Abstract
Dyslexia is classed as a neurobiological difficulty and is referred to as a Specific Learning Disability (SPLD) that primarily affects reading, writing, working memory (WM), and organisational skills. Positive psychology interventions (PPIs) have been found to increase self-esteem, self-efficacy, and confidence and lower anxiety among students with dyslexia. Therefore, to summarise the current evidence on PPIs, a narrative review was undertaken. The review synthesised the findings from six studies that investigated PPIs for dyslexic individuals across various education settings. Four key themes emerged: (1) characteristics and effectiveness of PPIs, (2) level of education, (3) gender differences, and (4) PPIs differences in Western and Eastern countries. The analysis revealed that group interventions in secondary schools positively impacted self-esteem and social skills among dyslexic pupils, while the efficacy of sunflower therapy for dyslexic children showed inconclusive results on academic performance but potential psychological benefits. Socioemotional wellbeing programmes for dyslexic children yielded mixed outcomes, with temporary increases in self-esteem post-programme. Mindfulness meditation demonstrated promise in improving reading accuracy and attention functions in adults with dyslexia. Positive psychology group interventions effectively enhanced subjective wellbeing, academic self-concept, and achievement among dyslexic children. Early interventions showed promise in improving coping strategies, perceived control, and overall wellbeing among students with dyslexia. This review highlights the potential benefits of diverse interventions across different educational settings, emphasising the importance of early support and targeted interventions for individuals with dyslexia.
1. Introduction
Dyslexia is classed as a neurobiological difficulty and is referred to as a specific learning disability (SLD) that primarily affects reading, writing, and organisational skills [1]. While no association has been found between dyslexia and intelligence (indeed, individuals with dyslexia often have average or above-average intelligence), they may struggle with certain tasks related to reading and language processing [2]. For example, children with dyslexia have demonstrated poor phonological skills (e.g., phonological short-term memory), nonphonological language skills (e.g., vocabulary), and auditory processing [3], as well as problems with general working memory (WM) and auditory temporal processing [4]. These skills are integral to language acquisition, reading, writing, and general language processing abilities [5].
The prevalence of dyslexia varies significantly across the world, which could be explained by differences in diagnostic criteria [6], as well as the general underdiagnosis of the condition globally [7]. The global prevalence has been estimated at 10% [8]; however, this varies widely between countries. Wagner et al. (2020) [1] reported that 10–12% of children in English-speaking countries have dyslexia, although this might vary depending on the severity and presence of symptoms needed for diagnosis. In the Netherlands, the reported prevalence falls between the range of 10–19%, 3–7% in the USA, 4% in Italy, 5% in Germany, and 4–9% in China [9,10,11]. Some have argued that the variance in prevalence between countries is due to orthographies. However, this does not explain the significant differences in dyslexia prevalence identified among children between districts within the same countries, such as Germany, Romania, and the Scandinavian nations who speak and write the same language [12].
Regarding gender differences, the diagnostic rate of dyslexia is generally higher in boys than girls [9,13], which can be explained by the severity and presentation of symptoms of inattention. Boys tend to present symptoms of inattention associated with dyslexia for longer periods of time (i.e., before and during school hours), whereas girls’ symptoms reach the same severity but generally for shorter periods of time (i.e., primarily during school hours) [14]. This therefore means that parents are more likely to see symptoms among boys at home and, in turn, are more likely to visit a health professional.
Studies have found a significant association between dyslexia and markers of wellbeing and mental health, such as self-esteem, confidence, anxiety, and self-efficacy [13,15,16]. Individuals with dyslexia often confront challenges beyond reading difficulties, impacting their perception of self-worth and confidence in their abilities [16,17]. The ongoing struggle to navigate academic tasks (such as reading and spelling) can lead to reduced self-esteem and confidence, exacerbating feelings of anxiety and reducing self-efficacy [17]. This complex but under-researched relationship between dyslexia and mental health highlights the importance of interventions that address not only academic needs but also mental health. For example, a scoping review conducted by Wilmot et al. (2023) [18] demonstrated that while factors such as self-esteem are often identified in research studies, research focusing on associations between mental health and these factors in the context of dyslexia were limited. Children often talk about worries, stress and embarrassment in the context of their dyslexic symptoms [19], and some links between dyslexia and poorer mental health in terms of higher rates of anxiety, depressive symptoms, and learned helplessness have been found [9,13,15,19]. However, there is a lack of research which investigates how PPIs can have a direct impact on mental health through the improvement of factors such as self-esteem in dyslexic students.
Positive psychology focuses on improving mental health and wellbeing, including decreasing anxiety, and increasing self-esteem, confidence, and self-efficacy; it offers a lot of potential to help dyslexic students. Research concerning positive psychology explores the understanding and enablement of happiness, wellbeing, and the value of life [20]. In the last 25 years, a variety of positive psychology interventions (PPIs) have been developed and found to decrease anxiety [21] and increase self-esteem [22], self-efficacy [23], and confidence [24]. PPIs comprise a wide range of empirically supported techniques aimed to enhance wellbeing, build resilience, and encourage individuals and communities to flourish [20]. For example, PPIs can include gratitude interventions, such as gratitude letters and keeping a gratitude journal [25]. Additionally, mindfulness meditation interventions have been explored which involve the deliberate focus of attention on the present moment with acceptance, curiosity, and openness [26]. Mindfulness-based interventions aim to cultivate present-moment awareness, alleviate stress, and support emotional regulation (e.g., via meditation and mindful breathing exercises) [27,28]. Furthermore, strength-based interventions centre on recognising and leveraging individual capabilities to overcome obstacles and work towards desirable goals. These interventions focus on recognising and utilising individual strengths to overcome obstacles, establish goals, and improve overall fulfilment [29]. Acts of kindness interventions promote positive moods and provide people with a feeling of purpose by encouraging selfless acts towards oneself and others [30]. Finally, social connection interventions, such as volunteering, improve interpersonal connections to boost social support networks and mental health and general wellbeing [31]. PPIs aim to increase wellbeing and often focus decreasing anxiety, and increasing self-esteem, confidence, and self-efficacy [32,33].
Within positive education, PPIs can be used to improve the mental health of students in schools and universities. For instance, Shoshani (2013) [34] conducted a study to evaluate the efficacy of a PPI aimed at enhancing the mental health of the staff and students at a large middle school in the centre of Israel. Seventh- to ninth-grade students (n = 537) participated in a 1-year intervention programme and were compared to 501 students in a demographically similar control school. Findings revealed the potential benefits of evidence-based PPIs for promoting the mental health of school children and point to the crucial need to make education for wellbeing an integral part of the school curriculum [34]. Furthermore, a recent review conducted by Benoit and Gabola (2021) highlighted the importance of PPIs in fostering various positive aspects of development in young children, including gratitude, positive emotions, life satisfaction, accomplishment, positive relationships, and self-esteem; however, it was recognised that more research was needed into PPIs in education [35].
Why It Is Important to Do This Review
PPIs are effective in supporting individuals in the educational setting [36], and have been found to increase self-esteem, self-efficacy, and confidence and decrease anxiety levels [36,37]. Although there has been an increase in research interest into PPIs involving students with dyslexia, a review has yet to be conducted which synthesises existing research into PPIs in relation to self-esteem, self-efficacy, confidence, and decreasing anxiety for students with dyslexia. The purpose of this review, therefore, is to explore the impacts of PPIs on self-esteem, self-efficacy, confidence, and anxiety levels among students with dyslexia in schools and universities, and to assess whether there are differences between the Eastern and Western countries. Findings from the review will provide a valuable and positive contribution to the fields of both dyslexia and positive psychology. This is important given that existing research primarily emphasises the negative influence of dyslexia on the language development of individuals who are diagnosed with dyslexia [38]. In addition, the review will provide a novel contribution to the broader field of positive psychology where evidence has yet to be synthesised in relation to the effects of PPIs on the mental health of individuals with dyslexia in different educational contexts. The primary research question of the present review is as follows: what are the characteristics and effectiveness of PPI interventions used to improve self-esteem, self-efficacy, and confidence and decrease anxiety in students with dyslexia?
2. Methods
A narrative review approach based on the guidelines by Demiris et al. (2019) [39] was adopted to answer the above review question. A narrative review was chosen to give a comprehensive overview of the existing literature and allow for the identification of key themes, trends, and gaps in the literature. Furthermore, this approach allowed for the inclusion of diverse studies, encompassing qualitative and quantitative research with various methodologies. A narrative synthesis of findings can offer a holistic understanding of the topic, highlighting the strengths and limitations of PPIs in the educational setting.
Keywords were identified using relevant articles in the fields of positive psychology, dyslexia, and wellbeing. A combination of keywords and Boolean phrases were searched, such as “Positive psych* intervention* ‘AND’ dyslexia ‘AND’ self-esteem ‘or’ self-efficacy ‘or’ confidence ‘or’ Anxiety”, and also the combination of gratitude intervention*, forgiveness intervention*, savouring intervention*, building strengths intervention*, meaning oriented intervention*, creativity intervention*, resiliency intervention*, courage intervention*, humour intervention*, engagement and flow intervention*, compassion intervention*, act of kindness intervention*, mindfulness and meditative intervention*, and physical positive psychology intervention* (see Table 1 for inclusion and exclusion criteria). Searches were conducted in eight research databases (CINAHL, Clinical Trials, ProQuest, Web of Science, PsycINFO, EMBASE, Medline, PubMed), in addition to Google Scholar up to 15th December 2023. Additionally, backwards and forwards citation searches were conducted of included studies and existing systematic reviews in relation to PPIs and dyslexia [27,28,32,33,35,36].

Table 1.
Inclusion and exclusion criteria.
The first round of screening was completed by two reviewers independently who read the titles and abstracts of the articles identified by the search strategy. Subsequently, an additional selection of articles was made by analysing the full text of the selected articles. Evaluations of article inclusions were performed separately by each reviewer. Any disagreements were solved through discussion with a third reviewer. The data from included studies were then extracted into a spreadsheet by two reviewers. Data extraction involved identifying and summarising key elements across the selected articles, comprising the study designs, participant demographics, interventions, and outcomes. In order to analyse the narratives, a thematic analysis (TA) was conducted, focusing on identifying recurrent themes and patterns within the data. TA is a flexible approach “searching across a data set—be that a number of interviews or focus groups, or a range of texts—to find repeated patterns of meaning” [40]. The key themes were identified both through the of prevalence of the themes within the text and based on the research question [40]. This approach facilitated the organisation of disparate findings into coherent narratives, allowing for a comprehensive understanding of the research topic.
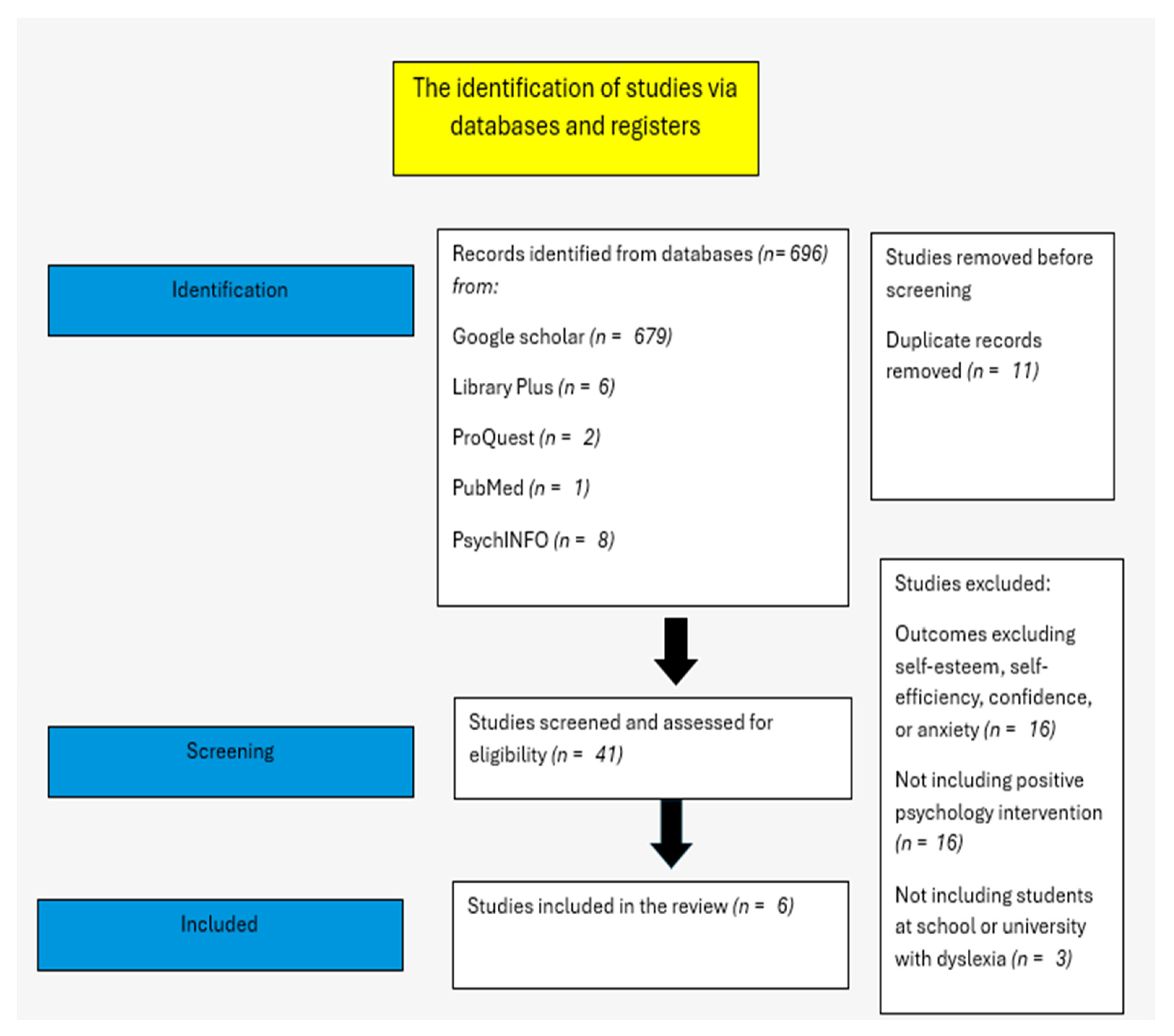
Our search using the above search terms across the databases and the grey literature yielded a total of 696 records and, after removing duplicates and irrelevant studies, we assessed 41 papers for inclusion (see Figure 1. PRISMA Flowchart). There are some studies which were excluded from this review (e.g., Daigle et al., 2022) [41] due to not including outcome measures in line with the current review criteria and lacking details about the nature of the PPIs (see Figure 1. PRISMA Flowchart).
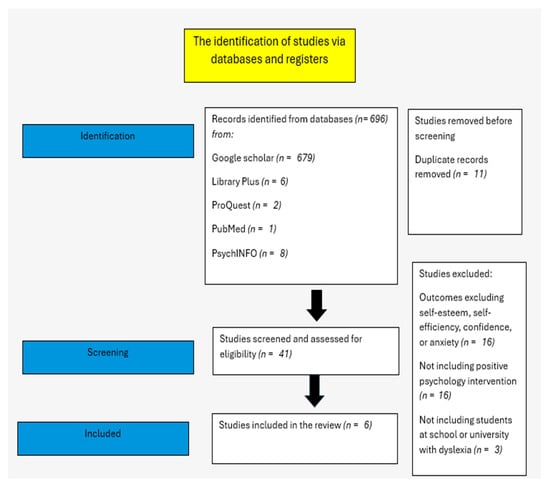
Figure 1.
PRISMA Flowchart. PRISMA flow diagram describing the different phases of this review.
Following the inspection of titles and abstracts for inclusion, we retrieved 41 full texts. Of those, 38 papers did not meet the criteria, but six studies (Bull, 2007 [42]; Burton, 2004 [43]; Boyes et al., 2021 [44]; Firth et al., 2013 [45]; Tarrasch et al., 2016 [46]; Upadhyay, 2021 [47]) were included in the final analysis (see Table 2 for study characteristics).
Table 2.
Included studies. Characteristics of studies included in the review (n = 6).
3. Results
The six studies that met the inclusion criteria were analysed. Using narrative synthesis, we identified the key characteristics of the included studies. There are four themes: (i) the characteristics and effectiveness of PPIs, (ii) the level of education, (iii) gender differences and PPIs, and (iv) PPIs in the West and East.
3.1. Characteristics and Effectiveness of PPIs
A variety of different PPIs in the educational setting have been found to be effective [48]. Although PPIs for supporting dyslexic students’ mental health are limited, this review identified six articles on the topic. Upadhyay’s (2021) [47] aim was to evaluate the effects of PPI on school-age (ages 8 to 12) children with SLDs in terms of their academic performance (AP), academic self-concept (ASC), and subjective wellbeing (SWB). In total, 75 students from three schools in Telangana State, India, took part in exercises in attributional style, mindfulness, and gratitude once a week, over four months. The findings showed that SWB, ASC, and AP had significantly improved after the intervention and that these benefits had persisted at the 6-month follow-up. According to the study, PPIs can improve academic achievement, happiness, and self-concept in children with SLD (e.g., dyslexia). The findings also suggested that the intervention may have wider uses in fostering positive feelings and resolving issues in children with a range of needs, as well as empowering parents and educators (e.g., Paul and Halt, 2017) [49].
Burton (2007) [43] conducted a group intervention for dyslexic children in a specialised programme within a standard secondary school; two groups composed of five boys each from Year 8 and 9 took part in various activities over six weeks, observed by educational psychologists and teachers. The aim of the intervention was to enhance self-esteem through structured self-esteem groups. Activities within the groups were adapted from existing materials and highlighted various aspects of self-esteemimprovement, such as recognizing positive attributes, reframing disappointments, managing interpersonal interactions, and giving and receiving positive recognition. Educational psychologists and teachers facilitated the groups, providing observation and modelling of facilitation skills. Qualitative interviews found that participants emphasised the value of working with peers who face similar issues. Teachers saw several beneficial results and advocated for routine integration of these groups into the school’s psychology services. Furthermore, the results showed that during the six-week programme, participants’ levels of self-esteem increased.
Boyes et al.’s (2021) [44] study examined the feasibility, efficacy, and acceptability of the ‘Clever Kids’ programme, designed to enhance socioemotional wellbeing; targeting skills and strategies to help children cope with dyslexia, regulate their emotions, build resilience, and improve self-esteem. The PPI was conducted in a primary school with 40 children with dyslexia (mean age = 10.35 years). In this randomised controlled trial, participating children attended either the Clever Kids programme or were assigned to a waiting list control group. The intervention aimed to foster acceptance of dyslexia and address associated difficulties through coping strategies, emotion regulation, resilience, and self-esteem enhancement. While the study did not find significant effects on coping, emotion regulation, resilience, or self-esteem overall, children in the intervention group reported a temporary increase in self-esteem post-programme. However, this effect was not sustained at the three-month follow-up.
Bull (2007) [42] investigated the clinical and perceived effectiveness of sunflower therapy—a combination of homoeopathy, herbal remedies, massage, physical manipulation, applied kinesiology, and neuro-linguistic programming in supporting the psychological wellbeing of dyslexic children. In a randomised controlled trial, seventy dyslexic children, ranging in age from six to thirteen, underwent assessments of their literacy, cognitive function, and self-worth prior to and following the intervention. The intervention consisted of eight appointments each lasting 40 min. The results showed no significant improvements in the treatment group’s cognition or literacy test scores, but there was a notable improvement in their reading and academic self-esteem. Most parents believed that sunflower therapy was effective; however, additional research is needed to explore these suggested benefits further.
As part of a larger dyslexia-related professional development initiative, the study by Firth et al. (2013) [45] introduced the “Success and Dyslexia” coping curriculum at two primary schools. The study aimed to investigate the impact of an intervention programme on coping strategies, perceived control, and wellbeing in students with dyslexia compared to those without dyslexia. The intervention was a comprehensive approach aimed at supporting year 6 students, including those with dyslexia, in developing coping strategies and promoting mental health within the school setting. It involved two main components: whole-school dyslexia professional development and change, and a universal classroom coping programme. The professional development programme provided all school staff with essential knowledge about dyslexia and facilitated the development of a dyslexia support action plan. Simultaneously, a 10-session coping programme, grounded in cognitive behavioural therapy principles, was delivered to all year 6 students, incorporating activities to enhance coping skills, positive thinking, assertion, and goal setting. The structured implementation of the programme included reinforcement activities to engage students and ensure effective learning. By integrating dyslexia support strategies into classroom activities and addressing the needs of all students, the intervention aimed to foster an inclusive and supportive school environment while promoting mental health and wellbeing throughout the school community. To evaluate effectiveness, twenty-three dyslexic sixth graders were surveyed prior to, during, and one year after the programme. The results demonstrated that dyslexic students had shown positive changes in coping strategies and locus of control, and that these changes had continued at follow-up. Furthermore, the results showed that at the 7-year follow-up, children with dyslexia reported similar perceived control and coping levels to their non-dyslexic peers. Additionally, the results showed higher wellbeing compared to students with dyslexia who did not receive the intervention.
In 2016, Tarrasch, Berman, and Friedman [46] examined the effects of a mindfulness-based stress reduction (MBSR) intervention on reading, attention, and psychological wellbeing in students with developmental dyslexia and/or attention issues. The MBSR workshop, which was developed by Kabat-Zinn (2003) [50], was a structured group programme aimed at reducing stress and promoting wellbeing. Participants attended eight weekly 2.5 h classes, including a half-day retreat during the sixth week, where they received training in mindfulness techniques. These techniques included body scan meditation, sitting meditation, mindful stretching exercises, and mindful eating. Participants were instructed to practice mindfulness for 45 min per day using provided CDs and MP3 files. The workshop, led by a trained clinical psychologist, emphasised integrating mindfulness into everyday life and responding more creatively to stressful situations. Prior to and following a two-month mindfulness training programme, the participants completed assessments of their attentiveness and reading comprehension. The results showed that following the sessions there were fewer reading errors overall, particularly those using the sub-lexical pathway. In addition, reduced impulsivity was correlated with fewer reading errors and better maintained attention. Moreover, the MBSR intervention enhanced mindfulness, showed stress reduction, decreased depression, anxiety, rumination, and improved sleep quality. MBSR did not directly target any one type of dyslexia, but it did help participants stay on the lexical route, which made reading easier. This demonstrates the link to enhanced reading. These results show a connection between improved reading through mindfulness and less impulsivity and better concentration.
3.2. Level of Education
The mental health of students with dyslexia can be affected at any level of education [51]. Levels of education vary significantly across different countries in the world as there are different frameworks for grades across different countries in the world (the school education comparison is shown in Table 3). The six studies used PPIs that were designed to target a range of educational levels within the educational system, with five out of the six included studies based within a school setting. The studies showed a disparity in education levels. For example, ‘The Clever Kids Wellbeing’ programme was designed for dyslexic children in upper primary school. It focused on improving coping mechanisms and self-worth over the course of 12 weeks through support groups and group activities [44]. Boyes et al. (2020) [44] conducted their study with children with a dyslexia diagnosis in their final years of primary school (Year 5 = 17; Year 6 = 23) and were encouraged to participate in a carefully structured literacy intervention. Burton (2004) conducted their research across two years of primary school (Year 5 = 17; Year 6 = 23). The “Success and Dyslexia” coping programme supported dyslexic primary school pupils during the crucial transition to high school by focusing on the development of better coping mechanisms [45]. Firth et al. (2013) [45] conducted their study with one hundred and two year 6 students with dyslexia in two primary schools to measure the effectiveness of the dyslexia intervention after their transition to secondary school, focusing on two levels of education, these being primary and secondary. Bull (2007) [42] conducted their study with dyslexic children in primary school children aged from 6 to 13 years old. Upadhyay (2021) [47] selected two CBSE schools (Central Board of Secondary Education) and one State Board school from the twin cities of Secunderabad and Hyderabad in Telangana state, India. The children were aged between 8 and 12 years of age, from Classes 3 to 7, with five pupils selected from Year 8 and five from Year 9. Additionally, one PPI was implemented within the university setting, Tarrasch, Berman, and Friedman (2016) [46] conducted their study with 17 participants who had been diagnosed with dyslexia. Throughout the six studies, the varied educational backgrounds demonstrated the applicability of PPIs to a range of educational levels. By addressing the specific needs of dyslexic students during school and university, PPIs can play a vital role in fostering resilience and promoting social integration.
Table 3.
Grade levels and age across countries.
3.3. Gender Differences and PPIs
With regard to gender, it has been argued that the numbers of boys who are identified with dyslexia is higher than the number of girls [52]. This is also the case across the six studies identified in this review, where more boys with dyslexia were identified and included in the PPI studies than girls, regardless of whether the study was conducted in an Eastern or Western country. For example, Upadhyay (2021) [47] conducted a study with 61 boys and 14 girls diagnosed with dyslexia. The findings showed a significant increase in the levels of subjective wellbeing, academic self-concept, and academic achievement of children with dyslexia after PPI. Burton (2004) [43] conducted their study with 10 boys with dyslexia (five from Year 8 and five from Year 9) because most pupils attending the resourced provision were male. Tarrasch et al. (2016) [46] conducted their study with 10 females and 16 males with dyslexia. Boyes et al. (2020) conducted their study with 26 males and 14 females with dyslexia. Bull (2007) [42] conducted their study on a sample size of 70 children, containing more males than females (M = 42, F = 28). Firth et al. (2013) [45] conducted their study with a sample where 46 students were males, and 56 were females with dyslexia.
The six included studies were reviewed to examine the gender split within the interventions. None of the studies explored the gender differences within the studies. For example, Firth et al. (2013) [45] did not confirm any difference related to gender regarding the quality of coping strategies by females in comparison with males. It was not clear from Firth’s study if females with dyslexia faced challenges related to adopting effective coping strategies and whether they responded more effectively to the PPI programme adopted in the study than males. In addition, Upadhyay (2021) [47] did not demonstrate a clear association between gender and the response of children with dyslexia to their PPI intervention. Given that gender-related factors, such as coping mechanisms, self-esteem, and social support systems, may affect how male and female dyslexic students respond to interventions [52], perceived social support, coping capability, and gender differences among young adults in the classroom could be an interesting area for future research on the effects of positive psychology interventions with dyslexic students. It is critical to consider any gender-specific obstacles, including confidence issues or academic self-concept, while constructing PPIs, in addition to the relationship between gender and social class. For example, therapies that emphasise resilience and self-compassion may be especially helpful for female students, but activities that encourage goal setting and assertiveness may be more useful for male students [53]. Incorporating group-based interventions that promote social ties and peer support may also be beneficial to both genders, improving academic achievement and general wellbeing. Schools and institutions can develop more inclusive and successful treatments suited to the various requirements of dyslexic students by recognising and addressing gender variations in PPIs. However, this may change if these males lack the necessary resources because of their social class (i.e., working class males may not have access to these types of interventions) [54,55,56].
3.4. PPIs in the West and East
The use of PPIs in schools and universities, particularly for dyslexic students, is increasingly recognized in Western countries. Indeed, the majority of the included studies were conducted in Western countries (e.g., England (n = 2) and Australia (n = 2)). These interventions cover various areas such as resilience, coping, and mindfulness, targeting aspects like self-esteem. However, research on their effectiveness is limited. For instance, the intervention by Boyes et al. (2021) [44] investigated resilience and coping intervention in Australia and the findings showed increases in self-esteem among students with dyslexia, though Boyes’ ‘Clever Kids’ intervention had no significant effect on self-esteem levels. In contrast, PPIs are less common in Eastern countries such as India [47] and Israel [46], with mindfulness interventions being the primary focus. Research in Israel [46] indicated the effectiveness of cognitive therapy based on mindfulness training in reducing social anxiety and increasing self-esteem among students with dyslexia. Similarly, a mindfulness workshop in Israel showed reductions in reported stress but not anxiety levels among university students with dyslexia. In India, a combination of PPIs, including gratitude and optimistic thinking, led to a significant increase in academic confidence among dyslexic school students. However, there is a lack of studies examining dyslexia’s impact on mental health in Western and Eastern countries.
4. Discussion
This narrative review aimed to explore the characteristics and effectiveness of PPIs in improving self-esteem, self-efficacy, and confidence and decreasing anxiety in dyslexic students. Following a search of nine databases, six studies met the inclusion criteria. The included studies all explored different PPIs; however, they all targeted individuals with dyslexia across various age groups and educational settings. For instance, the results showed that group interventions in secondary schools, as highlighted by the Burton (2004) [43] study, were effective in strengthening self-esteem and social skills among dyslexic pupils. Bull [42] emphasised the potential psychological benefits of sunflower therapy for dyslexic children, despite inconclusive findings on academic performance. Meanwhile, Boyes et al. (2021) [44] study suggests the need for further research on socioemotional wellbeing programmes like Clever Kids, which demonstrated short-term improvements in self-esteem post-programme. In university students, mindfulness meditation, as shown by Tarrasch et al. (2016) [46], showed promising results in enhancing reading accuracy and attention functions. Additionally, positive psychology group interventions, as shown by Upadhyay (2021) [47], were effective in improving subjective wellbeing, academic self-concept, and achievement among dyslexic children. Lastly, Firth et al. (2013) [45] highlighted the importance of early interventions in supporting coping strategies, perceived control, and overall wellbeing among students with dyslexia. Collectively, the findings showed promising outcomes for reducing stress, improving self-esteem, and enhancing overall wellbeing. This highlights the potential benefits of diverse PPIs in improving mental health outcomes for individuals with dyslexia, emphasising the significance of early intervention and targeted support across different educational settings.
The findings of the review were synthesised under four main themes. First, the nature of the different PPIs highlighted the diversity of interventions conducted among the included studies. For instance, Upadhyay (2021) [47] implemented a programme focusing on gratitude, mindfulness, and optimistic thinking for children with specific learning disabilities (SLDs), Burton (2007) [43] conducted a group intervention targeting self-esteem enhancement among dyslexic secondary school students, Boyes et al. (2021) [44] investigated the ‘Clever Kids’ programme’s feasibility, efficacy, and acceptability in primary school children with dyslexia, Bull (2007) [42] explored the effectiveness of sunflower therapy in enhancing the psychological wellbeing of dyslexic children, Firth et al. (2013) [45] introduced the “Success and Dyslexia” coping curriculum and lastly, Tarrasch et al. (2016) [46] examined the effects of mindfulness-based stress reduction (MBSR) on reading, attention and psychological wellbeing in students with dyslexia. These studies collectively illustrate the varied approaches to PPIs for students with dyslexia across different educational settings. Moreover, the diverse range of PPIs outlined in the studies emphasises the multifaceted approaches aimed at supporting the mental wellbeing and academic success of students with dyslexia across various educational settings. Future research could explore the mechanisms underlying the observed improvements and to develop tailored interventions that address the specific needs and challenges faced by dyslexic students at different stages of their education. By advancing our understanding of effective PPIs, researchers can better support the various needs of students with dyslexia and promote their overall wellbeing and academic success.
Additionally, the theme related to educational level highlights the range of ages the PPIs were aimed towards. The mental health of students with dyslexia can be impacted at any educational level, with studies indicating a focus on interventions primarily within a primary school setting. For instance, the “Clever Kids Wellbeing” programme targeted dyslexic children in upper primary school, while the “Success and Dyslexia” coping programme assisted primary school pupils. Other studies, such as those by Burton (2004) [43], Bull (2007) [42], and Upadhyay (2021) [47], focused on dyslexic children in primary schools, while Tarrasch et al. (2016) [46] implemented a programme within a university setting. These interventions highlight the applicability of psychosocial interventions across various educational levels, aiding in resilience-building and social integration among students with dyslexia. However, the majority of the interventions focused on primary school settings, highlighting a potential gap in the evidence base, suggesting that further research into interventions for dyslexic students at the university level could be beneficial. Expanding the focus of interventions to include higher education settings may help address the unique challenges faced by dyslexic students in this context and contribute to their overall wellbeing. Therefore, targeting university contexts with future research could indeed be a valuable area of exploration.
The theme exploring gender differences revealed that the majority of participants across the reviewed studies were males, which is in line with previously suggested gender-based prevalence rates [57]. However, despite differences in diagnostic prevalence and presentation of symptoms [9], none of the reviewed studies explored gender differences in terms of the effectiveness or impact of incorporating PPIs. It remains unclear whether female dyslexic students face unique challenges or respond differently to PPIs compared to males. Considering gender-specific factors such as coping mechanisms, perceived self-esteem, and social support systems, it is crucial to explore this further when designing PPIs for dyslexic students. Additionally, it is important to investigate the connection between gender and dyslexia interventions to tailor interventions effectively, considering potential obstacles such as confidence issues or academic self-concept, especially for female students. For example, therapies that emphasise resilience and self-compassion may be especially helpful for female students, but activities that encourage goal setting and assertiveness may be more useful for male students [53,54]. Incorporating group-based interventions that promote social ties and peer support may also be beneficial to both genders, improving academic achievement and general wellbeing. Ultimately, acknowledging and addressing gender differences in PPIs can lead to more person-centred, holistic, and inclusive interventions for students with dyslexia, ensuring that they meet the diverse needs of all individuals affected by dyslexia.
The final theme focused on the country in which the PPI was implemented (i.e., Western or Eastern countries). PPIs have been investigated worldwide; however, a systematic review by Hendriks et al. (2019) [58] found that 78.2% of PPI studies are from Western countries. Although, since 2014, there has been a rise in the number of publications from Eastern countries, indicating a movement towards the globalisation of PPIs. Positive psychology interventions (PPIs) are gaining recognition in Western countries, with studies conducted in England and Australia focusing on students with dyslexia. These interventions, such as those by Bull (2007) [42], Burton (2004) [43], Boyes et al. (2021) [44], and Firth et al. (2013) [45], address resilience, coping, and mindfulness to improve self-esteem. However, research on their effectiveness remains limited. For example, Boyes et al. (2021) [44] found increased self-esteem among dyslexic students in Australia, but the “Clever Kids” intervention had no significant effect on self-esteem levels.
In contrast, PPIs are less prevalent in Eastern countries such as India [47] and Israel [46], where mindfulness interventions are prominent. Research conducted in Israel [46] suggests that cognitive therapy based on mindfulness training can reduce social anxiety and boost self-esteem among dyslexic students. In India [47], a combination of PPIs enhanced academic confidence among dyslexic school students. However, while components of wellbeing such as self-esteem, self-efficacy, confidence, and anxiety have been studied in the past, there is a lack of comprehensive studies examining the impact of dyslexia on general mental health in both Western and Eastern countries, highlighting the need for further research in this area. Nevertheless, it is important to acknowledge that some non-Westernised countries may not have the resources, or strategies in place to effectively teach students with dyslexia in the first place. For example, a recent study evaluating the awareness and support available to students with dyslexia in South Africa has demonstrated that teachers struggle to implement strategies that provide screening, identification, and support strategies for dyslexia [59]. While understanding and acceptance appear to be higher in Western countries, it is clear there is still room for improvement, particularly regarding the underlying mechanisms of dyslexia [60] and ongoing issues with underdiagnosis [61]. Therefore, in addition to improving teachers’ overall understanding of dyslexia, teacher training would benefit from highlighting the compounding impact of negative emotions and individual differences in confidence and self-esteem identified in this review, as well as strategies to reduce these.
PPIs have gained increasing attention and application in educational settings, including schools and universities [34], aiming to promote students’ wellbeing, resilience, and academic success [35,36]. These interventions not only enhance students’ mental health but also contribute to a positive school climate and academic engagement [37]. In order to assist students in overcoming academic hurdles and changes, universities frequently offer resilience training, wellbeing workshops, and strengths-based interventions [62]. PPIs can take on different manifestations in different cultures [63], and these differences may reflect subtle Western and Eastern cultural educational differences and the philosophical foundations of each tradition. PPIs in Western universities and schools frequently highlight personal accomplishment, resiliency, and individual characteristics through interventions including goal-setting activities, gratitude journals, and cognitive behavioural methods. These interventions aim to enhance students’ self-esteem, motivation, and academic performance [58]. On the other hand, Eastern educational institutions incorporate PPIs that are based on interpersonal harmony and holistic wellbeing. These practices are derived from Confucian principles, mindfulness meditation, and compassion practices. Eastern PPIs promote the formation of moral character, social ties, empathy, and emotional equilibrium in students by emphasising collectivism [64]. Ultimately, both Western and Eastern PPIs aim to develop flourishing individuals within educational communities by addressing multiple aspects of resilience and wellbeing, even though their methods differ.
PPIs can be implemented at both the individual and collective levels, addressing the wellbeing of individuals or groups within communities [65]. Individual PPIs focus on the personalised approach and are tailored to the specific needs, strengths, and preferences of each participant, focusing on enhancing personal wellbeing and resilience. Examples of individual PPIs include keeping a gratitude journal, practising mindfulness exercises, engaging in acts of kindness towards oneself, or participating in strengths-based coaching sessions. Collective PPIs focus on the community-based approach, promoting wellbeing and resilience within groups, communities, or organisations, and emphasising shared values, social connections, and collaborative efforts. Examples of collective PPIs include group-based gratitude circles, peer support groups, and community-wide initiatives to promote kindness and compassion. In the reviewed studies, several interventions were conducted either in a group setting or on an individual basis. Group interventions included [43] a six-week self-esteem enhancement programme for dyslexic secondary school pupils, Firth et al.’s 2013 [45] “Success and Dyslexia” coping curriculum implemented in primary schools, and Boyes et al.’s 2021 [44] “Clever Kids” programme targeting socioemotional wellbeing in primary school children with dyslexia. On the other hand, individual interventions comprised Upadhyay’s 2021 [47] PPI focusing on gratitude, mindfulness, and optimistic thinking for school-age children with specific learning disabilities (SLDs), Bull’s [42] (2007) investigation of sunflower therapy for dyslexic children, and Tarrasch et al.’s (2016) [46] examination of Mindfulness-Based Stress Reduction (MBSR) in students with dyslexia and/or attention issues. These distinctions in intervention format are fundamental to understanding their implementation and potential effectiveness in addressing the needs of dyslexic students. Both individual and collective PPIs play important roles in promoting wellbeing; a combination of both individual and collective interventions may increase the effectiveness of these studies to enhance the quality of life for individuals with dyslexia in different educational contexts. However, there is an insufficient number of studies that use a combination of individual and collective PPIs designed to improve quality of life, and future research may be able to explore this (e.g., Novita, 2016 [66]).
The length of the PPIs can vary widely depending on the specific intervention and its intended goals, as well as individual preferences and needs. Some interventions may be brief and simple, lasting only a few minutes each day, while others may involve more extensive and structured activities conducted over weeks or even months [67]. For example, gratitude journaling or mindfulness exercises can be practised daily for just a few minutes at a time, making them relatively short-term interventions. On the other hand, interventions like strengths-based coaching or goal-setting workshops may involve multiple sessions spread out over several weeks or months to facilitate deeper exploration and sustained behavioural change [58,67]. The duration of PPIs may also be influenced by factors such as the severity of the issue being addressed, the availability of resources and support, and the individual’s level of engagement and commitment. Generally, PPI efficacy is correlated with the consistency and length of its practice; longer-term interventions tend to produce more long-lasting advantages in terms of wellbeing and personal development [68]. The selected articles that used PPIs to focus on dyslexic students showed different lengths, such as the intervention lasting the whole school year [45], 12 weeks [47], 6 days [43], 9 weeks [44], eight appointments which were 40 min long [42], and [46] an eight-week course of 2.5 h classes, including a half-day retreat during the sixth week. Furthermore, some of the interventions had follow-up measures to investigate the longer effectiveness of the interventions, such as the Clever Kids program [44] with a follow-up conducted three months after the intervention, and the “Success and Dyslexia” programme, which explored the effectiveness one year later [45]. This variety in intervention length allows for the examination of both immediate and longer-term impacts on students with dyslexia. Four of the included studies may have benefited from investigating the longer-term effects of PPIs, as without a follow up it is not clear if the advantages of PPIs would eventually diminish if continual reinforcement was not practised. Moreover, the follow-up data allow the investigation of longer-term effectiveness.
Overall, this review has highlighted the potentially beneficial role of PPIs for indices of dyslexic students’ wellbeing beyond the known benefits regarding their reading comprehension and writing skills. From the reviewed literature, if PPIs tackle negative emotions such as anxiety, low self-confidence, self-esteem, and self-efficacy, improvements in their school performance are likely to follow [63]. Previous research has shown a clear link between dyslexia and self-esteem, self-efficacy, confidence, and anxiety [64]. Indeed, these negative emotions may influence dyslexic students’ self-perception and belief in their ability to succeed in school. The findings from the included PPIs showed promising results for supporting students with dyslexia.
The studies included in this narrative review had many strengths; for instance, all have showcased real-world application. Burton’s study addresses the significant issue of self-esteem in dyslexic pupils through a practical intervention, and despite many of the studies having a small sample size, Burton’s study showed positive initial results, indicating observable increases in self-esteem scores and the potential effectiveness of the intervention. However, reliance on subjective parental reports diminishes the study’s ability to provide comprehensive insights into the therapy’s effectiveness. Addressing these weaknesses in future research endeavours could further enhance our understanding of sunflower therapy’s utility in managing dyslexia. Furthermore, two of the studies included more than one diagnosis: 53% of the participants had more than one diagnosis [47], while in another, 47% had co-morbid ADHD [46]. In the absence of sub-group analyses focusing purely on those with dyslexia, it is difficult to ascertain whether the effects or lack of effects found are unique to students with dyslexia. Future research is now needed to disentangle the beneficial effects of PPIs specifically for this population in order to develop tailored PPIs. Additionally, many of the studies highlighted the importance of considering literacy support alongside interventions and Boyes’ study suggests future research to explore the combination of both for optimal outcomes. Burton’s [43] study identifies areas for further research, emphasizing the need for larger-scale quantitative evaluation and suggesting avenues for enhancing the robustness of the findings. In the studies reviewed, some of the studies included control groups. For example, Firth’s and Boyes’ studies utilised a randomised controlled trial with a waiting list control condition, enabling a comparison of outcomes between intervention and control groups. In contrast, Upadhyay’s [47] study employed a one-group pre-test post-test design without a control group. Bull, Tarrasch, and Burton’s studies did not involve a control group, instead evaluating the intervention’s impact within the group of participants who received it. However, control groups play a crucial role in research by providing a basis for comparison, enhancing the validity of study findings, and allowing for more reliable conclusions about intervention efficacy [69]. Furthermore, in the studies discussed, there are instances where selection bias could potentially affect the validity of the findings due to a non-random selection of participants. For example, in the Firth et al. (2013) [45] study, participants were not randomly selected, but rather volunteered to participate, potentially leading to a sample that may not be representative of the broader population. Similarly, in the Bull (2007) [42] study, participants were recruited through various methods such as the national and regional press, potentially leading to a sample that may not be fully representative of the population of dyslexic students. Non-random selection of participants can introduce bias, as those who volunteer or are recruited may differ systematically from those who do not, affecting the generalisability of the findings. Randomized controlled trials, such as the Boyes et al. (2006) [44] study, help mitigate selection bias by randomly assigning participants to intervention and control groups, thereby increasing the likelihood of a representative sample and enhancing the validity of the study findings. In several of the studies discussed, outcomes were assessed using self-report measures, which can potentially introduce response bias or social desirability bias. For instance, in Upadhyay’s [47] study, subjective wellbeing, academic self-concept, and academic achievement were measured using self-reported scales. Similarly, the Burton [43] study evaluated self-esteem using a self-rating questionnaire. Students may feel pressure to present themselves in a positive light or may misrepresent their experiences to align with perceived societal norms or expectations. Additionally, response bias may have occurred when participants provided responses as they may have desired to please the researcher.
4.1. Limitations
Given the relatively small body of research into PPIs and dyslexia, a narrative review approach was deemed to be the most appropriate. However, despite thoroughly documenting the search and screening strategy, it is acknowledged that the current review is limited by the non-systematic approach and lack of quality appraisal. In addition, the inclusion only of studies written in English is problematic, as there may have been an underestimation of PPIs conducted with people with dyslexia, particularly in non-Western countries.
4.2. Future Research and Directions
To move the field forward, future research could explore several avenues to further enhance our understanding and improve outcomes for students with dyslexia. Long-term follow-up studies could assess the durability of intervention effects over time, shedding light on any continuous improvements in academic performance, self-esteem, and wellbeing among students with dyslexia. Comparative effectiveness research could help identify the most effective intervention approaches, such as cognitive behavioural therapy, mindfulness-based interventions, and educational interventions, to inform evidence-based practices. Furthermore, personalised interventions tailored to the individual needs of dyslexic learners could utilise advances in technology and personalised learning approaches to target specific cognitive, linguistic, and educational needs. Exploring inclusive education practices, family and community support, and culturally approachable interventions could further enhance the interventions’ effectiveness by promoting academic and social inclusion, providing social and emotional support, and addressing diverse cultural backgrounds.
All of the included studies were face-to-face interventions; as an alternative, online methods could be considered, as they are convenient, accessible, and scalable, meeting a range of requirements and preferences. They offer anonymity and self-paced activities, making them appropriate for people who are uncomfortable with face-to-face encounters even while they lack the individualised support and direct human connection of in-person sessions. By focusing on these research areas, future studies can contribute to the development of more effective, personalised, and inclusive interventions for individuals with dyslexia, ultimately improving their academic success, psychosocial wellbeing, and quality of life.
5. Conclusions
The aim of this narrative review was to synthesise the evidence base concerning PPIs and several wellbeing markers for students with dyslexia. Four key themes were identified; characteristics and effectiveness of PPIs, the level of education, gender differences, and differences between Western and Eastern countries. Overall, PPIs seem to be useful in improving self-esteem, self-efficacy, and confidence, while decreasing anxiety in students with dyslexia, though the conclusions should be considered with caution due to the limited research available. The potential positive implications of incorporating PPIs into curricula should be investigated further, focusing on short-term and long-term impacts and the feasibility of implementation of regular PPIs into educational systems, as well as enabling teachers, particularly in the Eastern countries, to implement strategies to support students with dyslexia.
Author Contributions
Conceptualization: D.A.O. and A.K.; Methodology: I.B. and C.S.; Validation: A.K., C.S. and D.A.O.; Formal analysis: D.A.O. and A.K., C.S.; Investigation: A.K.; Resources: A.K., D.A.O., C.S. and Y.I.; Data curation: A.K.; Writing Original draft preparation: A.K., D.A.O., C.S., I.B. and Y.I.; Writing: D.A.O., A.K., C.S., I.B. and Y.I.; Review and editing: A.K., D.A.O., C.S., Y.I. and I.B.; Visualization: A.K.; Supervision: A.K. and D.A.O.; project administration: A.K. and D.A.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wagner, R.K.; Zirps, F.A.; Edwards, A.A.; Wood, S.G.; Joyner, R.E.; Becker, B.J.; Liu, G.; Beal, B. The Prevalence of Dyslexia: A New Approach to Its Estimation. J. Learn. Disabil. 2020, 53, 354–365. [Google Scholar] [CrossRef]
- Berninger, V.W.; Abbott, R.D. differences between children with dyslexia who are and are not gifted in verbal reasoning. Gift. Child Q. 2013, 57, 223–233. [Google Scholar] [CrossRef]
- Fraser, J.; Goswami, U.; Conti-Ramsden, G. Dyslexia and specific language impairment: The role of phonology and auditory processing. Sci. Stud. Read. 2010, 14, 8–29. [Google Scholar] [CrossRef]
- Fostick, L.; Bar-El, S.; Ram-Tsur, R. Auditory Temporal Processing and Working Memory: Two Independent Deficits for Dyslexia. J. Psychol. Res. 2012, 2, 308–318. [Google Scholar] [CrossRef]
- Marshall, C.M.; Snowling, M.J.; Bailey, P.J. Rapid auditory processing and phonological ability in normal readers and readers with dyslexia. J. Speech Lang. Hear. Res. 2001, 44, 925–940. [Google Scholar] [CrossRef]
- Di Folco, C.; Guez, A.; Peyre, H.; Ramus, F. Epidemiology of developmental dyslexia: A comparison of DSM-5 and ICD-11 criteria. medRxiv 2020. [Google Scholar] [CrossRef]
- Francés, L.; Quintero, J.; Fernández, A.; Ruiz, A.; Caules, J.; Fillon, G.; Hervás, A.; Soler, C.V. Current state of knowledge on the prev-alence of neurodevelopmental disorders in childhood according to the DSM-5: A systematic review in accordance with the PRISMA criteria. Child Adolesc. Psychiatry Ment. Health 2022, 16, 27. [Google Scholar] [CrossRef]
- Catts, H.W.; Terry, N.P.; Lonigan, C.J.; Compton, D.L.; Wagner, R.K.; Steacy, L.M.; Farquharson, K.; Petscher, Y. Revisiting the definition of dyslexia. Ann. Dyslexia 2024, 1–21. [Google Scholar] [CrossRef]
- Yang, L.; Li, C.; Li, X.; Zhai, M.; An, Q.; Zhang, Y.; Zhao, J.; Weng, X. Prevalence of developmental dyslexia in primary school children: A systematic review and meta-analysis. Brain Sci. 2022, 12, 240. [Google Scholar] [CrossRef]
- Mather, N.; White, J.; Youman, M. Dyslexia around the World: A Snapshot. Learn. Disabil. Multidiscip. J. 2020, 25, 1–17. [Google Scholar] [CrossRef]
- Maunsell, M. Dyslexia in a global context: A cross-linguistic, cross-cultural perspective. Lat. Am. J. Content Lang. Integr. Learn. 2020, 13, 92–113. [Google Scholar] [CrossRef]
- Marinelli, C.V.; Romani, C.; Burani, C.; McGowan, V.A.; Zoccolotti, P. Costs and benefits of orthographic inconsistency in reading: Evidence from a cross-linguistic comparison. PLoS ONE 2016, 11, e0157457. [Google Scholar] [CrossRef]
- Wilmot, A.; Pizzey, H.; Leitão, S.; Hasking, P.; Boyes, M. Growing up with dyslexia: Child and parent perspectives on school struggles, self-esteem, and mental health. Dyslexia 2023, 29, 40–54. [Google Scholar] [CrossRef]
- Parhiala, P.; Torppa, M.; Eklund, K.; Aro, T.; Poikkeus, A.; Heikkilä, R.; Ahonen, T. Psychosocial functioning of children with and without dyslexia: A follow-up study from ages four to nine. Dyslexia 2015, 21, 197–211. [Google Scholar] [CrossRef]
- De Lima, R.F.; Salgado-Azoni, C.A.; Dell’Agli, B.A.; Baptista, M.N.; Ciasca, S.M. Behavior problems and depressive symptoms in de-velopmental dyslexia: Risk assessment in Brazilian students. Clin. Neuropsychiatry 2020, 17, 141. [Google Scholar]
- Gibby-Leversuch, R.; Hartwell, B.K.; Wright, S. Dyslexia, literacy difficulties and the self-perceptions of children and young people: A systematic review. Curr. Psychol. 2019, 40, 5595–5612. [Google Scholar] [CrossRef]
- Wakelin, G. How Pupils, with a Specific Learning Difference, Verbalise Their Academic Self-Image and Feelings of Self-Esteem. Available online: https://graciemay.co.uk/wordpress/wp-content/uploads/2020/12/How-pupils-with-a-specific-learning-difference-verbalise-their-academic-self-image-and-feelings-of-self-esteem.pdf (accessed on 2 March 2023).
- Wilmot, A.; Hasking, P.; Leitão, S.; Hill, E.; Boyes, M. Understanding mental health in developmental dyslexia: A scoping review. Int. J. Environ. Res. Public Health 2023, 20, 1653. [Google Scholar] [CrossRef]
- Ihbour, S.; Anarghou, H.; Boulhana, A.; Najimi, M.; Chigr, F. Mental health among students with neurodevelopment disorders: Case of dyslexic children and adolescents. Dement. Neuropsychol. 2021, 15, 533–540. [Google Scholar] [CrossRef]
- Seligman, M.E. Positive health. Appl. Psychol. 2008, 57, 3–18. [Google Scholar] [CrossRef]
- Brown, L.; Ospina, J.P.; Celano, C.M.; Huffman, J.C. The effects of positive psychological interventions on medical patients’ anxiety: A meta-analysis. Psychosom. Med. 2019, 81, 595–602. [Google Scholar] [CrossRef]
- Narafshan, M.H.; Noori, S. Enhancing self-esteem in classroom language learning: The potential of implementing a strength-based positive psychology intervention at higher education. Int. J. Lang. Teach. Educ. 2018, 2, 334–345. [Google Scholar] [CrossRef]
- Ouweneel, E.; Le Blanc, P.M.; Schaufeli, W.B. Do-it-yourself: An online positive psychology intervention to promote positive emo-tions, self-efficacy, and engagement at work. Career Dev. Int. 2013, 18, 173–195. [Google Scholar] [CrossRef]
- Archer, S.; Yates, J. Understanding potential career changers’ experience of career confidence following a positive psychology based coaching programme. Coach. Int. J. Theory Res. Pract. 2017, 10, 157–175. [Google Scholar] [CrossRef]
- Trom, P.; Burke, J. Positive psychology intervention (PPI) coaching: An experimental application of coaching to improve the effectiveness of a gratitude intervention. Coach. Int. J. Theory Res. Pract. 2021, 15, 131–142. [Google Scholar] [CrossRef]
- Ghanizadeh, A.; Al-Hoorie, A.H.; Jahedizadeh, S. Mindfulness. In Higher Order Thinking Skills in the Language Classroom: A Concise Guide; Springer Science and Business Media LLC: Dordrecht, The Netherlands, 2020; pp. 159–172. [Google Scholar]
- Mars, T.S.; Abbey, H. Mindfulness meditation practise as a healthcare intervention: A systematic review. Int. J. Osteopat. Med. 2010, 13, 56–66. [Google Scholar] [CrossRef]
- Zoogman, S.; Goldberg, S.B.; Hoyt, W.T.; Miller, L. Mindfulness interventions with youth: A meta-analysis. Mindfulness 2015, 6, 290–302. [Google Scholar] [CrossRef]
- Gander, F.; Proyer, R.T.; Ruch, W.; Wyss, T. Strength-based positive interventions: Further evidence for their potential in enhancing well-being and alleviating depression. J. Happiness Stud. 2013, 14, 1241–1259. [Google Scholar] [CrossRef]
- Curry, O.S.; Rowland, L.A.; Van Lissa, C.J.; Zlotowitz, S.; McAlaney, J.; Whitehouse, H. Happy to help? A systematic review and meta-analysis of the effects of performing acts of kindness on the well-being of the actor. J. Exp. Soc. Psychol. 2018, 76, 320–329. [Google Scholar] [CrossRef]
- Hogan, B.E.; Linden, W.; Najarian, B. Social support interventions: Do they work? Clin. Psychol. Rev. 2002, 22, 381–440. [Google Scholar] [CrossRef]
- Hendriks, T.; Schotanus-Dijkstra, M.; Hassankhan, A.; Graafsma, T.G.; Bohlmeijer, E.; de Jong, J. The efficacy of positive psychological interventions from non-western countries: A systematic review and meta-analysis. Int. J. Wellbeing 2018, 8. [Google Scholar] [CrossRef]
- Chakhssi, F.; Kraiss, J.T.; Sommers-Spijkerman, M.; Bohlmeijer, E.T. The effect of positive psychology interventions on well-being and distress in clinical samples with psychiatric or somatic disorders: A systematic review and meta-analysis. BMC Psychiatry 2018, 18, 211. [Google Scholar] [CrossRef]
- Shoshani, A.; Steinmetz, S. Positive psychology at school: A school-based intervention to promote adolescents’ mental health and well-being. J. Happiness Stud. 2014, 15, 1289–1311. [Google Scholar] [CrossRef]
- Benoit, V.; Gabola, P. Effects of positive psychology interventions on the well-being of young children: A systematic literature review. Int. J. Environ. Res. Public Health 2021, 18, 12065. [Google Scholar] [CrossRef]
- Tejada-Gallardo, C.; Blasco-Belled, A.; Torrelles-Nadal, C.; Alsinet, C. Effects of school-based multicomponent positive psychology interventions on well-being and distress in adolescents: A systematic review and meta-analysis. J. Youth Adolesc. 2020, 49, 1943–1960. [Google Scholar] [CrossRef]
- Alam, A. Positive psychology goes to school: Conceptualizing students’ happiness in 21st century schools while ‘minding the mind!’are we there yet? evidence-backed, school-based positive psychology interventions. ECS Trans. 2022, 107, 11199. [Google Scholar] [CrossRef]
- Huang, Y.; He, M.; Li, A.; Lin, Y.; Zhang, X.; Wu, K. Personality, behavior characteristics, and life quality impact of children with dyslexia. Int. J. Environ. Res. Public Health 2020, 17, 1415. [Google Scholar] [CrossRef]
- Demiris, G.; Oliver, D.P.; Washington, K.T. Defining and analyzing the problem. In Behavioral Intervention Research in Hospice and Palliative Care: Building an Evidence Base; Elsevier: Amsterdam, The Netherlands, 2019; pp. 27–39. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Daigle, E.; Guitard, J.; Roy-Charland, A. Exploration of the flourishing scale’s psychometric properties for french-canadians and its relationship with HEXACO personality traits. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 2022, 54, 79–84. [Google Scholar] [CrossRef]
- Bull, L. Sunflower therapy for children with specific learning difficulties (dyslexia): A randomised, controlled trial. Complement. Ther. Clin. Pract. 2007, 13, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Burton, S. Self-esteem groups for secondary pupils with dyslexia. Educ. Psychol. Pract. 2004, 20, 55–73. [Google Scholar] [CrossRef]
- Boyes, M.E.; Leitao, S.; Claessen, M.; Dzidic, P.; Badcock, N.A.; Nayton, M. Piloting ‘Clever Kids’: A randomized-controlled trial as-sessing feasibility, efficacy, and acceptability of a socioemotional well-being programme for children with dyslexia. Br. J. Educ. Psychol. 2021, 91, 950–971. [Google Scholar] [CrossRef]
- Firth, N.; Frydenberg, E.; Steeg, C.; Bond, L. Coping successfully with dyslexia: An initial study of an inclusive school-based resil-ience programme. Dyslexia 2013, 19, 113–130. [Google Scholar] [CrossRef]
- Tarrasch, R.; Berman, Z.; Friedmann, N. Mindful reading: Mindfulness meditation helps keep readers with dyslexia and ADHD on the lexical track. Front. Psychol. 2016, 7, 578. [Google Scholar] [CrossRef]
- Upadhyay, U.T. Improving Well-Being, Academic Self-Concept and Academic Achievement of Indian Children with Specific Learning Disability by utilising Positive Psychology Intervention. Disabil. CBR Incl. Dev. 2021, 32, 105–135. [Google Scholar] [CrossRef]
- Waters, L. A Review of school-based positive psychology interventions. Aust. Educ. Dev. Psychol. 2011, 28, 75–90. [Google Scholar] [CrossRef]
- Paul, C.; Holt, J. Involving the public in mental health and learning disability research: Can we, should we, do we? J. Psychiatr. Ment. Health Nurs. 2017, 24, 570–579. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based stress reduction (MBSR). Constr. Hum. Sci. 2003, 8, 73. [Google Scholar]
- Georgiou, G.K.; Parrila, R.; McArthur, G. Dyslexia and mental health problems: Introduction to the special issue. Ann. Dyslexia 2024, 74, 1–3. [Google Scholar] [CrossRef]
- Gonzalez-Gross, M.; Gracia-Marco, L.; Ortega, F.B.; Jiménez-Pavón, D.; Rodríguez, G.; Valtueña, J.; Díaz-Marténez, E.; González-Gross, M.; Castillo, M.J.; Vicente-Rodríguez, G.; et al. Contribution of bone turnover markers to bone mass in pubertal boys and girls. J. Pediatr. Endocrinol. Metab. 2011, 24, 971–974. [Google Scholar] [CrossRef]
- Tam, C.L.; Lim, S.G. Perceived social support, coping capability and gender differences among young adults. Sunway Acad. J. 2009, 6, 75–88. [Google Scholar]
- Duan, W.; Klibert, J.; Schotanus-Dijkstra, M.; Llorens, S.; van den Heuvel, M.; Mayer, C.H.; Tomasulo, D.; Liao, Y.; van Zyl, L.E. Positive psychological interventions: How, when and why they work: Beyond WEIRD contexts. Front. Psychol. 2022, 13, 1021539. [Google Scholar] [CrossRef]
- Cheney, G.; Schlösser, A.; Nash, P.; Glover, L. Targeted group-based interventions in schools to promote emotional well-being: A systematic review. Clin. Child Psychol. Psychiatry 2014, 19, 412–438. [Google Scholar] [CrossRef]
- Juvonen, J.; Lessard, L.M.; Rastogi, R.; Schacter, H.L.; Smith, D.S. Promoting social inclusion in educational settings: Challenges and opportunities. Educ. Psychol. 2019, 54, 250–270. [Google Scholar] [CrossRef]
- Jiménez, J.E.; de la Cadena, C.G.; Siegel, L.S.; O’shanahan, I.; García, E.; Rodríguez, C. Gender ratio and cognitive profiles in dyslexia: A cross-national study. Read. Writ. 2011, 24, 729–747. [Google Scholar] [CrossRef]
- Hendriks, T.; Schotanus-Dijkstra, M.; Hassankhan, A.; De Jong, J.; Bohlmeijer, E. The efficacy of multi-component positive psy-chology interventions: A systematic review and meta-analysis of randomized controlled trials. J. Happiness Stud. 2020, 21, 357–390. [Google Scholar] [CrossRef]
- Karimupfumbi, F.; Dwarika, V.M. Teachers’ experiences of using the screening, identification, assessment and support strategy to support learners who present with characteristics of dyslexia. S. Afr. J. Child. Educ. 2022, 12, 1107. [Google Scholar] [CrossRef]
- Makgato, M.M.; Leseyane-Kgari, M.; Cekiso, M.; Mandende, I.P.; Masha, R. Evaluating the awareness and knowledge of dyslexia among primary school teachers in Tshwane District, South Africa. Afr. J. Disabil. 2022, 11, 807. [Google Scholar] [CrossRef]
- Muktamath, V.U.; Hegde, P.R.; Koneru, R.; Lakashetti, R. Screening, Assessment and Identification Tools for Dyslexia. In Recent Advances in the Study of Dyslexia; IntechOpen: Rijeka, Croatia, 2024. [Google Scholar]
- Mendoza, S.T. Strengths Development: An Action Research Study of Academic Self-Efficacy in Undecided 1st-Year College Stu-dents. Ph.D. Dissertation, Azusa Pacific University, Azusa, CA, USA, 2022. [Google Scholar]
- Ng, W.; Ong, K.R. Using positive psychological interventions to improve well-being: Are they effective across cultures, for clinical and non-clinical samples? J. Contemp. Psychother. 2022, 52, 45–53. [Google Scholar] [CrossRef]
- Basurrah, A.A.; Di Blasi, Z.; Lambert, L.; Murphy, M.; Warren, M.A.; Setti, A.; Baddar, M.A.; Shrestha, T. The effects of positive psychology interventions in Arab countries: A systematic review. Appl. Psychol. Health Well-Being 2023, 15, 803–821. [Google Scholar] [CrossRef]
- Boniwell, I.; Tunariu, A.D. Positive Psychology: Theory, Research and Applications; McGraw-Hill Education: Berkshire, UK, 2019. [Google Scholar]
- Novita, S. Secondary symptoms of dyslexia: A comparison of self-esteem and anxiety profiles of children with and without dyslexia. Eur. J. Spéc. Needs Educ. 2016, 31, 279–288. [Google Scholar] [CrossRef]
- Carr, A.; Cullen, K.; Keeney, C.; Canning, C.; Mooney, O.; Chinseallaigh, E.; O’Dowd, A. Effectiveness of positive psychology inter-ventions: A systematic review and meta-analysis. J. Posit. Psychol. 2021, 16, 749–769. [Google Scholar] [CrossRef]
- Kreienkamp, M.; Wheatley, D.; Ndobo, A. Assessing the efficacy of a resilience training intervention for long-term improvements in well-being and resilience. Appl. Psychol. Health Well-Being 2024. [Google Scholar] [CrossRef] [PubMed]
- Au, J.; Gibson, B.C.; Bunarjo, K.; Buschkuehl, M.; Jaeggi, S.M. Quantifying the difference between active and passive control groups in cognitive interventions using two meta-analytical approaches. J. Cogn. Enhanc. 2020, 4, 192–210. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).