
Assessing the Level of Awareness of COVID-19 and Prevalence of General Anxiety Disorder among the Hail Community, Kingdom of Saudi Arabia

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Area and Population
2.3. Sampling Techniques
2.4. Data Collection
2.5. Data Management and Analysis
2.6. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization, Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 15 January 2021).
- Alshammari, T.M.; Altebainawi, A.F.; Alenzi, K.A. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an Example. Saudi Pharm. J. 2020, 28, 898–902. [Google Scholar] [CrossRef]
- Alahdal, H.; Basingab, F.; Alotaibi, R. An analytical study on the awareness, attitude and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J. Infect. Public Health 2020, 13, 1446–1452. [Google Scholar] [CrossRef]
- BioSpace. What We Now Know about Coronavirus Transmission: Where the Virus Goes in Your Body and How It Is Spread. Available online: https://www.biospace.com/article/all-the-ways-we-know-that-you-can-get-coronavirus/ (accessed on 24 October 2020).
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, perceptions, and attitude of egyptians towards the novel coronavirus disease (COVID-19). J. Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef]
- She, J.; Jiang, J.; Ye, L.; Hu, L.; Bai, C.; Song, Y. 2019 novel coronavirus of pneumonia in Wuhan, China: Emerging attack and management strategies. Clin. Transl. Med. 2020, 9, 19. [Google Scholar] [CrossRef]
- MERS-COV. Guidelines for Healthcare Professionals—May 2018—v5.1. Available online: https://www.moh.gov.sa/ccc/healthp/regulations/documents/mers-cov%20guidelines%20for%20healthcare%20professionals%20-%20may%202018%20-%20v5.1%20%281%29.pdf (accessed on 15 January 2021).
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 15 January 2021).
- Kutsuna, S.; Suzuki, T.; Hayakawa, K.; Tsuzuki, S.; Asai, Y.; Suzuki, T.; Ide, S.; Nakamura, K.; Moriyama, Y.; Kinoshita, N.; et al. SARS-CoV-2 Screening test for Japanese returnees from Wuhan, China, January 2020. Open Forum Infect. Dis. 2020, 7, 243. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200217-sitrep-28-covid-19.pdf?sfvrsn=a19cf2ad_2 (accessed on 24 October 2020).
- Villalba, N.L.; Maouche, Y.; Ortiz, M.B.A.; Sosa, Z.C.; Chahbazian, J.B.; Syrovatkova, A.; Pertoldi, P.; Andres, E.; Zulfiqar, A.-A. Anosmia and Dysgeusia in the Absence of Other Respiratory Diseases: Should COVID-19 Infection Be Considered? Eur. J. Case Rep. Intern. Med. 2020, 7, 001641. Available online: https://www.ejcrim.com/index.php/EJCRIM/article/view/1641 (accessed on 24 October 2020).
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance, 28 January 2020. Art. no. WHO/nCoV/Clinical/2020.3. 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 15 January 2021).
- CDC. Use Personal Protective Equipment (PPE). 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/downloads/A_FS_HCP_COVID19_PPE.pdf (accessed on 15 January 2021).
- Saudi Geological Survey. KSA in Facts. Available online: http://shop.sgs.org.sa (accessed on 15 January 2021).
- Kassahun, C.W.; Mekonen, A.G. Knowledge, attitude, practices and their associated factors towards diabetes mellitus among non diabetes community members of Bale Zone administrative towns, South East Ethiopia. A cross-sectional study. PLoS ONE 2017, 12, e0170040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semo, B.; Frissa, S.M. The Mental Health Impact of the COVID-19 Pandemic: Implications for Sub-Saharan Africa. Psychol. Res. Behav. Manag. 2020, 13, 73. Available online: https://www.dovepress.com/the-mental-health-impact-of-the-covid-19-pandemic-implications-for-sub-peer-reviewed-article-PRBM (accessed on 15 January 2021). [CrossRef] [PubMed]
- Hassounah, M.; Raheel, H.; Alhefzi, M. Digital Response during the COVID-19 Pandemic in Saudi Arabia. J. Med. Internet Res. 2020, 22, e19338. Available online: https://www.jmir.org/2020/9/e19338/ (accessed on 24 October 2020). [CrossRef]
- Alyami, H.S.; Orabi, M.A.; Aldhabbah, F.M.; Alturki, H.N.; Aburas, W.I.; Alfayez, A.I.; Alharbi, A.S.; Almasuood, R.A.; Alsuhaibani, N.A. Knowledge about COVID-19 and Patients Beliefs about and Use of Herbal Products during the COVID-19 Pandemic: A Cross-Sectional Study in Saudi Arabia. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.06.23.20138107v1 (accessed on 15 January 2021). [CrossRef]
- Wadood, M.A.; Mamun, A.S.; Rafi, M.A.; Kamrul Islam, M.; Mohd, S.; Lee, L.L.; Hossain, M.G. Knowledge, Attitude, Practice and Perception Regarding COVID-19 among Students in Bangladesh: Survey in Rajshahi University. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.04.21.20074757v1 (accessed on 15 January 2021). [CrossRef] [Green Version]
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 19. Emerg. Infect. Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Yang, B.; Zhang, R.; Cheng, X. Influencing factors of understanding COVID-19 risks and coping behaviors among the elderly population. Int. J. Environ. Res. Public Health 2020, 17, 5889. [Google Scholar]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Tran, B.X.; Dang, A.K.; Thai, P.K.; Le, H.T.; Le, X.T.T.; Do, T.T.T.; Nguyen, T.H.; Pham, H.Q.; Phan, H.T.; Vu, G.T. Coverage of Health Information by Different Sources in Communities: Implication for COVID-19 Epidemic Response. Int. J. Environ. Res. Public Health 2020, 17, 3577. [Google Scholar] [CrossRef]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E.-M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Sherman, A.C.; Williams, M.L.; Amick, B.C.; Hudson, T.J.; Messias, E.L. Mental health outcomes associated with the COVID-19 pandemic: Prevalence and risk factors in a southern US state. Psychiatry Res. 2020, 293, 113476. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.; Bakri, F.; Mahafzah, A. Conspiracy beliefs are associated with lower knowledge and higher anxiety levels regarding COVID-19 among students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17, 4915. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tee, M.; Roy, A.E.; Fardin, M.A.; Srichokchatchawan, W.; Habib, H.A.; Tran, B.X.; Hussain, S.; Hoang, M.T.; Le, X.T. The Impact of COVID-19 Pandemic on Physical and Mental Health of Asians: A Study of Seven Middle-Income Countries in Asia. PLoS ONE 2021, 16, e0246824. [Google Scholar]
- Algahtani, F.D.; Hassan SU, N.; Alsaif, B.; Zrieq, R. Assessment of the quality of life during COVID-19 pandemic: A cross-sectional survey from the kingdom of saudi arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, F.D.; Zrieq, R. Avoiding medical visits even when needed during the COVID-19 pandemic: A cross-sectional survey from Saudi Arabia. Syst. Rev. Pharm. 2020, 11, 649–654. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206. [Google Scholar] [CrossRef] [PubMed]
- Chudasama, Y.V.; Gillies, C.L.; Zaccardi, F.; Coles, B.; Davies, M.J.; Seidu, S.; Khunti, K. Impact of COVID-19 on routine care for chronic diseases: A global survey of views from healthcare professionals. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 965–967. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Total | Knowledge | Attitude | Practice | |||
|---|---|---|---|---|---|---|---|
| n (%) | Good n (%) | Bad n (%) | Positive n (%) | Negative n (%) | Good n (%) | Bad n (%) | |
| Overall | 412 (100) | 243 (59) | 169 (41) | 285 (69.2) | 127 (30.8) | 280 (68.0) | 132 (32.0) |
| Age group | |||||||
| 18–25 years | 157 (38.1) | 78 (49.7) | 79 (50.3) ** | 101 (64.3) | 56 (35.7) * | (59.2) 93 | 64 (40.8) ** |
| 26–49 years | 171 (41.5) | 109 (63.7) | 62 (36.3) | 117 (68.4) | 54 (31.6) | 121 (70.8) | 50 (29.2) |
| >50 years | 84 (20.4) | 56 (66.7) | 28 (33.3) | 67 (79.8) | 17 (20.2) | 66 (78.8) | 18 (21.4) |
| Gender | |||||||
| Male | 212 (51.5) | 129 (60.8) | 83 (39.2) ns | (70.8) 150 | 62 (29.2) ns | 137 (64.6) | 75 (35.4) ns |
| Female | 200 (48.5) | 114 (57.0) | 86 (43.0) | 135 (67.5) | 65 (32.5) | 143 (71.5) | 57 (28.5) |
| Occupation | |||||||
| Student | 150 (36.4) | 73 (48.7) | 77 (51.3) * | 97 (64.7) | 53 (35.3) *** | 90 (60.0) | 60 (40.0) ** |
| Employee | 137 (33.3) | 91 (66.4) | 46 (33.6) | 104 (75.9) | 33 (24.1) | 100 (73.0) | 37 (27.0) |
| Free business | 10 (2.4) | 6 (60.0) | 4 (40.0) | 8 (80.0) | 2 (20.0) | 8 (80.0) | 2 (20.0) |
| Housewife | 43 (10.4) | 31 (72.1) | (27.9) 12 | 32 (74.4) | 11 (25.6) | 32 (74.4) | 11 (25.6) |
| Unemployed | 22 (5.3) | 14 (63.6) | 8 (36.4) | 5 (22.7) | 17 (77.3) | 10 (45.5) | 12 (54.5) |
| Retired | 50 (12.1) | (56.0) 28 | 22 (44) | 39 (78.0) | 11 (22.0) | 40 (80.0) | 10 (20.0) |
| Marital status | |||||||
| Married | 180 (43.7) | 90 (50.0) | 90 (50.0) ** | 113 (62.8) | 67 (37.2) ** | 112 (62.2) | 68 (37.8) ns |
| Single | 222 (53.9) | 144 (64.9) | 78 (35.1) | 162 (73.0) | (27.0) 60 | 162 (73.0) | 60 (27.0) |
| Divorce | 10 (2.4) | 9 (90.0) | 1 (10.0) | 10 (100) | 0 | 6 (60.0) | 4 (40.0) |
| Residence | |||||||
| City | 383 (93.0) | 229 (59.8) | 154 (40.2) ns | 270 (70.5) | 113 (29.5) * | 264 (68.9) | 119 (31.1) ns |
| Village | 29 (7.0) | 14 (48.3) | 15 (51.7) | 15 (51.7) | 14 (48.3) | 16 (55.2) | 13 (44.8) |
| Chronic disease | |||||||
| Yes | 99 (24.0) | 66 (66.7) | 33 (33.3) ns | 71 (71.7) | 28 (28.3) ns | 205 (65.5) | 108 (34.5) ns |
| No | 313 (76.0) | 177 (56.5) | 136 (43.5) | 214 (68.4) | 99 (31.6) | 75 (75.8) | 24 (24.2) |
| Variables | Attitude | Practice |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Knowledge | ||
| Bad | Reference | Reference |
| Good | 1.45 (0.95–2.21) ns | 1.50 (0.98–2.27) ns |
| Attitude | ||
| Negative | Reference | Reference |
| Positive | - | 2.40 (1.54–3.99) *** |
| Age Group | ||
| 18–25 years | Reference | Reference |
| 26–49 years | 1.20 (0.76–1.90) ns | 1.67 (1.05–2.63) * |
| >50 yeas | 2.18 (1.17–4.08) * | 2.52 (1.37–4.65) ** |
| Occupation | ||
| Student | Reference | Reference |
| Employee | 1.72 (1.02–2.88) * | 1.80 (1.09–2.96) * |
| Free Business | 2.18 (0.45–10.6) ns | 2.66 (0.55–12.99) ns |
| Housewife | 1.59 (0.74–3.41) ns | 1.94 (0.91–4.14) ns |
| Unemployed | 0.16 (0.05–0.46) ** | 0.56 (0.22–1.37) ns |
| Retired | 1.94 (0.91–2.10) ns | 2.67 (1.24–5.74) * |
| Residence | ||
| City | Reference | Reference |
| Village | 0.45 (0.21–0.96) * | 0.55 (0.26–1.9) ns |
| Marital Status | ||
| Single | Reference | Reference |
| Married | 1.60 (1.04–2.44) * | 1.64 (1.07–2.50) * |
| Divorce | 0.99 (0.10–2.21) ns | 0.91 (0.25–3.34) ns |
| Variables | Anxiety Disorder | ||
|---|---|---|---|
| Yes n (%) | No n (%) | OR (95% CI) | |
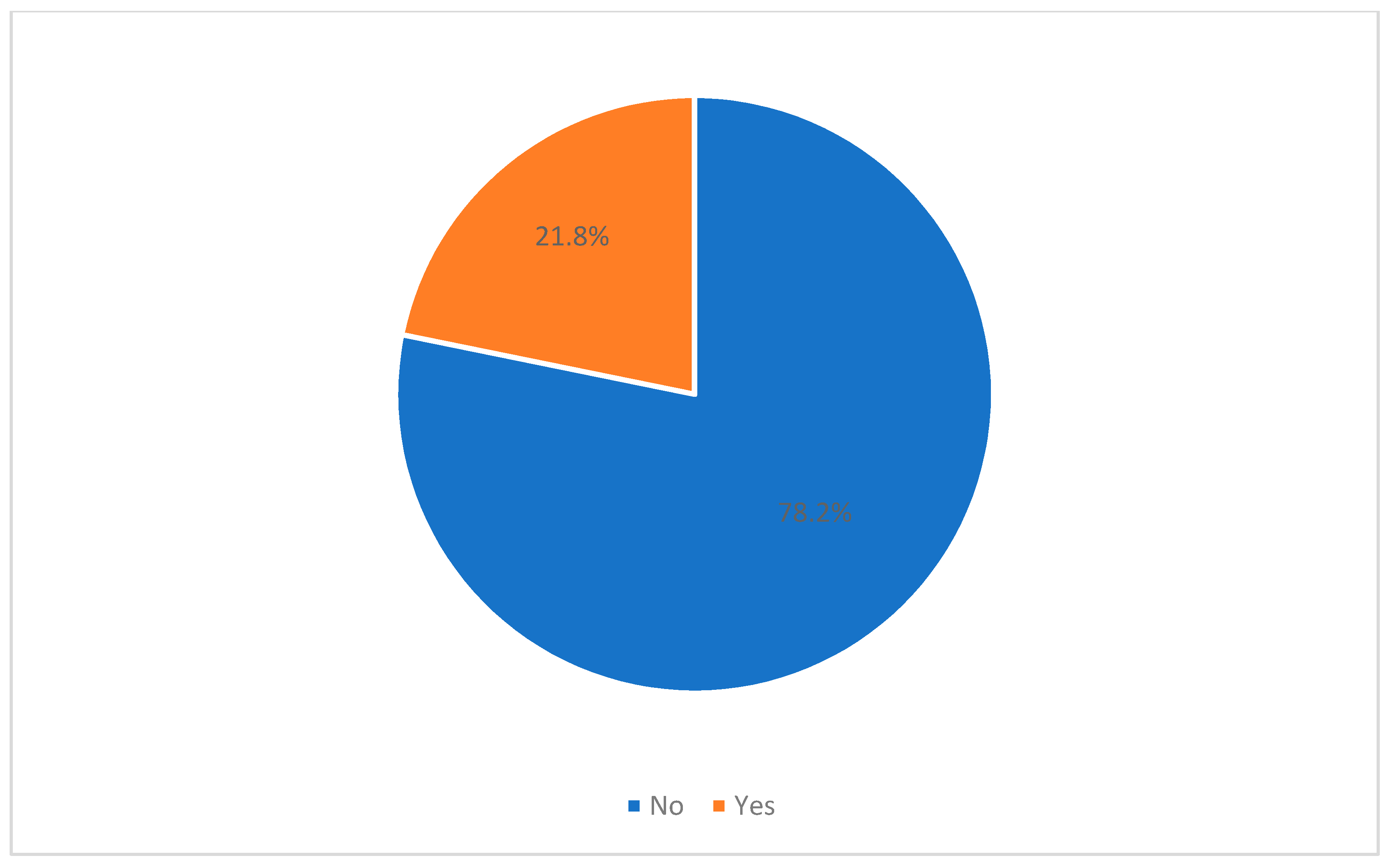
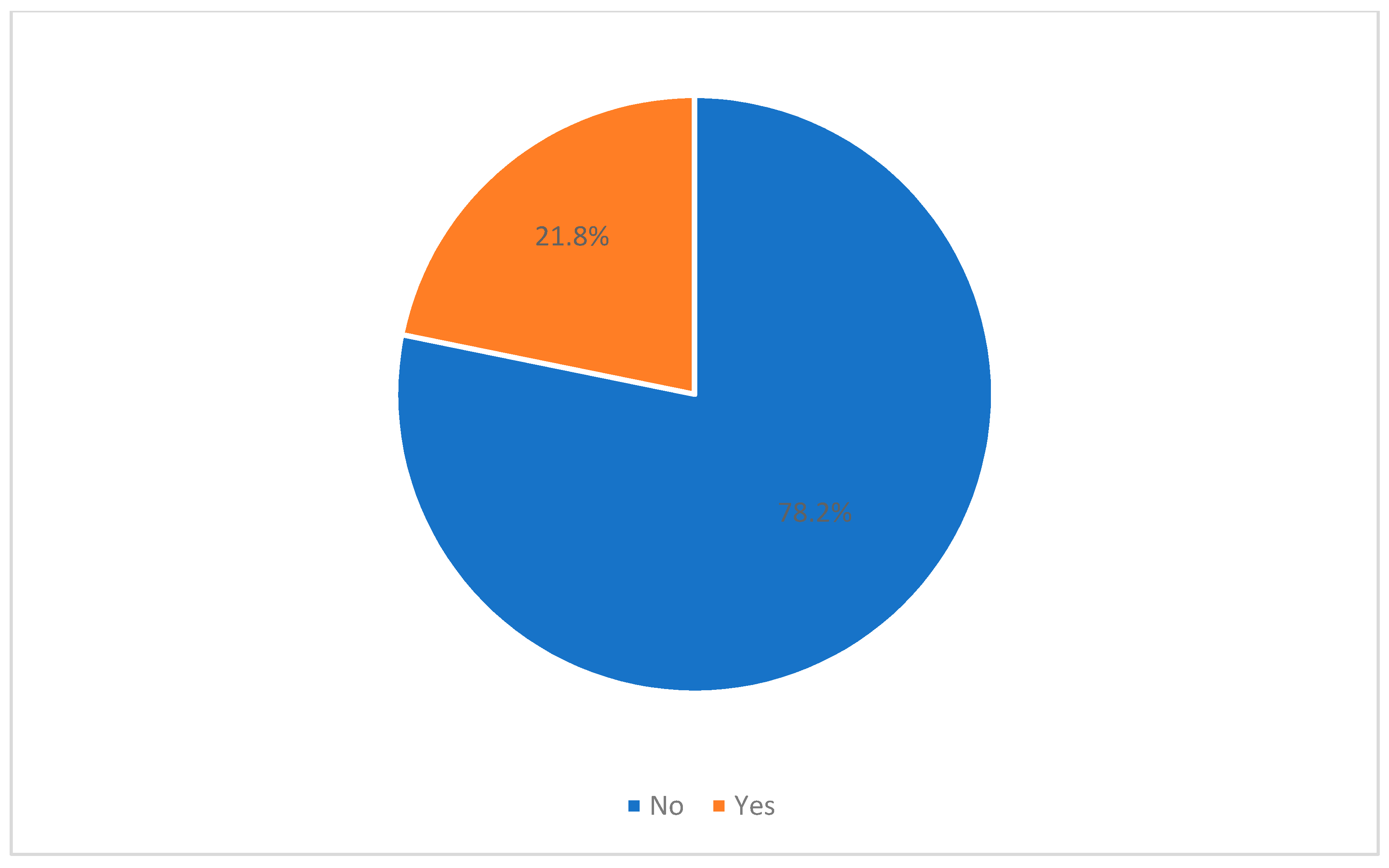
| Total | 90 (21.8) | 322 (78.2) | - |
| Knowledge | |||
| Good | 41 (16.9) | 202 (83.1) | Reference |
| Bad | 49 (29.0) | 120 (71.0) | 2.01 (1.25–3.22) ** |
| Age Group | |||
| 18–25 years | 43 (27.4) | 114 (72.6) | Reference |
| 26–49 years | 37 (21.6) | 134 (78.4) | 0.73 (0.44–1.21) ns |
| >50 yeas | 10 (11.9) | 74 (88.1) | 0.36 (0.17–0.76) ** |
| Gender | |||
| Male | 35 (16.5) | 177 (83.5) | Reference |
| Female | 55 (27.5) | 145 (72.5) | 1.92 (1.19–3.09) ** |
| Marital Status | |||
| Single | 53 (29.4) | 127 (70.6) | Reference |
| Married | 36 (16.2) | 186 (83.8) | 0.46 (1.07–2.50) ** |
| Divorce | 1 (10.0) | 9 (90.0) | 0.26 (0.03–2.15) ns |
| Chronic disease | |||
| No | 61 (19.5) | 252 (80.5) | Reference |
| Yes | 29 (29.3) | 70 (70.7) | 1.71 (1.02–2.86) * |
| Nationality | |||
| Saudi | 81 (20.8) | 308 (79.2) | Reference |
| Non-Saudi | 9 (39.1) | 14 (60.9) | 2.44 (1.02–5.85) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsaif, B.; Elhassan, N.E.E.; Itumalla, R.; Ali, K.E.; Alzain, M.A. Assessing the Level of Awareness of COVID-19 and Prevalence of General Anxiety Disorder among the Hail Community, Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 7035. https://doi.org/10.3390/ijerph18137035
Alsaif B, Elhassan NEE, Itumalla R, Ali KE, Alzain MA. Assessing the Level of Awareness of COVID-19 and Prevalence of General Anxiety Disorder among the Hail Community, Kingdom of Saudi Arabia. International Journal of Environmental Research and Public Health. 2021; 18(13):7035. https://doi.org/10.3390/ijerph18137035
Chicago/Turabian StyleAlsaif, Bandar, Najm Eldinn Elsser Elhassan, Ramaiah Itumalla, Kamal Elbassir Ali, and Mohamed Ali Alzain. 2021. "Assessing the Level of Awareness of COVID-19 and Prevalence of General Anxiety Disorder among the Hail Community, Kingdom of Saudi Arabia" International Journal of Environmental Research and Public Health 18, no. 13: 7035. https://doi.org/10.3390/ijerph18137035
APA StyleAlsaif, B., Elhassan, N. E. E., Itumalla, R., Ali, K. E., & Alzain, M. A. (2021). Assessing the Level of Awareness of COVID-19 and Prevalence of General Anxiety Disorder among the Hail Community, Kingdom of Saudi Arabia. International Journal of Environmental Research and Public Health, 18(13), 7035. https://doi.org/10.3390/ijerph18137035