
A Global Survey on Diagnostic, Therapeutic and Preventive Strategies in Intensive Care Unit—Acquired Weakness

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
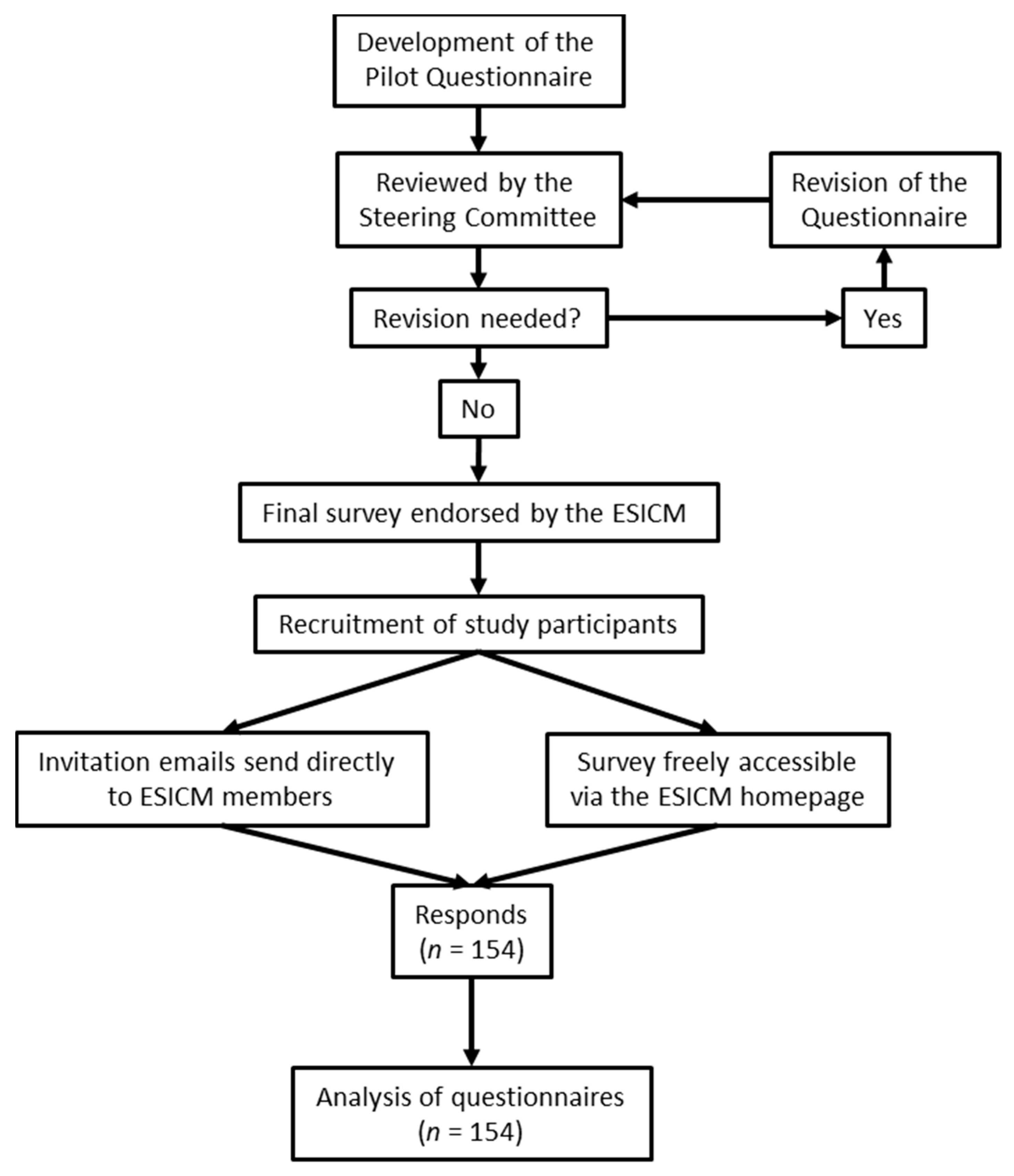
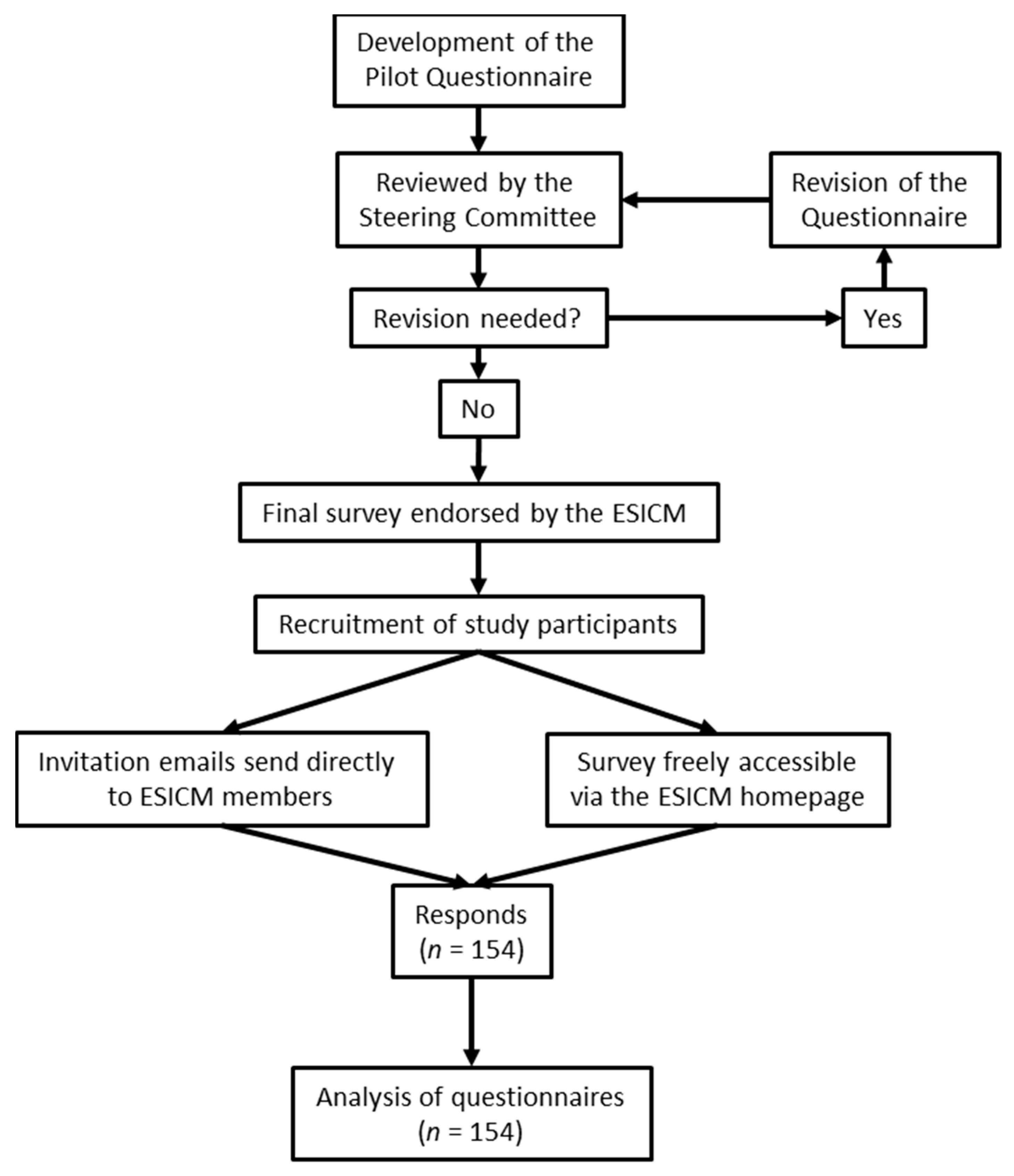
2.1. Questionnaire and Study Participation
2.2. Statistical Analysis
3. Results
3.1. Part One: Basic Demographic Data
3.2. Part Two: Diagnostic and Monitoring Strategies
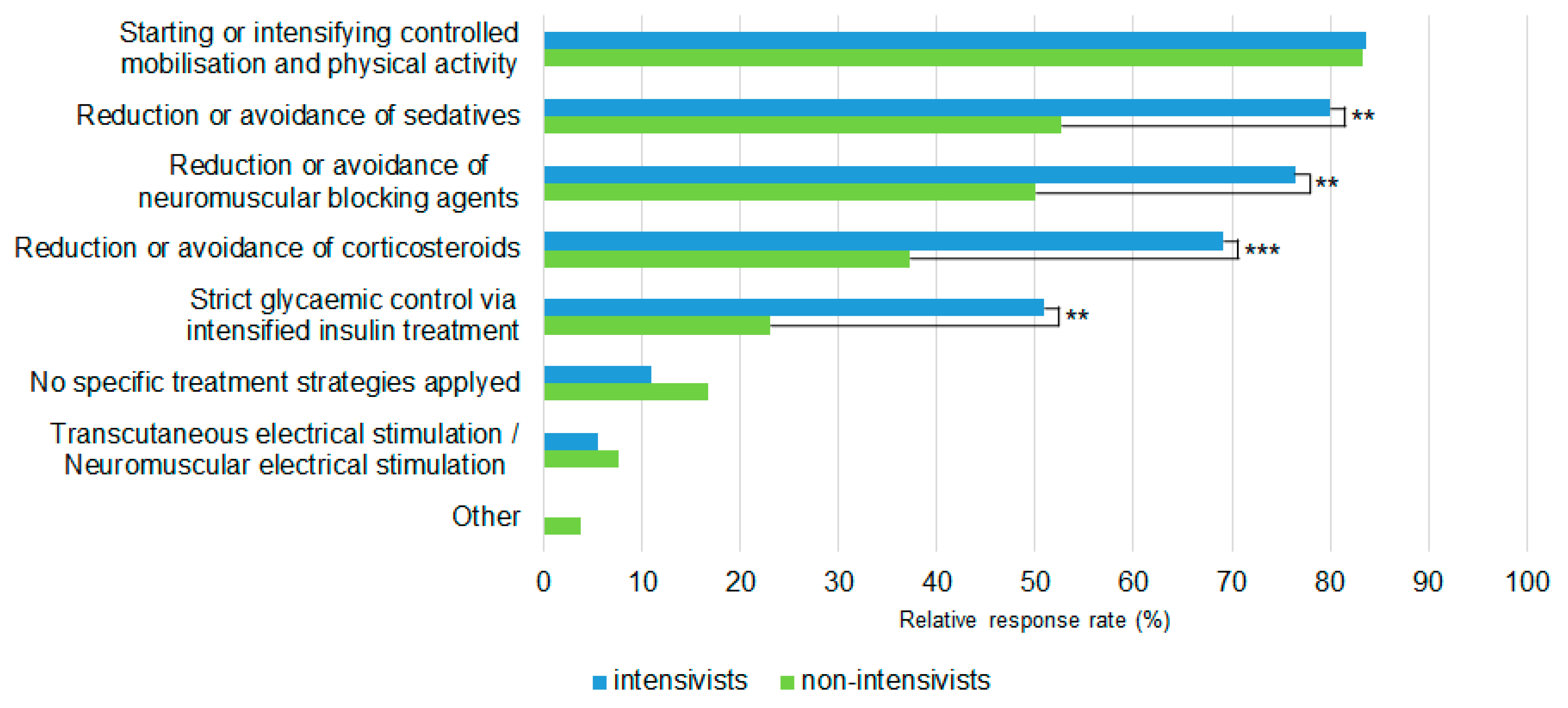
3.3. Part Three: Treatment and Prevention Strategies
4. Discussion
4.1. Diagnostic and Monitoring Strategies
4.2. Treatment and Prevention Strategies
4.3. Barriers and Deficits
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ali, N.A.; O’Brien, J.M.; Hoffmann, S.P.; Phillips, G.; Garland, A.; Finley, J.C.W.; Almoosa, K.; Hejal, R.; Wolf, K.M.; Lemeshow, S.; et al. Acquired Weakness, Handgrip Strength, and Mortality in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2008, 178, 261–268. [Google Scholar] [CrossRef]
- Sharshar, T.; Bastuji-Garin, S.; Stevens, R.D.; Durand, M.-C.; Malissin, I.; Rodriguez, P.; Cerf, C.; Outin, H.; De Jonghe, B. Presence and severity of intensive care unit-acquired paresis at time of awakening are associated with increased intensive care unit and hospital mortality. Crit. Care Med. 2009, 37, 3047–3053. [Google Scholar] [CrossRef]
- Sidiras, G.; Patsaki, I.; Karatzanos, E.; Dakoutrou, M.; Kouvarakos, A.; Mitsiou, G.; Routsi, C.; Stranjalis, G.; Nanas, S.; Gerovasili, V. Long term follow-up of quality of life and functional ability in patients with ICU acquired Weakness—A post hoc analysis. J. Crit. Care 2019, 53, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, O.; Reid, M.B.; Berghe, G.V.D.; Vanhorebeek, I.; Hermans, G.; Rich, M.M.; Larsson, L. The Sick and the Weak: Neuropathies/Myopathies in the Critically Ill. Physiol. Rev. 2015, 95, 1025–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, R.D.; Marshall, S.A.; Cornblath, D.R.; Hoke, A.; Needham, D.M.; De Jonghe, B.; Ali, N.; Sharshar, T. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit. Care Med. 2009, 37, S299–S308. [Google Scholar] [CrossRef] [PubMed]
- Van Aerde, N.; Meersseman, P.; Debaveye, Y.; Wilmer, A.; Gunst, J.; Casaer, M.P.; Bruyninckx, F.; Wouters, P.J.; Gosselink, R.; Berghe, G.V.D.; et al. Five-year impact of ICU-acquired neuromuscular complications: A prospective, observational study. Intensiv. Care Med. 2020, 46, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Van Aerde, N.; Meersseman, P.; Debaveye, Y.; Wilmer, A.; Casaer, M.P.; Gunst, J.; Wauters, J.; Wouters, P.J.; Goetschalckx, K.; Gosselink, R.; et al. Aerobic exercise capacity in long-term survivors of critical illness: Secondary analysis of the post-EPaNIC follow-up study. Intensiv. Care Med. 2021, 47, 1462–1471. [Google Scholar] [CrossRef]
- Nakanishi, N.; Tsutsumi, R.; Hara, K.; Takashima, T.; Nakataki, E.; Itagaki, T.; Matsuo, M.; Oto, J.; Sakaue, H. Urinary Titin Is a Novel Biomarker for Muscle Atrophy in Nonsurgical Critically Ill Patients: A Two-Center, Prospective Observational Study. Crit. Care Med. 2020, 48, 1327–1333. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Latronico, N.; Berghe, G.V.D. ICU-acquired weakness. Intensiv. Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef]
- Connolly, B.; Salisbury, L.; O’Neill, B.; Geneen, L.; Douiri, A.; Grocott, M.; Hart, N.; Walsh, T.S.; Blackwood, B. Exercise rehabilitation following intensive care unit discharge for recovery from critical illness: Executive summary of a Cochrane Collaboration systematic review. J. Cachex Sarcopenia Muscle 2016, 7, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, C.; Tipping, C.J. Physiotherapy management of intensive care unit-acquired weakness. J. Physiother. 2017, 63, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Luo, J.; Zhou, J.; Zhu, X. Intervention effect of neuromuscular electrical stimulation on ICU acquired weakness: A meta-analysis. Int. J. Nurs. Sci. 2020, 7, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Zhang, Z.; Zhang, C.; Yao, L.; Yang, L.; Jiang, B.; Wu, Y.; Jiang, L.; Tian, J. What is the optimum time for initiation of early mobilization in mechanically ventilated patients? A network meta-analysis. PLoS ONE 2019, 14, e0223151. [Google Scholar] [CrossRef] [PubMed]
- Schaller, S.J.; Anstey, M.; Blobner, M.; Edrich, T.; Grabitz, S.D.; Gradwohl-Matis, I.; Heim, M.; Houle, T.; Kurth, T.; Latronico, N.; et al. Early, goal-directed mobilisation in the surgical intensive care unit: A randomised controlled trial. Lancet 2016, 388, 1377–1388. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, Z.; Jiang, B.; Wang, G.; Wei, H.; Li, B.; Shen, X.; Zhang, C. Current practice and barriers to ICU-acquired weakness assessment: A cross-sectional survey. Physiotherapy 2021, 112, 135–142. [Google Scholar] [CrossRef]
- Sharma, A.; Duc, N.T.M.; Thang, T.L.L.; Nam, N.H.; Ng, S.J.; Abbas, K.S.; Huy, N.T.; Marušić, A.; Paul, C.L.; Kwok, J.; et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J. Gen. Intern. Med. 2021, 36, 3179–3187. [Google Scholar] [CrossRef]
- Schaller, S.J.; Scheffenbichler, F.T.; Bose, S.; Mazwi, N.; Deng, H.; Krebs, F.; Seifert, C.L.; Kasotakis, G.; Grabitz, S.D.; Latronico, N.; et al. Influence of the initial level of consciousness on early, goal-directed mobilization: A post hoc analysis. Intensiv. Care Med. 2019, 45, 201–210. [Google Scholar] [CrossRef]
- Hough, C.L.; Lieu, B.K.; Caldwell, E.S. Manual muscle strength testing of critically ill patients: Feasibility and interobserver agreement. Crit. Care 2011, 15, R43. [Google Scholar] [CrossRef] [Green Version]
- Kennouche, D.; Luneau, E.; Lapole, T.; Morel, J.; Millet, G.Y.; Gondin, J. Bedside voluntary and evoked forces evaluation in intensive care unit patients: A narrative review. Crit. Care 2021, 25, 157. [Google Scholar] [CrossRef]
- Zhang, W.; Wu, J.; Gu, Q.; Gu, Y.; Zhao, Y.; Ge, X.; Sun, X.; Lian, J.; Zeng, Q. Changes in muscle ultrasound for the diagnosis of intensive care unit acquired weakness in critically ill patients. Sci. Rep. 2021, 11, 18280. [Google Scholar] [CrossRef]
- Fisse, A.L.; May, C.; Motte, J.; Pedreiturria, X.; Breuer, T.G.K.; Schneider-Gold, C.; Marcus, K.; Gold, R.; Yoon, M.-S.; Pitarokoili, K. New Approaches to Critical Illness Polyneuromyopathy: High-Resolution Neuromuscular Ultrasound Characteristics and Cytokine Profiling. Neurocritical Care 2020, 35, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Latronico, N.; Bertolini, G.; Guarneri, B.; Botteri, M.; Peli, E.; Andreoletti, S.; Bera, P.; Luciani, D.; Nardella, A.; Vittorielli, E.; et al. Simplified electrophysiological evaluation of peripheral nerves in critically ill patients: The Italian multi-centre CRIMYNE study. Crit. Care 2007, 11, R11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patejdl, R.; Walter, U.; Rosener, S.; Sauer, M.; Reuter, D.A.; Ehler, J. Muscular Ultrasound, Syndecan-1 and Procalcitonin Serum Levels to Assess Intensive Care Unit-Acquired Weakness. Can. J. Neurol. Sci./J. Can. Sci. Neurol. 2019, 46, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Guarneri, B.; Bertolini, G.; Latronico, N. Long-term outcome in patients with critical illness myopathy or neuropathy: The Italian multicentre CRIMYNE study. J. Neurol. Neurosurg. Psychiatry 2008, 79, 838–841. [Google Scholar] [CrossRef]
- Jolley, S.E.; Bunnell, A.E.; Hough, C.L. ICU-Acquired Weakness. Chest 2016, 150, 1129–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; Le Peillet, D.; Fassier, T.; Prendki, V.; Trombert, V.; Reny, J.-L.; Roux, X. Functional Independence Measure score is associated with mortality in critically ill elderly patients admitted to an intermediate care unit. BMC Geriatr. 2020, 20, 334. [Google Scholar] [CrossRef]
- Menges, D.; Seiler, B.; Tomonaga, Y.; Schwenkglenks, M.; Puhan, M.A.; Yebyo, H.G. Systematic early versus late mobilization or standard early mobilization in mechanically ventilated adult ICU patients: Systematic review and meta-analysis. Crit. Care 2021, 25, 16. [Google Scholar] [CrossRef]
- Anekwe, D.E.; Milner, S.C.; Bussières, A.; de Marchie, M.; Spahija, J. Intensive care unit clinicians identify many barriers to, and facilitators of, early mobilisation: A qualitative study using the Theoretical Domains Framework. J. Physiother. 2020, 66, 120–127. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, W.; Cai, Z.; Liu, J.; Wu, J.; Deng, Y.; Yu, K.; Chen, X.; Zhu, L.; Ma, J.; et al. Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0223185. [Google Scholar] [CrossRef] [Green Version]
- Paton, M.; Lane, R.; Paul, E.; Cuthburtson, G.A.; Hodgson, C.L. Mobilization During Critical Illness: A Higher Level of Mobilization Improves Health Status at 6 Months, a Secondary Analysis of a Prospective Cohort Study. Crit. Care Med. 2021, 49, e860–e869. [Google Scholar] [CrossRef]
- Scheffenbichler, F.T.; Teja, B.; Wongtangman, K.; Mazwi, N.; Waak, K.; Schaller, S.J.; Xu, X.; Barbieri, S.; Fagoni, N.; Cassavaugh, J.; et al. Effects of the Level and Duration of Mobilization Therapy in the Surgical ICU on the Loss of the Ability to Live Independently: An International Prospective Cohort Study. Crit. Care Med. 2021, 49, e247–e257. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Combs, M.P.; Colantuoni, E.; King, L.M.; Niessen, T.; Neufeld, K.; Collop, N.A.; Needham, D.M. The association of sleep quality, delirium, and sedation status with daily participation in physical therapy in the ICU. Crit. Care 2016, 20, 261. [Google Scholar] [CrossRef] [Green Version]
- Shehabi, Y.; Chan, L.; Kadiman, S.; Alias, A.; Ismail, W.N.; Tan, M.A.T.I.; Khoo, T.M.; Ali, S.B.; Saman, M.A.; Shaltut, A.; et al. The Sedation Practice in Intensive Care Evaluation (SPICE) Study Group investigators. Sedation depth and long-term mortality in mechanically ventilated critically ill adults: A prospective longitudinal multicentre cohort study. Intensiv. Care Med. 2013, 39, 910–918. [Google Scholar] [CrossRef] [Green Version]
- Strøm, T.; Martinussen, T.; Toft, P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: A randomised trial. Lancet 2010, 375, 475–480. [Google Scholar] [CrossRef]
- Piva, S.; Fagoni, N.; Latronico, N. Intensive care unit–acquired weakness: Unanswered questions and targets for future research. F1000Research 2019, 8, 508. [Google Scholar] [CrossRef]
- Baron, R.; Binder, A.; Biniek, R.; Braune, S.; Buerkle, H.; Dall, P.; Demirakca, S.; Eckardt, R.; Eggers, V.; Eichler, I.; et al. Evidence and consensus based guideline for the management of delirium, analgesia, and sedation in intensive care medicine. Revision 2015 (DAS-Guideline 2015)—short version. Ger. Med. Sci. 2015, 13. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Xu, C.; Ma, X.; Zhang, X.; Xie, P. Intensive Care Unit-Acquired Weakness: A Review of Recent Progress With a Look Toward the Future. Front. Med. 2020, 7, 671. [Google Scholar] [CrossRef]
- Yang, T.; Li, Z.; Jiang, L.; Wang, Y.; Xi, X. Risk factors for intensive care unit-acquired weakness: A systematic review and meta-analysis. Acta Neurol. Scand. 2018, 138, 104–114. [Google Scholar] [CrossRef]
- Hermans, G.; Wilmer, A.; Meersseman, W.; Milants, I.; Wouters, P.J.; Bobbaers, H.; Bruyninckx, F.; Berghe, G.V.D. Impact of Intensive Insulin Therapy on Neuromuscular Complications and Ventilator Dependency in the Medical Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2007, 175, 480–489. [Google Scholar] [CrossRef] [Green Version]
- Van Den Berghe, G.; Schoonheydt, K.; Becx, P.; Bruyninckx, F.; Wouters, P.J. Insulin therapy protects the central and peripheral nervous system of intensive care patients. Neurology 2005, 64, 1348–1353. [Google Scholar] [CrossRef]
- Hermans, G.; De Jonghe, B.; Bruyninckx, F.; Berghe, G.V.D. Interventions for preventing critical illness polyneuropathy and critical illness myopathy. Cochrane Database Syst. Rev. 2014, 2014, CD006832. [Google Scholar] [CrossRef]
- Price, D.R.; Mikkelsen, M.E.; Umscheid, C.A.; Armstrong, E.J. Neuromuscular Blocking Agents and Neuromuscular Dysfunction Acquired in Critical Illness. Crit. Care Med. 2016, 44, 2070–2078. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Li, Z.; Jiang, L.; Xi, X. Corticosteroid use and intensive care unit-acquired weakness: A systematic review and meta-analysis. Crit. Care 2018, 22, 187. [Google Scholar] [CrossRef] [Green Version]
- Renew, J.R.; Ratzlaff, R.; Hernandez-Torres, V.; Brull, S.J.; Prielipp, R.C. Neuromuscular blockade management in the critically Ill patient. J. Intensiv. Care 2020, 8, 37. [Google Scholar] [CrossRef]
- Lyu, T.; Lee, Y.S.; Dhanvijay, S.; Freebairn, R. The effect of neuromuscular blocking agents uses in acute respiratory distress syndrome: A systematic review and meta-analysis of randomized controlled trials. Minerva Anestesiol. 2021, 87, 341–350. [Google Scholar] [CrossRef]
- Hermans, G.; van den Berghe, G. Clinical review: Intensive care unit acquired weakness. Crit. Care 2015, 19, 274. [Google Scholar] [CrossRef] [Green Version]
- Penoyer, D.A. Nurse staffing and patient outcomes in critical care: A concise review. Crit. Care Med. 2010, 38, 1521–1528. [Google Scholar] [CrossRef]
- Hermans, G.; Van Mechelen, H.; Clerckx, B.; Vanhullebusch, T.; Mesotten, D.; Wilmer, A.; Casaer, M.P.; Meersseman, P.; Debaveye, Y.; Van Cromphaut, S.; et al. Acute Outcomes and 1-Year Mortality of Intensive Care Unit–acquired Weakness. A Cohort Study and Propensity-matched Analysis. Am. J. Respir. Crit. Care Med. 2014, 190, 410–420. [Google Scholar] [CrossRef]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional Disability 5 Years after Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.L.; Taylor, S.P. Family Presence for Critically Ill Patients During a Pandemic. Chest 2021, 160, 549–557. [Google Scholar] [CrossRef]
- Lee, C.M.; Fan, E. ICU-acquired weakness: What is preventing its rehabilitation in critically ill patients? BMC Med. 2012, 10, 115. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Primary medical specialty (SC) | Absolute/Total (n/153) | Relative (%) |
| (a) Intensive Care Medicine | 64 | 41.8 |
| (b) Anesthesiology | 29 | 19.0 |
| (c) Internal Medicine | 16 | 10.5 |
| (d) Surgery | 1 | 0.7 |
| (e) Neurology | 2 | 1.3 |
| (f) Nursing | 4 | 2.6 |
| (g) Physiotherapy | 30 | 19.6 |
| (h) Other | 7 | 4.6 |
| Medical training status (SC) | Absolute/Total (n/142) | Relative (%) |
| (a) Resident/in-training | 10 | 7.0 |
| (b) Fellow/training completed | 22 | 15.5 |
| (c) Consultant/medical specialist | 77 | 54.2 |
| (d) Chief/Head of Department | 33 | 23.2 |
| Years of intensive care practice (SC) | Absolute/Total (n/152) | Relative (%) |
| (a) <5 | 18 | 11.8 |
| (b) 5–10 | 38 | 25.0 |
| (c) 11–15 | 25 | 16.4 |
| (d) 16–20 | 27 | 17.8 |
| (e) >20 | 44 | 28.9 |
| Type of hospital (SC) | Absolute/Total (n/152) | Relative (%) |
| (a) University hospital | 95 | 62.5 |
| (b) Non-university hospital | 57 | 37.5 |
| Number of ICU beds (SC) | Absolute/Total (n/153) | Relative (%) |
| (a) <10 | 10 | 6.5 |
| (b) 10–20 | 49 | 32.0 |
| (c) 21–50 | 51 | 33.3 |
| (d) >50 | 43 | 28.1 |
| Type of ICU specialty (MC) | Absolute/Total (n/153) | Relative (%) |
| (a) Perioperative (surgical/anesthesiological) | 15 | 9.8 |
| (b) Internal medicine | 11 | 7.2 |
| (c) Neurologic ICU | 5 | 3.3 |
| (d) Pediatric ICU | 2 | 1.3 |
| (e) Interdisciplinary (medical and surgical) ICU | 120 | 78.4 |
| Is research on ICU-AW a topic for you? (SC) | Absolute/Total (n/152) | Relative (%) |
| YES | 103 | 67.8 |
| NO | 45 | 29.6 |
| I don’t know | 4 | 2.6 |
| Is a standard I in-house protocol used for the screening of ICU-AW? (SC) | Absolute/Total (n/140) | Relative (%) |
| (a) Yes | 28 | 20.0 |
| (b) No | 112 | 80.0 |
| (c) I don’t know | 0 | 0 |
| Routinely used screening methods (MC) | Absolute/Total (n/141) | Relative (%) |
| (a) Clinical examination | 124 | 87.9 |
| (b) Selective scores (e.g., Medical Research Council—sum score, MRC-SS) | 46 | 32.6 |
| (c) Electrophysiology (electroneurography/electromyography) | 46 | 32.6 |
| (d) Neuromuscular ultrasound | 10 | 7.1 |
| (e) Laboratory diagnostics including body fluid biomarkers | 8 | 5.7 |
| (f) Muscle/nerve biopsy | 6 | 4.3 |
| (g) No screening is performed | 18 | 12.8 |
| (h) I do not know | 4 | 2.8 |
| (i) Other | 2 | 1.4 |
| Most likely circumstances of screening for ICU-AW (MC) | Absolute/Total (n/141) | Relative (%) |
| (a) Routinely, within the daily clinical examinations | 62 | 44.0 |
| (b) Occasionally, when ICU-AW seems likely according to disease severity and clinical course | 72 | 51.1 |
| (c) Occasionally, when my patient shows no spontaneous limb movements or inadequate motoric responses over a period of time | 50 | 35.5 |
| (d) Occasionally, after the first failed weaning from the respirator | 23 | 16.3 |
| (e) Screening for ICU-AW is not performed | 6 | 4.3 |
| (f) Other | 4 | 2.8 |
| Who should primarily screen? (SC) | Absolute/Total (n/141) | Relative (%) |
| (a) Physicians | 73 | 51.8 |
| (b) Nurses | 18 | 12.8 |
| (c) Physiotherapists | 46 | 32.6 |
| (d) I don’t know | 4 | 2.8 |
| Who is screening? (MC) | Absolute/Total (n/141) | Relative (%) |
| (a) Physicians | 100 | 70.9 |
| (b) Nurses | 38 | 27.0 |
| (c) Physiotherapists | 62 | 44.0 |
| (d) I don’t know | 7 | 5.0 |
| Screening intervals used (SC) | Absolute/Total (n/141) | Relative (%) |
| (a) Once per patient stay | 13 | 9.2 |
| (b) Once daily | 80 | 56.7 |
| (c) Once per ICU shift | 9 | 6.4 |
| (d) None of the above mentioned | 29 | 20.6 |
| (e) Never | 10 | 7.1 |
| Diagnostics after detection of ICU-AW (MC) | Absolute/Total (n/140) | Relative (%) |
| (a) Electrophysiology (electroneurography/electromyography) | 63 | 45.0 |
| (b) Neuromuscular ultrasound | 9 | 6.4 |
| (c) Muscle/nerve biopsy | 5 | 3.6 |
| (d) Consultation by an expert neurologist | 50 | 35.7 |
| (e) Laboratory diagnostics including body fluid biomarkers | 11 | 7.9 |
| (f) Further diagnostic is not performed | 39 | 27.9 |
| (g) I don’t know | 9 | 6.4 |
| (h) Other | 1 | 0.7 |
| Functional disability scores (MC) | Absolute/Total (n/141) | Relative (%) |
| (a) Modified Rankin scale (mRS) | 32 | 22.7 |
| (b) Barthel Index (BI) | 23 | 16.3 |
| (c) Functional independence measure (FIM) | 6 | 4.3 |
| (d) Physical function in the ICU test (PFIT) | 6 | 4.3 |
| (e) Functional status score for ICU (FSS-ICU) | 8 | 5.7 |
| (f) Acute Care Index of Function (ACIF) | 4 | 2.8 |
| (g) Scores are not used | 70 | 49.6 |
| (h) I don’t know | 9 | 6.4 |
| (i) Other | 14 | 9.9 |
| Are treatment strategies available at your ICU? (SC) | Absolute/Total (n/134) | Relative (%) |
| (a) Yes | 84 | 62.7 |
| (b) No | 44 | 32.8 |
| (c) I don’t know | 6 | 4.5 |
| What specific treatment/prevention strategies do you use? (MC) | Absolute/Total (n/134) | Relative (%) |
| (a) Starting or intensifying controlled mobilization and physical activity | 111 | 82.8 |
| (b) Transcutaneous electrical stimulation (TENS)/neuromuscular electrical stimulation | 9 | 6.7 |
| (c) Strict glycaemic control via intensified insulin treatment | 46 | 34.3 |
| (d) Reduction or avoidance of neuromuscular blocking agents | 81 | 60.4 |
| (e) Reduction or avoidance of corticosteroids | 67 | 50.0 |
| (f) Reduction or avoidance of sedatives | 85 | 63.4 |
| (g) We apply no specific treatment strategies after diagnosing ICU-AW | 19 | 14.2 |
| (h) Other | 3 | 2.2 |
| Specify the frequency of physiotherapeutic treatment at your ICU. (SC) | Absolute/Total (n/134) | Relative (%) |
| (a) Once a day | 73 | 54.5 |
| (b) Once a working shift | 23 | 17.2 |
| (c) Multiple times per working shift | 21 | 15.7 |
| (d) No regular intervals | 14 | 10.4 |
| (e) Never/none | 3 | 2.2 |
| Which deficits in regard to medical care of ICU-AW patients exist? (MC) | Absolute/Total (n/134) | Relative (%) |
| (a) Availability of diagnostic/therapeutic approaches | 81 | 60.4 |
| (b) Not enough physiotherapists available | 92 | 68.7 |
| (c) Not enough nurses available | 42 | 31.3 |
| (d) Not enough physicians available | 12 | 9.0 |
| (e) Not enough knowledge about ICU-AW within medical staff | 83 | 61.9 |
| (f) Not enough time to care about patients with ICU-AW within the medical staff | 54 | 40.3 |
| (g) There are no deficits | 1 | 0.7 |
| (h) I don’t know | 2 | 1.5 |
| (i) Other | 6 | 4.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klawitter, F.; Oppitz, M.-C.; Goettel, N.; Berger, M.M.; Hodgson, C.; Weber-Carstens, S.; Schaller, S.J.; Ehler, J. A Global Survey on Diagnostic, Therapeutic and Preventive Strategies in Intensive Care Unit—Acquired Weakness. Medicina 2022, 58, 1068. https://doi.org/10.3390/medicina58081068
Klawitter F, Oppitz M-C, Goettel N, Berger MM, Hodgson C, Weber-Carstens S, Schaller SJ, Ehler J. A Global Survey on Diagnostic, Therapeutic and Preventive Strategies in Intensive Care Unit—Acquired Weakness. Medicina. 2022; 58(8):1068. https://doi.org/10.3390/medicina58081068
Chicago/Turabian StyleKlawitter, Felix, Marie-Christine Oppitz, Nicolai Goettel, Mette M. Berger, Carol Hodgson, Steffen Weber-Carstens, Stefan J. Schaller, and Johannes Ehler. 2022. "A Global Survey on Diagnostic, Therapeutic and Preventive Strategies in Intensive Care Unit—Acquired Weakness" Medicina 58, no. 8: 1068. https://doi.org/10.3390/medicina58081068
APA StyleKlawitter, F., Oppitz, M.-C., Goettel, N., Berger, M. M., Hodgson, C., Weber-Carstens, S., Schaller, S. J., & Ehler, J. (2022). A Global Survey on Diagnostic, Therapeutic and Preventive Strategies in Intensive Care Unit—Acquired Weakness. Medicina, 58(8), 1068. https://doi.org/10.3390/medicina58081068