
The Effects of Different Types of Steroids on Clinical Outcomes in Neonates with Meconium Aspiration Syndrome: A Systematic Review, Meta-Analysis and GRADE Assessment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Risk-of-Bias (Quality) Assessment
2.3. Data Analyses
2.4. Quality of Evidence
3. Results
3.1. Search Strategy and Selection Criteria
3.2. Data Extraction and Risk-of-Bias Assessment
Study Characteristics
- Delivery of MSAF infants and retrieval of meconium from below the larynx on endotracheal tube suction;
- Development of respiratory distress within 4 to 6 h after birth and persistence beyond 24 h;
- Chest X-ray findings of infiltrates, hyperinflation, and atelectasis;
- Absence of any other causes of respiratory distress.
- Sepsis [30]
- Presence of clinical signs: poor feeding, weight loss, lethargy, temperature instability, sclerema, and capillary refill time of >3 s and;
- Positive blood culture, or;
- Two or more of the following laboratory abnormalities:
- (a)
- Total leukocyte count of <5000/mm3 or >30,000/mm3;
- (b)
- Immature/total neutrophil ratio of >0.2;
- (c)
- Micro-erythrocyte sedimentation rate of >5 mm in the first hour on the first day of life or >15 mm at any time;
- (d)
- Positive C-reactive protein.
3.3. Risk-of-Bias Assessment
3.4. Data Analyses
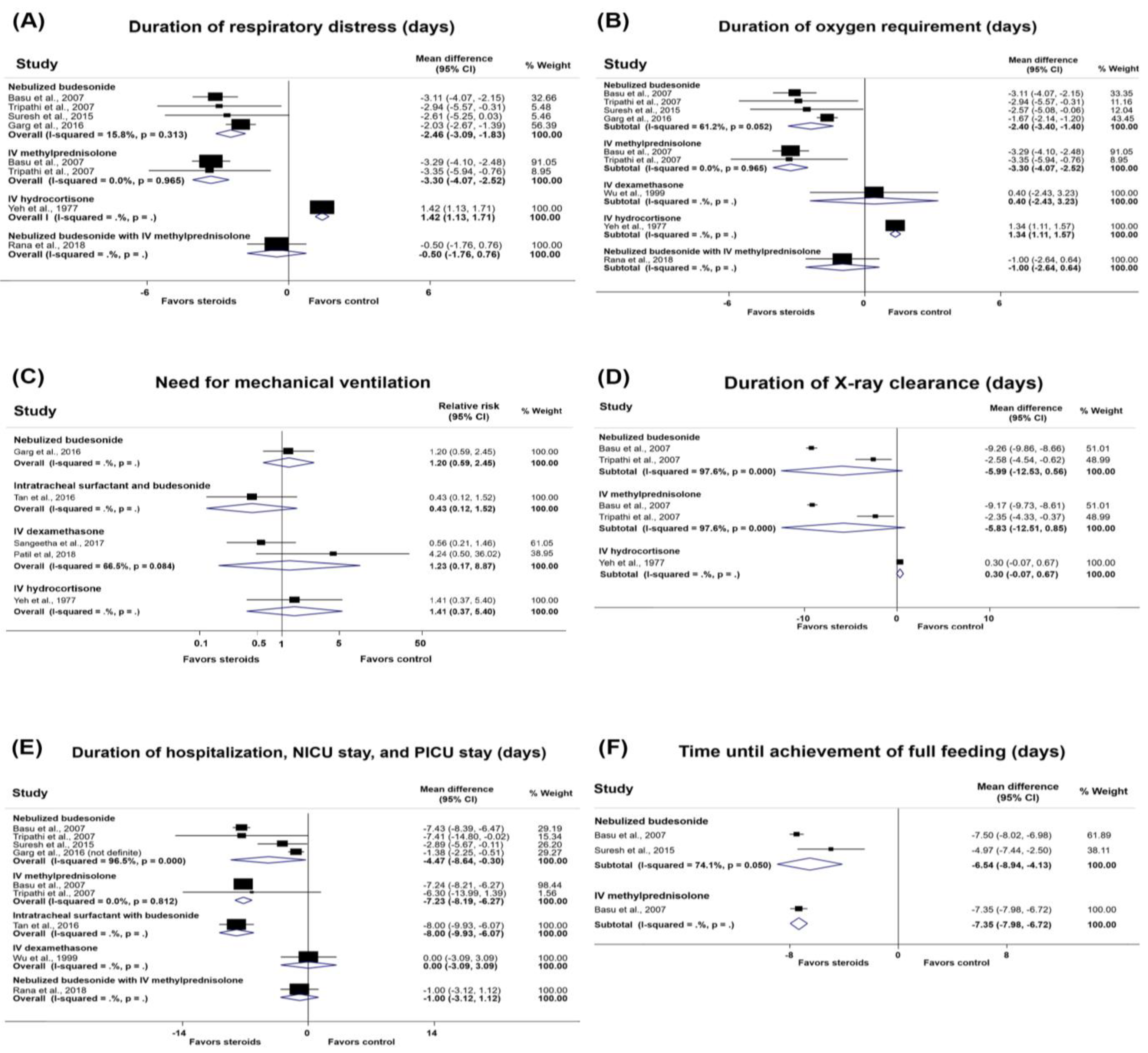
3.4.1. Duration of Respiratory Distress
3.4.2. Duration of Oxygen Requirement
3.4.3. Need for Mechanical Ventilation
3.4.4. Duration of Mechanical Ventilation
3.4.5. Downes’ Score
3.4.6. Duration of X-ray Clearance
3.4.7. Duration of Hospitalization, Neonatal Intensive Care Unit Stay, and Pediatric Intensive Care Unit Stay
3.4.8. Time until Achievement of Full Feeding
3.4.9. Duration of IV Fluid Requirement
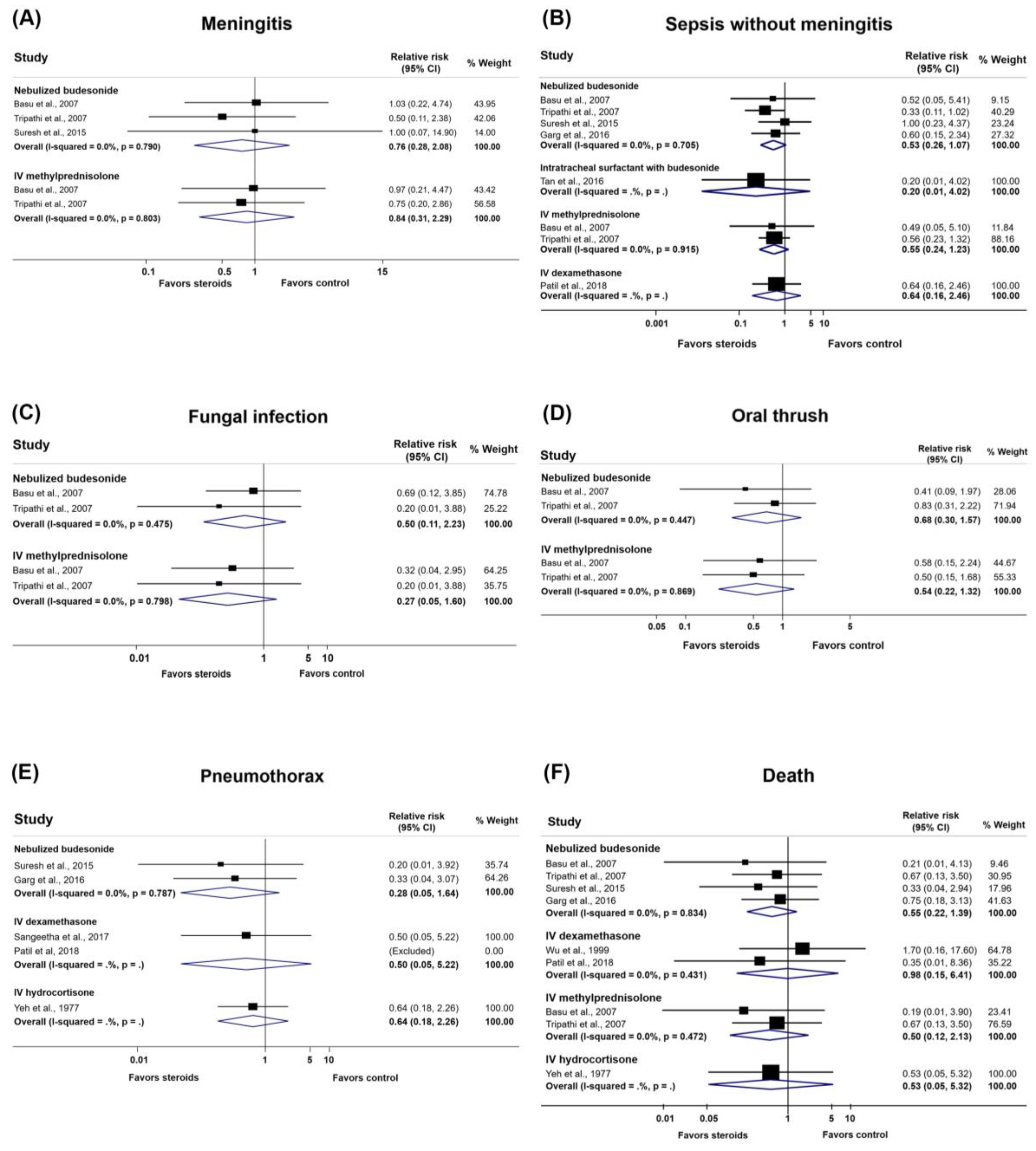
3.4.10. Infections and Complications
3.4.11. Death
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raju, U.; Sondhi, V.; Patnaik, S.K. Meconium Aspiration Syndrome: An Insight. Med. J. Armed Forces India 2010, 66, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Parker, T.A.; Kinsella, J.P. Respiratory Disorders in the Term Infant. In Avery’s Diseases of the Newborn, 10th ed.; Gleason, C.A., Juul, S.E., Eds.; Elsevier: Philadelphia, PA, USA, 2018. [Google Scholar]
- Gelfand, S.L.; Fanaroff, J.M.; Walsh, M.C. Meconium stained fluid: Approach to the mother and the baby. Pediatr. Clin. N. Am. 2004, 51, 655–667. [Google Scholar] [CrossRef]
- Greenough, A.; Pulikot, A.; Dimitriou, G. Prevention and management of meconium aspiration syndrome—assessment of evidence based practice. Eur. J. Pediatr. 2005, 164, 329–330. [Google Scholar] [CrossRef]
- Sawyer, T.L.; Rosenkrantz, T. Intubation and Tracheal Suctioning for Meconium Aspiration. Available online: https://emedicine.medscape.com/article/1413467 (accessed on 19 November 2020).
- Viraraghavan, V.R.; Nangia, S.; Prathik, B.H.; Madarkar, B.S.; Rani, D.; Saili, A. Yield of meconium in non-vigorous neonates undergoing endotracheal suctioning and profile of all neonates born through meconium-stained amniotic fluid: A prospective observational study. Paediatr. Int. Child Health 2018, 38, 266–270. [Google Scholar] [CrossRef]
- Vivian-Taylor, J.; Sheng, J.; Hadfield, R.M.; Morris, J.M.; Bowen, J.R.; Roberts, C.L. Trends in obstetric practices and meconium aspiration syndrome: A population-based study. BJOG 2011, 118, 1601–1607. [Google Scholar] [CrossRef]
- Paudel, P.; Sunny, A.K.; Poudel, P.G.; Gurung, R.; Gurung, A.; Bastola, R.; Chaudhary, R.N.; Budhathoki, S.S.; Ashish, K.C. Meconium aspiration syndrome: Incidence, associated risk factors and outcome-evidence from a multicentric study in low-resource settings in Nepal. J. Paediatr. Child Health 2020, 56, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.S.; Clark, R.H.; Powers, R.J.; Spitzer, A.R. Meconium aspiration syndrome remains a significant problem in the NICU: Outcomes and treatment patterns in term neonates admitted for intensive care during a ten-year period. J. Perinatol. 2009, 29, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Gurubacharya, S.M.; Rajbhandari, S.; Gurung, R.; Rai, A.; Mishra, M.; Sharma, K.; Aryal, D. Risk factors and outcome of neonates born through meconium stained amniotic fluid in a tertiary hospital of Nepal. J. Nepal Paediatr. Soc. 2015, 35, 44–48. [Google Scholar] [CrossRef]
- Sharma, V.; Berkelhamer, S.; Lakshminrusimha, S. Persistent pulmonary hypertension of the newborn. Matern. Health Neonatol. Perinatol. 2015, 1, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidalgo, H.A.; Helmke, R.J.; German, V.F.; Mangos, J.A. The effects of cyclosporine and dexamethasone on an alveolar macrophage cell line (NR8383). Transplantation 1992, 53, 620–623. [Google Scholar] [CrossRef]
- Barnes, P.J.; Pedersen, S. Efficacy and safety of inhaled corticosteroids in asthma. Report of a workshop held in Eze, France, October 1992. Am. Rev. Respir. Dis. 1993, 148 Pt 2, S1–S26. [Google Scholar] [CrossRef] [PubMed]
- Brattsand, R.; Linden, M. Cytokine modulation by glucocorticoids: Mechanisms and actions in cellular studies. Aliment. Pharmacol. Ther. 1996, 10 (Suppl. S2), 81–90. [Google Scholar] [CrossRef]
- Ward, M.; Sinn, J. Steroid therapy for meconium aspiration syndrome in newborn infants. Cochrane Database Syst. Rev. 2003, 2003, Cd003485. [Google Scholar] [CrossRef]
- Contributed by the CLARITY Group at McMaster University Tool to Assess Risk of Bias in Randomized Controlled Trials. Available online: https://www.evidencepartners.com/resources/methodological-resources/tool-to-assess-risk-of-bias-in-randomized-controlled-trials-distillersr (accessed on 24 February 2021).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ (Clin. Res. Ed.) 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clin. Res. Ed.) 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Davey, A.M.; Kueser, T.J.; Turner, H.F. Randomized controlled trial of early dexamethasone therapy in the treatment of meconium aspiration syndrome. Pediatr. Res. 1995, 37, 329. [Google Scholar]
- Yeh, T.; Srinivasan, G.; Harris, V.; Pildes, R.S. Hydrocortisone therapy in meconium aspiration syndrome: A controlled study. J. Pediatr. 1977, 90, 140–143. [Google Scholar] [CrossRef]
- Wu, J.M.; Yeh, T.F.; Wang, J.Y.; Wang, J.N.; Lin, Y.J.; Hsieh, W.S.; Lin, C.H. The role of pulmonary inflammation in the development of pulmonary hypertension in newborn with meconium aspiration syndrome (MAS). Pediatri. Pulm. Suppl. 1999, 18, 205–208. [Google Scholar] [CrossRef]
- Basu, S.; Kumar, A.; Bhatia, B.D.; Satya, K.; Singh, T.B. Role of steroids on the clinical course and outcome of meconium aspiration syndrome —A randomized controlled trial. J. Trop. Pediatr. 2007, 53, 331–337. [Google Scholar] [CrossRef]
- Tripathi, S.; Saili, A. The effect of steroids on the clinical course and outcome of neonates with Meconium Aspiration Syndrome. J. Trop. Pediatr. 2007, 53, 8–12. [Google Scholar] [CrossRef]
- Suresh, R.; Sudha, R.; Pinto, N.; Pradeep, N. Effect of nebulized Budesonide in improving the clinical outcome of neonates with meconium aspiration syndrome. Int. J. Biol. Med. Res. 2015, 6, 4942–4945. [Google Scholar]
- Garg, N.; Choudhary, M.; Sharma, D.; Dabi, D.; Choudhary, J.S.; Choudhary, S.K. The role of early inhaled budesonide therapy in meconium aspiration in term newborns: A randomized control study. J. Matern. Fetal Neonatal. Med. 2016, 29, 36–40. [Google Scholar] [CrossRef]
- Tan, X.Z.; Wu, S.G.; Zhang, J.H.; Li, X.F.; Gao, P.M.; Wang, Y. Clinical efficacy of porcine pulmonary surfactant combined with budesonide suspension intratracheal instillation in the treatment of neonatal meconium aspiration syndrome. Zhongguo Dang Dai Er Ke Za Zhi 2016, 18, 1237–1241. [Google Scholar]
- Sangeetha, T.; Ramanathan, R.; Yogavalli, S. Effectiveness of steroid therapy in newborns with meconium aspiration syndrome. J. Med. Sci. Clin. Res. 2017, 5, 22587–22590. [Google Scholar]
- Patil, M.M.; Lakhkar, B.B.; Patil, S.V. Dexamethasone and outcome of meconium aspiration syndrome: Vijayapur, Karnataka experience. Sri Lanka J. Child Health 2018, 47, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Rana, K.S.; Konar, M.C.; Islam, K.; Barik, K.L.; Nayek, K.; Datta, A.K. Study on effects of steroid on clinical course, short-term and long-term outcomes in neonates with meconium aspiration syndrome. J. Neonat. Nurs. 2018, 24, 257–260. [Google Scholar] [CrossRef]
- Mikolka, P.; Kopincova, J.; Tomcikova Mikusiakova, L.; Kosutova, P.; Antosova, M.; Calkovska, A.; Mokra, D. Effects of surfactant/budesonide therapy on oxidative modifications in the lung in experimental meconium-induced lung injury. J. Physiol. Pharmacol. 2016, 67, 57–65. [Google Scholar]
- Monfredini, C.; Cavallin, F.; Villani, P.E.; Paterlini, G.; Allais, B.; Trevisanuto, D. Meconium Aspiration Syndrome: A Narrative Review. Children 2021, 8, 230. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Yeh et al., 1977 [28] | Wu et al., 1999 [29] | Basu et al., 2007 [30] | Tripathi et al., 2007 [31] | Suresh et al., 2015 [32] | Garg et al., 2016 [33] | Tan et al., 2016 [34] | Sangeetha et al., 2017 [35] | Patil et al., 2018 [36] | Rana et al., 2018 [37] |
|---|---|---|---|---|---|---|---|---|---|---|
| Type of study | RCT | RCT | RCT | RCT | RCT | RCT | RCT | RCT | RCT | RCT |
| Location | Illinois, USA | Taipei, Taiwan | Varanasi, India | New Delhi, India | Karnataka, India | Rajasthan, India | Foshan Nanhai, China | Chidambaram, India | Karnataka, India | West Bengal, India |
| Inclusion criteria |
|
|
|
|
|
|
|
|
|
|
| Exclusion criteria | - | - |
|
|
|
|
|
|
|
|
| Randomization | Random number table | Randomization method not mentioned | Computer-generated random numbers | Computer-generated random numbers | Computer-generated random numbers | Computer-generated random numbers | Randomization method not mentioned | Randomization method not mentioned | Randomization method not mentioned | Randomization method not mentioned |
| Study period | 1 year (October 1974 to September 1975) | NR | 1 year | 1 year | 3 months (August to October 2013) | 5 months (May 2010 to December 2010) | 2 years (December 2013 to December 2015) | 1 year | 18 months | 3 years (April 2014 to March 2017) |
| All groups received | Standard care as protocol | Standard care as protocol | Supportive treatment as protocol of nursery | Standard care as unit protocol | Supportive treatment as protocol of nursery | Standard care as protocol | PS 100 mg/kg within 2 h | Standard care as unit protocol | Standard care as protocol | Standard care |
| Control | Placebo (lactose hydrous) | NSS | None |
| Nebulized NSS |
|
| None | None |
|
| Comparator (1) | Hydrocortisone 20 mg/kg IV for first bolus dose, then continue q 12 h for 4 more doses | Dexamethas1 mg/kg IV for initial dose, then 0.5 mg/kg q 12 h for days 1–3, then 0.25 mg/kg q 12 h for days 4–7 (started shortly after birth) | Methylprednisolone 0.5 mg/kg/day IV q 12 h for 7 days (started 24–36 h after birth) |
|
|
via nebulizer system |
within 2 h of admission | Dexamethasone 0.5 mg/kg IV q 12 h for days 1–3, then 0.25 mg/kg q 12 h for days 4–7 |
|
|
| Comparator (2) | Nebulized budesonide 50 µg + NSS 2.5 mL via jet nebulizer q 12 h for 7 days (started 24–36 h after birth) |
| - | - | - | - | - | |||
| Follow up | - | - | Weekly for 2 weeks, then monthly | - | Once every 2 weeks for 3 months | - | - | - | - | 1, 3, and 6 months for any complications |
| Outcomes |
|
|
| Efficacy outcomes:
|
|
|
|
|
|
|
| Patient or Population: Neonates with MAS Intervention: Steroids Comparison: Placebo, no treatment, or usual care | ||||||
| Outcomes | No. of Participants (Studies) | Relative Effects (95% CI) | Absolute Effect Estimates | Certainty/Quality of Evidence | Plain Language Summary | |
| Baseline Risk for Control Group 1 | Difference (95% CI) | |||||
| Duration of respiratory distress (days) | ||||||
| Budesonide | 208 (4 studies) | - | The median duration of respiratory distress in the control groups was 5.71 days | MD −2.46 days (−3.09 to −1.83) | Moderate ⊕⊕⊕⊝ (serious risk of bias) | Budesonide probably reduces duration of respiratory distress. |
| Methylprednisolone | 96 (2 studies) | - | The median duration of respiratory distress in the control groups was 5.71 days | MD −3.30 days (−4.07 to −2.52) | Moderate ⊕⊕⊕⊝ (serious risk of bias) | Methylprednisolone probably reduces duration of respiratory distress. |
| Duration of oxygen requirement (days) | ||||||
| Budesonide | 208 (4 studies) | - | The median duration of oxygen requirement in the control groups was 4.94 days | MD −2.40 days (−3.40 to −1.40) | Low ⊕⊕⊝⊝ (serious risk of bias, serious inconsistency) | Budesonide may reduce duration of oxygen requirement. |
| Methylprednisolone | 96 (2 studies) | - | The median duration of oxygen requirement in the control groups was 4.94 days | MD −3.30 days (−4.07 to −2.52) | Moderate ⊕⊕⊕⊝ (serious risk of bias) | Methylprednisolone probably reduces duration of oxygen requirement. |
| Need for mechanical ventilation | ||||||
| Dexamethasone | 130 (2 studies) | 1.23 (0.17 to 8.87) | 25.00% | 5.75 (−20.75 to 196.75) | Very low ⊕⊝⊝⊝ (serious risk of bias, serious inconsistency, and serious imprecision) | The effect of dexamethasone on the need for mechanical ventilation is very uncertain. |
| Duration of hospitalization, NICU stay, and PICU stay (days) | ||||||
| Budesonide | 208 (4 studies) | - | The median duration of hospitalization/NICU stay in the control groups was 14 days | MD −4.47 days (−8.64 to −0.30) | Low ⊕⊕⊝⊝ (serious risk of bias, serious inconsistency) | Budesonide may reduce the duration of hospitalization, NICU stay, and PICU stay. |
| Methylprednisolone | 96 (2 studies) | - | The median duration of hospitalization/NICU stay in the control groups was 14 days | MD −7.23 days (−8.19 to −6.27) | Moderate ⊕⊕⊕⊝ (serious risk of bias) | Methylprednisolone probably reduces the duration of hospitalization, NICU stay, and PICU stay. |
| Infections and death | ||||||
| Meningitis | ||||||
| Budesonide | 139 (3 studies) | 0.76 (0.28 to 2.08) | 10.00% | −2.40 (−7.20 to 10.80) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Budesonide may not increase the number of participants with meningitis. |
| Methylprednisolone | 101 (2 studies) | 0.84 (0.31 to 2.29) | 10.00% | −1.60 (−6.90 to 12.90) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Methylprednisolone may not increase the number of participants with meningitis. |
| Sepsis without meningitis | ||||||
| Budesonide | 217 (4 studies) | 0.53 (0.26 to 1.07) | 15.42% | −7.25 (−11.41 to 1.08) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Budesonide may not increase the number of participants with sepsis without meningitis. |
| Methylprednisolone | 101 (2 studies) | 0.55 (0.24 to 1.23) | 15.42% | −6.94 (−11.72 to 3.55) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Methylprednisolone may not increase the number of participants with sepsis without meningitis. |
| Death | ||||||
| Budesonide | 217 (4 studies) | 0.55 (0.22 to 1.39) | 11.43% | −5.14 (−8.92 to 4.46) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Budesonide may not increase the number of participants with death. |
| Dexamethasone | 120 (2 studies) | 0.98 (0.15 to 6.41) | 11.43% | −0.23 (−9.72 to 61.84) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Dexamethasone may not increase the number of participants with death. |
| Methylprednisolone | 101 (2 studies) | 0.50 (0.12 to 2.13) | 11.43% | −5.72 (−10.06 to 12.92) | Low ⊕⊕⊝⊝ (serious risk of bias, serious imprecision) | Methylprednisolone may not increase the number of participants with death. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phattraprayoon, N.; Ungtrakul, T.; Tangamornsuksan, W. The Effects of Different Types of Steroids on Clinical Outcomes in Neonates with Meconium Aspiration Syndrome: A Systematic Review, Meta-Analysis and GRADE Assessment. Medicina 2021, 57, 1281. https://doi.org/10.3390/medicina57111281
Phattraprayoon N, Ungtrakul T, Tangamornsuksan W. The Effects of Different Types of Steroids on Clinical Outcomes in Neonates with Meconium Aspiration Syndrome: A Systematic Review, Meta-Analysis and GRADE Assessment. Medicina. 2021; 57(11):1281. https://doi.org/10.3390/medicina57111281
Chicago/Turabian StylePhattraprayoon, Nanthida, Teerapat Ungtrakul, and Wimonchat Tangamornsuksan. 2021. "The Effects of Different Types of Steroids on Clinical Outcomes in Neonates with Meconium Aspiration Syndrome: A Systematic Review, Meta-Analysis and GRADE Assessment" Medicina 57, no. 11: 1281. https://doi.org/10.3390/medicina57111281
APA StylePhattraprayoon, N., Ungtrakul, T., & Tangamornsuksan, W. (2021). The Effects of Different Types of Steroids on Clinical Outcomes in Neonates with Meconium Aspiration Syndrome: A Systematic Review, Meta-Analysis and GRADE Assessment. Medicina, 57(11), 1281. https://doi.org/10.3390/medicina57111281