Current Approaches to the Treatment of Gastric Varices: Glue, Coil Application, TIPS, and BRTO

Abstract
:1. Introduction
2. Treatment
- (1)
- In endoscopic treatment gastric variceal sclerotherapy, gastric variceal band ligation (GVL), glue application with varix occlusion, endoscopic ultrasound (EUS)-guided coil/glue application, thrombin applications or a combination is used.
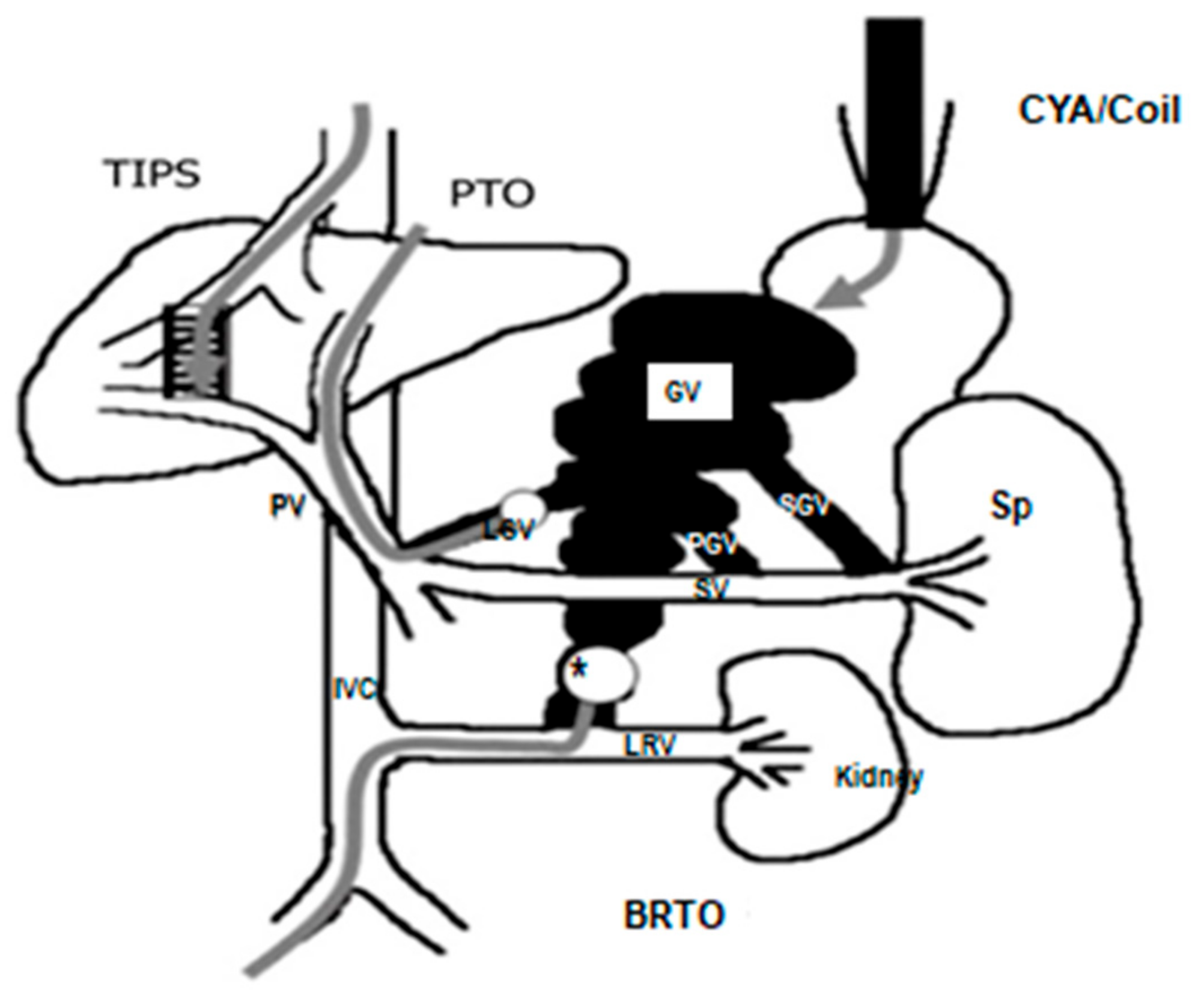
- (2)
- Radiologic treatments include TIPS (transjugular intrahepatic portosystemic shunt) and BRTO (balloon retrograde transvenous obliteration).
Author Contributions
Conflicts of Interest
References
- Garcia-Pagán, J.C.; Barrufet, M.; Cardenas, A.; Escorsell, A. Management of gastric varices. Clin. Gastroenterol. Hepatol. 2014, 12, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Wani, Z.A.; Bhat, R.A.; Bhadoria, A.S.; Maiwall, R.; Choudhury, A. Gastric varices: Classification, endoscopic and ultrasonographic management. J. Res. Med. Sci. 2015, 20, 1200–1207. [Google Scholar] [PubMed]
- Lo, G.H. Endoscopic treatments for portal hypertension. Hepatol. Int. 2018, 12, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.; Mostafa, I.; Devière, J. New Developments in Managing Variceal Bleeding. Gastroenterology 2018, 154, 1964–1969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-J.; Hou, M.-C.; Liao, W.-C.; Chen, P.-H.; Lin, H.-C.; Lee, F.-Y.; Lee, S.-D. Management of acute gastric varices bleeding. J. Chin. Med Assoc. 2013, 76, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Binmoeller, K.F. Endoscopic Ultrasound–Guided Coil and Glue Injection for Gastric Variceal Bleeding. Gastroenterol. Hepatol. 2018, 14, 123–126. [Google Scholar]
- Hwang, J.H.; Shergill, A.K.; Acosta, R.D.; Chandrasekhara, V.; Chathadi, K.V.; Decker, G.A.; Early, D.S.; Evans, J.A.; Fanelli, R.D.; Fisher, D.A.; et al. The role of endoscopy in the management of variceal hemorrhage. American Society for Gastrointestinal Endoscopy. Gastrointest. Endosc. 2014, 80, 221–227. [Google Scholar] [CrossRef]
- Fujii-Lau, L.L.; Law, R.; Wong Kee Song, L.M.; Levy, M.J. Novel techniques for gastric variceal obliteration. Dig. Endosc. 2015, 27, 189–196. [Google Scholar] [CrossRef]
- Mukkada, R.J.; Antony, R.; Chooracken, M.J.; Francis, J.V.; Chettupuzha, A.P.; Mathew, P.G.; Augustine, P.; Koshy, A. Endoscopic ultrasound-guided coil or glue injection in post-cyanoacrylate gastric variceal re-bleed. Indian J. Gastroenterol. 2018, 37, 153–159. [Google Scholar] [CrossRef]
- Jhajharia, A.; Wanjari, S.J.; Ashdhir, P.; Pokharna, R.; Nijhawan, S. Role and safety of human thrombin injection for the treatment of bleeding gastric varices. Indian J. Gastroenterol. 2018, 37, 321–325. [Google Scholar] [CrossRef]
- Frost, J.W.; Hebbar, S. EUS-guided thrombin injection for management of gastric fundal varices. Endosc. Int. Open. 2018, 6, E664–E668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Kumar, A. Endoscopic Treatment of Gastric Varices. Clin. Liver Dis. 2014, 18, 809–827. [Google Scholar] [CrossRef] [PubMed]
- Fujii-Lau, L.L.; Law, R.; Wong Kee Song, L.M.; Gostout, C.J.; Kamath, P.S.; Levy, M.J. Endoscopic ultrasound (EUS)-guided coil injection therapy of esophagogastric and ectopic varices. Surg. Endosc. 2016, 30, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Ríos Castellanos, E.; Seron, P.; Gisbert, J.P.; Bonfill Cosp, X. Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension. Cochrane Database Syst. Rev. 2015, 5, CD010180. [Google Scholar] [CrossRef] [PubMed]
- Jer Hwang, H.; Málaga, I.; Curvale, C.; Guidi, M.; Matano, R. Refractory gastric variceal bleeding treated through endoscopic ultrasound-guided coiling and N-butyl-2-cyanoacrylate application. Rev. Gastroenterol. Mex. 2018. [Google Scholar] [CrossRef]
- Khoury, T.; Nadella, D.; Wiles, A.; Marshall, C.; Kumar, M.; Shapira, G.; Ludvik, N.; Schumann, A.; Mahamid, M.; Mizrahi, M. A review article on gastric varices with focus on the emerging role of endoscopic ultrasound-guided angiotherapy. Eur. J. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, I.; Miraglia, R.; Amata, M.; Ligresti, D.; Cipolletta, F.; Maruzzelli, L.; Traina, M. Endoscopic ultrasound-guided angiotherapy in refractory gastrointestinal bleeding from large isolated gastric varices: A same-session combined approach. Endoscopy 2018, 50, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Pandhi, M.B.; Khabbaz, R.C.; Gaba, R.C.; Lipnik, A.J. Endovascular Treatment for Variceal Hemorrhage: TIPS, BRTO, and Combined Approaches. Semin. Interv. Radiol. 2018, 35, 169–184. [Google Scholar] [CrossRef]
- Kobayakawa, M.; Ohnishi, S.; Suzuki, H. Recent development of balloon-occluded retrograde transvenous obliteration. J. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef]
- Ma, L.L.; Luo, T.C.; Tseng, Y.J.; Huang, X.Q.; Luo, J.J.; Zhang, W.; Li, B.; Chen, S.Y. Balloon-occluded Retrograde Transvenous Obliteration of Portovenous Shunts during Endoscopic Therapy for the Treatment of Gastric Varices. Surg. Laparosc. Endosc. Percutan Tech. 2018. [Google Scholar] [CrossRef]
- Strunk, H.; Marinova, M. Transjugular Intrahepatic Portosystemic Shunt (TIPS): Pathophysiologic Basics, Actual Indications and Results with Review of the Literature. Rofo 2018, 190, 701–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantaka, A.; Tsetis, D.; Hatzidakis, A.; Kouroumalis, E.A.; Samonakis, D.N. Successful management of refractory gastric variceal bleeding via a combined percutaneous approach in sinistral portal hypertension. Gastroenterol. Hepatol. Open Access 2018, 9, 1. [Google Scholar]
- Abraldes, J.G.; Villanueva, C.; Aracil, C.; Turnes, J.; Hernandez-Guerra, M.; Genesca, J.; Rodriguez, M.; Castellote, J.; García-Pagán, J.C.; Torres, F.; et al. Addition of simvastatin to standard therapy for the prevention of variceal rebleeding does not reduce rebleeding but increases survival in patients with cirrhosis. Gastroenterology 2016, 150, 1160–1170. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, R.; Maruzzelli, L.; Di Piazza, A.; Mamone, G.; Caruso, S.; Gentile, G.; Tuzzolino, F.; Floridia, G.; Petridis, I.; Volpes, R.; et al. Transjugular Intrahepatic Portosystemic Shunt Using the New Gore Viatorr Controlled Expansion Endoprosthesis: Prospective, Single-Center, Preliminary Experience. Cardiovasc. Intervent. Radiol. 2019, 42, 78–86. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, C.; Pellicano, C.; Carucci, P.; Bruno, M.; Repici, A.; Goss, M.; Fagoonee, S.; Saracco, G.; Rizzetto, M. Endoscopic ultrasonography in hepatology: Focus on portal hypertension. Minerva Gastroenterol. Dietol. 2008, 54, 131–139. [Google Scholar]
- Kameda, N.; Higuchi, K.; Shiba, M.; Kadouchi, K.; Machida, H.; Okazaki, H.; Tanigawa, T.; Watanabe, T.; Tominaga, K.; Fujiwara, Y.; et al. Management of gastric fundal varices without gastro-renal shunt in 15 patients. World J. Gastroenterol. 2008, 14, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Sabri, S.S.; Saad, W.E.A. Balloon-occluded Retrograde Transvenous Obliteration (BRTO): Technique and Intraprocedural Imaging. Semin. Intervent. Radiol. 2011, 28, 303–313. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Shiozawa, K.; Ikehara, T.; Nakano, S.; Kougame, M.; Otsuka, T.; Kikuchi, Y.; Ishii, K.; Igarashi, Y.; Sumino, Y. Short-Term Effects and Early Complications of Balloon-Occluded Retrograde Transvenous Obliteration for Gastric Varices. Gastroenterology 2012, 2012, 919371. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trade Name | Manufacturer | Active Component | Drug | Polymerization Rate | Lipiodol Requirement |
|---|---|---|---|---|---|
| Indermil | Covidien | N-butyl-2-cyanoacrylate | 05. mL/liquid amp | Fast | yes |
| Cyanoacrylate | TissueSeal | N-butyl-2-cyanoacrylate | 05. mL/liquid amp | Fast | yes |
| Dermabond | Ethicon | 2-Octyl- cyanoacrylate | 05. mL/liquid amp | Slow | no |
| Glubran 2 | GEM, Italy | N-butyl-2-cyanoacrylate + methacryloyloxy sulfolane | 0.25 mL–05 mL and 1 mL/liquid amp | Slow | no |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goral, V.; Yılmaz, N. Current Approaches to the Treatment of Gastric Varices: Glue, Coil Application, TIPS, and BRTO. Medicina 2019, 55, 335. https://doi.org/10.3390/medicina55070335
Goral V, Yılmaz N. Current Approaches to the Treatment of Gastric Varices: Glue, Coil Application, TIPS, and BRTO. Medicina. 2019; 55(7):335. https://doi.org/10.3390/medicina55070335
Chicago/Turabian StyleGoral, Vedat, and Nevin Yılmaz. 2019. "Current Approaches to the Treatment of Gastric Varices: Glue, Coil Application, TIPS, and BRTO" Medicina 55, no. 7: 335. https://doi.org/10.3390/medicina55070335
APA StyleGoral, V., & Yılmaz, N. (2019). Current Approaches to the Treatment of Gastric Varices: Glue, Coil Application, TIPS, and BRTO. Medicina, 55(7), 335. https://doi.org/10.3390/medicina55070335