
Pregnancy- and Birth-Related Experiences among Postpartum Women during the Third Wave of the COVID-19 Pandemic—A Multinational European Study

 ,
,  ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Results
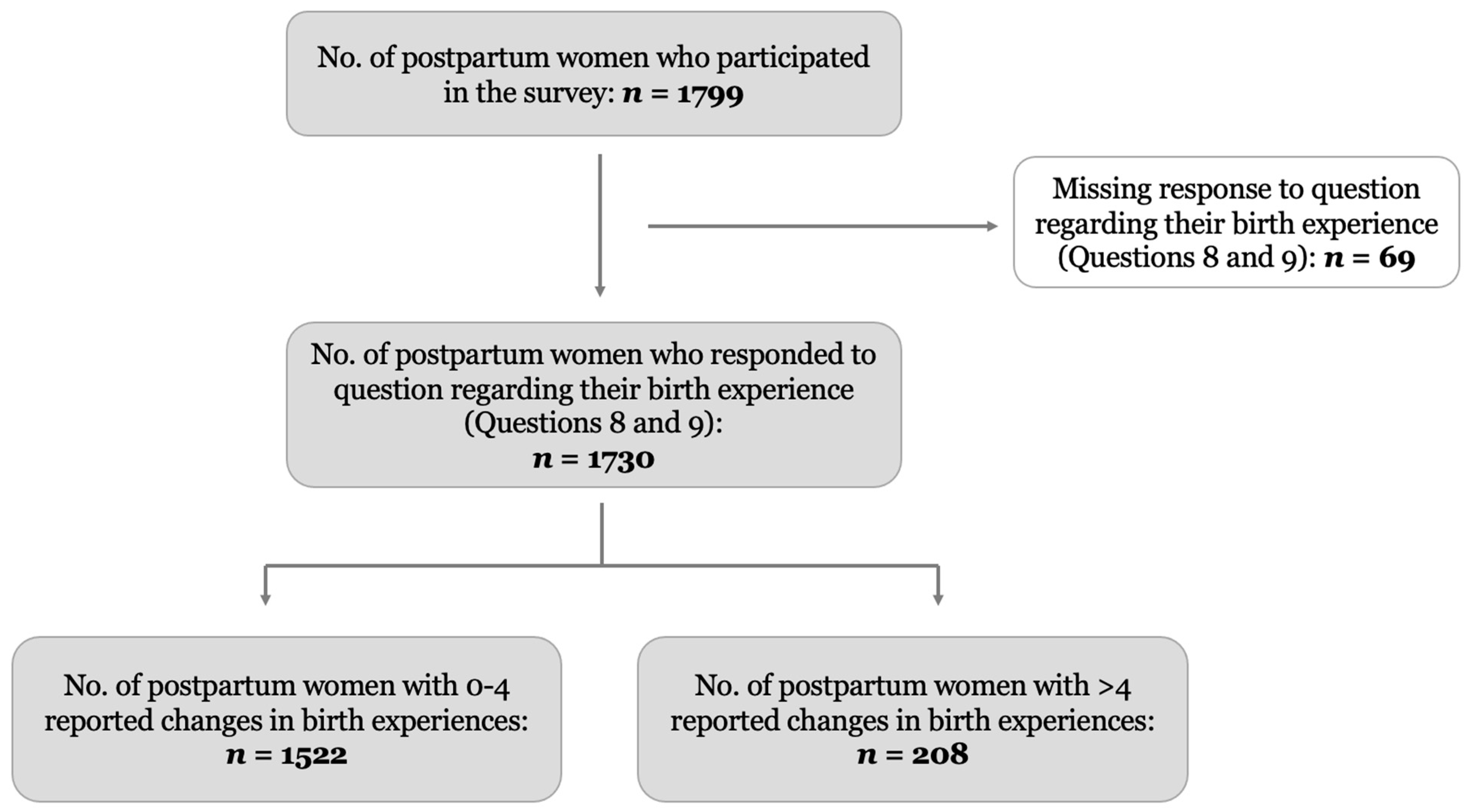
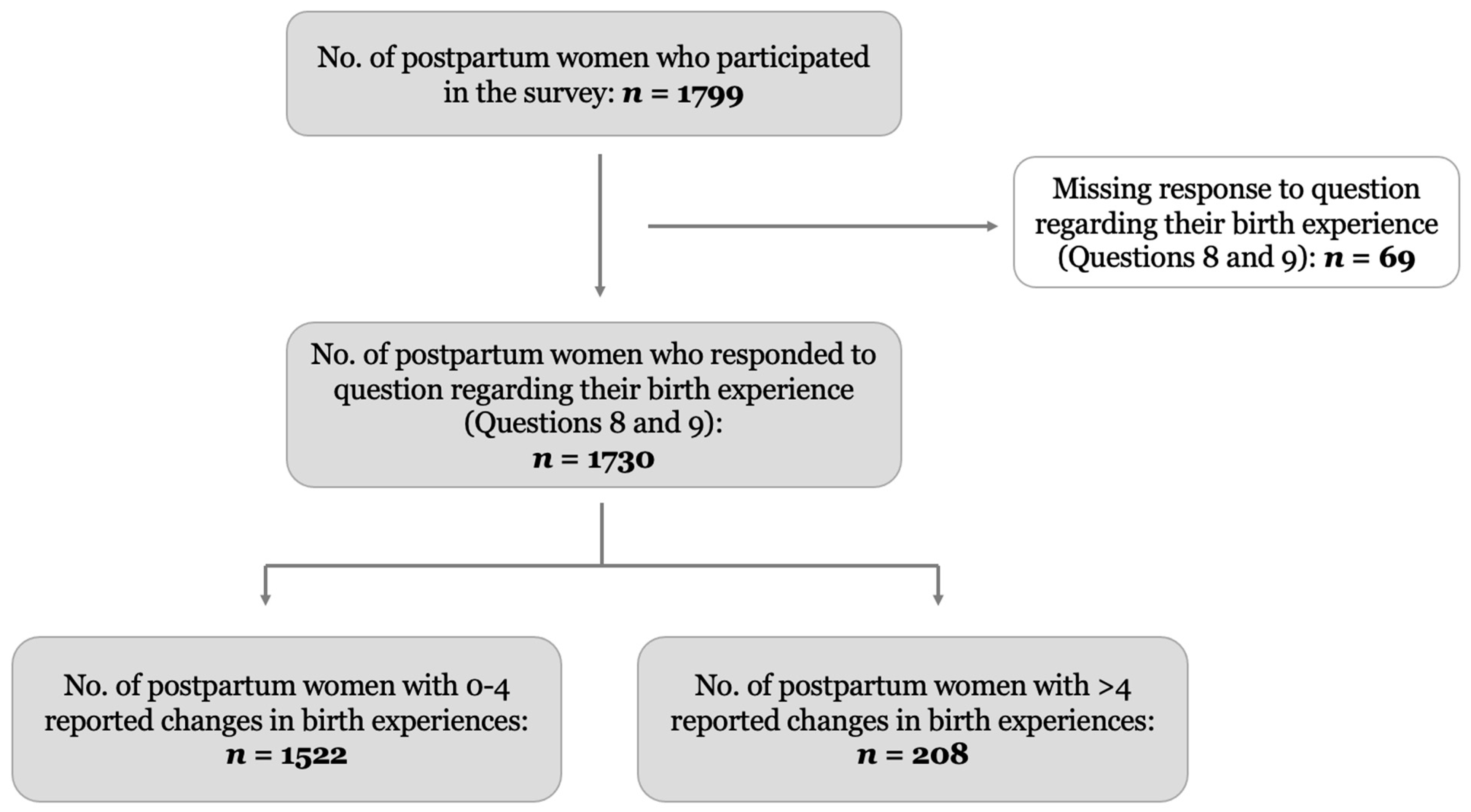
2.1. Characteristics of the Study Participants
2.2. Pregnancy- and Birth-Related Changes during the COVID-19 Pandemic
2.3. Mental Health Status of Postpartum Women
2.4. Factors Associated with Major Depressive and Anxiety Symptoms
3. Discussion
Strengths and Limitations
4. Methods and Materials
4.1. Design and Study Population
4.2. Measures
4.2.1. Women’s Pregnancy and Birth-Related Experiences during the COVID-19 Pandemic
4.2.2. Mental Health Measures
4.2.3. Sociodemographic Characteristics
4.2.4. COVID-19 Status, Health Characteristics, and Reproductive Characteristics
4.3. Statistical Analyses
4.4. Ethical Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus Disease |
| CI | Confidence Interval |
| EDS | Edinburgh Depression Scale |
| OR | Odds Ratio |
| UK | United Kingdom |
References
- Aydin, E.; Glasgow, K.A.; Weiss, S.M.; Khan, Z.; Austin, T.; Johnson, M.H.; Barlow, J.; Lloyd-Fox, S. Giving birth in a pandemic: Women’s birth experiences in England during COVID-19. BMC Pregnancy Childbirth 2022, 22, 304. [Google Scholar] [CrossRef]
- Liu, C.H.; Koire, A.; Erdei, C.; Mittal, L. Unexpected changes in birth experiences during the COVID-19 pandemic: Implications for maternal mental health. Arch. Gynecol. Obstet. 2021, 306, 687–697. [Google Scholar] [CrossRef]
- Morniroli, D.; Consales, A.; Colombo, L.; Bezze, E.; Zanotta, L.; Plevani, L.; Fumagalli, M.; Mosca, F.; Giannì, M. Exploring the Impact of Restricted Partners’ Visiting Policies on Non-Infected Mothers’ Mental Health and Breastfeeding Rates during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6347. [Google Scholar] [CrossRef] [PubMed]
- Mayopoulos, G.A.; Ein-Dor, T.; Dishy, G.A.; Nandru, R.; Chan, S.J.; Hanley, L.E.; Kaimal, A.J.; Dekel, S. COVID-19 is associated with traumatic childbirth and subsequent mother-infant bonding problems. J. Affect. Disord. 2020, 282, 122–125. [Google Scholar] [CrossRef] [PubMed]
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018.
- Vedeler, C.; Nilsen, A.B.V.; Blix, E.; Downe, S.; Eri, T.S. What women emphasise as important aspects of care in childbirth—An online survey. BJOG Int. J. Obstet. Gynaecol. 2021, 129, 647–655. [Google Scholar] [CrossRef]
- Gildner, T.E.; Thayer, Z.M. Birth plan alterations among American women in response to COVID-19. Health Expect. 2020, 23, 969–971. [Google Scholar] [CrossRef]
- Tauqeer, F.; Ceulemans, M.; Gerbier, E.; Passier, A.; Oliver, A.; Foulon, V.; Panchaud, A.; Lupattelli, A.; Nordeng, H. Mental health of pregnant and postpartum women during the third wave of the Covid-19 pandemic—A European cross-sectional study. BMJ Open 2023, 13, e063391. [Google Scholar] [CrossRef]
- Eri, T.S.; Blix, E.; Downe, S.; Vedeler, C.; Nilsen, A.B.V. Giving birth and becoming a parent during the COVID-19 pandemic: A qualitative analysis of 806 women’s responses to three open-ended questions in an online survey. Midwifery 2022, 109, 103321. [Google Scholar] [CrossRef]
- Perzow, S.E.; Hennessey, E.-M.P.; Hoffman, M.C.; Grote, N.K.; Davis, E.P.; Hankin, B.L. Mental health of pregnant and postpartum women in response to the COVID-19 pandemic. J. Affect. Disord. Rep. 2021, 4, 100123. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.; Wendt, A.; Bennett, I.M.; Bhat, A. Suicide and Maternal Mortality. Curr. Psychiatry Rep. 2022, 24, 239–275. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef]
- Iyengar, U.; Jaiprakash, B.; Haitsuka, H.; Kim, S. One Year Into the Pandemic: A Systematic Review of Perinatal Mental Health Outcomes During COVID-19. Front. Psychiatry 2021, 12, 674194. [Google Scholar] [CrossRef]
- Fisher, J.; De Mello, M.C.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: A systematic review. Bull. World Health Organ. 2012, 90, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.-L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- López-Morales, H.; del Valle, M.V.; Canet-Juric, L.; Andrés, M.L.; Galli, J.I.; Poó, F.; Urquijo, S. Mental health of pregnant women during the COVID-19 pandemic: A longitudinal study. Psychiatry Res. 2020, 295, 113567. [Google Scholar] [CrossRef]
- Ceulemans, M.; Foulon, V.; Ngo, E.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; et al. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic—A multinational cross-sectional study. Acta Obstet. Gynecol. Scand. 2021, 151, 146–147. [Google Scholar] [CrossRef]
- Zilver, S.J.M.; Hendrix, Y.M.G.A.; Broekman, B.F.P.; Leeuw, R.A.; de Groot, C.J.M.; van Pampus, M.G. Fear of childbirth in pregnancy was not increased during the COVID-19 pandemic in the Netherlands: A cross-sectional study. Acta Obstet. Gynecol. Scand. 2022, 00, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.J.; Fisher, A.C.; Nicholson, S.C. Interest in Home Birth During the COVID-19 Pandemic: Analysis of Google Trends Data. J. Midwifery Women’s Health 2022, 67, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Viaux-Savelon, S.; Maurice, P.; Rousseau, A.; Leclere, C.; Renout, M.; Berlingo, L.; Cohen, D.; Jouannic, J.M. Impact of COVID-19 lockdown on maternal psychological status, the couple’s relationship and mother-child interaction: A prospective study. BMC Pregnancy Childbirth 2022, 22, 732. [Google Scholar] [CrossRef]
- Guo, J.; De Carli, P.; Lodder, P.; Bakermans-Kranenburg, M.J.; Riem, M.M.E. Maternal mental health during the COVID-19 lockdown in China, Italy, and the Netherlands: A cross-validation study. Psychol. Med. 2021, 52, 3349–3359. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ (Clin. Res. Ed.) 2020, 371, m4022. [Google Scholar] [CrossRef] [PubMed]
- Smith-Nielsen, J.; Egmose, I.; Wendelboe, K.I.; Steinmeier, P.; Lange, T.; Vaever, M.S. Can the Edinburgh Postnatal Depression Scale-3A be used to screen for anxiety? BMC Psychol. 2021, 9, 118. [Google Scholar] [CrossRef]
- Isikalan, M.M.; Özkaya, B.; Özkaya, E.B.; Gümüş, M.; Ferlibaş, E.; Acar, A. Does wearing double surgical masks during the COVID-19 pandemic reduce maternal oxygen saturation in term pregnant women? A prospective study. Arch. Gynecol. Obstet. 2022, 305, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Toprak, E.; Bulut, A.N. The effect of mask use on maternal oxygen saturation in term pregnancies during the COVID-19 process. J. Périnat. Med. 2020, 49, 148–152. [Google Scholar] [CrossRef]
- Elling, C.; Sleutel, M.R.; Wells, J.; Newcomb, P.; Valdez, E.; Walker, K.; Nguyen, T. Women’s and Nurses’ Perceptions of Visitor Restrictions After Childbirth During the COVID-19 Pandemic. Nurs. Women’s Health 2022, 26, 278–287. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observa-tional Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Using the Edinburgh Postnatal Depression Scale, Side 112. Department of Health, Government of Western Australia. (2006). Edinburgh Postnatal Depression Scale (EPDS): Translated Versions—Validated. Perth, Western Australia: State Perinatal Mental Health Reference Group. Available online: mcpapformoms.org (accessed on 14 October 2022).

{kind=link}
| Total | Pregnancy and Birth-Related Changes | ||
|---|---|---|---|
| n = 1730 | 0–4 n = 1522 | >4 Changes n = 208 | |
| n (%) | n (%) | n (%) | |
| Socio-demographic characteristics | |||
| Country * | |||
| Norway | 1113 (64.3) | 959 (63.0) | 154 (74.0) |
| Belgium | 213 (12.3) | 192 (12.6) | 21 (10.1) |
| Switzerland | 160 (9.2) | 149 (9.8) | 11 (5.3) |
| The Netherlands | 146 (8.4) | 131 (8.6) | 15 (7.2) |
| UK | 98 (5.7) | 91 (6.0) | 7 (3.4) |
| Maternal age (years) | |||
| 18–30 | 675 (39.0) | 581 (38.2) | 94 (45.2) |
| 31–40 | 897 (51.8) | 796 (52.3) | 101 (48.6) |
| >40 | 44 (2.5) | 38 (2.5) | 6 (2.9) |
| Relationship status | |||
| Married/cohabiting/partner | 1595 (92.2) | 1398 (91.9) | 197 (94.7) |
| Single | 21 (1.2) | 17 (1.1) | 4 (1.9) |
| Professional status | |||
| Professionally active | 1430 (82.7) | 1249 (82.1) | 181 (87.0) |
| Not professionally active | 176 (10.2) | 157 (10.3) | 19 (9.1) |
| Education level | |||
| Low | 34 (2.0) | 29 (1.9) | 5 (2.4) |
| Medium | 290 (16.8) | 259 (17.0) | 31 (14.9) |
| High | 1279 (73.9) | 1114 (73.2) | 165 (79.3) |
| Healthcare worker | |||
| Yes | 486 (28.1) | 423 (27.8) | 63 (30.3) |
| No | 947 (54.7) | 828 (54.4) | 119 (57.2) |
| Smoking status | |||
| Smoking in pregnancy | 6 (0.3) | 5 (0.3) | 1 (0.4) |
| Smoking postpartum | 18 (1.0) | 16 (1.1) | 2 (1.0) |
| Both | 13 (0.8) | 12 (0.8) | 1 (0.4) |
| None | 1579 (91.3) | 1382 (90.8) | 197 (94.7) |
| COVID-19 characteristics | |||
| COVID-19 status a * | |||
| Positive test | 93 (5.4) | 87 (5.7) | 6 (2.9) |
| Symptomatic b | 154 (8.9) | 128 (8.4) | 26 (12.5) |
| None | 1425 (82.4) | 1255 (82.5) | 170 (81.7) |
| Severity of the infection | |||
| No or mild symptoms | 94 (5.4) | 83 (5.5) | 11 (5.3) |
| Moderate symptoms | 69 (4.0) | 61 (4.0) | 8 (3.9) |
| Hospitalized/long-term symptoms | 29 (1.7) | 24 (1.6) | 5 (2.4) |
| Family member with COVID-19 | |||
| Yes | 343 (19.8) | 304 (20.0) | 39 (18.8) |
| No | 1387 (80.2) | 1218 (80.0) | 169 (81.3) |
| Health and reproductive characteristics | |||
| Chronic mental illness c | 34 (2.0) | 30 (2.0) | 4 (1.9) |
| Chronic somatic illness d | 457 (26.4) | 390 (25.6) | 67 (32.2) |
| Infant age | |||
| ≤6 weeks | 653 (37.7) | 584 (38.4) | 69 (33.2) |
| 6–12 weeks | 1077 (62.3) | 938 (61.6) | 139 (66.8) |
| Currently breastfeeding e | |||
| Yes | 1576 (91.1) | 1387 (91.1) | 189 (90.9) |
| No | 154 (8.9) | 135 (8.9) | 19 (9.1) |
| Previous breastfeeding experience * | |||
| Yes | 651 (37.6) | 593 (39.0) | 58 (27.9) |
| No | 925 (53.5) | 794 (52.2) | 131 (63.0) |
| Presence of support during delivery | |||
| Partner | 1529 (88.4) | 1343 (88.2) | 186 (89.4) |
| Relative, friend or other | 27 (1.6) | 22 (1.4) | 5 (2.4) |
| None f | 24 (1.4) | 19 (1.2) | 5 (2.4) |
| n | % | |
|---|---|---|
| Partner not allowed to accompany me to pregnancy care appointments (e.g., ultrasound) | 1439 | 83.2 |
| Changed settings for prenatal care (e.g., no more group classes) | 1114 | 64.4 |
| Cancellation of hospital visits for information | 739 | 42.7 |
| Change in schedule of persons (e.g., midwife, gynaecologist) providing pregnancy care | 403 | 23.3 |
| Cancellation or reduction of appointments for prenatal examination | 370 | 21.4 |
| Change from in-person prenatal visits to virtual visits | 358 | 20.7 |
| Other a | 168 | 9.7 |
| No pregnancy or birth-related changes | 80 | 4.6 |
| Change in schedule for C-section or induction of labour | 61 | 3.5 |
| Change of plan: from one selected hospital/birth centre to another | 58 | 3.4 |
| Change of plan: from hospital birth to home birth | 30 | 1.7 |
| Change of plan: from home birth to hospital birth | 24 | 1.4 |
| Pregnancy and Birth-Related Changes | Presence of Support During Delivery a | |||||||
|---|---|---|---|---|---|---|---|---|
| 0–4 Changes | >4 Changes | Yes | No | |||||
| (n = 1522) | (n = 208) | (n = 1556) | (n = 24) | |||||
| N | % | N | % | N | % | N | % | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | |||||
| Depression | ||||||||
| Moderate | 452 | 29.7 | 86 | 41.3 ** | 487 | 31.3 | 10 | 43.5 |
| Score ≥ 10 | (28.0–32.7) | (34.8–48.3) | (29.0–33.6) | (27.4–65.3) | ||||
| Major | 237 | 15.6 | 52 | 25.0 ** | 256 | 16.5 | 6 | 26.1 |
| Score ≥ 13 | (14.1–7.8) | (19.2–31.1) | (14.7–18.4) | (14.6–49.8) | ||||
| EDS-3A | ||||||||
| Anxiety | 491 | 32.3 | 86 | 41.3 * | 521 | 33.5 | 10 | 43.5 |
| (30.6–35.4) | (34.8–48.3) | (31.2–35.9) | (27.5–65.4) | |||||
| N | Major Depressive Symptoms (EDS ≥ 13) | Anxiety Symptoms (EDS-3A ≥ 5) | |||
|---|---|---|---|---|---|
| cOR 95% CI | aOR a 95% CI | cOR 95% CI | aOR b 95% CI | ||
| Changes in pregnancy and birth experience | |||||
| 0–4 changes | 1522 | Ref | Ref | Ref | Ref |
| >4 changes | 208 | 1.77 (1.25–2.48) | 1.75 (1.20–2.55) | 1.44 (1.07–1.94) | 1.55 (1.13–2.12) |
| Presence of support during delivery | |||||
| Yes | 1556 | Ref | Ref | Ref | Ref |
| No | 24 | 2.09 (0.86–5.09) | 1.12 (0.31–3.96) | 1.68 (0.78–3.78) | 1.15 (0.42–3.16) |
| Pregnancy and Birth-Related Changes (Yes vs. No, Reference Category: No) a | Major Depressive Symptoms (EDS ≥ 13) | Anxiety Symptoms (EDS-3A ≥ 5) | ||
|---|---|---|---|---|
| aOR | 95% CI | aOR | 95% CI | |
| Change of plan: from home birth to hospital birth | 3.46 | 1.31–8.72 | 2.27 | 0.90–5.78 |
| Change of plan: from one selected hospital/birth centre to another | 3.01 | 1.59–5.51 | 2.32 | 1.29–4.16 |
| Change in schedule for C-section or induction of labour | 2.63 | 1.41–4.75 | 2.64 | 1.50–4.67 |
| Cancellation or reduction of appointments for prenatal examination | 2.43 | 1.79–3.28 | 1.78 | 1.38–2.31 |
| Change in schedule of persons (e.g., midwife, gynaecologist) providing pregnancy care | 1.70 | 1.26–2.29 | 1.50 | 1.17–1.92 |
| Changed settings for prenatal care (e.g., no more group classes) | 1.50 | 1.10–2.06 | 1.28 | 1.01–1.64 |
| Change from in-person prenatal visits to virtual visits | 1.46 | 1.05–1.99 | 1.37 | 1.05–1.77 |
| Cancellation of hospital visits for information | 1.36 | 1.02–1.82 | 1.26 | 1.00–1.58 |
| Partner not allowed to attend pregnancy care appointments (e.g., ultrasound) | 1.06 | 0.73–1.59 | 1.21 | 0.89–1.65 |
| Change of plan: from hospital birth to home birth | 0.92 | 0.30–2.31 | 0.77 | 0.32–1.71 |
| Other | 0.88 | 0.52–1.41 | 0.75 | 0.50–1.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araya, R.A.; Tauqeer, F.; Ceulemans, M.; Gerbier, E.; Maisonneuve, E.; Passier, A.; Oliver, A.; Panchaud, A.; Lupattelli, A.; Nordeng, H. Pregnancy- and Birth-Related Experiences among Postpartum Women during the Third Wave of the COVID-19 Pandemic—A Multinational European Study. Pharmacoepidemiology 2023, 2, 54-67. https://doi.org/10.3390/pharma2010006
Araya RA, Tauqeer F, Ceulemans M, Gerbier E, Maisonneuve E, Passier A, Oliver A, Panchaud A, Lupattelli A, Nordeng H. Pregnancy- and Birth-Related Experiences among Postpartum Women during the Third Wave of the COVID-19 Pandemic—A Multinational European Study. Pharmacoepidemiology. 2023; 2(1):54-67. https://doi.org/10.3390/pharma2010006
Chicago/Turabian StyleAraya, Robin A., Fatima Tauqeer, Michael Ceulemans, Eva Gerbier, Emeline Maisonneuve, Anneke Passier, Alison Oliver, Alice Panchaud, Angela Lupattelli, and Hedvig Nordeng. 2023. "Pregnancy- and Birth-Related Experiences among Postpartum Women during the Third Wave of the COVID-19 Pandemic—A Multinational European Study" Pharmacoepidemiology 2, no. 1: 54-67. https://doi.org/10.3390/pharma2010006
APA StyleAraya, R. A., Tauqeer, F., Ceulemans, M., Gerbier, E., Maisonneuve, E., Passier, A., Oliver, A., Panchaud, A., Lupattelli, A., & Nordeng, H. (2023). Pregnancy- and Birth-Related Experiences among Postpartum Women during the Third Wave of the COVID-19 Pandemic—A Multinational European Study. Pharmacoepidemiology, 2(1), 54-67. https://doi.org/10.3390/pharma2010006