Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Features
3.2. Clinical Findings
3.3. Microbiology
3.4. Treatment
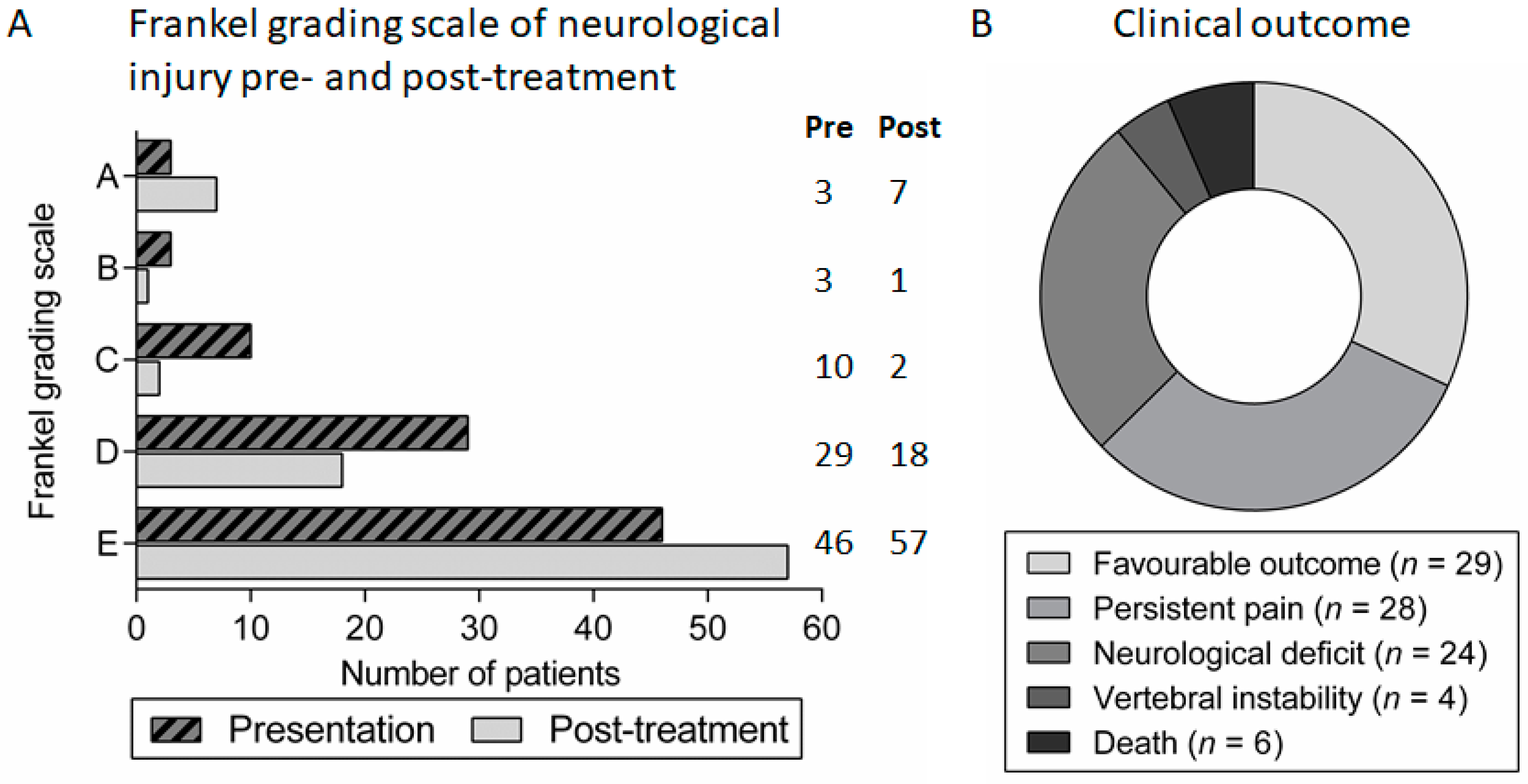
3.5. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M., III; Petermann, G.W.; et al. 2015 infectious diseases society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin. Infect. Dis. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, W. Vertebral osteomyelitis. N. Engl. J. Med. 2010, 362, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, T.; Chikuda, H.; Yasunaga, H.; Horiguchi, H.; Fushimi, K.; Saita, K. Incidence and risk factors for mortality of vertebral osteomyelitis: A retrospective analysis using the Japanese diagnosis procedure combination database. BMJ Open 2013, 3, e002412. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, E.K.; Sinha, R. Vertebral osteomyelitis in adults: An update. Br. Med. Bull. 2016, 117, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Frankel, H.L.; Hancock, D.O.; Hyslop, G.; Melzak, J.; Michaelis, L.S.; Ungar, G.H.; Vernon, J.D.; Walsh, J.J. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia 1969, 7, 179–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.K. Treatment of tuberculosis of the spine with neurologic complications. Clin. Orthop. Relat. Res. 2002, 398, 75–84. [Google Scholar] [CrossRef]
- Rossbach, B.P.; Niethammer, T.R.; Paulus, A.C.; Melcher, C.; Birkenmaier, C.; Jansson, V.; Wegener, B. Surgical treatment of patients with spondylodiscitis and neurological deficits caused by spinal epidural abscess (SEA) is a predictor of clinical outcome. J. Spinal. Disord. Tech. 2014, 27, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Arko, L.T.; Quach, E.; Nguyen, V.; Chang, D.; Sukul, V.; Kim, B.S. Medical and surgical management of spinal epidural abscess: A systematic review. Neurosurg. Focus 2014, 37, E4. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, C.; Scorzolini, L.; Massetti, A.P.; Carnevalini, M.; d’Ettorre, G.; Venditti, M.; Vullo, V.; Orsi, G.B. A seven-year prospective study on spondylodiscitis: Epidemiological and microbiological features. Infection 2010, 38, 102–107. [Google Scholar] [CrossRef] [PubMed]
- McHenry, M.C.; Easley, K.A.; Locker, G.A. Vertebral osteomyelitis: Long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin. Infect. Dis. 2002, 34, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Gouliouris, T.; Aliyu, S.H.; Brown, N.M. Spondylodiscitis: Update on diagnosis and management. J. Antimicrob. Chemother. 2010, 65, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Koslow, M.; Kuperstein, R.; Eshed, I.; Perelman, M.; Maor, E.; Sidi, Y. The unique clinical features and outcome of infectious endocarditis and vertebral osteomyelitis co-infection. Am. J. Med. 2014, 127, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Lemaignen, A.; Ghout, I.; Dinh, A.; Gras, G.; Fantin, B.; Zarrouk, V.; Carlier, R.; Loret, J.E.; Denes, E.; Greder, A.; et al. Characteristics of and risk factors for severe neurological deficit in patients with pyogenic vertebral osteomyelitis: A case-control study. Medicine 2017, 96, e6387. [Google Scholar] [CrossRef] [PubMed]
- Garkowski, A.; Zajkowska, A.; Czupryna, P.; Lebkowski, W.; Letmanowski, M.; Golebicki, P.; Moniuszko, A.; Ustymowicz, A.; Pancewicz, S.; Zajkowska, J. Infectious Spondylodiscitis—A case series analysis. Adv. Med. Sci. 2014, 59, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Donovan, J.; Skittrall, J.P.; Moore, T.; Sargent, C.; Agranoff, D.; Llewelyn, M. An ageing population and changing UK bacteraemia profile may affect the characteristics and microbiology of infective spondylodiscitis. J. Infect. 2016, 73, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Conterno, L.O.; Turchi, M.D. Antibiotics for treating chronic osteomyelitis in adults. Cochrane Database Syst. Rev. 2013, 9, CD004439. [Google Scholar] [CrossRef] [PubMed]
- Bernard, L.; Dinh, A.; Ghout, I.; Simo, D.; Zeller, V.; Issartel, B.; Le Moing, V.; Belmatoug, N.; Lesprit, P.; Bru, J.P.; et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: An open-label, non-inferiority, randomised, controlled trial. Lancet 2015, 385, 875–882. [Google Scholar] [CrossRef]
- Roblot, F.; Besnier, J.M.; Juhel, L.; Vidal, C.; Ragot, S.; Bastides, F.; Le Moal, G.; Godet, C.; Mulleman, D.; Azais, I.; et al. Optimal duration of antibiotic therapy in vertebral osteomyelitis. Semin. Arthritis Rheum. 2007, 36, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Stengel, D.; Bauwens, K.; Sehouli, J.; Ekkernkamp, A.; Porzsolt, F. Systematic review and meta-analysis of antibiotic therapy for bone and joint infections. Lancet Infect. Dis. 2001, 1, 175–188. [Google Scholar] [CrossRef]
- Tsai, T.T.; Yang, S.C.; Niu, C.C.; Lai, P.L.; Lee, M.H.; Chen, L.H.; Chen, W.J. Early surgery with antibiotics treatment had better clinical outcomes than antibiotics treatment alone in patients with pyogenic spondylodiscitis: A retrospective cohort study. BMC Musculoskelet. Disord. 2017, 18, 175. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.D.; Melikian, R.; Ju, K.L.; Zurakowski, D.; Wood, K.B.; Bono, C.M.; Harris, M.B. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014, 14, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Alton, T.B.; Bransford, R.J.; Lee, M.J.; Bellabarba, C.B.; Chapman, J.R. Spinal epidural abscesses: Risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014, 14, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Cho, O.H.; Lee, Y.M.; Moon, C.; Park, S.Y.; Moon, S.M.; Lee, J.H.; Park, J.S.; Ryu, K.N.; Kim, S.H.; et al. Therapeutic outcomes of hematogenous vertebral osteomyelitis with instrumented surgery. Clin. Infect. Dis. 2015, 60, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Rayes, M.; Colen, C.B.; Bahgat, D.A.; Higashida, T.; Guthikonda, M.; Rengachary, S.; Eltahawy, H.A. Safety of instrumentation in patients with spinal infection. J. Neurosurg. Spine 2010, 12, 647–659. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Pathogen | Total | Single Organism Isolated | Multiple Organisms Isolated |
|---|---|---|---|---|
| Gram positive | All | 58 | 46 | 12 |
| Staphylococcus aureus | 35 | 33 | 2 | |
| Coagulase negative Staphylococci | 11 | 6 | 5 | |
| Enterococcus faecalis | 3 | 1 | 2 | |
| Streptococcus pneumoniae | 3 | 3 | 0 | |
| Viridans group Streptococci | 3 | 1 | 2 | |
| Group B Streptococci | 2 | 2 | 0 | |
| Group C/G Streptococci | 1 | 0 | 1 | |
| Gram negative | All | 17 | 13 | 4 |
| Escherichia coli | 11 | 10 | 1 | |
| Klebsiella pneumoniae | 2 | 1 | 1 | |
| Others | 4 | 2 | 2 | |
| Anaerobes | All | 9 | 3 | 6 |
| Proprionibacterium acnes | 4 | 2 | 2 | |
| Others | 5 | 1 | 4 |
| Risk Factor | Total (n = 91) | Favourable Outcome (n = 29) | Unfavourable Outcome 1 (n = 62) | p-Value 2 Univariate Analysis |
|---|---|---|---|---|
| Background | ||||
| Age (median (range)) | 62.5 (17–91) | 59 (17–90) | 64 (35–91) | 0.121 |
| Diabetes mellitus (n (%)) | 16 (18) | 1 (3) | 15 (24) | 0.017 * |
| Immune compromise (n (%)) | 18 (20) | 3 (10) | 15 (24) | 0.162 |
| Post-surgical (n (%)) | 16 (18) | 5 (17) | 11 (18) | >0.99 |
| Presenting features | ||||
| Sepsis (n (%)) | 22 (24) | 7 (24) | 15 (24) | >0.99 |
| Frankel grading scale A–D (n (%)) | 46 (51) | 5 (17) | 39 (63) | <0.001 * |
| Duration of symptoms (median days (range)) | 36 (1–203) | 27 (1–71) | 41 (2–203) | 0.049 * |
| C-reactive protein (median mg/L (range)) | 170 (4–508) | 143 (15–395) | 181 (4–508) | 0.157 |
| White blood cell count (median × 109 (range)) | 13.1 (6.0–33.7) | 12.2 (6.6–24.3) | 13.6 (6.0–33.7) | 0.18 |
| Endocarditis | 4 (4) | 1 (3) | 3 (5) | >0.99 |
| Radiological features | ||||
| Epidural abscess (n (%)) | 55 (60) | 16 (55) | 39 (63) | 0.467 |
| Multiple level discitis (n (%)) | 27 (30) | 6 (20) | 21 (34) | 0.228 |
| Cord/cauda equina compression (n (%)) | 32 (35) | 5 (17.2) | 27 (44) | 0.018 * |
| Vertebral instability (n (%)) | 12 (13) | 2 (7) | 10 (16) | 0.325 |
| Microbiological diagnosis | ||||
| Bacteraemia (n (%)) | 47 (52) | 18 (62) | 29 (47) | 0.187 |
| Staphylococcus aureus (n (%)) | 35 (39) | 10 (35) | 25 (40) | 0.649 |
| Risk Factor | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Diabetes mellitus | 5.88 | 1.40–24.68 | 0.008 |
| Frankel grading scale A–D | 4.52 | 1.25–16.39 | 0.019 |
| Duration of symptoms | 1.02 | 1.00–1.04 | 0.019 |
| Spinal cord/cauda equina compression | 6.49 | 1.42–29.70 | 0.009 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widdrington, J.D.; Emmerson, I.; Cullinan, M.; Narayanan, M.; Klejnow, E.; Watson, A.; Ong, E.L.C.; Schmid, M.L.; Price, D.A.; Schwab, U.; et al. Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice. Med. Sci. 2018, 6, 96. https://doi.org/10.3390/medsci6040096
Widdrington JD, Emmerson I, Cullinan M, Narayanan M, Klejnow E, Watson A, Ong ELC, Schmid ML, Price DA, Schwab U, et al. Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice. Medical Sciences. 2018; 6(4):96. https://doi.org/10.3390/medsci6040096
Chicago/Turabian StyleWiddrington, John D., Ingrid Emmerson, Milo Cullinan, Manjusha Narayanan, Eleanor Klejnow, Alistair Watson, Edmund L. C. Ong, Matthias L. Schmid, D. Ashley Price, Ulrich Schwab, and et al. 2018. "Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice" Medical Sciences 6, no. 4: 96. https://doi.org/10.3390/medsci6040096
APA StyleWiddrington, J. D., Emmerson, I., Cullinan, M., Narayanan, M., Klejnow, E., Watson, A., Ong, E. L. C., Schmid, M. L., Price, D. A., Schwab, U., & Duncan, C. J. A. (2018). Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice. Medical Sciences, 6(4), 96. https://doi.org/10.3390/medsci6040096