
Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
3. Results
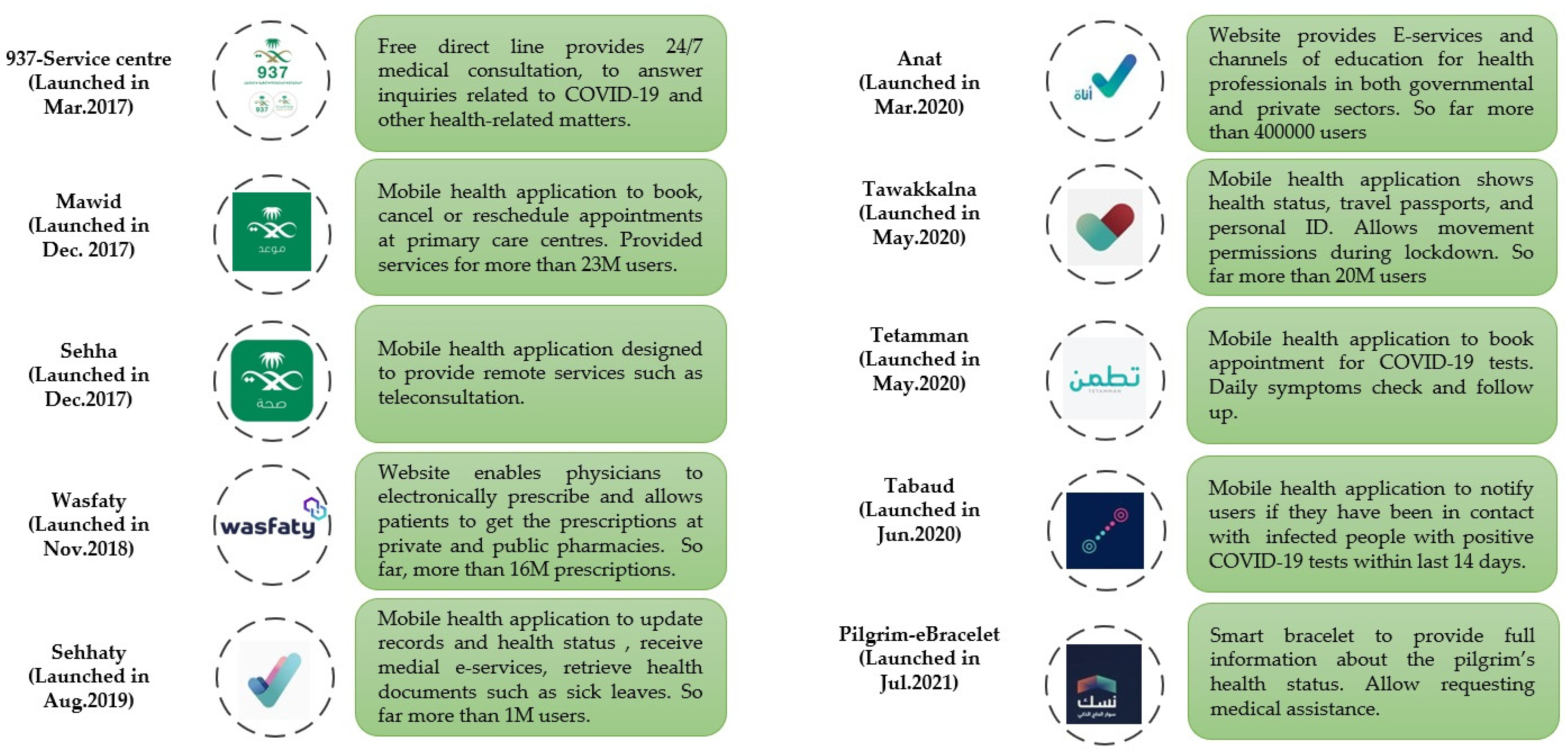
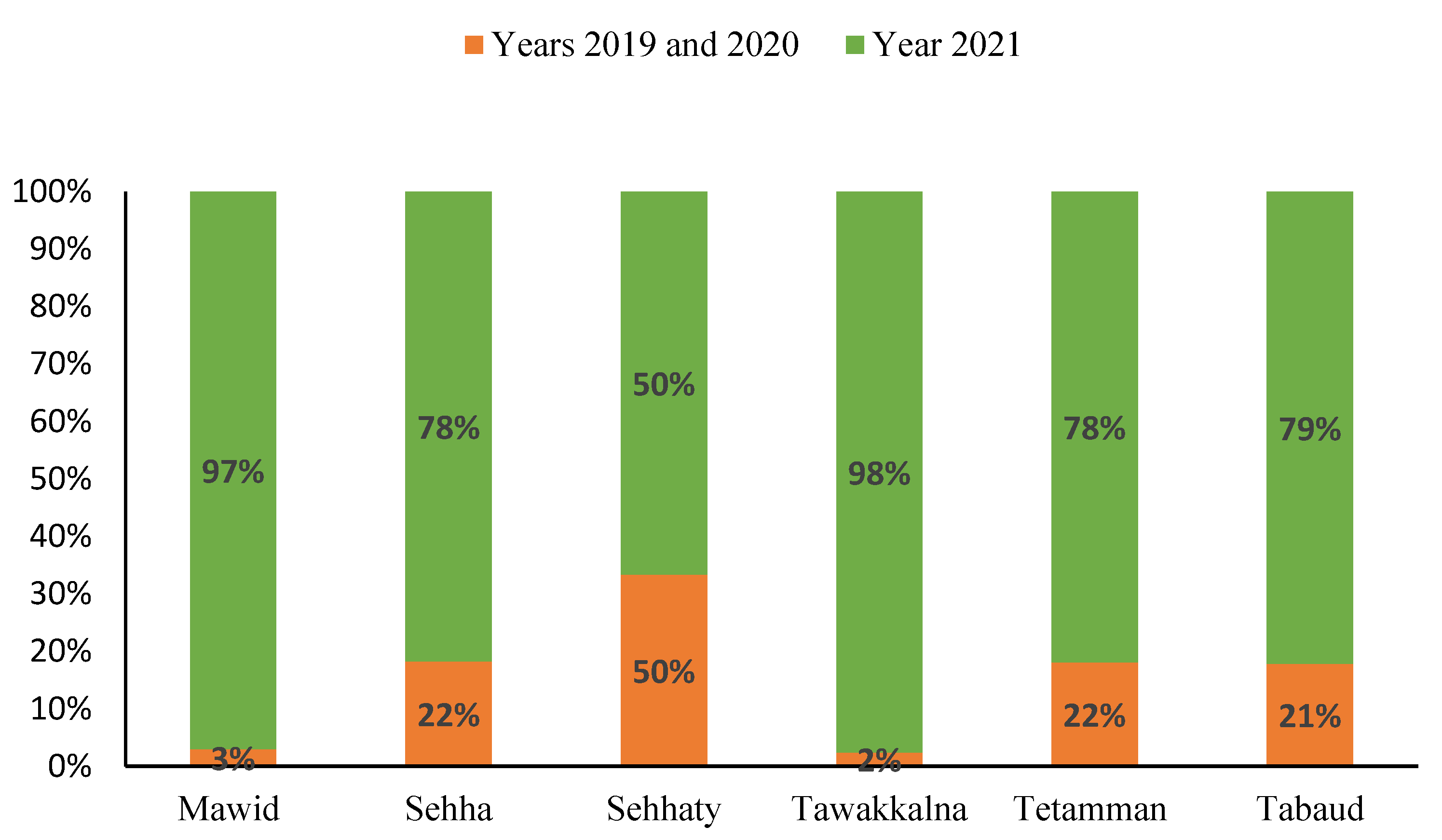
3.1. Digital Response in Saudi Arabia
3.2. Determinants for Optimising DHTPs
3.3. DHTPs and Hajj Season
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministry of Health (Saudi Arabia). COVID-19 Daily Briefing. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter (accessed on 1 November 2021).
- Hassounah, M.; Raheel, H.; Alhefzi, M. Digital response during the COVID-19 pandemic in Saudi Arabia. J. Med. Internet Res. 2020, 22, e19338. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Alghamdi, S.M.; Aldhahir, A.M.; Althobiani, M.; Oyelade, T. Key toolkits of non-pharmacological management in COPD: During and beyond COVID-19. Front. Biosci. 2021, 7, 246–252. [Google Scholar]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Alsofayan, Y.M.; Alahmari, A.A.; Alowais, J.M.; Algwizani, A.R.; Alserehi, H.A.; Assiri, A.M.; Jokhdar, H.A. COVID-19 in Saudi Arabia: The national health response. East. Mediterr. Health J. 2021. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef]
- Vaishya, R.; Javaid, M.; Khan, I.H.; Haleem, A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Alassaf, N.; Bah, S.; Almulhim, F.; AlDossary, N.; Alqahtani, M. Evaluation of official healthcare informatics applications in Saudi Arabia and their role in addressing COVID-19 Pandemic. Health Inform. Res. 2021, 27, 255–263. [Google Scholar] [CrossRef]
- Kushwaha, S.; Bahl, S.; Bagha, A.K.; Parmar, K.S.; Javaid, M.; Haleem, A.; Singh, R.P. Significant applications of machine learning for COVID-19 pandemic. J. Ind. Integr. Manag. 2020, 5, 453–479. [Google Scholar] [CrossRef]
- Omran, N.F.; Ghany, S.F.A.-E.; Saleh, H.; Ali, A.A.; Gumaei, A.; Al-Rakhami, M. Applying deep learning methods on time-series data for forecasting COVID-19 in Egypt, Kuwait, and Saudi Arabia. Complexity 2021, 2021, 6686745. [Google Scholar] [CrossRef]
- Adeniyi, E.A.; Awotunde, J.B.; Ogundokun, R.O.; Kolawole, P.O.; Abiodun, M.K.; Adeniyi, A.A. Mobile health application and COVID-19: Opportunities and challenges. J. Crit. Rev. 2020, 7, 3481–3488. [Google Scholar]
- Fagherazzi, G.; Goetzinger, C.; Rashid, M.A.; Aguayo, G.A.; Huiart, L. Digital health strategies to fight COVID-19 worldwide: Challenges, recommendations, and a Call for Papers. J. Med. Internet Res. 2020, 22, e19284. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Tseng, R.M.W.W.; Tham, Y.-C.; Wong, T.Y. Applications of digital health for public health responses to COVID-19: A systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit. Med. 2021, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Jokhdar, H.; Khan, A.; Asiri, S.; Motair, W.; Assiri, A.; Alabdulaali, M. COVID-19 mitigation plans during Hajj 2020: A success story of zero cases. Health Secur. 2021, 19, 133–139. [Google Scholar] [CrossRef]
- Ministry of Health (Saudi Arabia). National E-Health Strategy. Available online: https://www.moh.gov.sa/en/Ministry/nehs (accessed on 1 November 2021).
- Alghamdi, S.M.; Alqahtani, J.; Aldhahir, A.M. Current status of telehealth in Saudi Arabia during COVID-19. J. Fam. Commun. Med. 2020, 27, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Aldhahir, A.M.; Althobiani, M.A.; Alghamdi, S.M.; Alanazi, A.F.; Alnaim, N.; Alqarni, A.A.; Alwafi, H. Current knowledge, satisfaction, and use of E-health mobile application (Seha) among the general population of Saudi Arabia: A national survey. JMIR uHealth 2021. [Google Scholar] [CrossRef]
- Gagnon, M.-P.; Attieh, R.; Ghandour, E.K.; Légaré, F.; Ouimet, M.; Estabrooks, C.A.; Grimshaw, J. A systematic review of instruments to assess organizational readiness for knowledge translation in health care. PLoS ONE 2014, 9, e114338. [Google Scholar] [CrossRef] [PubMed]
- Al-Dossary, R.; Alamri, M.; AlBaqawi, H.; Al Hosis, K.; Aljeldah, M.; Aljohan, M.; Aljohani, K.; Almadani, N.; Alrasheadi, B.; Falatah, R.; et al. Awareness, attitudes, prevention, and perceptions of COVID-19 outbreak among nurses in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 8269. [Google Scholar] [CrossRef]
- Blandford, A.; Wesson, J.; Amalberti, R.; AlHazme, R.; Allwihan, R. Opportunities and challenges for telehealth within, and beyond, a pandemic. Lancet Glob. Health 2020, 8, e1364–e1365. [Google Scholar] [CrossRef]
- Alomari, M.O.; Jenkins, J. Exploring the Attitudes of patients towards using the seha application (Telehealth) in Saudi Arabia during the Coronavirus epidemic. ABC J. Adv. Res. 2021, 10, 9–22. [Google Scholar] [CrossRef]
- Alhamam, N.M.; Buhalim, R.A.; Almakhayitah, I.H.; AlBahr, A.W.; AlYaeesh, I.A. Telemedicine for musculoskeletal care during the COVID-19 pandemic: Evaluating readiness of Saudi citizens. Cureus 2021, 13, e13380. [Google Scholar] [CrossRef]
- Alharbi, A.; Alzuwaed, J.; Qasem, H. Evaluation of e-health (Seha) application: A cross-sectional study in Saudi Arabia. BMC Med. Inform. Decis. Mak. 2021, 21, 103. [Google Scholar] [CrossRef]
- Robert, A.A.; Al Saeed, A.; Al Dawish, M.A. COVID-19 among people with diabetes mellitus in Saudi Arabia: Current situation and new perspectives. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102231. [Google Scholar] [CrossRef]
- Mubaraki, A.A.; Alrabie, A.D.; Sibyani, A.K.; Aljuaid, R.S.; Bajaber, A.S.; Mubaraki, M.A. Advantages and disadvantages of telemedicine during the COVID-19 pandemic era among physicians in Taif, Saudi Arabia. Saudi Med. J. 2021, 42, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Nasser, A.A.; Alzahrani, R.M.; Al-Falah, C.A.; Jreash, D.M.; Almouled, N.T.; Bakula, D.S.; Ra’Oof, R.A. Measuring the patients’ satisfaction about telemedicine used in Saudi Arabia during COVID-19 pandemic. Cureus 2021, 13, e13382. [Google Scholar] [CrossRef]
- National Digital Transformation Report Annual Report. 16 September 2020. Available online: https://ndu.gov.sa/en/ (accessed on 1 November 2021).
- Alhudhaif, A. Role of Technology in Managing COVID-19: A Case of Saudi Arabia. In Proceedings of the 2021 8th International Conference on Computing for Sustainable Global Development (INDIACom), New Delhi, India, 17–19 March 2021. [Google Scholar]
- Daem Service. Saudi Commission for Health Specialties. 2021. Available online: https://www.scfhs.org.sa/en/eservices/trainees/Pages/TrainingGuidanceServiceDesc.aspx (accessed on 1 November 2021).
- Bachar, M.; Khamsi, M.A.; Bounkhel, M. A mathematical model for the spread of COVID-19 and control mechanisms in Saudi Arabia. Adv. Differ. Equ. 2021, 2021, 253. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Ahmed, S.S. IoT-based analysis for controlling & spreading prediction of COVID-19 in Saudi Arabia. Soft. Comput. 2021, 25, 12551–12563. [Google Scholar]
- Mohamed, I.A.; Ben Aissa, A.; Hussein, L.F.; Taloba, A.I.; Kallel, T. A new model for epidemic prediction: COVID-19 in kingdom saudi arabia case study. Mater. Today Proc. 2021. [Google Scholar] [CrossRef]
- Komies, S.; Aldhahir, A.M.; Almehmadi, M.; Alghamdi, S.M.; Alqarni, A.; Oyelade, T.; Alqahtani, J.S. COVID-19 Outcomes in Saudi Arabia and the UK: A tale of two kingdoms. medRxiv 2020. [Google Scholar]
- Alshammari, F.S. A mathematical model to investigate the transmission of COVID-19 in the Kingdom of Saudi Arabia. Comput. Math. Methods Med. 2020, 2020, 9136157. [Google Scholar] [CrossRef]
- Alyami, M.H.; Naser, A.Y.; Orabi, M.A.A.; Alwafi, H.; Alyami, H.S. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: An Ecological Study. Front. Public Health 2020, 8, 506. [Google Scholar] [CrossRef]
- Adly, H.M.; Aljahdali, I.A.; Garout, M.A.; Khafagy, A.A.; Saati, A.A.; Saleh, S.A.K. Correlation of COVID-19 pandemic with healthcare system response and prevention measures in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 6666. [Google Scholar] [CrossRef] [PubMed]
- Algaissi, A.A.; Alharbi, N.K.; Hassanain, M.; Hashem, A.M. Preparedness and response to COVID-19 in Saudi Arabia: Building on MERS experience. J. Infect. Public Health 2020, 13, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Saudi Center for Disease Prevention and Control. (COVID-19) Disease Interactive Dashboard. 10 August 2021. Available online: https://covid19.cdc.gov.sa/daily-updates (accessed on 1 November 2021).
- Alqahtani, J.; Aldabayan, Y.; AlAhmari, M.; AlRabeeah, S.; Aldhahir, A.; Alghamdi, S.; Oyelade, T.; Althobiani, M.; Alrajeh, A. Clinical practice and barriers of ventilatory support management in COVID-19 patients in Saudi Arabia: A survey of respiratory therapists. Saudi J. Med. Med Sci. 2021, 9, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Saquib, J. Internet addiction among Saudi Arabian youth. Int. J. Health Sci. 2020, 14, 1. [Google Scholar]
- National Digital Transformation Report. Samrt Hajj. 2021. Available online: https://ndu.gov.sa/report/Hajj-report.pdf (accessed on 1 November 2021).
- A Memish, Z.; Zumla, P.S.A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; Al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M.; et al. Hajj: Infectious disease surveillance and control. Lancet 2014, 383, 2073–2082. [Google Scholar] [CrossRef]
- Al-Shaery, A.M.; Hejase, B.; Tridane, A.; Farooqi, N.S.; Jassmi, H.A. Agent-based modeling of the Hajj Rituals with the possible spread of COVID-19. Sustainability 2021, 13, 6923. [Google Scholar] [CrossRef]
- Alshalani, H.; Alnaghaimshi, N.; Eljack, S. ICT System for Crowd Management: Hajj as a Case Study. In Proceedings of the 2020 International Conference on Computing and Information Technology (ICCIT-1441), Tabuk, Saudi Arabia, 9–10 September 2020. [Google Scholar]
- Shambour, M.K.; Gutub, A. Progress of IoT research technologies and applications serving Hajj and Umrah. Arab. J. Sci. Eng. 2021, 1–21. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| DHTP Terminology | Application during COVID-19 Outbreak |
|---|---|
| Digital Health Technology Platforms (DHTPs) | Using information and communication technologies to provide distance health services for people as well as support decision-making processes for healthcare professionals [7]. |
| Artificial Intelligence (AI) | Using machines to screen people in large public places, provide fast diagnosis, and detect infected people with fever [8,9]. |
| Machine Learning (ML) | Using mathematical algorithms to predict infected cases, mortality, and vaccinations [10,11]. |
| Mobile health applications | Using mobile apps to track daily symptoms of infected and non-infected people as well as book appointments and vaccinations [12]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghamdi, S.M.; Alsulayyim, A.S.; Alqahtani, J.S.; Aldhahir, A.M. Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience. Healthcare 2021, 9, 1517. https://doi.org/10.3390/healthcare9111517
Alghamdi SM, Alsulayyim AS, Alqahtani JS, Aldhahir AM. Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience. Healthcare. 2021; 9(11):1517. https://doi.org/10.3390/healthcare9111517
Chicago/Turabian StyleAlghamdi, Saeed M., Abdullah S. Alsulayyim, Jaber S. Alqahtani, and Abdulelah M. Aldhahir. 2021. "Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience" Healthcare 9, no. 11: 1517. https://doi.org/10.3390/healthcare9111517
APA StyleAlghamdi, S. M., Alsulayyim, A. S., Alqahtani, J. S., & Aldhahir, A. M. (2021). Digital Health Platforms in Saudi Arabia: Determinants from the COVID-19 Pandemic Experience. Healthcare, 9(11), 1517. https://doi.org/10.3390/healthcare9111517