Abstract
Spine surgery generally yields a notable improvement in patients’ health state, and there is variability in measured patient outcomes after spine surgery. The present work aimed to describe for clinicians how appraisal underlies their patients’ experience of healthcare interventions. This prospective longitudinal cohort study (n = 156) included adults undergoing spine surgery for degenerative spinal conditions. The analysis was a descriptive illustration of the relationship between change in the spine-related disability using the Oswestry Disability Index and change in cognitive-appraisal processes using the Quality-of-Life Appraisal Profilev2-Short Form, early versus later during the recovery trajectory (i.e., between baseline and 3 months post-surgery; and between 3 and 12 months post-surgery). Cognitive-appraisal processes related to Sampling of Experience showed greater change soon after surgery, whereas Standards of Comparison appraisals changed more later in the recovery trajectory. Different appraisal processes were emphasized by patients who reported worsening of the spine-related disability, as compared to those who reported no change or improvement. These findings suggest that changes in appraisal differ depending on the individual’s experience of the impact of spine surgery. Appraisal processes thus reflect an ongoing dynamic in adaptation to changing function.
1. Introduction
Spine surgery generally yields a notable improvement in patients’ health state, reducing pain and increasing function [1,2,3]. There is, however, some variability in measured patient outcomes after spine surgery, related to demographic [4], clinical [5], psychological [6,7,8], and other contextual factors [9]. One notable factor of particular relevance to personalized medicine is cognitive-appraisal processes (i.e., how people recall past experiences and to whom they compare themselves) [10]. Past research has documented that appraisal processes are relevant to chronic pain [11,12,13,14] and spine-specific disability and mental-health functioning and suggested that such processes are modifiable targets of intervention [15].
The concept of appraisal has a long history in psychological research. Perhaps the first mention of appraisal was in the Folkman and Lazarus stress and coping model [16], in which the term was used to refer to whether an individual thought of a stressor as controllable by doing something constructive (i.e., problem-focused coping), or as having to be accepted (emotion-focused coping) [16]. In the field of quality-of-life (QOL) research, appraisal processes focused more on how individuals thought about health when answering survey questions [17,18]. These cognitive-appraisal processes were characterized as comprising four domains: Frame of Reference, Sampling of Experience, Standards of Comparison, and Combinatory Algorithm (i.e., patterns of emphasis) [18]. Such processes were explicitly considered in the Rapkin and Schwartz Appraisal Theory [18], which expanded upon the Sprangers and Schwartz Response Shift Theory [19]. Both theoretical models sought to explain adaptation effects in the face of changing health (i.e., a “catalyst”), and both included reference to stable characteristics of the individual (i.e., “antecedents”), behavioral “mechanisms” for reacting to these health-state changes (i.e., “mechanisms”), response-shift effects, and an unexpected QOL outcome (i.e., higher or lower QOL than would be expected). Response shift was conceptualized as a change in the meaning of one’s self-evaluation of a target construct as a result of: (a) a change in the respondent’s internal standards of measurement (scale recalibration, in psychometric terms); (b) a change in the respondent’s values (i.e., the importance of component domains constituting the target construct); or (c) a redefinition of the target construct (i.e., reconceptualization) [18,19]. Whereas the earlier model provided examples of response shift that overlapped considerably with “mechanisms” (e.g., goal reordering as a both change in priorities/values and a coping mechanism), the Rapkin and Schwartz model distinguished cognitive-appraisal processes as a part of the model, resulting from both antecedents and mechanisms. This model operationalized response shift as “when change in appraisal explained the discrepancy between expected and observed QOL [18]”. Thus began a long research path developing and validating a series of increasingly viable measures of appraisal [18,20].
In this long research path, cognitive-appraisal processes were documented to explain substantial variance in a wide range of patient samples [21], and to help to explain why two individuals in identical health states rate their QOL differently [22]. Appraisal assessment helps to identify and explain how contextual and psychological factors matter in patients’ subjective evaluation of their physical and emotional health [21,22,23]. With this growth in the evidence base for appraisal, there has also been increasing parsimony in appraisal assessment [20] and in statistical methods for working with appraisal [23]. These statistical methods have relied on data reduction and relatively complex multivariate analyses which, though useful for summarizing findings at the aggregate level, may also make the findings hard to parse for clinicians and others not familiar with complex statistical modeling.
The present work was motivated by the gap between the abovementioned complexity and the need for clinicians to understand how appraisal underlies their patients’ experience of healthcare interventions. Focusing on the experience of spine surgery and subsequent recovery over time (catalyst), we sought to describe the ramifications of the surgery for patients along the improvement continuum in the initial three months after surgery, and in the subsequent nine months post-surgery. Two research questions were asked: (1) What drives changes in appraisal after spine surgery? (2) How does change in appraisal vary in response to change in functioning early versus later post-surgery?
2. Materials and Methods
2.1. Sample and Design
This prospective longitudinal cohort study included adults recruited from a spine-surgery practice at a Canadian academic teaching hospital. Eligibility criteria included being over the age of 18 and having undergone elective spinal decompression and/or fusion surgery for diagnoses of disc herniation, radiculopathy/sciatica, spinal stenosis with neurogenic claudication, or degenerative spondylolisthesis. Exclusionary criteria entailed having had prior lumbar surgery at the same level, or being unable to understand and complete the English survey-related documents. All patients provided written informed consent prior to study entry. Data were collected online or by mail pre-surgery and at approximately 3 and 12 months post-surgery using a secure, Health Information Portability and Accountability Act (HIPAA)-compliant interface [24]. The study was reviewed and approved by the Sunnybrook Health Centre Research Ethics Board (#2591).
2.2. Measures
Spine-specific disability was measured using the Oswestry Disability Index (ODI) [25]. This measure is the most commonly used tool in both operative and non-operative spine-patient cohorts. The ODI assesses the level of pain and interference with a range of activities of daily living and physical activities. Each item is scored from 0 to 5 (0, severe disability, to 5, which is no disability). The ODI is scored such that higher scores reflect more disability, with a range from 0 to 100.
Cognitive-appraisal processes were measured using items from two domains of the QOL Appraisal Profilev2 Short-Form (QOLAPv2-SF) [20]. The 14 Sampling-of-Experience items query what types of experiences people recall or think about when responding to QOL measures. The 8 Standards-of-Comparison items query to whom or what the individual compares themself to when thinking about QOL. Items utilized a 5-point rating scale (Never, Rarely, Sometimes, Often, Always), with higher values reflecting more endorsement. “Not applicable” responses were recoded to “Never” for the analysis.
To describe the sample, demographic and clinical characteristics were collected, including age, gender, smoking status, and education. Clinical data included diagnosis, primary procedure, number of vertebrae fused if fusion surgery had occurred, pain-medicine frequency, and comorbidities, the latter of which was assessed using the Self-Administered Comorbidity Questionnaire [26].
2.3. Statistical Analysis
This analysis is a descriptive illustration of the relationship between change in spine-related disability and change in cognitive-appraisal processes. We conducted dependent samples’ t-tests within each group during two time intervals: between baseline and 3 months post-surgery (1st interval); and between 3 and 12 months post-surgery (2nd interval). Descriptive statistics summarized the mean change of these ODI scores and cognitive-appraisal items for each time interval.
The study sample was sorted into groups according to the magnitude of change in ODI scores using Cohen’s d in each of the two time intervals according to the following distribution-based criteria [27]: no effect-size (ES) change = d < 0.2; small ES change = d ≥ 0.2 and <0.49; medium ES change = d ≥ 0.5 and <0.79; and large ES change = d ≥ 0.8. Cohen’s d was also used to characterize the magnitude of change in cognitive-appraisal processes. Additionally, since Hedge’s g is considered by some to be more accurate or conservative for smaller sample sizes because the mean difference is divided by the sample variance rather than the within-sample standard deviation (SD) in the denominator [28,29,30], we also considered results using Hedge’s g1 for the appraisal comparisons. Stability in cognitive-appraisal processes was defined as a mean change in the QOLAPv2-SF item response of less than a small ES (i.e., d < 0.2 SD of the baseline mean), and change was defined as a change of at least 0.2 SD of the baseline mean. An analysis of variance (ANOVA) tested group differences in QOLAPv2-SF item response at each time interval.
Software
Data were analyzed using IBM SPSS version 29 [31] and Microsoft Excel 365.
3. Results
Table 1 provides a summary of baseline demographic and clinical characteristics of the whole study sample. The study sample included 156 people who underwent spine surgery. Most (63%) patients received a laminectomy/discectomy; 12% received instrumentation/fusion; and 19% instrumentation/fusion and laminectomy/discectomy.

Table 1.
Descriptive statistics of study sample †.
3.1. Change-Group Differences in ODI
The study sample had an average ODI score of 46.7, 23.1, and 22.0 at baseline (pre-surgery), and 3 and 12 months post-surgery, respectively. The average change was −23.6 points between baseline and 3 months post-surgery and was −1.1 points between 3 and 12 months post-surgery. Based on the present sample’s standard deviation of 16 on the baseline ODI, a change score of 3.2 points represented a small ES change, of 8 points a medium ES, and of 12.8 points a large ES.
Based on the ODI change scores in the baseline-to-3-month and 3-to-12-month windows, the sample was stratified into five groups for each time interval: (1) Disability worsened; (2) No effect; (3) Small effect; (4) Medium effect; and (5) Large effect. Table 2 displays the crosstab comparing group membership in the two time intervals.
Table 2.
Cross-tabulation of number of patients per group at the two time intervals.
Nine patients of the total sample of one hundred fifty-six worsened in the first interval (i.e., baseline to 3 mo.). Among these 9 patients, 1 continued to worsen, 2 had a small ODI improvement, and 6 had a large ODI improvement at the second interval. Among the 10 who had no change in the first interval, in the second interval 6 worsened, 1 continued to have no change, and 1 and 2 had small and medium ODI improvements, respectively. Among the 14 with small changes in the first interval, 4 worsened, 4 had no change, and 1, 1, and 4 had small, medium, and large ODI improvements, respectively, at the second interval. Among the 17 with a medium change in the first interval, 6 worsened, 1 had no change, and 2, 3, and 5 had small, medium, and large ODI improvements, respectively, during the second interval. Among the 106 with large improvements in the first interval, by the second interval, 47 worsened, 17 had no change, and 18, 9, and 15 had small, medium and large ODI improvements, respectively.
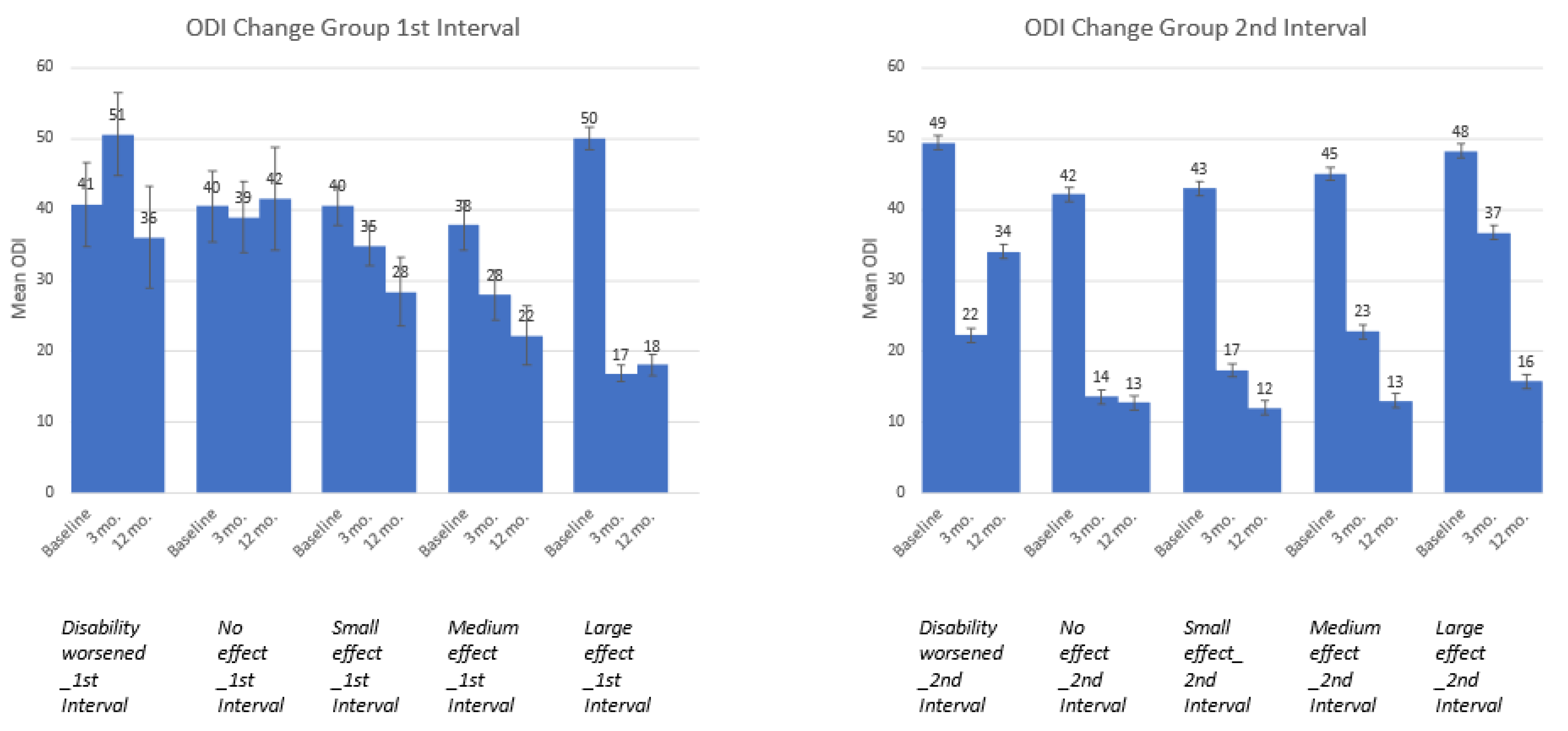
A comparison of ODI trajectories by time interval is shown in Figure 1. In total, the figure displays 10 groups, since there are five groups per interval. Overall, the five groups derived from the first interval data differed on ODI at baseline (F = 3.962, df = 4, p = 0.004), and a visual inspection of Figure 1 suggests that the large ES group had the worst ODI scores (i.e., highest scores) at baseline. Post-hoc Scheffe comparisons suggested a trend (p = 0.06) difference between the medium and large ES groups at the first interval, but the small samples sizes for all but the large ES group undermined our confidence in the statistical power of this analysis. In contrast, the groups derived using second-interval ODI scores did not differ from each other at baseline but did differ at 3 and 12 months post-surgery (F = 1.37, 9.52, and 16. 88; p = 0.247, 0.0001, and 0.0001, respectively). Of note, among the second-interval group whose disability worsened, their ODI did not revert to their baseline score. Furthermore, on average, this group’s ODI change still represents a large effect size improvement at 12 months post-surgery relative to baseline. The other groups showed continued ODI-score improvement, with the second-interval no-effect group showing maintenance of a large effect immediately after surgery, and the other groups showed more of a step-function improvement trajectory.
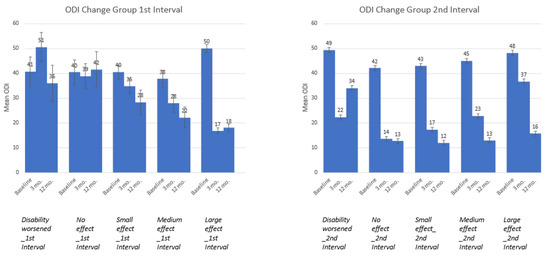
Figure 1.
ODI means and standard errors at baseline, 3 mo. and 12 mo. by ODI-change groups.
3.2. Appraisal Change over Time
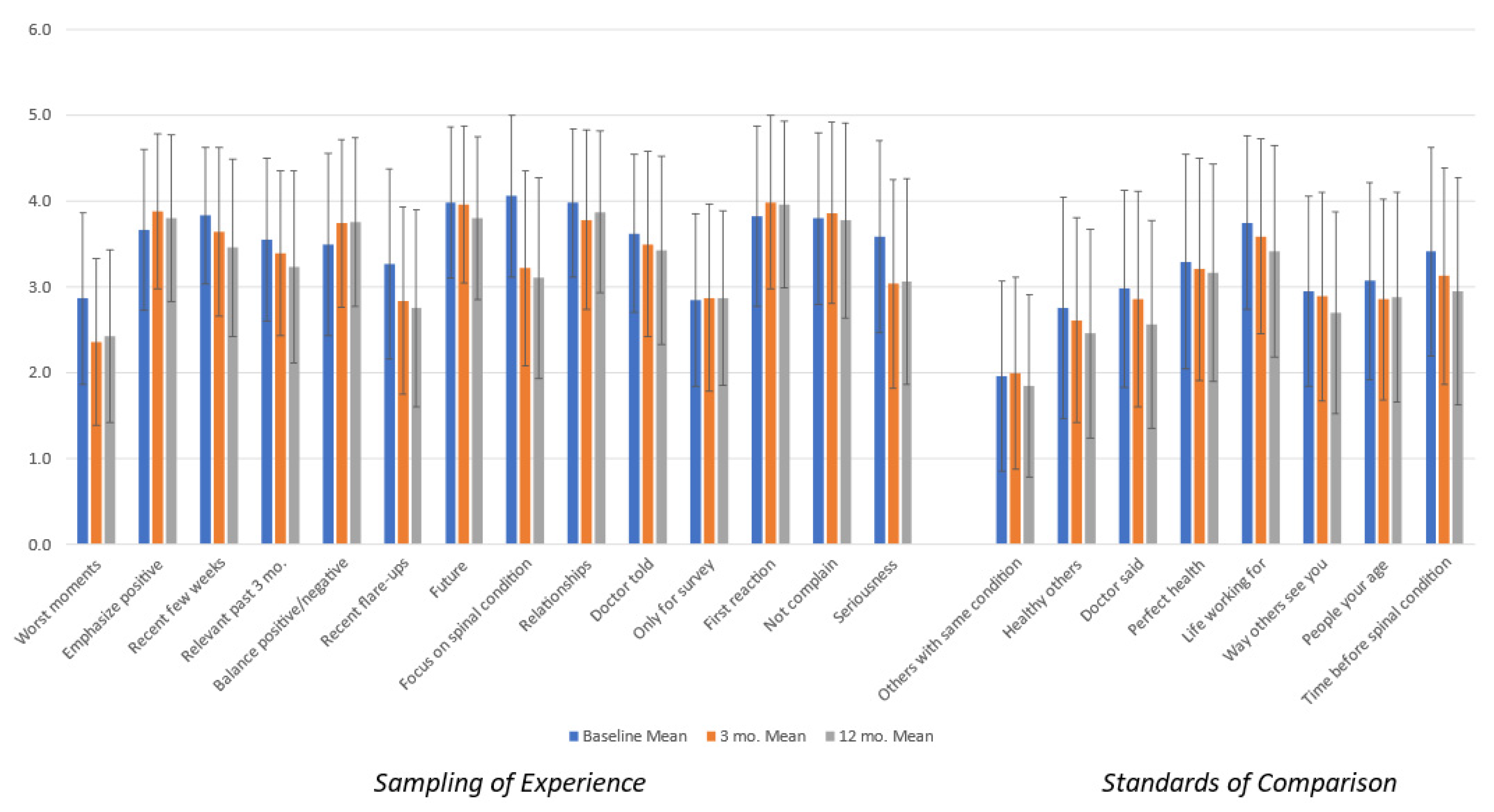
Figure 2 shows the appraisal means for the overall sample, revealing that over time patients generally de-emphasized their worst moments, recent flare-ups, and their spinal condition. The error bars shown on the figure suggest that there is substantial variability at each time point, which is consistent with the premise of the appraisal theory that notable differences in appraisal processes appear both between individuals and within individuals over time in response to a catalyst (i.e., health-state change) [18,21,22].
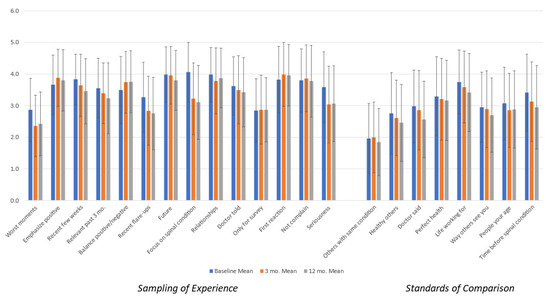
Figure 2.
Overall appraisal means and standard deviations by time point.
Accordingly, Table 3 provides a comparison of changes in appraisal item endorsement over time by the ODI-change group for the two time intervals using Cohen’s d ES. (Due to concerns about the small sample sizes in some groups, we also evaluated Hedge’s g in the two time intervals and found highly similar results). Conditional formatting indicates the magnitude and direction of the ESs: the more saturated the color, the larger the effect, and pink fill indicates a negative direction (i.e., later appraisal-endorsement items are smaller than earlier scores) while green fill indicates a positive direction (i.e., later appraisal-endorsement items are larger than earlier scores).
Table 3.
Appraisal change for two time windows: Cohen’s d.
During the first interval, individuals decreasingly tended to focus on their spinal condition when considering people in disability-worsened group as compared to the large-effect (improvement) group. In fact, focusing on one’s spinal condition had the largest magnitude of Cohen’s d value for the large-effect group. Additionally, while the disability-worsened group increased their focus on the worst moments and the seriousness of their condition during the first interval, the large-effect group decreased their focus on these areas to a similar degree. Finally, during the first interval, those in the medium and large ES groups did not shift in their focus on what their doctor told them, whereas there was a small increase for those whose disability worsened and a small decrease for those in the no-effect or small-effect groups.
During the second interval, while individuals whose disability worsened tended to increasingly focus on their spinal condition, those whose disability improved decreased their focus regarding this appraisal process. Further, whereas those whose disability worsened or did not change decreasingly focused on balancing the positive and negatives, those whose disability improved increasingly focused on this appraisal process. Next, whereas most comparisons of oneself to other standards decreased across all groups, for those whose disability improved, only a small number of individuals increased their comparison with perfect health. Finally, the medium-effect group increased their focus on balancing the positives and the negatives, while decreasing their focus on others with the same spinal condition. This pattern was not observed for those in the large-effect group.
In addition to group differences within each interval, there were also notable patterns of differences between the first and second interval. For example, there were more medium and large changes in the first as compared to the second time interval. Further, there were notable group differences in the magnitude and direction of appraisal change in the first interval, which are seen to a lesser degree in the second interval. For example, individuals whose disability worsened tended to increase their endorsement of selected appraisal processes (e.g., worse moments, the seriousness of their condition, comparing themselves to the life they are working for, etc.), whereas those with no disability change (i.e., the no-effect group) tended to decrease their endorsement of other appraisal processes (e.g., emphasizing the positive, focusing on the future, their spinal condition, or relationships, and comparing themselves to healthy others). Further, those with small, medium or large ES changes in ODI in this first interval tended to increase their focus on still other appraisal processes, increasingly focusing on emphasizing the positive, balancing the positives and the negatives, and sharing their first reaction, and decreasingly focus on their worst moments. In the second time interval, the effect sizes were generally small, and fewer group differences emerged in the direction of appraisal change.
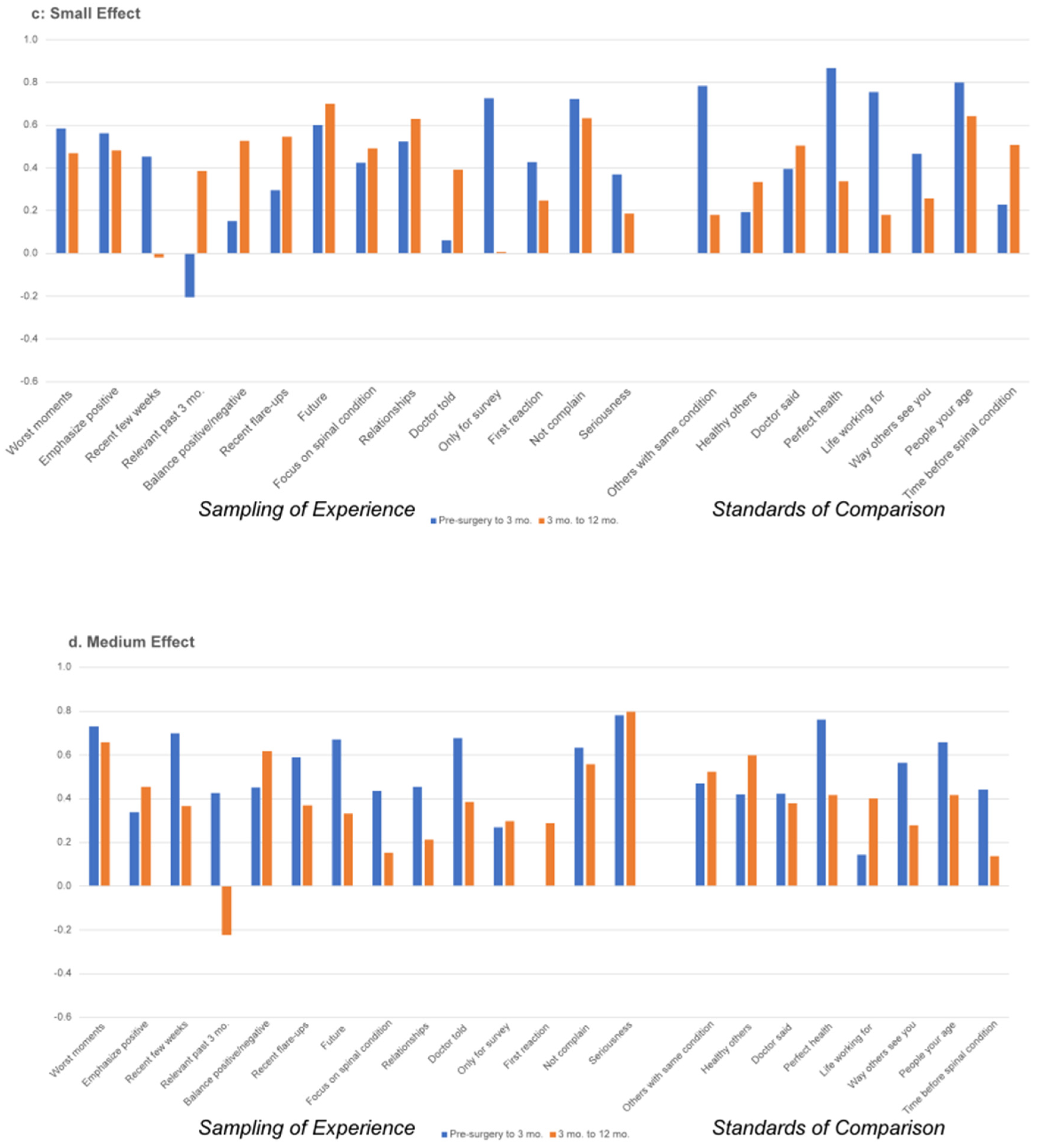
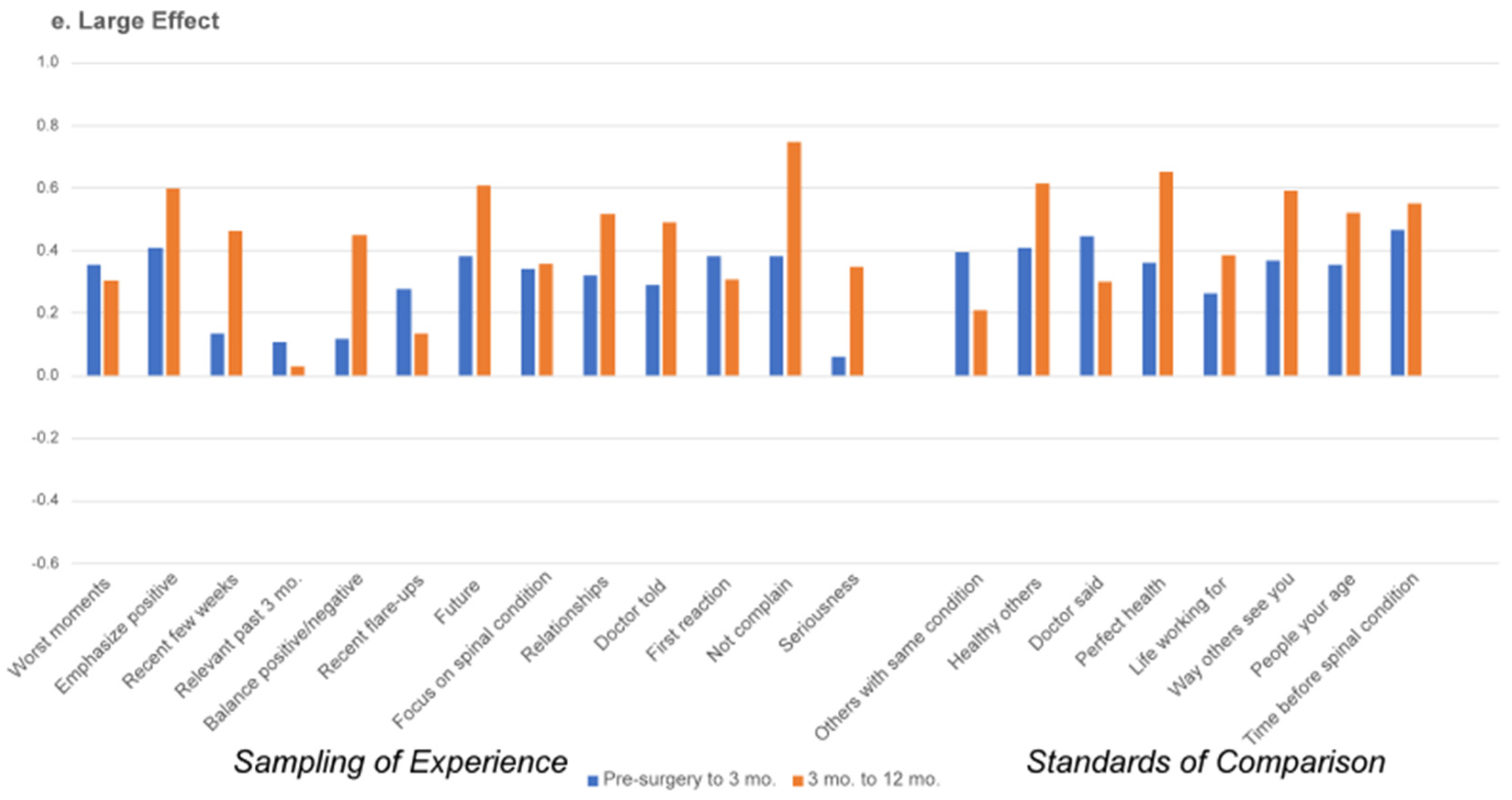
Figure 3a–e display the Pearson correlation coefficients between appraisal processes in the first and second interval by ODI-change group. These figures suggest that for those with large ES improvements in spine-related disability, there is increasing stability (i.e., a higher correlation) in appraisal processes used by those large-ES patients in the second interval as compared to the large-ES patients in the first interval post-surgery. In other words, among patients who experienced a large reduction in spine-specific disability between 3 and 12 months post-surgery, there was consistent endorsement of specific appraisal processes (Figure 3e). By comparison, there was lesser consistency in appraisal processes endorsed in those patients who experienced a large reduction in spine-specific disability between pre-surgery and 3 months post-surgery (Figure 3e). For those with small and medium ES improvements, there are less apparent differences in the stability of appraisal processes, and the earlier interval often has higher correlations between pre-surgery and 3 months).

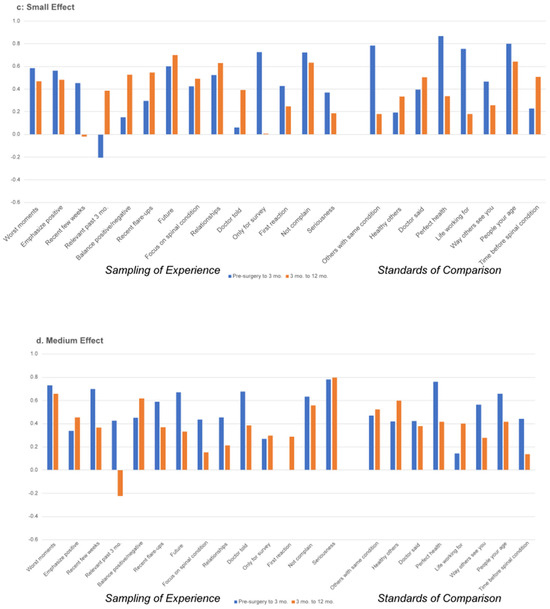
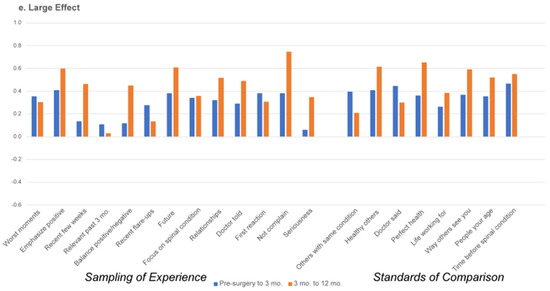
Figure 3.
(a–e) Appraisal item stability by magnitude of ODI change: comparison between first and second time intervals.
4. Discussion
This study is among the first to address the stability or changeability of QOL appraisal processes in the context of recovery from a major health intervention. We found that proximity to the catalyst of spine surgery led to more changes in Sampling of Experience appraisals (i.e., more changes in appraisal processes in the first interval, not the second interval), which is consistent with the response-shift theory [18]. In contrast, we found that changes in Standards of Comparison appraisals were more prominent later in the recovery trajectory rather than earlier. Further, the ODI-change groups were more similar in their changes in Standards of Comparison in this second interval, with almost all changes suggesting decreasing endorsements of such comparisons. Finally, we found that those whose disability decreased quite a bit in the second time interval exhibited greater stability overall in the appraisal processes endorsed. In contrast, the other disability-change groups showed more changeability in appraisal within and across time intervals.
Our results also underscore the personalized nature of ODI change after surgery. Given that spinal disorders are degenerative processes, it is likely that some deterioration over an extended time period after surgery is due to the natural history of continued progression. In some cases, individuals may not have shown improvement at three months, but then show considerable improvement at twelve months post-surgery. Further, al-though not directly related to the research question at hand, our findings also have implications for the concept of a minimal clinically important difference. The ODI change that reflected a large ES change using distribution-based methods (i.e., based on the standard deviation) was also the same number as that suggested by Copay and colleagues as a minimal clinically important difference (emphasis added) [32] and smaller than the number suggested by Nakarai and colleagues [33]. Recent systematic reviews also noted a wide range of MCID values for the same patient-reported spine-outcome measure [34,35], underscoring why it is problematic to treat it as a stable and consistent indicator of minimally important change. In addition to this empirical evidence of the variability and sample-specific nature of the MCID, the response-shift theory would hypothesize that the magnitude of the MCID would depend on many contextual factors, including stable characteristics of the individual (i.e., antecedents), the individual’s coping approaches (i.e., mechanisms), the cognitive-appraisal processes favored by the individual at a particular time (i.e., appraisal), and the impact of the catalyst on perceived functional change (i.e., change in QOL).
4.1. Clinical Implications
Our findings suggest that changes in appraisal differ depending on the individual’s experience of the impact of spine surgery. Building on a substantial evidence base documenting the effectiveness of cognitive–behavioral treatments for chronic pain [36], past research on appraisal has noted that some appraisal processes, such as focusing on the positive, appear to be adaptive because they co-vary with better outcomes [37,38]. The present work seems to provide a more nuanced perspective, suggesting that when patients’ outcomes are better, they focus on more positive appraisal processes. Conversely, when their outcomes are worse, they focus on more negative appraisal processes. Thus, actual functioning and self-reported outcomes are always a product of an ongoing “dialogue” between the perception and interpretation of one’s level of and change in functioning. This is akin to the chicken-and-egg question: are positive appraisals supportive of better outcomes or are better outcomes causally related to more positive appraisals? Future research might formally test this research question by randomizing patients to a coaching intervention where more positively focused appraisals were emphasized and comparing the impact of the intervention as a function of improvement in spine-related disability.
4.2. Limitations
The present work is limited by the relatively small ODI-change subgroup sample sizes for all but the large-ES group in the first interval and the disability-worsened group in the second interval. Although we used ES rather than p-values to characterize notable changes, the study findings must be interpreted with caution and should be replicated in more robust sample sizes. Future work in larger patient samples might stratify the analyses by age group (e.g., young adult vs. older adult) and by diagnosis to investigate whether findings differ by group. Additionally, future work might also consider the impact of psychological profiles as moderators of the appraisal–outcome relationship.
5. Conclusions
Cognitive-appraisal processes related to Sampling of Experience showed greater change soon after surgery, whereas Standards of Comparison appraisals changed more later in the recovery trajectory. Among the small proportion of patients who experienced a worsening of spine-related disability, they tended to focus on and emphasize different appraisal processes than those who experienced no change. Among the larger proportion of patients who experienced greater degrees of improvement, they tended to emphasize still other appraisal processes. These findings suggest that appraisal processes reflect an ongoing dynamic in adaptation to changing function.
Author Contributions
Conceptualization, C.E.S., K.B., B.D.R. and J.A.F.; methodology, C.E.S. and K.B.; software, K.B.; validation, C.E.S., K.B. and B.D.R.; formal analysis, C.E.S. and K.B.; data curation, K.B.; writing—original draft preparation, C.E.S.; writing—review and editing, C.E.S., K.B., B.D.R. and J.A.F.; visualization, C.E.S.; supervision, C.E.S.; project administration, C.E.S. and J.A.F.; funding acquisition, J.A.F. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Feldberg Chair in Spinal Research, Sunnybrook Health Sciences Centre.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the Sunnybrook Health Centre Research Ethics Board (Protocol #2591, 1 November 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used in these analyses are confidential and thus not able to be shared.
Acknowledgments
The authors are grateful to the study participants, without whom this work would not be possible.
Conflicts of Interest
The authors declare no conflicts of interest.
Notes
| 1 | Hedge’s g is interpreted as follows: 0.15 to 0.359 is a small effect, 0.36–0.649 is a medium effect, and >0.65 is a large effect. |
References
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Skinner, J.S.; Hanscom, B.; Tosteson, A.N.; Herkowitz, H.; Fischgrund, J.; Cammisa, F.P.; Albert, T.; et al. Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006, 296, 2451–2459. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Tosteson, A.N.; Blood, E.; Abdu, W.A.; Herkowitz, H.; Hilibrand, A.; Fischgrund, J. Surgical versus non operative treatment for lumbar disc herniation: Four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine 2008, 33, 2789–2800. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D.; et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N. Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef]
- Khor, S.; Lavallee, D.C.; Cizik, A.M.; Bellabarba, C.; Dagal, A.; Hart, R.A.; Howe, C.R.; Martz, R.D.; Shonnard, N.; Flum, D.R. Hospital and surgeon variation in patient-reported functional outcomes after lumbar spine fusion: A statewide evaluation. Spine 2020, 45, 465–472. [Google Scholar] [CrossRef]
- Alvin, M.D.; Lubelski, D.; Alam, R.; Williams, S.K.; Obuchowski, N.A.; Steinmetz, M.P.; Wang, J.C.; Melillo, A.J.; Pahwa, A.; Benzel, E.C. Spine surgeon treatment variability: The impact on costs. Glob. Spine J. 2018, 8, 498–506. [Google Scholar] [CrossRef]
- Block, A.R.; Gatchel, R.J.; Deardorff, W.W.; Guyer, R.D. The Psychology of Spine Surgery; American Psychological Association: Washington, DC, USA, 2003. [Google Scholar]
- Kaptain, G.J.; Shaffrey, C.I.; Alden, T.D.; Young, J.N.; Whitehill, R. The influence of secondary gain on surgical outcome: A comparison between cervical and lumbar discectomy. Neurosurg. Focus 1998, 5, e6. [Google Scholar] [CrossRef]
- Crombez, G.; Vlaeyen, J.W.; Heuts, P.H.; Lysens, R. Pain-related fear is more disabling than pain itself: Evidence on the role of pain-related fear in chronic back pain disability. Pain 1999, 80, 329–339. [Google Scholar] [CrossRef]
- Kanaan, S.F.; Melton, B.L.; Waitman, L.R.; Simpson, M.H.; Sharma, N.K. The effect of age and gender on acute postoperative pain and function following lumbar spine surgeries. Physiother. Res. Int. 2021, 26, e1888. [Google Scholar] [CrossRef]
- Finkelstein, J.A.; Stark, R.B.; Lee, J.; Schwartz, C.E. Patient factors that matter in predicting spine surgery outcomes: A machine learning approach. J. Neurosurg. Spine 2021, 35, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.K.; Herr, K.A.; Sohn, J.N.; Cha, B.K.; Yom, Y.H. Prediction of pain outcomes in Korean older adults: Use of a structural equation model. Pain Med. 2007, 8, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Karp, J.F.; Reynolds, C.F., III; Butters, M.A.; Dew, M.A.; Mazumdar, S.; Begley, A.E.; Lenze, E.; Weiner, D.K. The relationship between pain and mental flexibility in older adult pain clinic patients. Pain Med. 2006, 7, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Kerns, R.D. Evidence that cognitive decline mediates the relationship between pain and disability in the elderly. Pain Med. 2006, 7, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Spinhoven, P.; Ter, K.M.; Kole-Snijders, A.M.; Hutten, M.M.; Den Ouden, D.J.; Vlaeyen, J.W. Catastrophizing and internal pain control as mediators of outcome in the multidisciplinary treatment of chronic low back pain. Eur. J. Pain 2004, 8, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.E.; Rapkin, B.D.; Borowiec, K.; Finkelstein, J.A. Cognitive processes during recovery: Moving toward personalized spine surgery outcomes. J. Pers. Med. 2022, 12, 1545. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. An analysis of coping in a middle-aged community sample. J. Health Soc. Behav. 1980, 21, 219–239. [Google Scholar] [CrossRef]
- Tourangeau, R.; Rips, L.J.; Rasinski, K. The Psychology of Survey Response; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Rapkin, B.D.; Schwartz, C.E. Toward a theoretical model of quality-of-life appraisal: Implications of findings from studies of response shift. Health Qual. Life Outcomes 2004, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Sprangers, M.A.G.; Schwartz, C.E. Integrating response shift into health-related quality of life research: A theoretical model. Soc. Sci. Med. 1999, 48, 1507–1515. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Stark, R.B.; Rapkin, B.D. Creating idiometric short-form measures of cognitive appraisal: Balancing theory and pragmatics. J. Patient-Rep. Outcomes 2021, 5, 57. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Stark, R.B.; Rapkin, B.D. Capturing patient experience: Does quality-of-life appraisal entail a new class of measurement? J. Patient-Rep. Outcomes 2020, 4, 85. [Google Scholar] [CrossRef]
- Rapkin, B.D.; Schwartz, C.E. Advancing quality-of-life research by deepening our understanding of response shift: A unifying theory of appraisal. Qual. Life Res. 2019, 28, 2623–2630. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.E.; Borowiec, K.; Rapkin, B.D. Depression trajectories during the COVID-19 pandemic: A secondary analysis of the impact of cognitive-appraisal processes. J. Patient-Rep. Outcomes 2023, 7, 67. [Google Scholar] [CrossRef]
- Alchemer. Boulder, CO, USA. Available online: https://www.alchemer.com (accessed on 19 March 2024).
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef] [PubMed]
- Sangha, O.; Stucki, G.; Liang, M.H.; Fossel, A.H.; Katz, J.N. The Self-Administered Comorbidity Questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Care Res. 2003, 49, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Rosnow, R.L.; Rosenthal, R. Effect sizes for experimenting psychologists. Can. J. Exp. Psychol./Rev. Can. De Psychol. Expérimentale 2003, 57, 221–237. [Google Scholar] [CrossRef]
- Brydges, C.R. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov. Aging 2019, 3, igz036. [Google Scholar] [CrossRef]
- Lovakov, A.; Agadullina, E.R. Empirically derived guidelines for effect size interpretation in social psychology. Eur. J. Soc. Psychol. 2021, 51, 485–504. [Google Scholar] [CrossRef]
- IBM. IBM SPSS Statistics for Windows, version 26; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef]
- Nakarai, H.; Kato, S.; Kawamura, N.; Higashikawa, A.; Takeshita, Y.; Fukushima, M.; Ono, T.; Hara, N.; Azuma, S.; Tanaka, S. Minimal clinically important difference in patients who underwent decompression alone for lumbar degenerative disease. Spine J. 2022, 22, 549–560. [Google Scholar] [CrossRef]
- Copay, A.G.; Chung, A.S.; Eyberg, B.; Olmscheid, N.; Chutkan, N.; Spangehl, M.J. Minimum clinically important difference: Current trends in the orthopaedic literature, part I: Upper extremity: A systematic review. JBJS Rev. 2018, 6, e1. [Google Scholar] [CrossRef]
- Copay, A.G.; Eyberg, B.; Chung, A.S.; Zurcher, K.S.; Chutkan, N.; Spangehl, M.J. Minimum clinically important difference: Current trends in the orthopaedic literature, part II: Lower extremity: A systematic review. JBJS Rev. 2018, 6, e2. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.; Morley, S. Cognitive-behavioral treatments for chronic pain: What works for whom? Clin.J.Pain 2005, 21, 1–8. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Zhang, J.; Rapkin, B.D.; Finkelstein, J.A. Reconsidering the minimally important difference: Evidence of instability over time and across groups. Spine J. 2019, 19, 726–734. [Google Scholar] [CrossRef]
- Sniderman, J.; Stark, R.B.; Schwartz, C.E.; Imam, H.; Finkelstein, J.A.; Nousiainen, M.T. Patient Factors That Matter in Predicting Hip Arthroplasty Outcomes: A Machine-Learning Approach. J. Arthroplast. 2021, 36, 2024–2032. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).