
Left Ventricular and Atrial Deformation in Patients with Acute Decompensated Heart Failure: A Pilot Study

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design
- History of chronic heart failure fulfilling the ESC diagnostic criteria [6];
- Presence of HF signs and symptoms severe enough to seek urgent medical aid (not manageable with short-term ambulatory intravenous diuretic therapy);
- NT-proNBP levels ≥ 125 ng/L on admission;
- Good imaging quality on echocardiography allowing for the performance of 2D ST analysis;
- No end-stage kidney or liver disease, recent (last 6 months) or disabling stroke or active malignancy.
- No history of cardiovascular disease;
- No medication affecting the cardiovascular system;
- No family history of cardiovascular disease before the age of 65 years;
- Normal serum NT-proBNP levels;
- Sinus rhythm with no abnormalities on ECG;
- No evidence of structural heart disease on echocardiography.
2.2. Echocardiography and 2D ST Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients and Controls
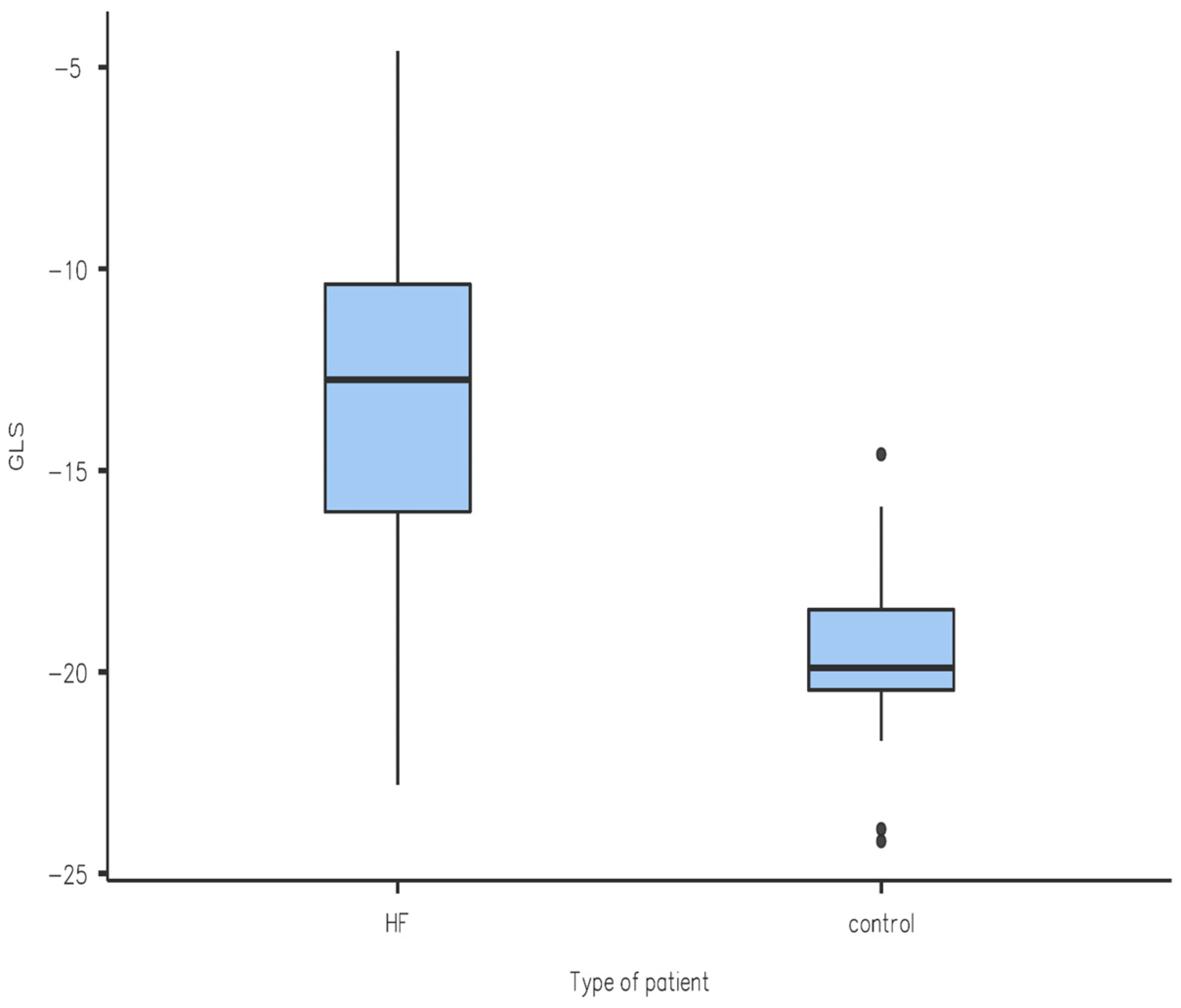
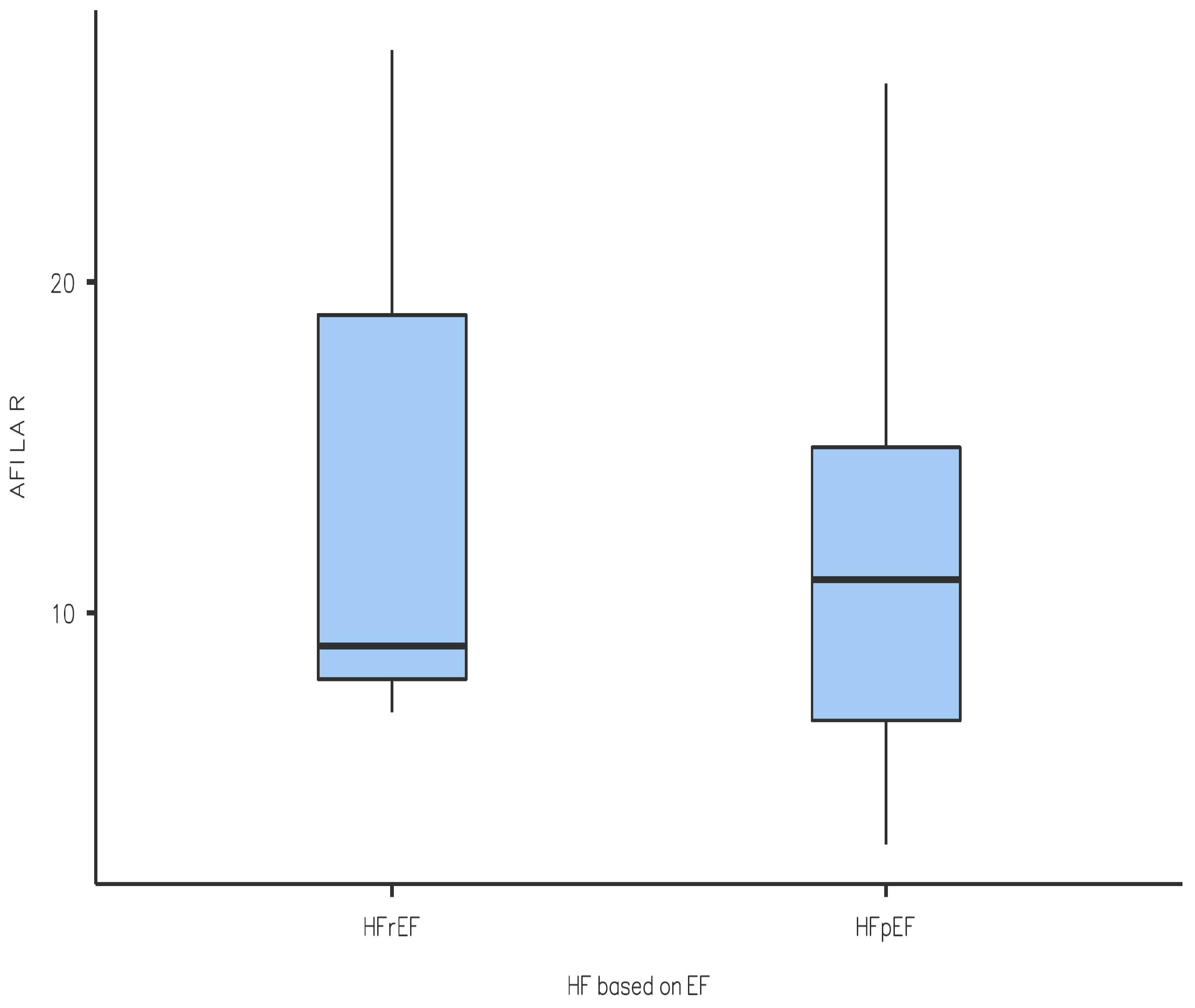
3.2. 2D Speckle-Tracking Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jin, X.; Nauta, J.F.; Hung, C.L.; Ouwerkerk, W.; Teng, T.K.; Voors, A.A.; Lam, C.S.; van Melle, J.P. Left atrial structure and function in heart failure with reduced (HFrEF) versus preserved ejection fraction (HFpEF): Systematic review and meta-analysis. Heart Fail. Rev. 2022, 27, 1933–1955. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Negishi, T.; Somerset, E.; Negishi, K.; Penicka, M.; Lemieux, J.; Aakhus, S.; Miyazaki, S.; Shirazi, M.; Galderisi, M.; et al. SUCCOUR Investigators. Strain-guided management of potentially cardiotoxic cancer therapy. J. Am. Coll. Cardiol. 2021, 77, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Dal Canto, E.; Remmelzwaal, S.; Van Ballegooijen, A.J.; Handoko, M.L.; Heymans, S.; Van Empel, V.; Paulus, W.J.; Nijpels, G.; Elders, P.; Beulens, J.W.J. Diagnostic value of echocardiographic markers for diastolic dysfunction and heart failure with preserved ejection fraction. Heart Fail. Rev. 2022, 27, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.V.; Obokata, M.; Egbe, A.; Yang, J.H.; Pislaru, S.; Lin, G.; Carter, R.; Borlaug, B.A. Left atrial strain and compliance in the diagnostic evaluation of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Galli, E.; Schnell, F. Left Atrial Strain: A Must or a Plus for Routine Clinical Practice? Circ. Cardiovasc. Imaging 2017, 10, e007023. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. 2016–2018 EACVI Scientific Documents Committee 2016–2018 EACVI Scientific Documents Committee. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar] [PubMed]
- Bshiebish HA, H.; Al-Musawi, A.H.; Khudeir, S.A. Role of global longitudinal strain in assessment of left ventricular systolic function in patients with heart failure with preserved ejection fraction. J. Saudi Heart Assoc. 2019, 31, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Lam CS, P.; Voors, A.A.; de Boer, R.A.; Solomon, S.D.; van Veldhuisen, D.J. Heart failure with preserved ejection fraction: From mechanisms to therapies. Eur. Heart J. 2018, 39, 2780–2792. [Google Scholar] [CrossRef] [PubMed]
- Deferm, S.; Martens, P.; Verbrugge, F.H.; Bertrand, P.B.; Dauw, J.; Verhaert, D.; Dupont, M.; Vandervoort, P.M.; Mullens, W. LA Mechanics in Decompensated Heart Failure: Insights From Strain Echocardiography with Invasive Hemodynamics. JACC Cardiovasc. Imaging 2020, 13, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Zairi, I.; Bejar, M.A.; Ben Mrad, I.; Mzoughi, K.; Kraiem, S. Prognostic value of atrial strain in non-ischemic dilated cardiomyopathy. Tunis. Med. 2021, 99, 644–651. [Google Scholar] [PubMed]
- Katogiannis, K.; Thymis, J.; Kousathana, F.; Pavlidis, G.; Korakas, E.; Kountouri, A.; Balampanis, K.; Prentza, V.; Kostelli, G.; Michalopoulou, H.; et al. Effects of Liraglutide, Empagliflozin and Their Combination on Left Atrial Strain and Arterial Function. Medicina 2024, 60, 395. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HFrEF Subgroup | HFpEF Subgroup | Control Group | |
|---|---|---|---|
| Number of patients (men/women) | 6 (5/1) | 10 (6/4) | 16 (13/3) |
| Age | 71 (56–78) | 76 (64–84) | 32 (20–54) |
| Beta-blockers at admission/upon release (%) | 83.3/100 | 80/80 | 0 |
| ACE inhibitors, AT1RB, ARNI at admission/upon release (%) | 33.3/66.7 | 70/80 | 0 |
| MRA at admission/upon release (%) | 83.3/100 | 30/70 | 0 |
| SGLT2i at admission/upon release (%) | 16.7/16.7 | 0/0 | 0 |
| CRT at admission/upon release (%) | 0/0 | 0/0 | 0 |
| Digoxin at admission/upon release (%) | 33.3/33.3 | 30/30 | 0 |
| Loop diuretics at admission/upon release (%) | 83.3/100 | 60/100 | 0 |
| BMI (kg/m2) | 28 ± 5.4 | 26.7 ± 4.3 | 24.9 ± 3.5 |
| Serum creatinine (µmol/L) | 100.7 ± 35.3 | 133.7 ± 117.5 | 80.3 ± 11.2 |
| GFR calculated using Cockroft–Gault equation (mL/min/1.73 m2) | 67.5 ± 23.2 | 58.3 ± 31.7 | N/E |
| ALT (µkat/L) | 0.47 ± 0.28 | 0.38 ± 0.24 | N/E |
| AST (µkat/L) | 0.61 ± 0.30 | 0.53 ± 0.25 | N/E |
| NT-proBNP (pg/mL) | 7153.1 ± 7254.4 | 8453.2 ± 6032.0 | 46.0 ± 9.4 |
| Hemoglobin (g/L) | 130.6 ± 15.9 | 115.3 ± 8.9 | N/E |
| Total serum protein (g/L) | 60.2 ± 15.8 | 63.1 ± 8.1 | N/E |
| EF LV (%) | 30.5 ± 9.2 | 50.3 ± 6.9 | 58.6 ± 1.1 |
| Myocardial revascularization (%) | 50 | 33 | 0 |
| History of MI (%) | 66.7 | 33 | 0 |
| Atrial fibrillation (%) | 50 | 60 | 0 |
| Valve disease—moderate to severe (%) | 83.3 | 50 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurica, J.; Péč, M.J.; Cingel, M.; Bolek, T.; Barbierik Vachalcová, M.; Horná, S.; Galajda, P.; Mokáň, M.; Samoš, M. Left Ventricular and Atrial Deformation in Patients with Acute Decompensated Heart Failure: A Pilot Study. Diagnostics 2024, 14, 1368. https://doi.org/10.3390/diagnostics14131368
Jurica J, Péč MJ, Cingel M, Bolek T, Barbierik Vachalcová M, Horná S, Galajda P, Mokáň M, Samoš M. Left Ventricular and Atrial Deformation in Patients with Acute Decompensated Heart Failure: A Pilot Study. Diagnostics. 2024; 14(13):1368. https://doi.org/10.3390/diagnostics14131368
Chicago/Turabian StyleJurica, Jakub, Martin Jozef Péč, Marek Cingel, Tomáš Bolek, Marianna Barbierik Vachalcová, Simona Horná, Peter Galajda, Marián Mokáň, and Matej Samoš. 2024. "Left Ventricular and Atrial Deformation in Patients with Acute Decompensated Heart Failure: A Pilot Study" Diagnostics 14, no. 13: 1368. https://doi.org/10.3390/diagnostics14131368
APA StyleJurica, J., Péč, M. J., Cingel, M., Bolek, T., Barbierik Vachalcová, M., Horná, S., Galajda, P., Mokáň, M., & Samoš, M. (2024). Left Ventricular and Atrial Deformation in Patients with Acute Decompensated Heart Failure: A Pilot Study. Diagnostics, 14(13), 1368. https://doi.org/10.3390/diagnostics14131368