
Comparison of Choroidal Thickness, Foveal Avascular Zone, and Macular Capillary Density in Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Ranibizumab or Aflibercept—A Prospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Assessment of Clinical Outcome
2.4. Statistical Analysis
3. Results
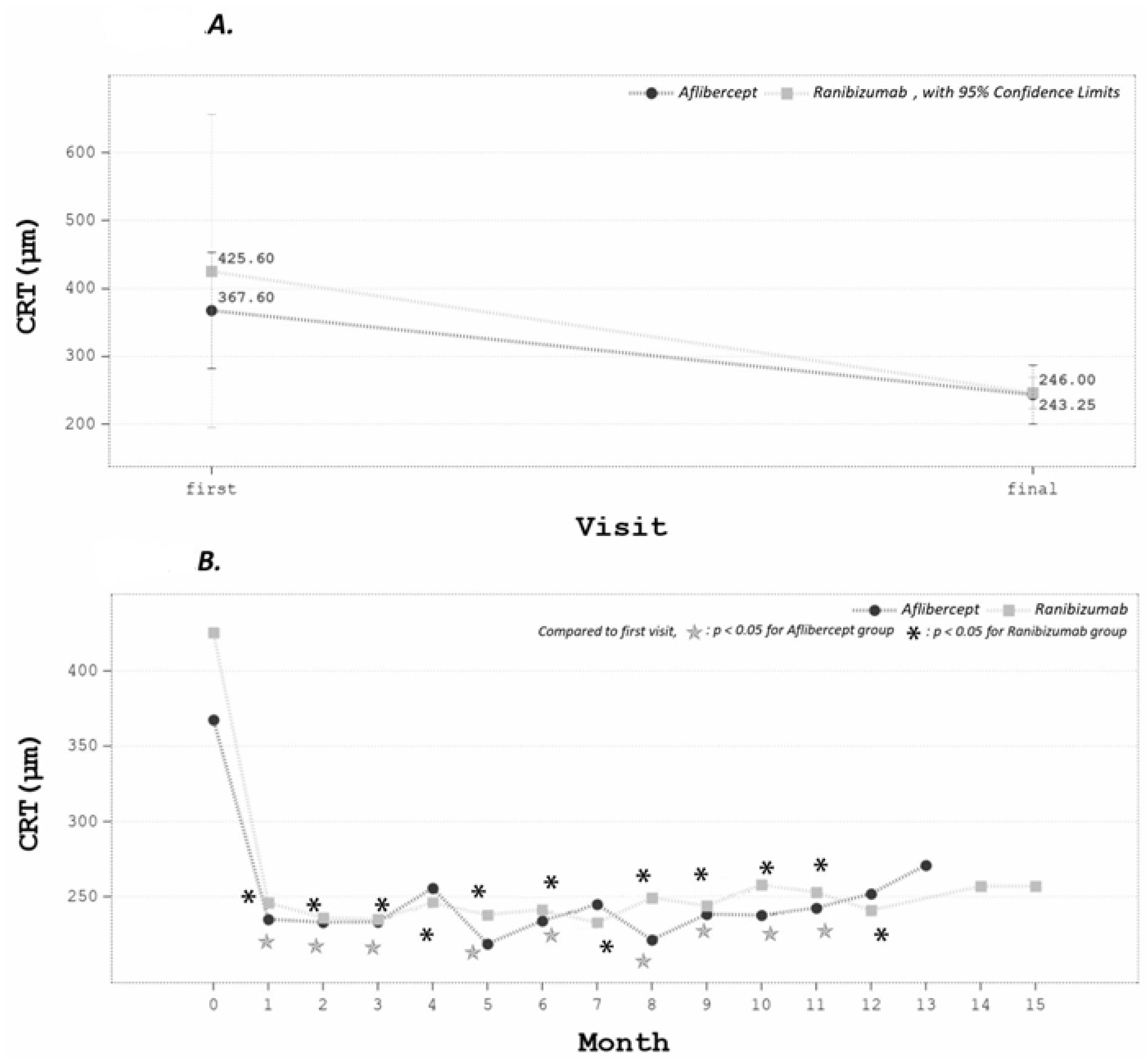
3.1. CRT Changes
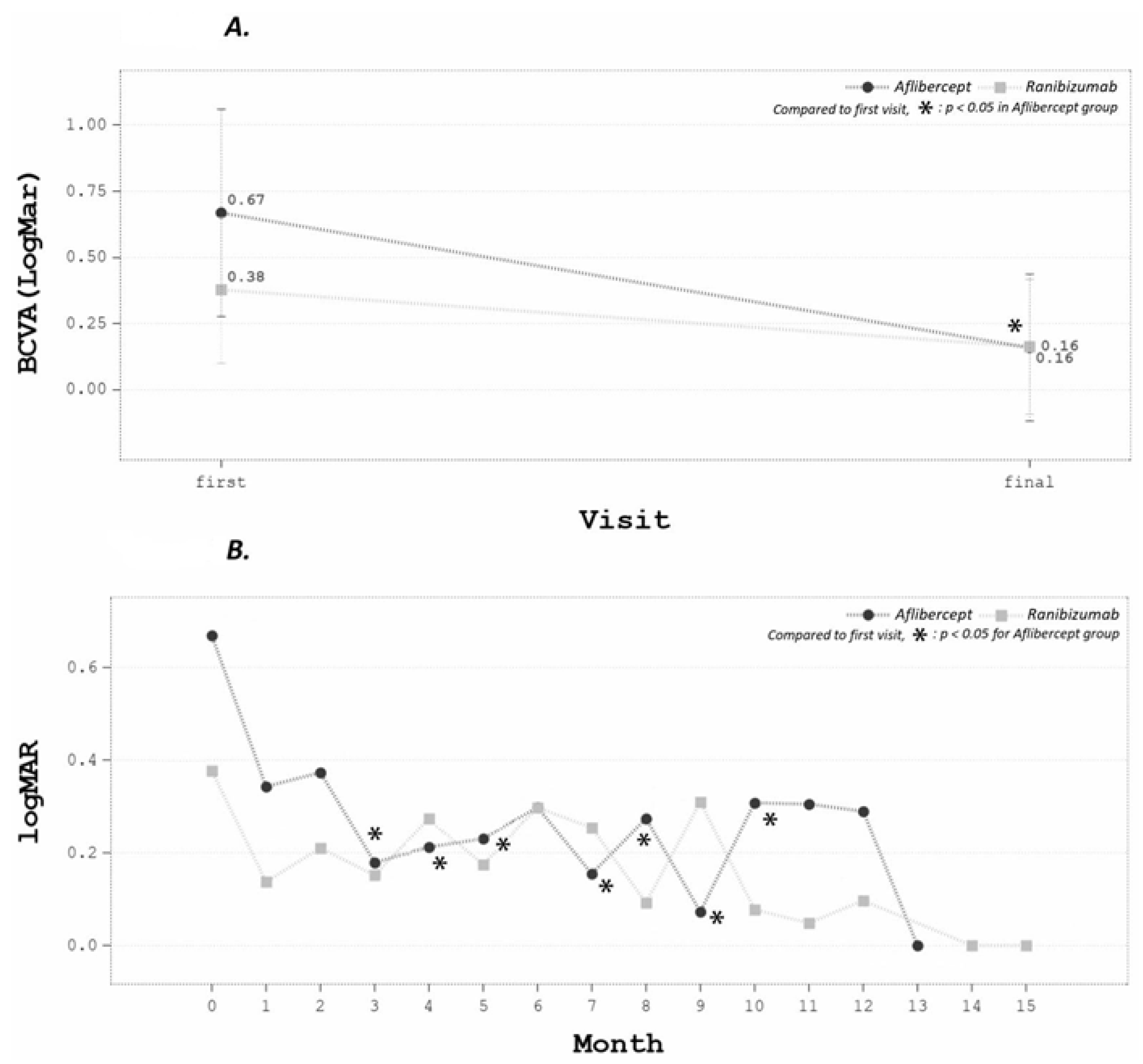
3.2. BCVA Changes
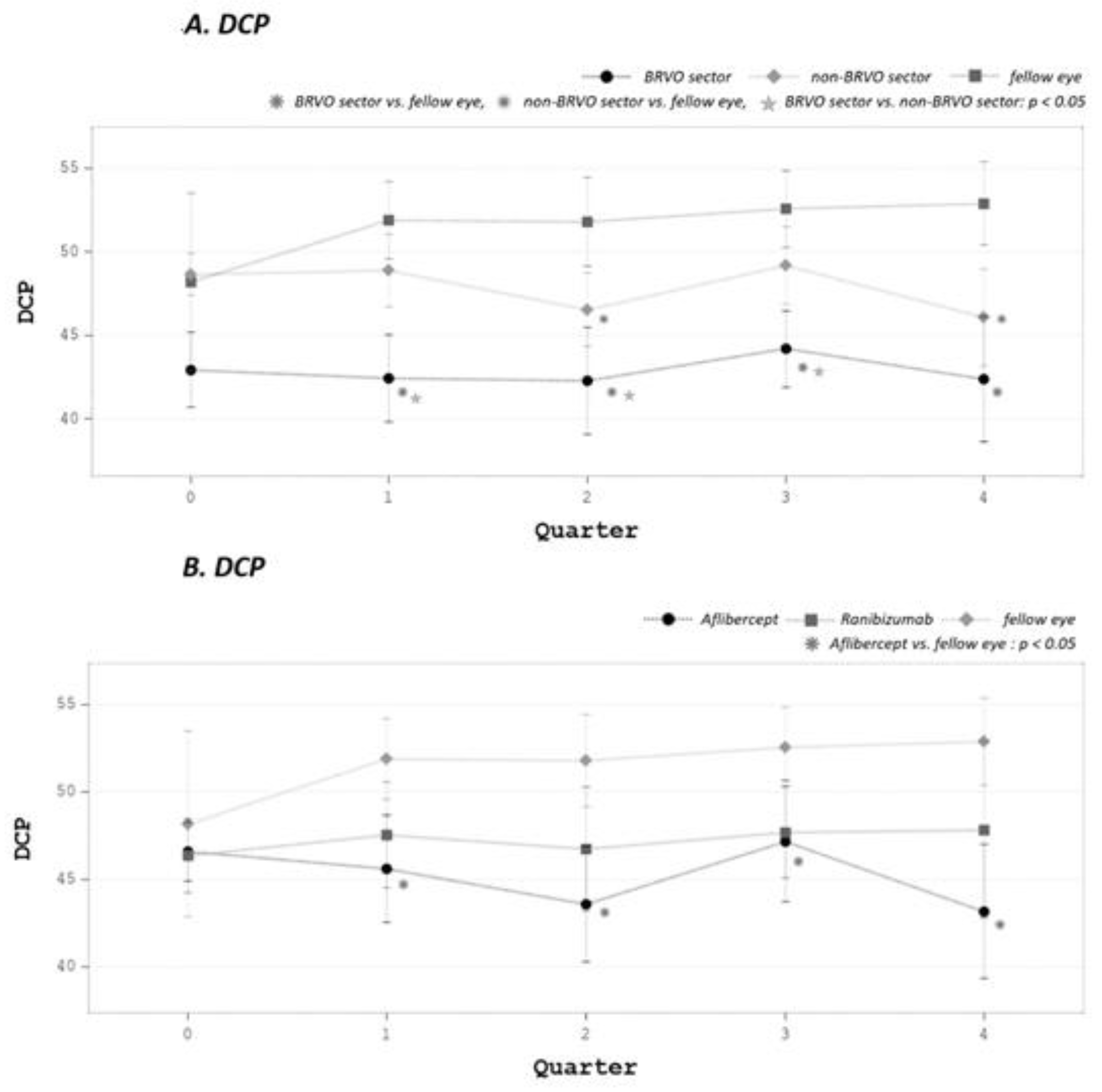
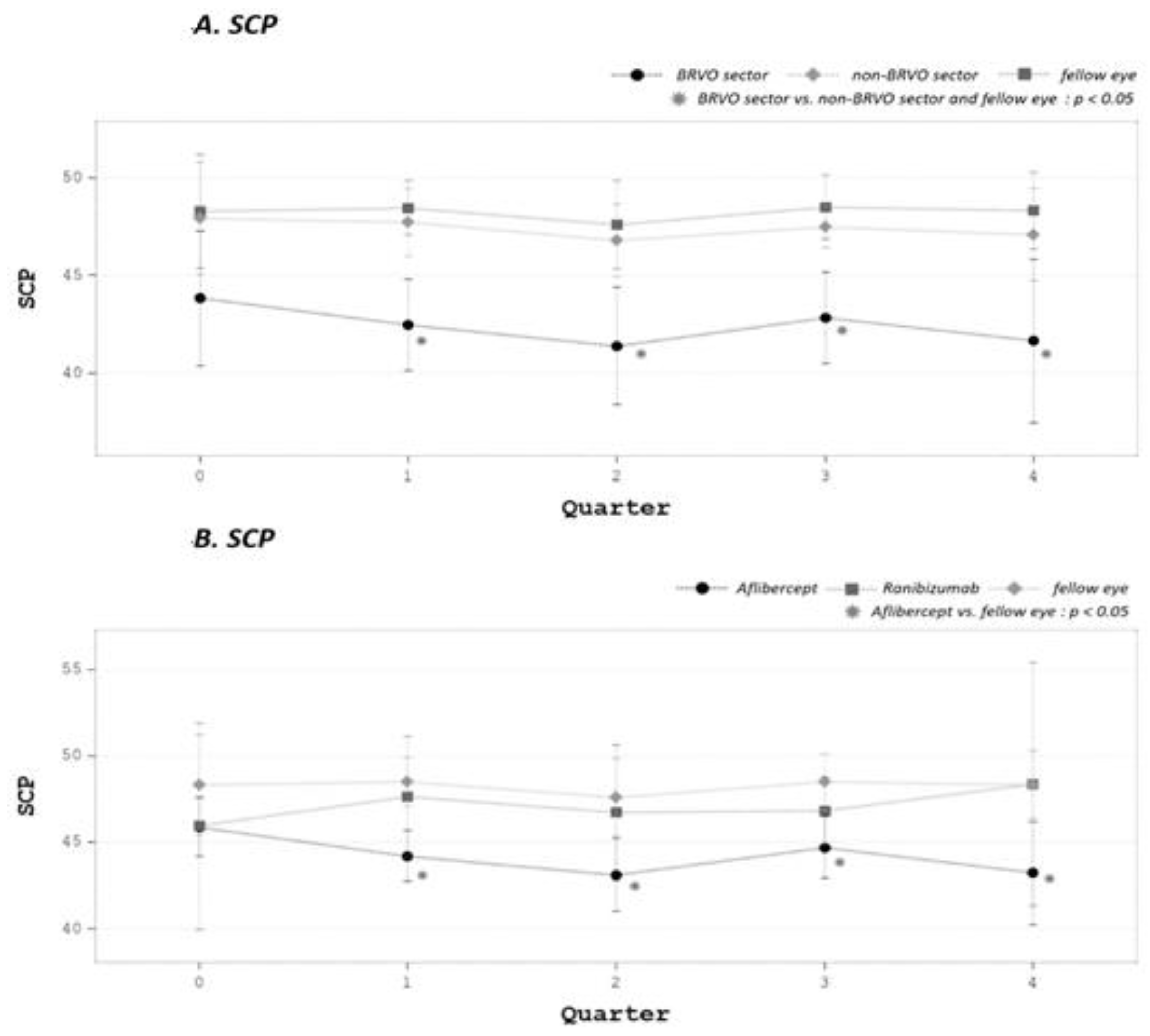
3.3. SCP and DCP Changes
3.4. FAZ, NPA, ORFA Changes

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diseased Eye | Fellow Eye | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (DB) | Final Visit (DF) | p (DB vs. DF) | Baseline (FB) | Final Visit (FF) | p (FB vs. FF) | p (DB vs. FB) | p (DF vs. FF) | |
| NPA | 19.16 ± 4.74 | 23.97 ± 2.60 | 0.0282 * | 21.66 ± 3.21 | 23.13 ± 3.48 | 0.1109 | 0.1894 | 0.5676 |
| FAZ | 0.25 ± 0.10 | 0.32 ± 0.09 | 0.1146 | 0.39 ± 0.30 | 0.32 ± 0.12 | 0.5410 | 0.2418 | 0.8256 |
| SCP_WHOLE | 45.90 ± 3.34 | 45.33 ± 5.20 | 0.5593 | 48.30 ± 3.78 | 48.15 ± 5.06 | 0.9653 | 0.1850 | 0.3805 |
| SCP_BRVO | 43.83 ± 4.15 | 41.68 ± 7.73 | 0.3291 | 48.84 ± 3.54 | 47.46 ± 4.42 | 0.5866 | 0.0353 * | 0.1244 |
| SCP_UNAFFECTED | 47.92 ± 3.44 | 47.32 ± 4.07 | 0.6601 | 48.76 ± 2.95 | 48.51 ± 5.71 | 0.8905 | 0.5782 | 0.6862 |
| DCP_WHOLE | 46.49 ± 1.47 | 46.60 ± 5.03 | 0.9870 | 48.17 ± 6.93 | 52.77 ± 4.98 | 0.1412 | 0.4699 | 0.0054 * |
| DCP_BRVO | 42.92 ± 2.67 | 43.06 ± 5.88 | 0.9302 | 49.63 ± 8.17 | 51.51 ± 6.67 | 0.5449 | 0.0356 * | 0.0024 * |
| DCP_UNAFFECTED | 48.65 ± 1.50 | 48.36 ± 5.61 | 0.8859 | 48.23 ± 6.85 | 53.20 ± 4.14 | 0.1064 | 0.8932 | 0.0312 * |
3.5. CCT Changes
3.6. Parameters Correlated to BCVA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jaulim, A.; Ahmed, B.; Khanam, T.; Chatziralli, I.P. Branch retinal vein occlusion: Epidemiology, pathogenesis, risk factors, clinical features, diagnosis, and complications. An update of the literature. Retina 2013, 33, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolar, P. Risk factors for central and branch retinal vein occlusion: A meta-analysis of published clinical data. J. Ophthalmol. 2014, 2014, 724780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivaprasad, S.; Amoaku, W.M.; Hykin, P.; RVO Guideline Group. The Royal College of Ophthalmologists Guidelines on retinal vein occlusions: Executive summary. Eye 2015, 29, 1633–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, M.G.; Heier, J.S. Venous obstructive disease of the retina. In Ophthalmology, 3rd ed.; Yanoff, M., Duker, J.S., Eds.; Elsevier Mosby: Maryland Heights, MO, USA, 2009; pp. 597–605. [Google Scholar]
- Cheung, N.; Klein, R.; Wang, J.J.; Cotch, M.F.; Islam, A.F.M.; Klein, B.E.K.; Cushman, M.; Wong, T.Y. Traditional and novel cardiovascular risk factors for retinal vein occlusion: The multiethnic study of atherosclerosis. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4297–4302. [Google Scholar] [CrossRef]
- Spooner, K.; Hong, T.; Fraser-Bell, S.; Chang, A.A. Current Outcomes of Anti-VEGF Therapy in the Treatment of Macular Oedema Secondary to Branch Retinal Vein Occlusions: A Meta-Analysis. Ophthalmologica 2019, 242, 163–177. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Sophie, R.; Pearlman, J.; Brown, D.M.; Boyer, D.S.; Heier, J.S.; Marcus, D.M.; Feiner, L.; Patel, A.; RETAIN Study Group. Log-term outcomes in patients with retinal vein occlusion treated with ranibizumab: The RETAIN study. Ophthalmology 2014, 121, 209–219. [Google Scholar] [CrossRef]
- Sangroongruangsri, S.; Ratanapakorn, T.; Wu, O.; Anothaisintawee, T.; Chaikledkaew, U. Comparative efficacy of bevacizumab, ranibizumab, and aflibercept for treatment of macular edema secondary to retinal vein occlusion: A systematic review and network meta-analysis. Expert Rev. Clin. Pharmacol. 2018, 11, 903–916. [Google Scholar] [CrossRef] [Green Version]
- Garweg, J.G.; Zandi, S. Retinal vein occlusion and the use of a dexamethasone intravitreal implant (Ozurdex®) in its treatment. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 1257–1265. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.; Kiss, S. Ultra-wide-field fluorescein angiography in retinal disease. Curr. Opin. Ophthalmol. 2014, 25, 213–220. [Google Scholar] [CrossRef]
- Werner, J.U.; Böhm, F.; Lang, G.E.; Dreyhaupt, J.; Lang, G.K.; Enders, C. Comparison of foveal avascular zone between optical coherence tomography angiography and fluorescein angiography in patients with retinal vein occlusion. PLoS ONE 2019, 14, e0217849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellam, A.; Glacet-Bernard, A.; Coscas, F.; Miere, A.; Coscas, G.; Souied, E.H. Qualitative and quantitative follow-up using optical coherence tomography angiography of retinal vein occlusion treated with anti-VEGF: Optical coherence tomography angiography follow-up of retinal vein occlusion. Retina 2017, 37, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi Falavarjani, K.; Iafe, N.A.; Hubschman, J.P.; Tsui, I.; Sadda, S.R.; Sarraf, D. Optical Coherence Tomography Angiography Analysis of the Foveal Avascular Zone and Macular Vessel Density After Anti-VEGF Therapy in Eyes with Diabetic Macular Edema and Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2017, 58, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Kadomoto, S.; Muraoka, Y.; Ooto, S.; Miwa, Y.; Iida, Y.; Suzuma, K.; Murakami, T.; Ghashut, R.; Tsujikawa, A.; Yoshimura, N. Evaluation of macular ischemia in eyes with branch retinal vein occlusion: An optical coherence tomography angiography study. Retina 2018, 38, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Wylęgała, A.; Teper, S.; Dobrowolski, D.; Wylęgała, E. Optical coherence angiography: A review. Medicine 2016, 95, e4907. [Google Scholar] [CrossRef] [PubMed]
- Turgut, B. Optical coherence tomography angiography: A general view. Eur. Ophthalmol. Rev. 2016, 10, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-I.; Li, T.-C.; Liu, C.-S.; Lin, W.-Y.; Chen, C.-C.; Yang, S.-Y.; Lin, C.-C. Extreme values of hemoglobin A1C are associated with increased risks of chronic obstructive pulmonary disease in patients with type 2 diabetes: A competing risk analysis in national cohort of Taiwan diabetes study. Medicine 2015, 94, e367. [Google Scholar] [CrossRef]
- Cheong, K.X.; Lim, L.W.; Li, K.Z.; Tan, C.S. A novel and faster method of manual grading to measure choroidal thickness using optical coherence tomography. Eye 2018, 32, 433–438. [Google Scholar] [CrossRef]
- Kashani, A.H.; Chen, C.L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef]
- Mo, B.; Zhou, H.Y.; Jiao, X.; Zhang, F. Evaluation of hyperreflective foci as a prognostic factor of visual outcome in retinal vein occlusion. Int. J. Ophthalmol. 2017, 10, 605–612. [Google Scholar] [PubMed]
- Shiono, A.; Kogo, J.; Sasaki, H.; Yomoda, R.; Jujo, T.; Tokuda, N.; Kitaoka, Y.; Takagi, H. Optical coherence tomography findings as a predictor of clinical course in patients with branch retinal vein occlusion treated with ranibizumab. PLoS ONE 2018, 13, e0199552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujihara-Mino, A.; Mitamura, Y.; Inomoto, N.; Sano, H.; Akaiwa, K.; Semba, K. Optical coherence tomography parameters predictive of visual outcome after anti-VEGF therapy for retinal vein occlusion. Clin. Ophthalmol. 2016, 10, 1305–1313. [Google Scholar] [PubMed] [Green Version]
- Suzuki, M.; Nagai, N.; Minami, S.; Kurihara, T.; Kamoshita, M.; Sonobe, H.; Watanabe, K.; Shinoda, H.; Tsubota, K.; Ozawa, Y. Predicting recurrences of macular edema due to branch retinal vein occlusion during anti-vascular endothelial growth factor therapy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanhart, J.; Tiosano, L.; Averbukh, E.; Banin, E.; Hemo, I.; Chowers, I. Fellow eye effect of unilateral intravitreal bevacizumab injection in eyes with diabetic macular edema. Eye 2014, 28, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Nasir, M.A.; Rabena, M.D.; Maia, M.; et al. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab, and ranibizumab. Retina 2017, 37, 1847–1858. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Zhan, Z.; Xiao, J.; Lan, Y. Radiation-Induced Optical Coherence Tomography Angiography Retinal Alterations in Patients with Nasopharyngeal Carcinoma. Front. Med. 2021, 7, 630880. [Google Scholar] [CrossRef]
- Bonnin, S.; Mané, V.; Couturier, A.; Julien, M.; Paques, M.; Tadayoni, R.; Gaudric, A. New insight into the macular deep vascular plexus imaged by optical coherence tomography angiography. Retina 2015, 35, 2347–2352. [Google Scholar] [CrossRef]
- Chex, X.; Rahimy, E.; Sergott, R.C.; Nunes, R.P.; Souza, E.C.; Choudhry, N.; Cutler, N.E.; Houston, S.K.S.; Munk, M.R.; Fawzi, A.A. Spectrum of retinal vascular diseases associated with paracentral acute middle maculopathy. Am. J. Ophthalmol. 2015, 160, 26–34. [Google Scholar]
- Campochiaro, P.A.; Bhisitkul, R.B.; Shapiro, H.; Rubio, R.G. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology 2013, 120, 795–802. [Google Scholar] [CrossRef]
- Suzuki, N.; Hirano, Y.; Tomiyasu, T.; Esaki, Y.; Uemura, A.; Yasukawa, T.; Yoshida, M.; Ogura, Y. Retinal Hemodynamics Seen on Optical Coherence Tomography Angiography Before and After Treatment of Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5681–5687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansour, A.M.; Bynoe, L.A.; Welch, J.C.; Pesavento, R.; Mahendradas, P.; Ziemssen, F.; Pai, S.A. Retinal vascular events after intravitreal bevacizumab. Acta Ophthalmol. 2010, 88, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Shimura, M.; Yasuda, K. Macular ischemia after intravitreal bevacizumab injection in patients with central retinal vein occlusion and a history of diabetes and vascular disease. Br. J. Ophthalmol. 2010, 94, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.E.; Yun, C.; Cha, J.; Kim, S.W. OCT angiography features associated with macular edema recurrence after intravitreal bevacizumab treatment in branch retinal vein occlusion. Sci. Rep. 2019, 9, 14153. [Google Scholar] [CrossRef] [PubMed]
- Balaratnasingam, C.; Inoue, M.; Ahn, S.; McCann, J.; Dhrami-Gavazi, E.; Yannuzzi, L.A.; Freund, K.B. Visual acuity is correlated with the area of the foveal avascular zone in diabetic retinopathy and retinal vein occlusion. Ophthalmology 2016, 123, 2352–2367. [Google Scholar] [CrossRef]




| All (n = 10) | Aflibercept (n = 5) | Ranibizumab (n = 5) | p | |
|---|---|---|---|---|
| Age | 61.40 ± 7.83 | 61.80 ± 10.26 | 61.00 ± 5.70 | 0.883 |
| Gender (F) | 5 (50%) | 2 (40%) | 3 (60%) | 0.527 |
| Eye (OD) | 5 (50%) | 3 (60%) | 2 (40%) | 0.527 |
| SBP | 151.60 ± 19.49 | 147.80 ± 20.90 | 155.40 ± 19.55 | 0.569 |
| IOP | 15.70 ± 2.91 | 14.20 ± 2.49 | 17.20 ± 2.68 | 0.104 |
| CRT | 396.60 ±135.64 | 367.60 ± 68.61 | 425.60 ±185.97 | 0.531 |
| CCT | 208.67 ± 94.02 | 214.20 ±129.33 | 201.75 ± 33.98 | 0.129 |
| S | 0.57 ± 1.48 | 0.67 ± 1.61 | 0.50 ± 1.62 | 0.932 |
| C | −0.61 ± 0.61 | −0.75 ± 0.90 | −0.50 ± 0.41 | 0.418 |
| BCVA | 0.52 ± 0.30 | 0.67 ± 0.32 | 0.38 ± 0.22 | 0.832 |
| NPA | 19.16 ± 4.74 | 19.02 ± 5.71 | 19.30 ± 4.23 | 0.858 |
| FAZ | 0.25 ± 0.10 | 0.23 ± 0.08 | 0.28 ± 0.12 | 0.898 |
| SCP | 45.90 ± 3.34 | 45.88 ± 1.36 | 45.93 ± 4.82 | 0.637 |
| DCP | 46.49 ± 1.47 | 46.60 ± 1.38 | 46.38 ± 1.71 | 0.833 |
| Total injections | 5.80 ±2.53 (3.00~9.00) | 7.00 ±2.12 (4.00~9.00) | 4.60 ±2.51 (3.00~7.00) | 0.141 |
| Follow-up months | 11.39 ± 2.14 (7.97~15.43) | 11.72 ± 1.41 (9.53~13.30) | 11.06 ± 2.84 (7.97~15.43) | 0.654 |
| With LogMAR | |||
|---|---|---|---|
| Side | Variable | PCC | p |
| Diseased Eye | NPA | −0.24546 | 0.0165 * |
| FAZ | −0.04474 | 0.6668 | |
| SCP (whole) | −0.40927 | <0.0001 * | |
| SCP (BRVO) | −0.38861 | 0.0001 * | |
| SCP (unaffected) | −0.44414 | <0.0001 * | |
| DCP (whole) | −0.49930 | <0.0001 * | |
| DCP (BRVO) | −0.45791 | <0.0001 * | |
| DCP (unaffected) | −0.42122 | <0.0001 * | |
| Fellow Eye | NPA | −0.51187 | <0.0001 * |
| FAZ | 0.19560 | 0.0588 | |
| SCP (whole) | −0.06948 | 0.5058 | |
| SCP (BRVO) | −0.17612 | 0.0949 | |
| SCP (unaffected) | −0.12261 | 0.2469 | |
| DCP (whole) | −0.55549 | <0.0001 * | |
| DCP (BRVO) | −0.58967 | <0.0001 * | |
| DCP (unaffected) | −0.45140 | <0.0001 * | |
| GLM Model Selection Summary | ||||||
|---|---|---|---|---|---|---|
| Effect | DF | Estimate | Adjusted R-Square | AIC | F Value | Pr > F |
| Intercept | 1 | 1.37352 | 0 | −151.4508 | 0 | 1 |
| DCP of Affected Sector | 1 | −0.015374 | 0.152 | −165.4669 | 17.13 | <0.0001 |
| DCP of Affected Sector, fellow eye | 1 | −0.009168 | 0.4375 | −201.8591 | 46.19 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-T.; Wang, I.; Lin, C.-J.; Lai, C.-T.; Hsia, N.-Y.; Chen, H.-S.; Tien, P.-T.; Bair, H.; Lin, J.-M.; Chen, W.-L.; et al. Comparison of Choroidal Thickness, Foveal Avascular Zone, and Macular Capillary Density in Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Ranibizumab or Aflibercept—A Prospective Study. Medicina 2022, 58, 540. https://doi.org/10.3390/medicina58040540
Huang Y-T, Wang I, Lin C-J, Lai C-T, Hsia N-Y, Chen H-S, Tien P-T, Bair H, Lin J-M, Chen W-L, et al. Comparison of Choroidal Thickness, Foveal Avascular Zone, and Macular Capillary Density in Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Ranibizumab or Aflibercept—A Prospective Study. Medicina. 2022; 58(4):540. https://doi.org/10.3390/medicina58040540
Chicago/Turabian StyleHuang, Yu-Te, I Wang, Chun-Ju Lin, Chun-Ting Lai, Ning-Yi Hsia, Huan-Sheng Chen, Peng-Tai Tien, Henry Bair, Jane-Ming Lin, Wen-Lu Chen, and et al. 2022. "Comparison of Choroidal Thickness, Foveal Avascular Zone, and Macular Capillary Density in Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Ranibizumab or Aflibercept—A Prospective Study" Medicina 58, no. 4: 540. https://doi.org/10.3390/medicina58040540
APA StyleHuang, Y. -T., Wang, I., Lin, C. -J., Lai, C. -T., Hsia, N. -Y., Chen, H. -S., Tien, P. -T., Bair, H., Lin, J. -M., Chen, W. -L., Chen, C. -H., Wu, W. -C., & Tsai, Y. -Y. (2022). Comparison of Choroidal Thickness, Foveal Avascular Zone, and Macular Capillary Density in Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Ranibizumab or Aflibercept—A Prospective Study. Medicina, 58(4), 540. https://doi.org/10.3390/medicina58040540