Distance Special Education Delivery by Social Robots

 ,
, 

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Digital Material for the Asynchronous Sessions
- Information on current events: Emphasis was placed on clarifying the basic information that children need to know about COVID-19 precautions and hygiene measures. At the same time, the areas that parents should pay attention to during the children’s engagement with the material are highlighted by accompanying information leaflets.
- Strengthening resilience: Modern research defines resilience as a dynamic process of positive adjustment of the individual despite the existence of adverse conditions and risks or despite the experience of traumatic events. Therefore, due to the present conditions, the focus on strengthening the protective factors associated with resilience is important [14,15]. The aim of the proposed activities is to accept and empower children, to promote a positive attitude towards the changing circumstances of their daily lives, to strengthen the emotional support they receive through the provision of information that will be given to the family environment, to promote techniques and activities that reduce the sense of isolation, and finally, to maintain coherence in the therapeutic process [16].
- Creative engagement: Although children with ASD may feel more comfortable with social withdrawal, as in the case in a quarantine situation [17], it is also possible that they become distressed by even small changes in their routine, which usually involves multiple activities aimed at developing their skills. One such routine activity was their in-person sessions for the protocol twice a week. Maintaining a routine as much as possible reduces the negative effects and maintains balance in the family (see [18]). In the present conditions, it is even more important to enhance the experiences that promote feelings of enjoyment and satisfaction and adopt activities that calm children and strengthen their sense of control, thus strengthening their independence.
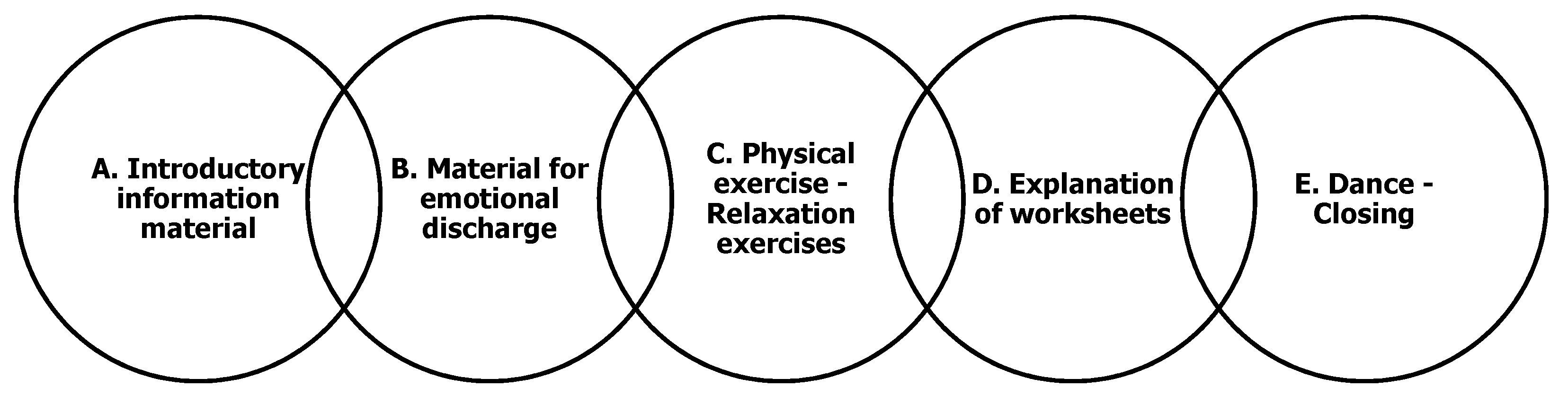
- Introductory information material: The introductory section of the first SIP is dedicated to explaining the current situation, what is the SARS-CoV2 virus and the need to stay at home, and the various steps that need to be taken in order to stay safe. On the other hand, the introductory section of the second SIP encourages the child to describe its life so far, its activities with its family, and advocates the maintenance of a healthy lifestyle through healthy eating and exercise.
- Material for emotional regulation: The second section of the SIP contains material for dealing with boredom and tediousness as well as other negative emotions. The material offers ideas for indoors activities but also offers advice for dealing with negative emotions.
- Physical exercise-Relaxation exercises: Physical exercise and especially coordination and endurance exercises are very effective in children with ASD [19]. Movements similar to those that manifest as stereotyped behavior by children with ASD, appear to be helpful in providing the necessary feedback to the body. This can reduce repetitive behaviors, such as hitting the arm or “flailing” with the upper extremities [20,21]. Research shows that there is a reciprocal relationship between physical exercise and social functionality for people with ASD, reporting better emotional regulation, among other benefits [22,23]. The SIP also contains step-by-step instructions for conducting breathing exercises aiming at relaxation, which can also be used when the child becomes emotionally overwhelmed.
- Explanation of worksheets: This section of the SIP includes information and instructions for both children, parents/caregivers on how to use the accompanying worksheets. Included in this section are the optional questionnaires where, at the end of the process, parents can provide feedback regarding the support material and record their children’s response to it, even though a telephone interview was preferred, as will be explained later. Additionally, the section includes information targeted specifically to parents with advice on how to communicate effectively with the child, explanations for the material provided in the RIS and advice on how to appropriately respond to any difficult behaviors that may occur.
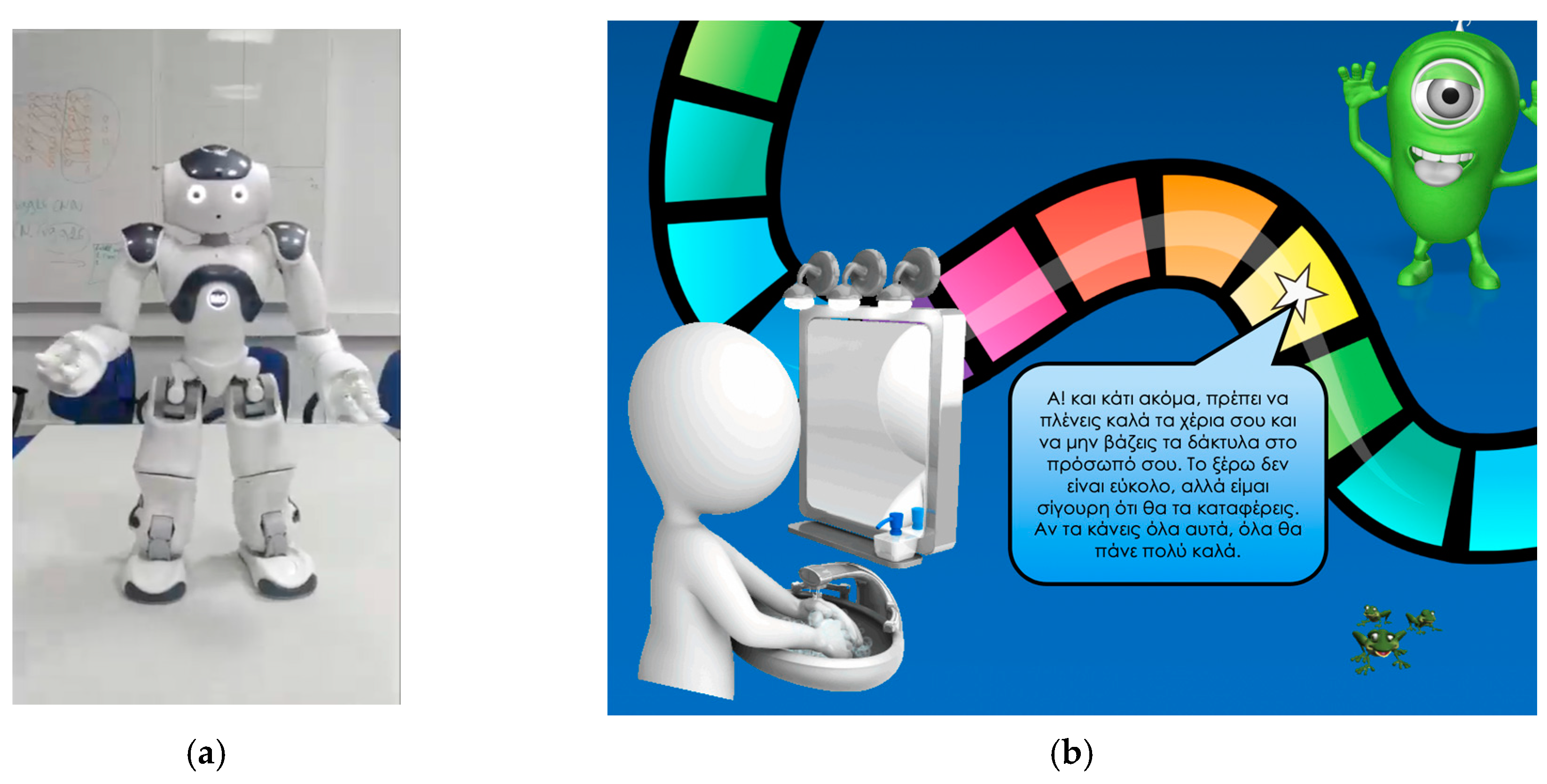
- Dance-Closing: In this section the importance of the washing of the hands is explained and the process is demonstrated using graphics and video. The end of the section is marked by a visually appealing dance.
2.2. Educational Scenario for the Synchronous Sessions
- Greeting: The robot greets the child using gestures and gives instructions on how to conduct the video call. Instructions include the way the child should stand in front of the camera and how the child should speak so that effective visual and auditory interaction can be achieved.
- Communication skills: For the second part of the scenario, the robot initiates an imitation exercise designed to determine if the child remembers the imitation skills obtained during the in-person sessions. At the same time, the scenario is attempting to teach the child how to conduct itself in light of the special circumstances of the pandemic. For this reason, embedded in the actions to be imitated are explanations why these actions are needed. For example, the child is shown how to say hello from a distance using gestures, or explanations why wearing a mask is needed.
- Dance: The robot asks the child whether it wants it to perform a dance and requests that the child replicates the movements as an exercise. The dance is chosen from the list of dances that are actually part of the original intervention scenario, so that the child is already familiar with the movements and music.
- Relaxation: The relaxation scenario involves breathing exercises guided by the robot, conducted in the same manner as the in-person meetings. At the end of the relaxation activity, the robot says goodbye and the session is concluded by the therapist.
2.3. Implementation on the Robot
2.4. Evaluation Method
3. Results
3.1. Asynchronous Sessions
3.2. Synchronous Sessions
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Leite, I.; Martinho, C.; Paiva, A. Social Robots for Long-Term Interaction: A Survey. Int. J. Soc. Robot. 2013, 5, 291–308. [Google Scholar] [CrossRef]
- Mubin, O.; Stevens, C.J.; Shahid, S.; Mahmud, A.A.; Dong, J.-J. A Review of the Applicability of Robots in Education. Technol. Educ. Learn. 2013, 1. [Google Scholar] [CrossRef] [Green Version]
- Belpaeme, T.; Kennedy, J.; Ramachandran, A.; Scassellati, B.; Tanaka, F. Social robots for education: A review. Sci. Robot. 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Martin, E.; Escalona, F.; Cazorla, M. Socially Assistive Robots for Older Adults and People with Autism: An Overview. Electronics 2020, 9, 367. [Google Scholar] [CrossRef] [Green Version]
- Lytridis, C.; Bazinas, C.; Papakostas, G.A.; Kaburlasos, V. On Measuring Engagement Level During Child-Robot Interaction in Education. In Advances in Intelligent Systems and Computing; Merdan, M., Lepuschitz, W., Koppensteiner, G., Balogh, R., Obdržálek, D., Eds.; Springer: Cham, Switzerland; Vienna, Austria, 2020; Volume 1023, pp. 3–13. ISBN 9783030269449. [Google Scholar]
- Pachidis, T.; Vrochidou, E.; Kaburlasos, V.G.; Kostova, S.; Bonković, M.; Papić, V. Social Robotics in Education: State-of-the-Art and Directions. In Advances in Service and Industrial Robotics; Springer: Cham, The Netherlands, 2019; Volume 67, pp. 689–700. [Google Scholar]
- Kaburlasos, V.G.; Vrochidou, E. Social Robots for Pedagogical Rehabilitation: Trends and Novel Modeling Principles. In Cyber-Physical Systems for Social Applications; Advances in Systems Analysis, Software Engineering, and High Performance Computing (ASASEHPC); Dimitrova, M., Wagatsuma, H., Eds.; IGI Global: Hershey, PA, USA, 2019; pp. 1–21. [Google Scholar]
- Pachidis, T.P.; Vrochidou, E.; Kaburlasos, V.; Kostova, S.; Bonkovic, M.; Papić, V. Social Robots as Tools in Special Education (SRTSE). In National Strategic Reference Framework, 2014–2020; Ministry of Economy and Finance: Athens, Greece, 2018; Project no. Τ1ΕΔΚ-00929 2018. [Google Scholar]
- American Psychiatric Association DSM-5 Diagnostic Classification. In Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013.
- Blackman, A.L.; Jimenez-Gomez, C.; Shvarts, S. Comparison of the efficacy of online versus in-vivo behavior analytic training for parents of children with autism spectrum disorder. Behav. Anal. Res. Pract. 2020, 20, 13–23. [Google Scholar] [CrossRef]
- Ferguson, J.; Craig, E.A.; Dounavi, K. Telehealth as a Model for Providing Behaviour Analytic Interventions to Individuals with Autism Spectrum Disorder: A Systematic Review. J. Autism Dev. Disord. 2019, 49, 582–616. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, R.; Trembath, D.; Hodge, M.A.; Rose, V.; Roberts, J. Telehealth and autism: Are telehealth language assessments reliable and feasible for children with autism? Int. J. Lang. Commun. Disord. 2019, 54, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Holeva, V.; Nikopoulou, V.-A.; Papadopoulou, M.; Vrochidou, E.; Papakostas, G.A.; Kaburlasos, V.G. Toward Robot-Assisted Psychosocial Intervention for Children with Autism Spectrum Disorder (ASD). In Lecture Notes in Computer Science, Proceedings of the Social Robotics, Madrid, Spain, 26–29 November 2019; Salichs, M.A., Ge, S.S., Barakova, E.I., Cabibihan, J.-J., Wagner, A.R., Castro-González, Á., He, H., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 484–493. [Google Scholar]
- Kaboski, J.; McDonnell, C.G.; Valentino, K. Resilience and Autism Spectrum Disorder: Applying Developmental Psychopathology to Optimal Outcome. Rev. J. Autism Dev. Disord. 2017. [Google Scholar] [CrossRef]
- Szatmari, P. Risk and resilience in autism spectrum disorder: A missed translational opportunity? Dev. Med. Child. Neurol. 2018, 60, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Purkis, Y.; Goodall, E.; Nugent, J. The Guide to Good Mental Health on the Autism Spectrum; Jessica Kingsley Publishers: London, UK, 2016. [Google Scholar]
- Minnesota’s First Autism Resource Autism Society of Minnesota Guide to Managing Self-Quarantine and Social Distancing. Available online: https://ausm.org/images/docs/PandemicGuideforASDAdults2020.pdf (accessed on 10 March 2020).
- Hume, K.; Waters, V.; Sam, A.; Steinbrenner, J.; Perkins, Y.; Dees, B.; Tomaszewski, B.; Rentschler, L.; Szendrey, S.; McIntyre, N.; et al. Supporting Individuals with Autism through Uncertain Times; UNC FPG Child Development Institute Autism Team: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Toscano, C.V.A.; Carvalho, H.M.; Ferreira, J.P. Exercise Effects for Children With Autism Spectrum Disorder: Metabolic Health, Autistic Traits, and Quality of Life. Percept. Mot. Skills 2018, 125, 126–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.; Koegel, L.K.; Ashbaugh, K.; Regester, A.; Ence, W.; Smith, W. Physical exercise and individuals with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2010, 4, 565–576. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Ghiarone, T.; Júnior, C.R.C.; Furtado, G.E.; Carvalho, H.M.; Machado-Rodrigues, A.M.; Toscano, C.V.A. Effects of Physical Exercise on the Stereotyped Behavior of Children with Autism Spectrum Disorders. Medicina (B Aires) 2019, 55, 685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinders, N.J.; Branco, A.; Wright, K.; Fletcher, P.C.; Bryden, P.J. Scoping Review: Physical Activity and Social Functioning in Young People With Autism Spectrum Disorder. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, S.; Nacario, A.; Braithwaite, R.E.; Hopper, C. The effect of physical activity interventions on youth with autism spectrum disorder: A meta-analysis. Autism Res. 2018, 11, 818–833. [Google Scholar] [CrossRef] [PubMed]
- Autism Society COVID-19 Preparedness and Resources. Available online: https://www.autism-society.org/news/covid-19-preparedness-and-resources/ (accessed on 10 March 2020).
- Autism Speaks COVID-19 Information and Resources. Available online: https://www.autismspeaks.org/covid-19-information-and-resources (accessed on 10 March 2020).
- Psygrams Ideas in Words. Available online: http://www.psygrams.com/ (accessed on 10 March 2020).
- Zoom Video Communications, I. Video Conferencing, Web Conferencing, Webinars, Screen Sharing Software; Zoom: San Jose, CA, USA, 2019; Available online: https://www.troopmessenger.com/blogs/video-conferencing (accessed on 10 March 2020).
- IBM Corp SPSS Statistics. Version 26.0; IBM Software Business Analysis; IBM Corp: Armonk, NY, USA, 2019.
- Pennisi, P.; Tonacci, A.; Tartarisco, G.; Billeci, L.; Ruta, L.; Gangemi, S.; Pioggia, G. Autism and social robotics: A systematic review. Autism Res. 2016, 9, 165–183. [Google Scholar] [CrossRef] [PubMed]
- Syriopoulou-Delli, C.K.; Gkiolnta, E. Review of assistive technology in the training of children with autism spectrum disorders. Int. J. Dev. Disabil. 2020, 1–13. [Google Scholar] [CrossRef]
- Diehl, J.J.; Schmitt, L.M.; Villano, M.; Crowell, C.R. The clinical use of robots for individuals with Autism Spectrum Disorders: A critical review. Res. Autism Spectr. Disord. 2012, 6, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | Robot-Assisted Group |
|---|---|
| visualized material in the form of a presentation | visualized material with the NAO robot |
| digitized material with children’s activities | digitized material with activities involving the NAO robot |
| information leaflets for parents | information leaflets for parents |
| Questions |
|---|
| 1. How would you rate you child’s satisfaction in relation to the Supporting Information Package you received? |
| 2. How would you rate your satisfaction in relation to the Supporting Information Package you received? |
| 3. How would you rate your child’s engagement in relation to the Supporting Information Package you received? Could you give me an example? |
| 4. How would you rate the usefulness of the supplemental activities you received? |
| 5. How would you rate your child’s feeling of connectedness to the intervention procedure after the Supporting Information Package you received a. Did he/she mention the robot’s or therapist’s name? b. Did he/she mention anything related to the intervention? |
| 6. Please rate your satisfaction in receiving the upcoming Supporting Information Packages. |
| Variables | Group | n | M | S.D. | Std. Error Mean | t |
|---|---|---|---|---|---|---|
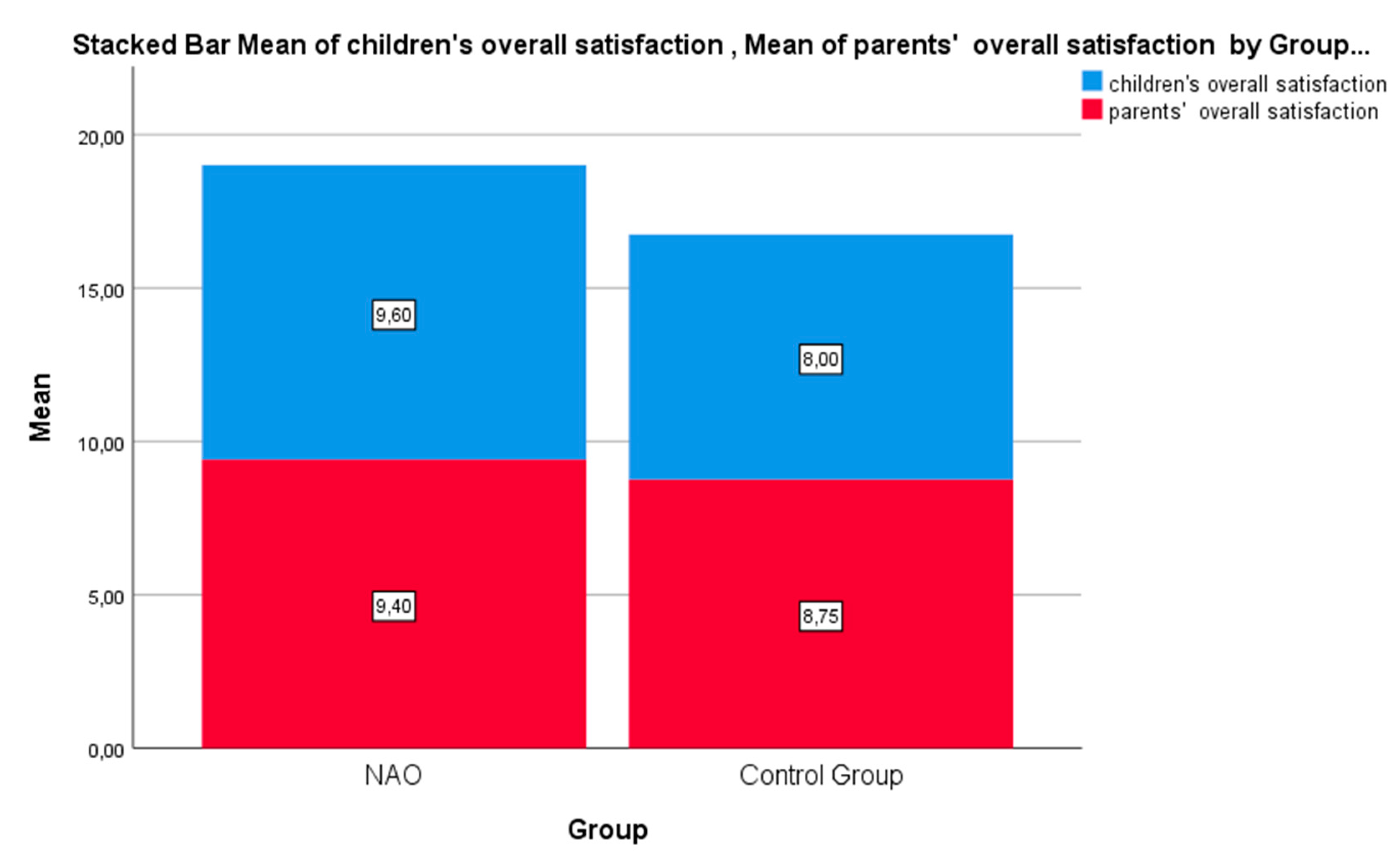
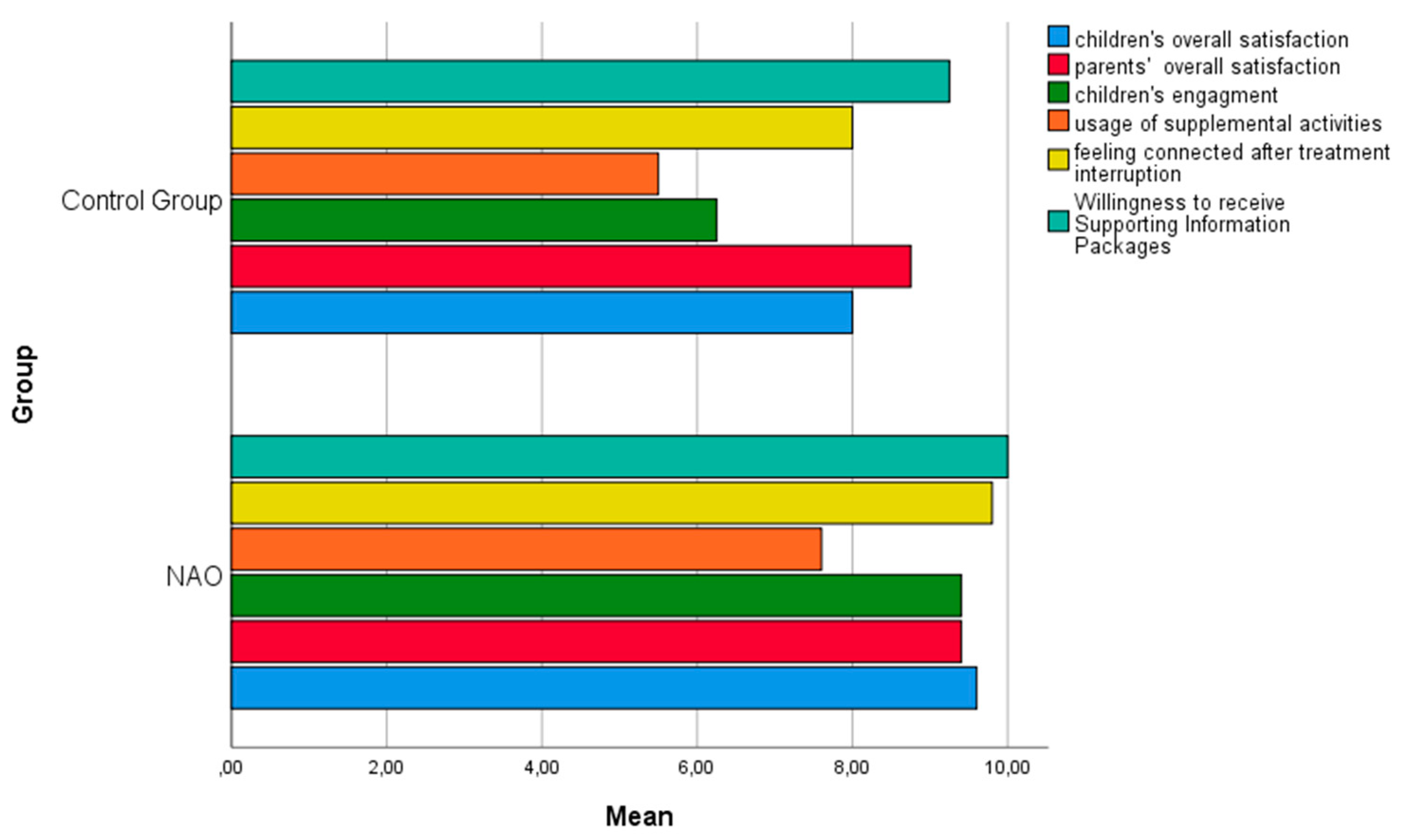
| Children’s overall satisfaction | NAO | 5 | 9.60 | 0.54 | 0.24 | 1.61 |
| Control Group | 4 | 8.00 | 2.16 | 1.08 | p > 0.001 | |
| Parents’ overall satisfaction | NAO | 5 | 9.40 | 0.54 | 0.24 | 1.05 |
| Control Group | 4 | 8.75 | 1.25 | 0.62 | p > 0.001 | |
| Children’s Engagement | NAO | 5 | 9.40 | 0.89 | 0.40 | 2.27 |
| Control Group | 4 | 6.25 | 2.98 | 1.49 | p > 0.001 | |
| Usage of Supplemental Activities | NAO | 5 | 7.60 | 1.14 | 0.50 | 1.19 |
| Control Group | 4 | 5.50 | 3.78 | 1.89 | p > 0.001 | |
| Feeling connected after treatment interruption | NAO | 5 | 9.80 | 0.44 | 0.20 | 2.39 |
| Control Group | 4 | 8.00 | 1.63 | 0.816 | p = 0.048 | |
| Willingness to receive Supporting Information Packages | NAO | 5 | 10.00 | 0.00 | 0.00 | 1.78 |
| Control Group | 4 | 9.25 | 0.95 | 0.47 | p > 0.001 |
| Variables | Session | n | M (SD) | Mea Dif. (SD) | S. E. Mean Dif. | t | p Value |
|---|---|---|---|---|---|---|---|
| Pair 1: Children’s overall satisfaction | Video | 5 | 9.50 (0.57) | 1.75 (2.36) | 1.81 | 1.48 | 0.235 |
| Zoom | 5 | 7.75 (0.18) | - | 4 | - | - | |
| Pair 2: Parents’ overall satisfaction | NAO | 5 | 9.40 (0.54) | 0.80 (1.92) | 0.86 | 1.05 | 0.405 |
| Zoom | 5 | 8.60 (1.67) | - | - | - | - | |
| Pair 3: Children’s Engagement | NAO | 5 | 9.25 (0.95) | - | - | - | - |
| Zoom | 5 | 9.25 (0.95) | - | - | - | - | |
| Pair 4: Feeling connected after treatment interruption | NAO | 5 | 9.75 (0.50) | −0.25 (0.50) | 0.25 | 2.39 | 0.391 |
| Zoom | 5 | 10.00 (0.00) | - | 0 | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lytridis, C.; Bazinas, C.; Sidiropoulos, G.; Papakostas, G.A.; Kaburlasos, V.G.; Nikopoulou, V.-A.; Holeva, V.; Evangeliou, A. Distance Special Education Delivery by Social Robots. Electronics 2020, 9, 1034. https://doi.org/10.3390/electronics9061034
Lytridis C, Bazinas C, Sidiropoulos G, Papakostas GA, Kaburlasos VG, Nikopoulou V-A, Holeva V, Evangeliou A. Distance Special Education Delivery by Social Robots. Electronics. 2020; 9(6):1034. https://doi.org/10.3390/electronics9061034
Chicago/Turabian StyleLytridis, Chris, Christos Bazinas, George Sidiropoulos, George A. Papakostas, Vassilis G. Kaburlasos, Vasiliki-Aliki Nikopoulou, Vasiliki Holeva, and Athanasios Evangeliou. 2020. "Distance Special Education Delivery by Social Robots" Electronics 9, no. 6: 1034. https://doi.org/10.3390/electronics9061034
APA StyleLytridis, C., Bazinas, C., Sidiropoulos, G., Papakostas, G. A., Kaburlasos, V. G., Nikopoulou, V.-A., Holeva, V., & Evangeliou, A. (2020). Distance Special Education Delivery by Social Robots. Electronics, 9(6), 1034. https://doi.org/10.3390/electronics9061034