while four patients in the dexamethasone group were administered tocilizumab (p = 0.029).
CRP, ferritin, D-dimer, lactic acid, PO2, O2 saturation, NLR, sodium, chloride, AGR, and SGPT were higher among the methylprednisolone group, while RBS, insulin, bicarbonate, hematocrit, hemoglobin, WBC, platelet count, potassium, bilirubin, total protein, and alkaline phosphatase were higher among dexamethasone group, though not significantly (Table 1). Creatinine was significantly higher among the methylprednisolone group (2.0 mg/dL vs. 1.2 mg/dL, p = 0.041), while calcium was significantly higher among the dexamethasone group (8.1 mg/dl vs. 8.6 mg/dL, p = 0.002).
The time interval between steroid administration and death was significantly lower among the methylprednisolone group compared to the dexamethasone group (321.4 h vs. 451.4 h, p = 0.014). The time interval between hospital admission and steroid administration was significantly higher among the methylprednisolone group compared to the dexamethasone group (32.3 h vs. 8.4 h, p < 0.001). The time interval between hospital admission and ICU admission was significantly lower among the methylprednisolone group, compared to the dexamethasone group (90.7 h vs. 429.5 h, p = 0.002). Table 1 shows the comparison of demographic, clinical, and laboratory characteristics between patients administered methylprednisolone and dexamethasone.
In-hospital mortality (66.0% vs. 75.0%, p = 0.381) and hospital length of stay (17.0 days vs. 18.5 days, p = 0.307) were lower among the methylprednisolone group, compared to the dexamethasone group, though not significantly (Figure 1).
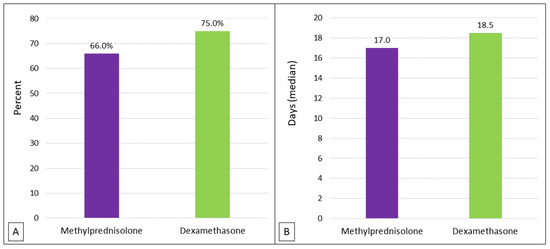
Figure 1.
Comparison of methylprednisolone and dexamethasone on (A) in-hospital mortality and (B) hospital length of stay.
A Kaplan–Meier survival analysis showed that there were no significant differences in survival between the methylprednisolone and dexamethasone groups (Logrank p = 0.978) (Figure 2).
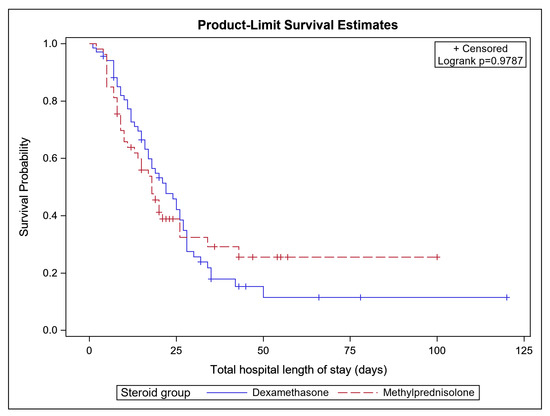
Figure 2.
Kaplan–Meier curves comparing in-hospital mortality between COVID-19 patients on methylprednisolone and dexamethasone.
A Cox proportional regression analysis showed that in-hospital mortality was lower among COVID-19 patients receiving methylprednisolone, compared to the dexamethasone group, though not significantly (hazard ratio (HR), 0.64; CI: 0.35–3.17). However, other factors such as age (HR, 1.02; CI: 1.01–1.03, p = 0.024), days on steroids (HR, 0.87; CI: 0.83–0.92, p = <0.001), CRP (HR, 1.44; CI: 1.06–1.97, p = 0.018), creatinine (HR, 1.72; CI: 1.10–2.69, p = 0.016), tocilizumab (HR, 0.35; CI: 0.14–0.86, p = 0.021), and time interval from admission to steroid administration (HR, 0.97; CI: 0.96–0.99, p = 0.001) showed significant associations in our analysis (Table 2).
Table 2.
Differences in in-hospital mortality between patients administered dexamethasone and methylprednisone.
A Multivariate linear regression analysis showed that the mean hospital length of stay was not different between the methylprednisolone and dexamethasone groups (Estimate, 3.83; 95% CI: −0.53, 8.18, p = 0.084) (Table 3).
Table 3.
Differences in length of stay between patients administered dexamethasone and methylprednisone.
4. Discussion
The COVID-19 pandemic has caused considerable morbidity and mortality worldwide. Although vaccines successfully prevent the disease, the emergence of newer strains and incomplete penetrance of the vaccine among different populations is still a challenge to the healthcare community. Due to these factors, control over infection and mortality has been inadequate. Hence, patients are still being admitted, and physicians are treating them using existing guidelines. Since COVID-19 was first reported, there have been many studies on the pathophysiology of the disease, and therapeutic and procedural interventions. For example, since a patient’s own immunological mechanisms cause much harm and deterioration, immunosuppressive medications have gained importance.
In our study, we compared hospital outcomes between COVID-19 patients administered dexamethasone or methylprednisolone to understand which medication is more efficacious. We found that although mortality was lower among the methylprednisolone group, they did not differ statistically between the two groups. Similar to our findings, in a triple-blinded randomized controlled trial, though mortality rates were lower among patients administered methylprednisolone, they were not statistically different from dexamethasone [12]. In a quasi-experimental study of 100 moderate-to-severe COVID-19 patients, mortality rates did not differ significantly between those administered dexamethasone or methylprednisolone [14]. This study also showed that there were substantial improvements in factors such as CRP, fever, and oxygen requirements in both groups. Likewise, in a single-center retrospective study of ICU-admitted COVID-19 patients, mortality rates did not differ between hydrocortisone, methylprednisolone or dexamethasone [15]. However, patients on methylprednisolone had significantly fewer sepsis rates. Contrary to these findings, in a retrospective study among 262 COVID-19 patients requiring mechanical ventilation, methylprednisolone significantly decreased mortality compared to dexamethasone [16]. Similarly, a prospective cohort study among 414 patients diagnosed with severe COVID-19 showed that mortality rates were significantly lower among those administered methylprednisolone [17]. Interestingly, even among studies that did not show significant differences, mortality rates were lower among the methylprednisolone group. This could be explained by the fact that methylprednisolone achieves greater lung penetrance and higher concentration in the lung epithelial lining fluid [18,19]. Our results non-significantly favored methylprednisolone. This could have been due to the relatively smaller sample size of our study.
Our regression analysis showed that factors such as older age, and higher levels of CRP and creatinine were detrimental, whereas days on steroids, greater duration from admission to steroid administration, and Tocilizumab use were protective. These findings are not surprising and have been demonstrated in other studies as well. An increase in CRP levels is indicative of systemic inflammation and is seen in viral and bacterial infections. Studies have shown that a higher level of CRP is associated with increased mortality among COVID-19 patients [20,21]. Higher serum creatinine levels within 24 h of admission among COVID-19 patients is an independent risk factor for mortality [22,23]. We also found that a greater time interval for starting steroid administration was associated with higher mortality. The RECOVERY collaborative showed that early administration of dexamethasone did not significantly decrease mortality [24]. In another study, Bahl et al. showed that delaying steroid administration increased survival benefits [25]. Though some evidence has contrarily demonstrated that early administration of steroids could be beneficial among COVID-19 patients, there has been no clear consensus on when the doses should be administered [26,27,28]. These findings could be due to profound immunosuppression by steroids in the absence of inflammation [29].
Another interesting finding was that the time interval between hospital admission and steroid administration was significantly higher among the methylprednisolone group, whereas the time interval between hospital admission and ICU admission was significantly higher among the dexamethasone group. This discrepancy could be due to the fact that a greater number of patients were treated with methylprednisolone in the early months of the pandemic, and these patients could have been admitted earlier to the ICU, (lower APACHE score), compared to patients treated with dexamethasone. This indicates that the understanding of natural history and pathogenesis of COVID-19 and its ICU management strategies evolved and changed during the study period.
We found that hospital length of stay was higher among the methylprednisolone group; however, that did not differ statistically between the two groups. Contrary to our finding, in a study by Ranjbar et al., hospital length of stay was significantly lower among COVID-19 patients receiving methylprednisolone than dexamethasone [12]. In a meta-analysis by Bajaj et al., a pooled analysis showed no significant differences in length of stay between methylprednisolone and dexamethasone [30]. In our study, univariate analysis showed that the length of stay was lower among the methylprednisolone group compared to the dexamethasone group. However, directionality reversed in the multivariate analysis and lost significance, even after accounting for mortality. Given these inconsistencies, future large-scale studies should investigate more on these relationships.
Limitations
In the current study being a retrospective analysis, we did not have adequate control over the type of steroid used. In addition, we did not have data on the dosage and frequency of these medications. In our sample, 43.8% of the patients received methylprednisolone, and 56.2% received dexamethasone. In our analysis, we considered only the steroids that were prescribed for COVID-19 treatment. However, some of these patients may have also received steroids for other conditions. In addition, other COVID-19-specific therapies could have been co-administered with steroids. We only included hydroxychloroquine and tocilizumab and did not include other medications in our models. This could have affected some of our findings. Our study included only ventilated COVID-19 patients who received steroids. Only a few patients who were not on ventilators received steroids and were excluded from the analysis. Hence, we could not assess the effect of steroids on outcomes among non-ventilated patients. Nearly 80% of our patients were Hispanic, so our findings may not be generalizable to other diverse populations. We did not include the ROX score and data on high-flow nasal oxygen therapy because of the large number of missing values. In addition, we did not have data on co-infection at mechanical ventilation onset and secondary infections during the ICU course. Finally, we had a small sample size and did not have information on complications and imaging data.
5. Conclusions
Our study showed that in-hospital mortality was lower and hospital length of stay was higher in COVID-19 patients receiving methylprednisolone in comparison to dexamethasone. However, these findings were not statistically significant and could have been due to the small sample size and limited scope of the study. Therefore, we recommend that further large-scale studies evaluate and confirm this study’s findings.
Author Contributions
Conceptualization, M.C.; methodology, A.S. and M.R.; validation, K.N.W.; formal analysis, M.A.A. and Z.Z.; writing—original draft preparation, V.R.; writing—review and editing, P.M.; supervision, M.C. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité—Universitätsmedizin Berlin.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Baptist Health South Florida (protocol code 1696214–1).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and confidentiality.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 16 January 2023).
- Sabetian, G.; Moghadami, M.; Hashemizadeh Fard Haghighi, L.; Shahriarirad, R.; Fallahi, M.J.; Asmarian, N.; Moeini, Y.S. COVID-19 infection among healthcare workers: A cross-sectional study in southwest Iran. Virol. J. 2021, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Søreide, K.; Hallet, J.; Matthews, J.B.; Schnitzbauer, A.A.; Line, P.D.; Lai, P.; Otero, J.; Callegaro, D.; Warner, S.G.; Baxter, N.N. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. J. Br. Surg. 2020, 107, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Young, B.; Tan, T.T.; Leo, Y.S. The place for remdesivir in COVID-19 treatment. Lancet Infect. Dis. 2021, 21, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Vetter, P.; Kaiser, L.; Calmy, A.; Agoritsas, T.; Huttner, A. Dexamethasone and remdesivir: Finding method in the COVID-19 madness. Lancet Microbe 2020, 1, e309–e310. [Google Scholar] [CrossRef]
- Shahriarirad, R.; Khodamoradi, Z.; Erfani, A.; Hosseinpour, H.; Ranjbar, K.; Emami, Y.; Mirahmadizadeh, A.; Lotfi, M.; Shirazi Yeganeh, B.; Dorrani Nejad, A. Epidemiological and clinical features of 2019 novel coronavirus diseases (COVID-19) in the South of Iran. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Mandourah, Y.; Al-Hameed, F.; Sindi, A.A.; Almekhlafi, G.A.; Hussein, M.A.; Jose, J.; Pinto, R.; Al-Omari, A.; Kharaba, A. Corticosteroid therapy for critically ill patients with Middle East respiratory syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: Systematic review of treatment effects. PLoS Med. 2006, 3, e343. [Google Scholar] [CrossRef]
- Duman, I.; Celik, J.B.; Iyisoy, M.S.; Degirmencioglu, S.; Korkmaz, A.; Duman, A. Evaluation of personalized methylprednisolone therapy in critically ill COVID-19 patients: An observational comparative study using real-life data. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 4497–4508. [Google Scholar]
- Sterne, J.A.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Gholampoor Saadi, M.H. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed]
- Fatima, S.A.; Asif, M.; Khan, K.A.; Siddique, N.; Khan, A.Z. Comparison of efficacy of dexamethasone and methylprednisolone in moderate to severe covid 19 disease. Ann. Med. Surg. 2020, 60, 413–416. [Google Scholar] [CrossRef]
- Du Plessis, E.; Lalla, U.; Allwood, B.; Louw, E.; Nortje, A.; Parker, A.; Taljaard, J.; Ayele, B.; Nyasulu, P.; Koegelenberg, C. Corticosteroids in critical COVID-19: Are all corticosteroids equal? South Afr. Med. J. 2021, 111, 550–553. [Google Scholar]
- Ko, J.J.; Wu, C.; Mehta, N.; Wald-Dickler, N.; Yang, W.; Qiao, R. A comparison of methylprednisolone and dexamethasone in intensive care patients with COVID-19. J. Intensive Care Med. 2021, 36, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.A.M.; Mohamed, A.H.; Owaynat, A.H. Comparison between methylprednisolone infusion and dexamethasone in COVID-19 ARDS mechanically ventilated patients. Egypt. J. Intern. Med. 2022, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Analysis, A.P. Methylprednisolone Achieves Greater Concentrations in the Lung Than Prednisolone. Am. Rev. Respir Dis. 1991, 144, 586–592. [Google Scholar]
- Braude, A.; Rebuck, A. Prednisone and methylprednisolone disposition in the lung. Lancet 1983, 322, 995–997. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Nguy, V.; Aphinyanaphongs, Y.; Newman, J.D.; Xia, Y.; Reynolds, H.R.; Hochman, J.S.; Fishman, G.I.; Berger, J.S. Multiple biomarker approach to risk stratification in COVID-19. Circulation 2021, 143, 1338–1340. [Google Scholar] [CrossRef]
- Alfano, G.; Ferrari, A.; Fontana, F.; Mori, G.; Ligabue, G.; Giovanella, S.; Magistroni, R.; Meschiari, M.; Franceschini, E.; Menozzi, M. Twenty-four-hour serum creatinine variation is associated with poor outcome in the novel coronavirus disease 2019 (COVID-19) patients. Kidney Res. Clin. Pract. 2021, 40, 231. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.; Van Biesen, W.; Hoste, E.; Vanholder, R. The prevention of acute kidney injury: An in-depth narrative review Part 1: Volume resuscitation and avoidance of drug- and nephrotoxin-induced AKI. Clin. Kidney J. 2008, 1, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Group RECOVERY Collaborative. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Bahl, A.; Johnson, S.; Chen, N.-W. Timing of corticosteroids impacts mortality in hospitalized COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S. Early short-course corticosteroids in hospitalized patients with COVID-19. Clin. Infect. Dis. 2020, 71, 2114–2120. [Google Scholar] [CrossRef]
- Lee, N.; Chan, K.C.A.; Hui, D.S.; Ng, E.K.O.; Wu, A.; Chiu, R.W.K.; Wong, V.W.S.; Chan, P.K.S.; Wong, K.T.; Wong, E.; et al. Effects of early corticosteroid treatment on plasma SARS-associated Coronavirus RNA concentrations in adult patients. J. Clin. Virol. 2004, 31, 304–309. [Google Scholar] [CrossRef]
- Ni, Y.-N.; Chen, G.; Sun, J.; Liang, B.-M.; Liang, Z.-A. The effect of corticosteroids on mortality of patients with influenza pneumonia: A systematic review and meta-analysis. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. Lancet Infect. Dis. 2013, 13, 260–268. [Google Scholar] [CrossRef]
- Bajaj, D.; Gupta, M.; Manek, G.; Manek, G.; Hu, K.; Boregowda, U. Dexamethasone versus Methylprednisolone in Hospitalized COVID-19 Patients: A Systematic Review and Meta-Analysis. Int. J. Crit. Care Emerg. Med. 2021, 7, 128. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).