Evaluation of SARS-CoV-2 Serological Testing in Patients with Multiple Myeloma and Other Hematologic Malignancies on Monoclonal Antibody Therapies

Abstract
:1. Introduction
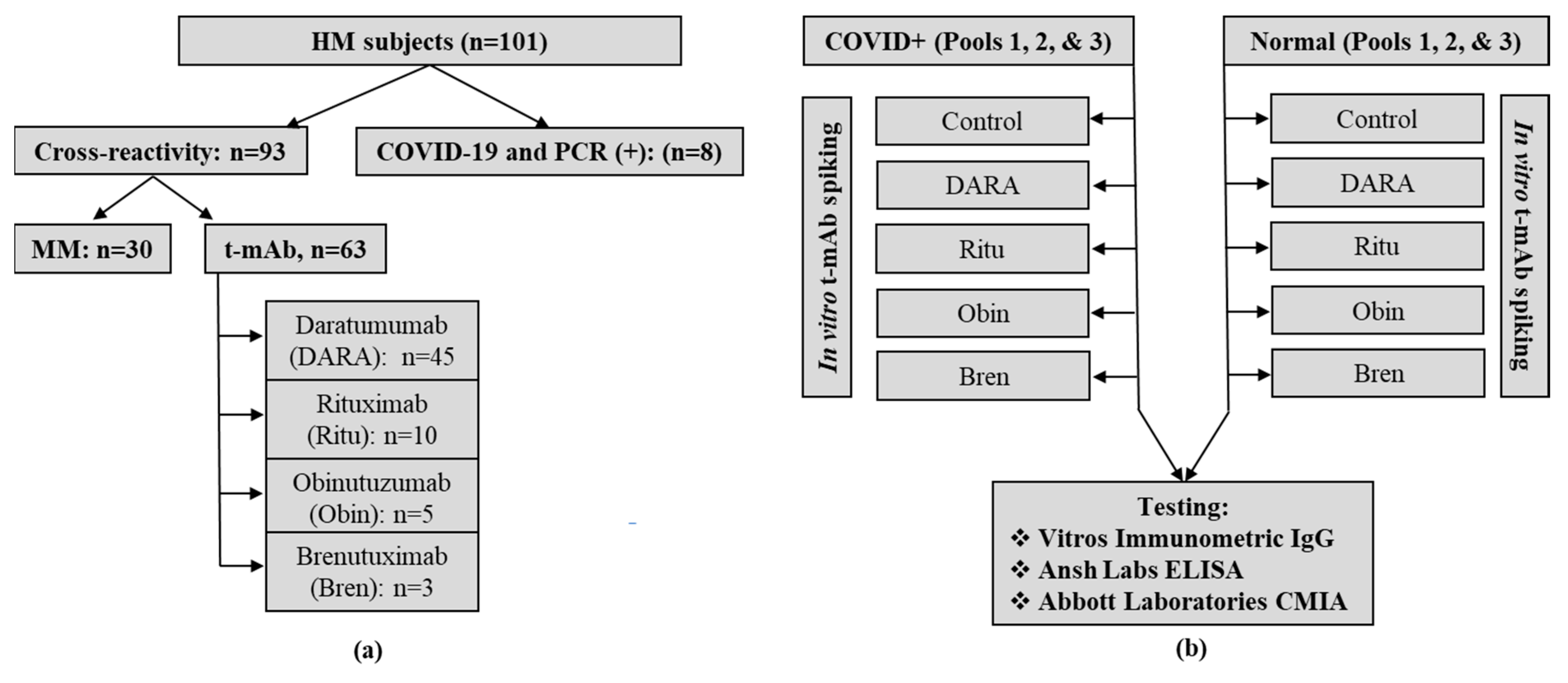
2. Materials and Methods
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lee, L.Y.W.; Cazier, J.-B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, A.N.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [PubMed]
- He, W.; Chen, L.; Yuan, G.; Fang, Y.; Chen, W.; Wu, D.; Liang, B.; Lu, X.; Ma, Y.; Li, L.; et al. COVID-19 in persons with haematological cancers. Leukemia 2020, 34, 1637–1645. [Google Scholar] [PubMed]
- Aries, J.A.; Davies, J.K.; Auer, R.L.; Hallam, S.L.; Montoto, S.; Smith, M.; Sevillano, B.; Foggo, V.; Wrench, B.; Zegocki, K.; et al. Clinical outcome of coronavirus disease 2019 in haemato-oncology patients. Br. J. Haematol. 2020, 190, e64–e67. [Google Scholar] [PubMed]
- Lee, S.J.; Borrello, I. Role of the immune response in disease progression and therapy in multiple myeloma. Cancer Treat. Res. 2016, 169, 207–225. [Google Scholar] [PubMed]
- Kumar, S.K.; Anderson, K.C. Immune therapies in multiple myeloma. Clin. Cancer Res. 2016, 22, 5453–5460. [Google Scholar] [PubMed] [Green Version]
- Blimark, C.; Holmberg, E.; Mellqvist, U.-H.; Landgren, O.; Björkholm, M.; Hultcrantz, M.; Kjellander, C.; Turesson, I.; Kristinsson, S.Y. Multiple myeloma and infections: a population-based study on 9253 multiple myeloma patients. Haematologica 2015, 100, 107–113. [Google Scholar] [PubMed] [Green Version]
- Wang, B.; Van Oekelen, O.; Mouhieddine, T.H.; Del Valle, D.M.; Richter, J.; Cho, H.J.; Richard, S.; Chari, A.; Gnjatic, S.; Merad, M.; et al. A tertiary center experience of multiple myeloma patients with COVID-19: lessons learned and the path forward. J. Hematol. Oncol. 2020, 13, 94. [Google Scholar] [PubMed]
- Cook, G.; Ashcroft, A.J.; Pratt, G.; Popat, R.; Ramasamy, K.; Kaiser, M.; Jenner, M.; Henshaw, S.; Hall, R.; Sive, J.; et al. Real-world assessment of the clinical impact of symptomatic infection with severe acute respiratory syndrome coronavirus (COVID-19 disease) in patients with multiple myeloma receiving systemic anti-cancer therapy. Br. J. Haematol. 2020, 190, e83–e86. [Google Scholar]
- Long, Q.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar]
- King, R.I.; Florkowski, C.M. How paraproteins can affect laboratory assays: spurious results and biological effects. Pathology 2010, 42, 397–401. [Google Scholar] [PubMed]
- Willrich, M.A.V.; Ladwig, P.M.; Andreguetto, B.D.; Barnidge, D.R.; Murray, D.L.; Katzmann, A.J.; Snyder, M.R. Monoclonal antibody therapeutics as potential interferences on protein electrophoresis and immunofixation. Clin. Chem. Lab. Med. 2016, 54, 1085–1093. [Google Scholar]
- McDonald, S.; Courtney, D.M.; Clark, A.E.; Muthukumar, A.; Lee, F.; Balani, J.; Mahimainathan, L.; Bararia, A.; Oliver, D.; Sarode, R.; et al. Diagnostic performance of a rapid point-of-care test for SARS-CoV-2 in an urban emergency department setting. Acad. Emerg. Med. 2020, 27, 764–766. [Google Scholar]


{kind=link}
| (a) | |||||||||||||
| Specimen | Vitros Immunodiagnostics | Ansh Labs | Abbott Laboratories | ||||||||||
| Result | Interpretation | Result | Interpretation | Result | Interpretation | ||||||||
| MM (n = 30) mean ± SD | 0.030 ± 0.009 | NR | 2.107 ± 0.842 | NR | 0.030 ± 0.081 | Neg | |||||||
| HM + t-mAb (n = 63) mean ± SD | DARA (n = 45) | 0.026 ± 0.007 | NR | 2.393 ± 1.130 | NR | 0.028 ± 0.084 | Neg | ||||||
| Ritu (n = 10) | 0.040 ± 0.012 | NR | 2.360 ± 1.313 | NR | 0.067 ± 0.156 | Neg | |||||||
| Obin (n = 5) | 0.042 ± 0.019 | NR | 2.640 ± 1.165 | NR | 0.080 ± 0.140 | Neg | |||||||
| Bren (n = 3) | 0.050 ± 0.010 | NR | 1.700 ± 0.721 | NR | 0.027 ± 0.015 | Neg | |||||||
| HM + CoV (n = 8) Index or Unit (*) | Patient #1 | 10.2 | R | 10.2 | INT | 1.80 | Pos | ||||||
| Patient #2 | 211 | R | 211 | R | 5.65 | Pos | |||||||
| Patient #3 | 840 | R | 118.98 | R | 7.12 | Pos | |||||||
| Patient #4 | 770 | R | 95.55 | R | 7.32 | Pos | |||||||
| Patient #5 | 810 | R | 130.72 | R | 8.11 | Pos | |||||||
| Patient #6 | 940 | R | 132.42 | R | 7.62 | Pos | |||||||
| Patient #7 | 590 | R | 82.97 | R | 7.58 | Pos | |||||||
| Patient #8 | 620 | R | 34.71 | R | 7.05 | Pos | |||||||
| (b) | |||||||||||||
| Assay Type | Pooled Normal Samples—Index/Unit (Non-Reactive/Negative) | Pooled COVID-19 Samples—Index/Unit (Reactive/Positive) | |||||||||||
| Control | DARA | Ritu | Obin | Bren | Control | DARA | Ritu | Obin | Bren | ||||
| Vitros Immuno-diagnostics | 1 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 135 | 154 | 196 | 137 | 158 | ||
| 2 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 11.5 | 10.9 | 11.0 | 10.9 | 12.1 | |||
| 3 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 460 | 442 | 448 | 448 | 437 | |||
| Ansh Labs | 1 | 1.6 | 1.3 | 1.1 | 2.1 | 3.1 | 98.80 | 96.79 | 85.04 | 100.16 | 81.20 | ||
| 2 | 2.5 | 3.1 | 2.5 | 1.3 | 2.1 | 15.84 | 14.00 | 13.64 | 16.66 | 13.43 | |||
| 3 | 2.4 | 3.1 | 1.5 | 3.6 | 4.1 | 95.16 | 101.68 | 97.32 | 105.14 | 94.67 | |||
| Abbott Laboratories | 1 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 6.89 | 6.89 | 7.15 | 6.89 | 7.03 | ||
| 2 | 0.08 | 0.08 | 0.07 | 0.08 | 0.08 | 1.86 | 1.90 | 1.79 | 1.83 | 1.84 | |||
| 3 | 0.07 | 0.07 | 0.07 | 0.07 | 0.08 | 6.35 | 6.24 | 6.45 | 6.41 | 6.33 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahimainathan, L.; Narasimhan, M.; Corchado, R.; Patel, H.; Kansagra, A.; Devaraj, S.; Geethakumari, P.R.; Muthukumar, A. Evaluation of SARS-CoV-2 Serological Testing in Patients with Multiple Myeloma and Other Hematologic Malignancies on Monoclonal Antibody Therapies. Diagnostics 2020, 10, 992. https://doi.org/10.3390/diagnostics10120992
Mahimainathan L, Narasimhan M, Corchado R, Patel H, Kansagra A, Devaraj S, Geethakumari PR, Muthukumar A. Evaluation of SARS-CoV-2 Serological Testing in Patients with Multiple Myeloma and Other Hematologic Malignancies on Monoclonal Antibody Therapies. Diagnostics. 2020; 10(12):992. https://doi.org/10.3390/diagnostics10120992
Chicago/Turabian StyleMahimainathan, Lenin, Madhusudhanan Narasimhan, Rolando Corchado, Hetalkumari Patel, Ankit Kansagra, Sridevi Devaraj, Praveen Ramakrishnan Geethakumari, and Alagarraju Muthukumar. 2020. "Evaluation of SARS-CoV-2 Serological Testing in Patients with Multiple Myeloma and Other Hematologic Malignancies on Monoclonal Antibody Therapies" Diagnostics 10, no. 12: 992. https://doi.org/10.3390/diagnostics10120992
APA StyleMahimainathan, L., Narasimhan, M., Corchado, R., Patel, H., Kansagra, A., Devaraj, S., Geethakumari, P. R., & Muthukumar, A. (2020). Evaluation of SARS-CoV-2 Serological Testing in Patients with Multiple Myeloma and Other Hematologic Malignancies on Monoclonal Antibody Therapies. Diagnostics, 10(12), 992. https://doi.org/10.3390/diagnostics10120992