Form Matters—Technical Cues in the Single Leg Heel Raise to Failure Test Significantly Change the Outcome: A Study of Convergent Validity in Australian Football Players


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Player Characteristics
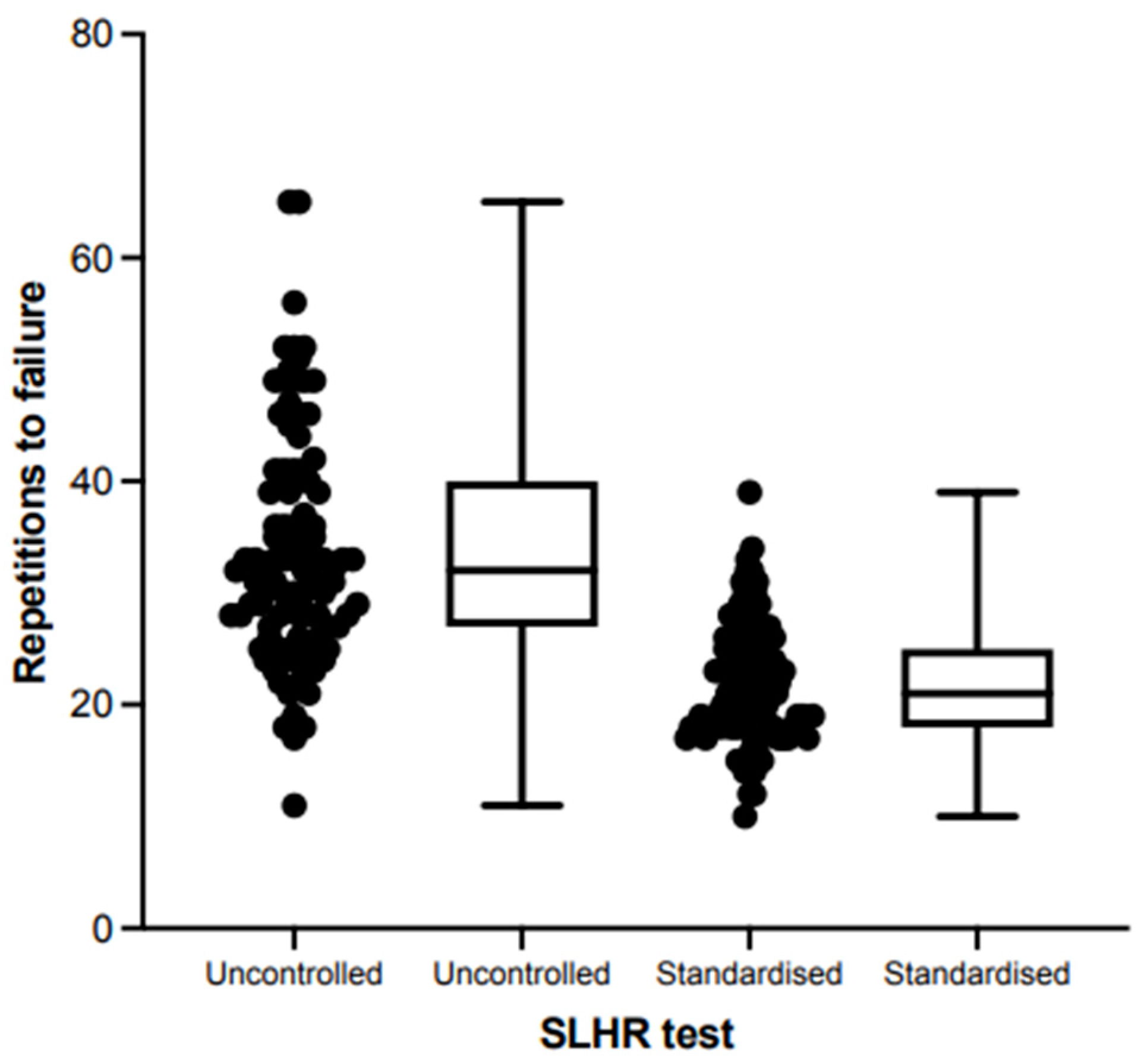
3.2. Calf Muscle Strength–Endurance
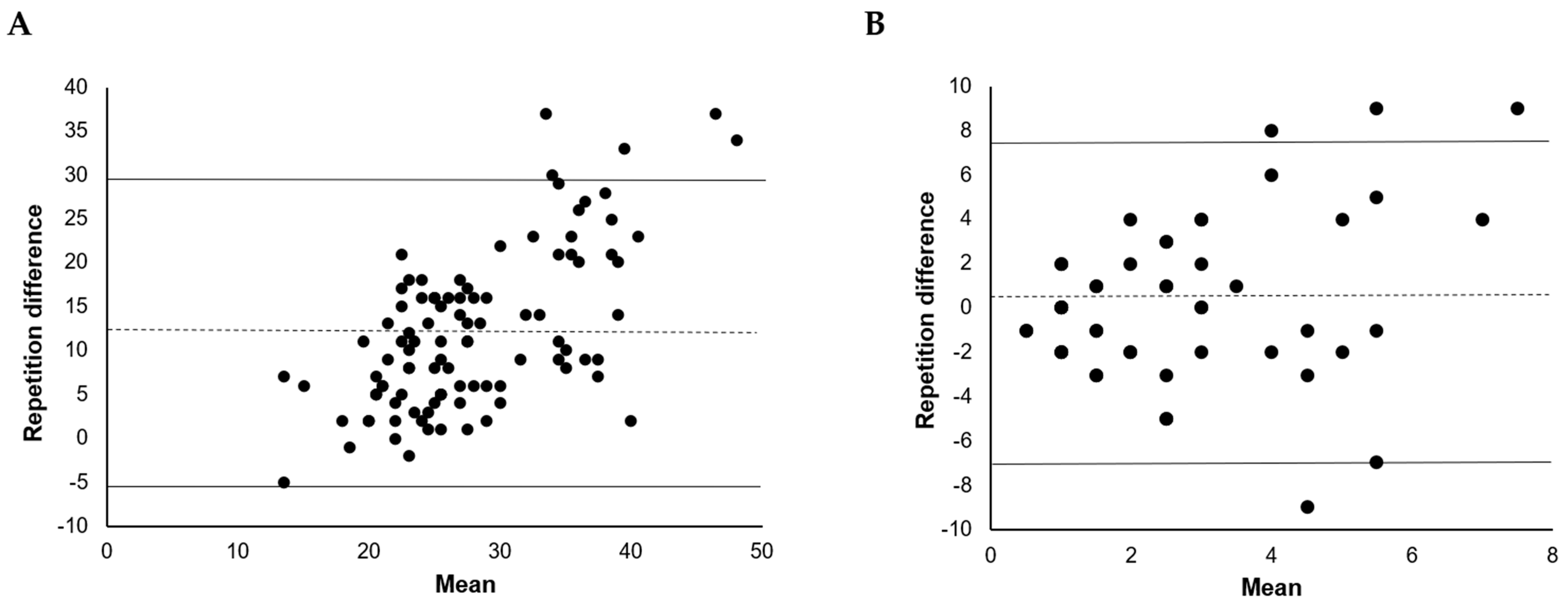
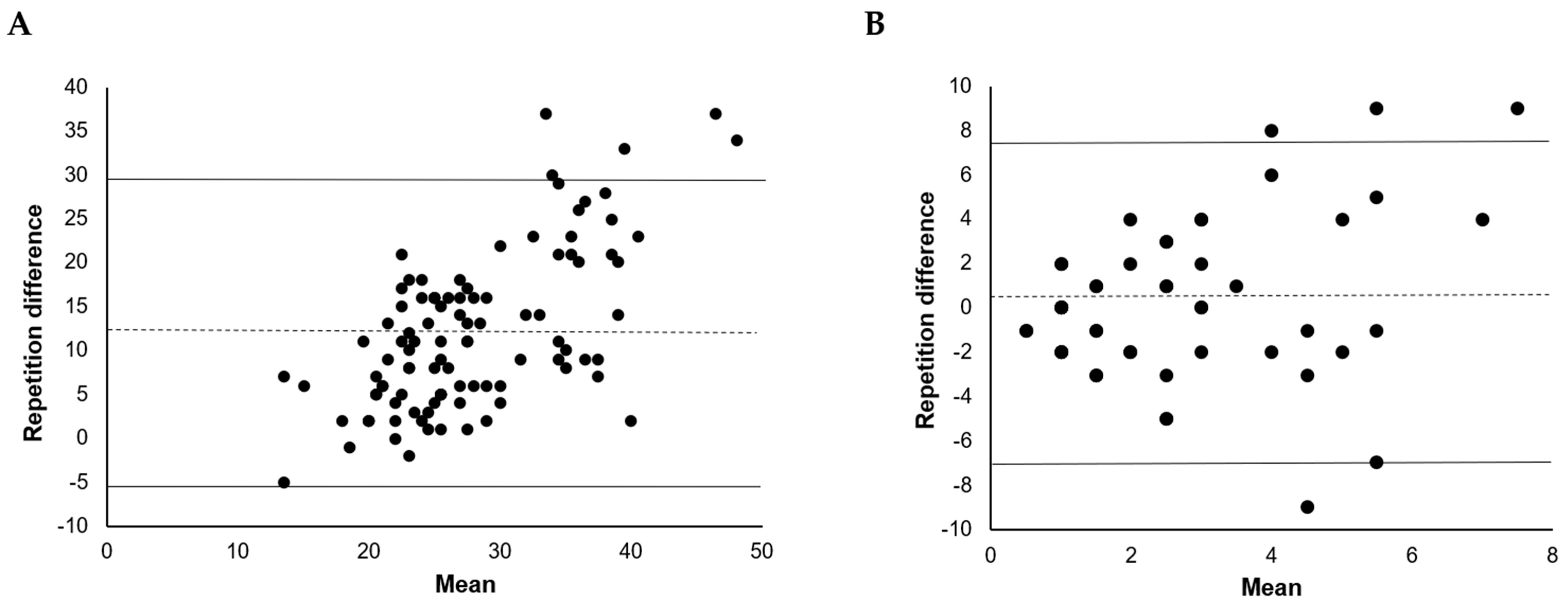
3.3. Agreement between Tests
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamner, S.R.; Delp, S.L. Muscle contributions to fore-aft and vertical body mass center accelerations over a range of running speeds. J. Biomech. 2013, 46, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Maniar, N.; Schache, A.G.; Cole, M.H.; Opar, D.A. Lower-limb muscle function during sidestep cutting. J. Biomech. 2019, 82, 186–192. [Google Scholar] [CrossRef]
- Schache, A.G.; Lai, A.K.M.; Brown, N.A.T.; Crossley, K.M.; Pandy, M.G. Lower-limb joint mechanics during maximum acceleration sprinting. J. Exp. Biol. 2019, 222, jeb209460. [Google Scholar] [CrossRef] [PubMed]
- Sara, L.K.; Gutsch, S.B.; Hunter, S.K. The single-leg heel raise does not predict maximal plantar flexion strength in healthy males and females. PLoS ONE 2021, 16, e0253276. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Rio, E.; Debenham, J.; Docking, S.; Travers, M.; Gibson, W. Evaluating the progress of mid-portion achilles tendinopathy during rehabilitation: A review of outcome measures for muscle structure and function, tendon structure, and neural and pain associated mechanisms. Int. J. Sports Phys. Ther. 2018, 13, 537–551. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Ngawhika, T.M.; Balsalobre-Fernandez, C.; O’Neill, S. Calf muscle abilities are related to sprint performance in male Rugby Union players. Phys. Ther. Sport 2023, 64, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Ngawhika, T.M.; Gill, N.; Balsalobre-Fernandez, C. Validity, reliability, and normative data on calf muscle function in rugby union players from the Calf Raise application. Sports Biomech. 2022, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Hebert-Losier, K.; Schneiders, A.G.; Newsham-West, R.J.; Sullivan, S.J. Scientific bases and clinical utilisation of the calf raise test. Phys. Ther. Sport 2009, 10, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. The heel-raise test for ankle plantarflexor strength: A scoping review and meta-analysis of studies providing norms. J. Phys. Ther. Sci. 2022, 34, 528–531. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef]
- Barillas, S.R.; Oliver, J.L.; Lloyd, R.S.; Pedley, J.S. Kinetic Responses to External Cues Are Specific to Both the Type of Cue and Type of Exercise in Adolescent Athletes. J. Strength Cond. Res. 2023, 37, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; McClelland, J.A.; Semciw, A.I.; Schache, A.G.; McCall, A.; Pizzari, T. The Assessment, Management and Prevention of Calf Muscle Strain Injuries: A Qualitative Study of the Practices and Perspectives of 20 Expert Sports Clinicians. Sports Med. Open 2022, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Sman, A.D.; Hiller, C.E.; Imer, A.; Ocsing, A.; Burns, J.; Refshauge, K.M. Design and reliability of a novel heel rise test measuring device for plantarflexion endurance. BioMed Res. Int. 2014, 2014, 391646. [Google Scholar] [CrossRef] [PubMed]
- Lehecka, B.J.; Daniels, T.; Koester, B.; Kropp, W.; Reeves, M.; Waterson, R. Effects of Verbal and Tactile Cues on Gluteal Force Production and Broad Jump Distance. Int. J. Sports Phys. Ther. 2024, 19, 284–289. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M.R.; Cormack, S.J.; Gill, N.D. Strength and Power Profiling of Athletes: Selecting Tests and How to Use the Information for Program Design. Strength Cond. J. 2013, 35, 7–14. [Google Scholar] [CrossRef]
- Alcazar, J.; Csapo, R.; Ara, I.; Alegre, L.M. On the Shape of the Force-Velocity Relationship in Skeletal Muscles: The Linear, the Hyperbolic, and the Double-Hyperbolic. Front. Physiol. 2019, 10, 438208. [Google Scholar] [CrossRef]
- Cormie, P.; McGuigan, M.R.; Newton, R.U. Developing maximal neuromuscular power: Part 1--biological basis of maximal power production. Sports Med. 2011, 41, 17–38. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.C.; Debenham, J.; Bulsara, C.; Chivers, P.; Rio, E.K.; Docking, S.; Travers, M.; Gibson, W. Assessment and monitoring of Achilles tendinopathy in clinical practice: A qualitative descriptive exploration of the barriers clinicians face. BMJ Open Sport Exerc. Med. 2022, 8, e001355. [Google Scholar] [CrossRef] [PubMed]
- Meek, W.M.; Kucharik, M.P.; Eberlin, C.T.; Naessig, S.A.; Rudisill, S.S.; Martin, S.D. Calf Strain in Athletes. JBJS Rev. 2022, 10, e21.00183. [Google Scholar] [CrossRef]
- van der Vlist, A.C.; Breda, S.J.; Oei, E.H.G.; Verhaar, J.A.N.; de Vos, R.J. Clinical risk factors for Achilles tendinopathy: A systematic review. Br. J. Sports Med. 2019, 53, 1352–1361. [Google Scholar] [CrossRef]
- O’Neill, S.; Barry, S.; Watson, P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: The role of soleus. Phys. Ther. Sport 2019, 37, 69–76. [Google Scholar] [CrossRef]
- Kelly, S.; Pollock, N.; Polglass, G.; Clarsen, B. Injury and Illness in Elite Athletics: A Prospective Cohort Study Over Three Seasons. Int. J. Sports Phys. Ther. 2022, 17, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Hultman, K.; Szukics, P.F.; Grzenda, A.; Curriero, F.C.; Cohen, S.B. Gastrocnemius Injuries in Professional Baseball Players: An Epidemiological Study. Am. J. Sports Med. 2020, 48, 2489–2498. [Google Scholar] [CrossRef]
- Green, B.; Lin, M.; McClelland, J.A.; Semciw, A.I.; Schace, A.G.; Rotstein, A.; Cook, J.; Pizzari, T. Return to play and recurrence after calf muscle strain injuries in elite Australian football players. Am. J. Sports Med. 2020, 48, 363546520959327. [Google Scholar] [CrossRef]
- Orchard, J.W.; Jomaa, M.C.; Orchard, J.J.; Rae, K.; Hoffman, D.T.; Reddin, T.; Driscoll, T. Fifteen-week window for recurrent muscle strains in football: A prospective cohort of 3600 muscle strains over 23 years in professional Australian rules football. Br. J. Sports Med. 2020, 54, 1103–1107. [Google Scholar] [CrossRef]
- Hebert-Losier, K.; Wessman, C.; Alricsson, M.; Svantesson, U. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy 2017, 103, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Schneiders, A.G.; García, J.A.; Sullivan, S.J.; Simoneau, G.G. Influence of knee flexion angle and age on triceps surae muscle activity during heel raises. J. Strength Cond. Res. 2012, 26, 3124–3133. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef]
- Lee, M.; Lancaster, M.; Tulloch, L.; O’Leary, B.; Power, E.; Howes, D.; Sourbuts, B.; Berry, A.; Maher, F.; O’Neill, S. Normative isometric plantarflexion strength values for professional level, male rugby union athletes. Phys. Ther. Sport 2023, 61, 114–121. [Google Scholar] [CrossRef]
- Green, B.; Lin, M.; Schache, A.G.; McClelland, J.A.; Rotstein, A.H.; Semciw, A.I.; Cook, J.; Pizzari, T. Calf muscle strain injuries in elite Australian football players: A descriptive epidemiological evaluation. Scand. J. Med. Sci. Sports 2020, 30, 174–184. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Yasui, Y.; Tonogai, I.; Rosenbaum, A.J.; Shimozono, Y.; Kawano, H.; Kennedy, J.G. The Risk of Achilles Tendon Rupture in the Patients with Achilles Tendinopathy: Healthcare Database Analysis in the United States. BioMed. Res. Int. 2017, 2017, 7021862. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef]
- van Stralen, K.J.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Measuring agreement, more complicated than it seems. Nephron Clin. Pract. 2012, 120, c162–c167. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.C.; Travers, M.; Chivers, P.; Debenham, J.; Docking, S.I.; Rio, E.K.; Gibson, W.; Ardern, C. Can we really say getting stronger makes your tendon feel better? No current evidence of a relationship between change in Achilles tendinopathy pain or disability and changes in Triceps Surae structure or function when completing rehabilitation: A systematic review. J. Sci. Med. Sport. 2023, 26, 253–260. [Google Scholar] [CrossRef]
- Green, B.; Pizzari, T. Calf muscle strain injuries in sport: A systematic review of risk factors for injury. Br. J. Sports Med. 2017, 51, 1189–1194. [Google Scholar] [CrossRef]
- Orchard, J.W. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am. J. Sports Med. 2001, 29, 300–303. [Google Scholar] [CrossRef]
- Orchard, J.; Orchard, J.; Seward, H. A Comparison between Australian Football League (AFL) Injuries in Australian Indigenous versus Non-indigenous Players. Sports 2013, 1, 69–77. [Google Scholar] [CrossRef]
- Fujiwara, K.; Asai, H.; Toyama, H.; Kunita, K.; Yaguchi, C.; Kiyota, N.; Tomita, H.; Jacobs, J.V. Changes in muscle thickness of gastrocnemius and soleus associated with age and sex. Aging Clin. Exp. Res. 2010, 22, 24–30. [Google Scholar] [CrossRef]
- Kubo, K.; Morimoto, M.; Komuro, T.; Yata, H.; Tsunoda, N.; Kanehisa, H.; Fukunaga, T. Effects of Plyometric and Weight Training on Muscle-Tendon Complex and Jump Performance. Med. Sci. Sports Exerc. 2007, 39, 1801–1810. [Google Scholar] [CrossRef]
- Bertelson, M.L.; Hulme, A.; Peterson, J.; Brund, R.K.; Sørensen, H.; Finch, C.F.; Parner, E.T.; Nielsen, R.O. A framework for the etiology of running-related injuries. Scand. J. Med. Sci. Sports 2017, 27, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.H.; Hornsby, W.G.; Suarez, D.G.; Duca, M.; Pierce, K.C. Training Specificity for Athletes: Emphasis on Strength-Power Training: A Narrative Review. J. Funct. Morphol. Kinesiol. 2022, 7, 102. [Google Scholar] [CrossRef] [PubMed]
- Vaara, J.P.; Kyröläinen, H.; Niemi, J.; Ohrankämmen, O.; Häkkinen, A.; Kocay, S.; Häkkinen, K. Associations of maximal strength and muscular endurance test scores with cardiorespiratory fitness and body composition. J. Strength Cond. Res. 2012, 26, 2078–2086. [Google Scholar] [CrossRef] [PubMed]
- Ishøi, L.; Krommes, K.; Husted, R.S.; Juhl, C.B.; Thorborg, K. Diagnosis, prevention and treatment of common lower extremity muscle injuries in sport—Grading the evidence: A statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF). Br. J. Sports Med. 2020, 54, 528–537. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Non-Cued SLHR | Cued SLHR | |||||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Range | Mean (SD) | Median (IQR) | Range | |
| All legs | 33.9 (10.3) * | 32 (27–40) | 11–65 | 21.9 (5.3) | 21 (18–25) | 10–39 |
| Leg dominance | ||||||
| Dominant | 34.1 (9.9) | 32 (27.8–40.3) | 18–65 | 21.5 (5.3) | 22 (18–25) | 10–34 |
| Non-dominant | 33.6 (10.8) | 31 (25–40.5) | 11–65 | 22.2 (5.5) | 21 (18–26) | 12–39 |
| Sex | ||||||
| Women | 30.3 (9.2) | 29 (24–33.5) | 11–52 | 21.2 (5.6) | 19 (17–24) | 14–39 |
| Men | 36.8 (10.4) ^ | 35 (29–45) | 17–65 | 22.3 (5.1) | 22 (19–26) | 10–33 |
| RT history | ||||||
| Completing Calf RT | 35.7 (10.4) ^ | 33 (28–41) | 21–65 | 23.1 (5.5) ^ | 22.5 (18.8–27.3) | 14–39 |
| Not completing Calf RT | 30.9 (9.6) | 29.5 (25–36.3) | 11–51 | 19.8 (4.4) | 19 (17–23) | 10–29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Green, B.; Coventry, M.; Pizzari, T.; Rio, E.K.; Murphy, M.C. Form Matters—Technical Cues in the Single Leg Heel Raise to Failure Test Significantly Change the Outcome: A Study of Convergent Validity in Australian Football Players. BioMed 2024, 4, 89-99. https://doi.org/10.3390/biomed4020007
Green B, Coventry M, Pizzari T, Rio EK, Murphy MC. Form Matters—Technical Cues in the Single Leg Heel Raise to Failure Test Significantly Change the Outcome: A Study of Convergent Validity in Australian Football Players. BioMed. 2024; 4(2):89-99. https://doi.org/10.3390/biomed4020007
Chicago/Turabian StyleGreen, Brady, Molly Coventry, Tania Pizzari, Ebonie K. Rio, and Myles C. Murphy. 2024. "Form Matters—Technical Cues in the Single Leg Heel Raise to Failure Test Significantly Change the Outcome: A Study of Convergent Validity in Australian Football Players" BioMed 4, no. 2: 89-99. https://doi.org/10.3390/biomed4020007
APA StyleGreen, B., Coventry, M., Pizzari, T., Rio, E. K., & Murphy, M. C. (2024). Form Matters—Technical Cues in the Single Leg Heel Raise to Failure Test Significantly Change the Outcome: A Study of Convergent Validity in Australian Football Players. BioMed, 4(2), 89-99. https://doi.org/10.3390/biomed4020007