
Assessment of Factors Influencing Personal Exposure to Air Pollution on Main Roads in Bogota: A Mixed-Method Study


 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
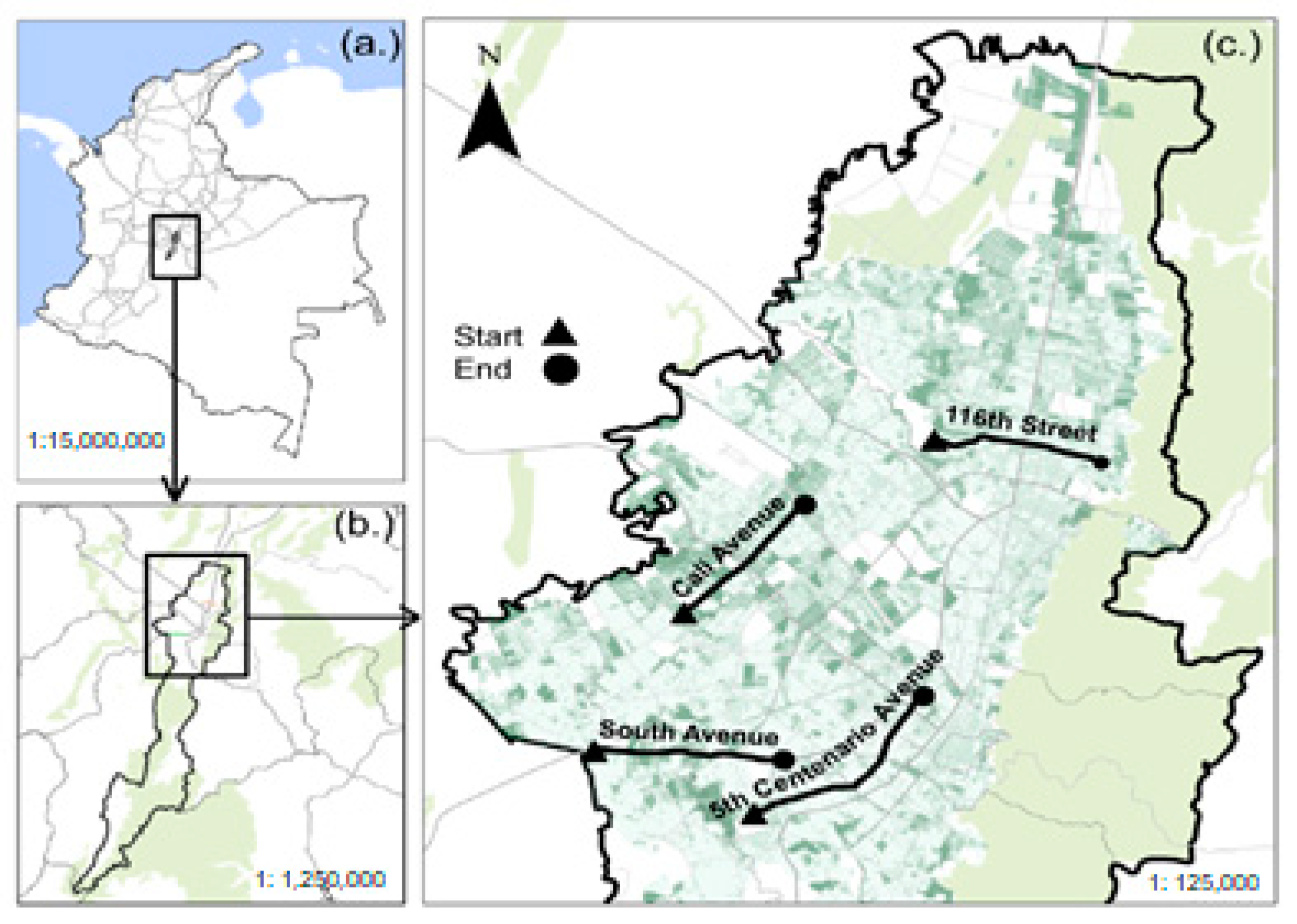
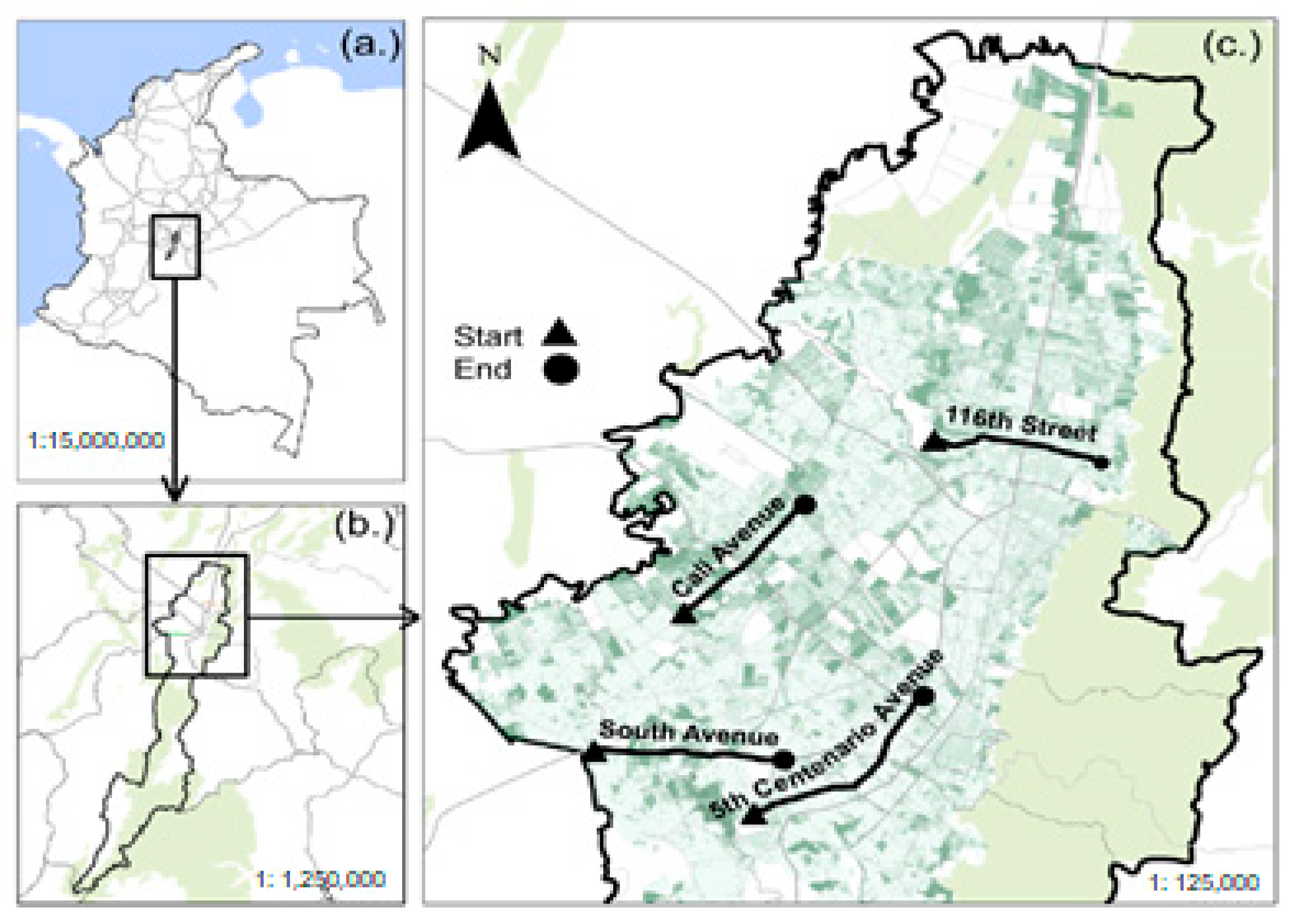
2.1. Study Area
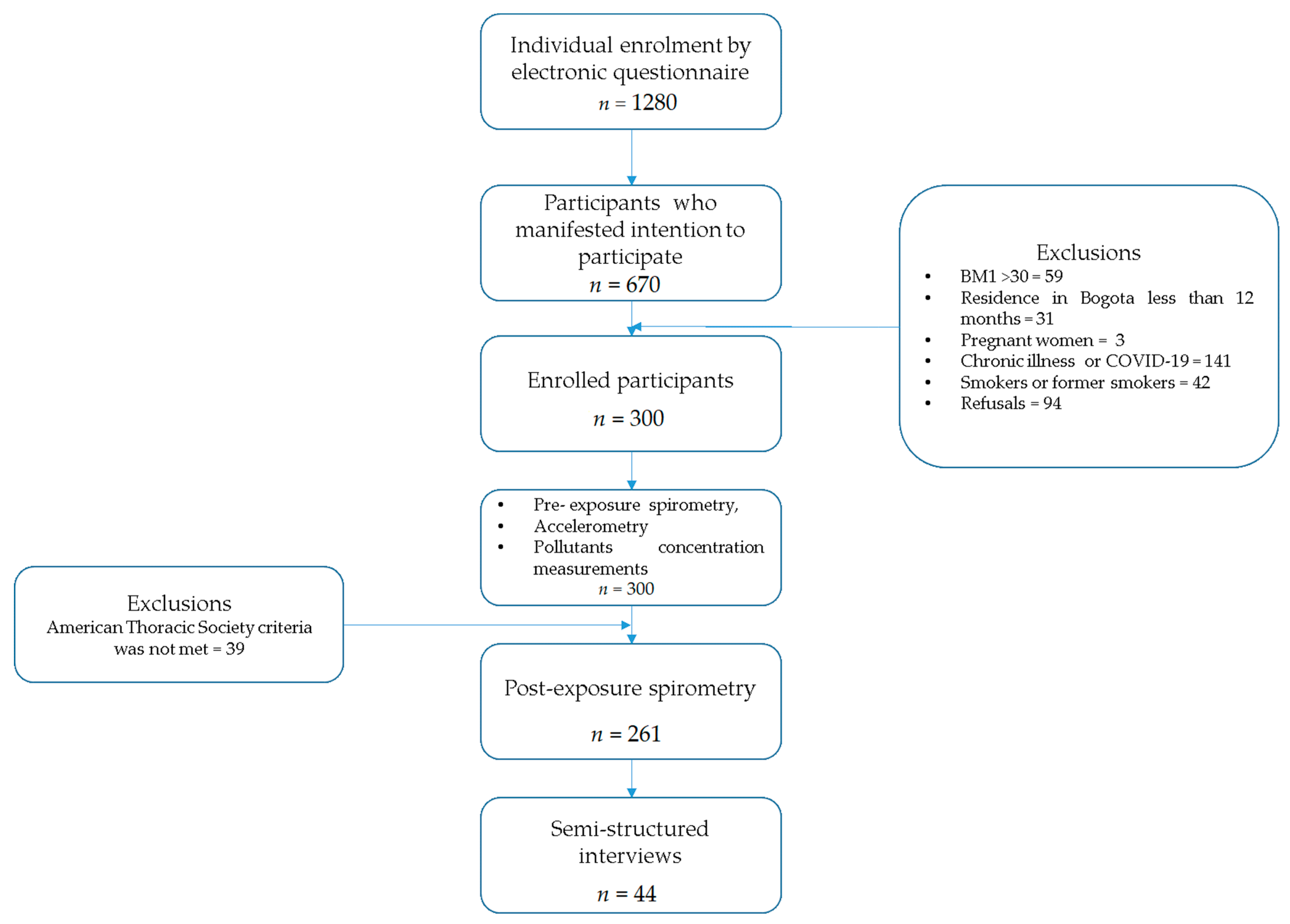
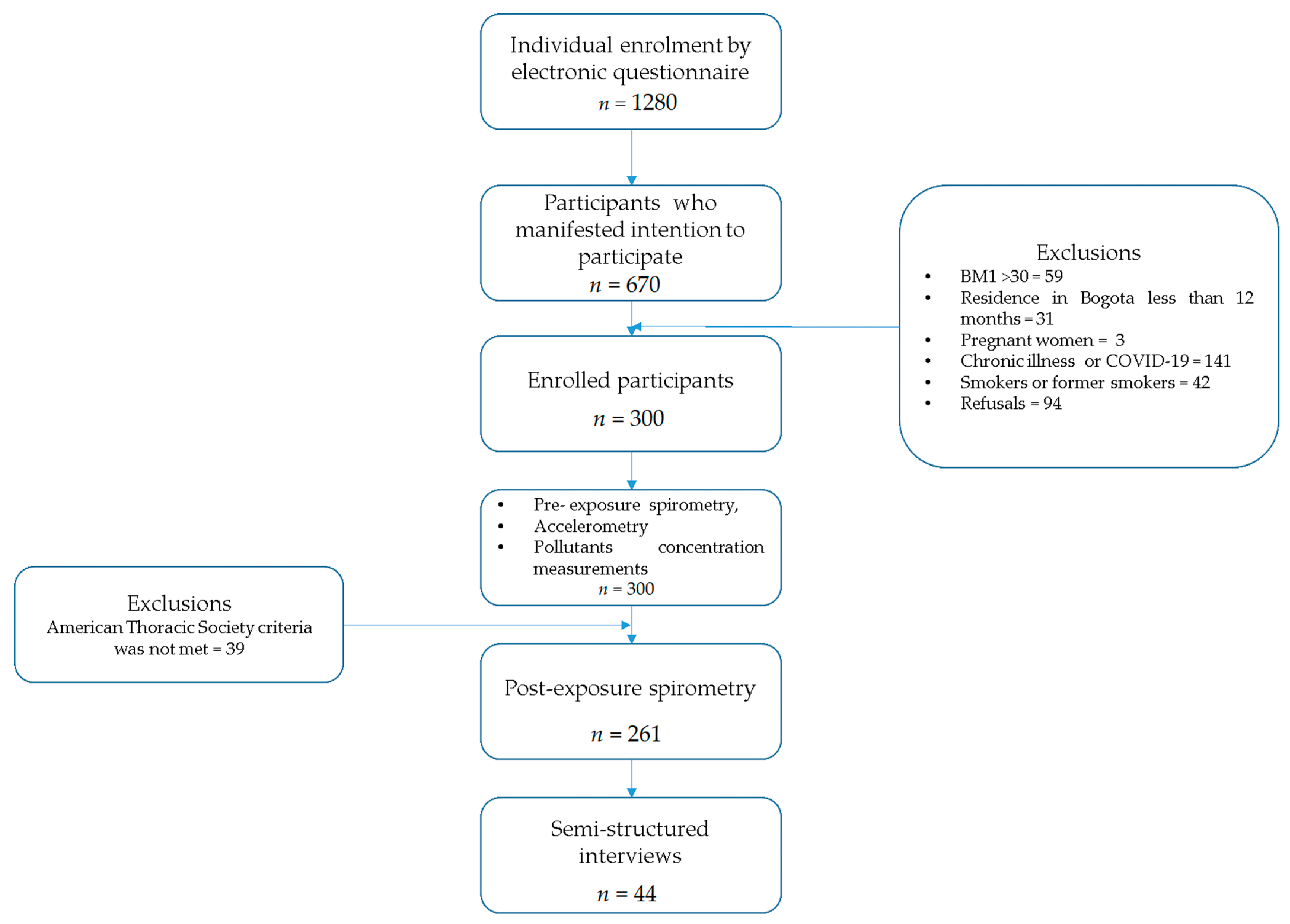
2.2. Sample and Sampling
2.3. Data Collection
2.3.1. Inhaled Doses
2.3.2. Lung Function
2.3.3. Measurements for Monitoring Personal Exposure to PM2.5 and BC
2.3.4. Semi-Structured Interviews
2.4. Data Analysis
2.4.1. Information Processing and Analysis—Quantitative Data
2.4.2. Information Processing and Analysis—Qualitative Data
2.4.3. Triangulation and Integration of Results
3. Results
3.1. Sociodemographic Characteristics
3.2. Air Quality Perception
3.3. Spirometry Parameters
3.4. Personal Exposure
3.5. Inhaled Dose
3.6. Multivariate Model
3.7. Semi-Structured Interviews
3.7.1. Knowledge of Air Quality and Its Relationship with Health
P 8: male cent bici–8:2 The pollution is awful, and, well, in the quality of the air that one breathes. you perceive it in the smell. One says, not here, it smells terrible. Even if you are not seeing the smoke that is coming out of the car, you feel it.
P 6: male 116 van–6:6 The issue of mobile sources, especially public service, and cargo transportation, is what most influences (air quality), and I would say that the second activity would be industrial activities in some areas of the city.
P26: male autosur bus–26:9 Allergies and discomforts such as eye and skin irritation, as in the short term some cancer, a disease in the background is long term because it results from being exposed for a long time.
P 7: female cent bici–7:24 Clearly, between the perception of air quality, or between the perception of pollutants and emotional processes, there is something very, very strong, and that is that we read the world through what we perceive, and we are going to do that through our senses. Then, I do believe that there is a close relationship, I think that this fosters a lot of the mental health problems that we have today. I think that it also makes people prone to violence because it also becomes a violent, hostile context.
3.7.2. Attitudes toward Exposure
P20: female cali van–20:8 when I see a car that is smoking too much, I always try to cover myself, not to inhale; that’s like my attitude. It’s about self-protection.
P25: fem auto sur bus–25:10 It is difficult because what I tell you, it is like getting used to living in this atmosphere, like all the time for me it is normal.
3.7.3. Practices toward Exposure
P 8: male cent bici–8:14. The muscle of the entities is deficient. Colombia is full of standards, at an environmental level, there are many standards, but the muscle to enforce those standards, the legal and economic muscle of the companies, can be more than the standard. So, if that does not change in this society (which is another of the things that bother me at a social level), substantial changes will not be seen.
3.8. Triangulation of the Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buckley, R.M.; Clarke Annez, P.; Spence, M. Urbanization and Growth; The World Bank: Washington, DC, USA, 2008; ISBN 978-0-8213-7573-0. [Google Scholar]
- Pino, P.; Iglesias, V.; Garreaud, R.; Cortés, S.; Canals, M.; Folch, W.; Burgos, S.; Levy, K.; Naeher, L.P.; Steenland, K. Chile Confronts Its Environmental Health Future After 25 Years of Accelerated Growth. Ann. Glob. Health 2015, 81, 354–367. [Google Scholar] [CrossRef] [PubMed]
- Nyhan, M.; McNabola, A.; Misstear, B. Comparison of Particulate Matter Dose and Acute Heart Rate Variability Response in Cyclists, Pedestrians, Bus and Train Passengers. Sci. Total Environ. 2014, 468–469, 821–831. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, C.U.; de Leon, A.P.; Junger, W.; Gouveia, N. Air Pollution and Its Impacts on Health in Vitoria, Espirito Santo, Brazil. Rev. Saúde Pública 2016, 50, 4. [Google Scholar] [CrossRef] [PubMed]
- Pasqua, L.A.; Damasceno, M.V.; Cruz, R.; Matsuda, M.; Garcia Martins, M.; Lima-Silva, A.E.; Marquezini, M.; Saldiva, P.H.N.; Bertuzzi, R. Exercising in Air Pollution: The Cleanest versus Dirtiest Cities Challenge. Int. J. Environ. Res. Public Health 2018, 15, 1502. [Google Scholar] [CrossRef]
- Rodríguez-Villamizar, L.A.; Rojas-Roa, N.Y.; Blanco-Becerra, L.C.; Herrera-Galindo, V.M.; Fernández-Niño, J.A. Short-Term Effects of Air Pollution on Respiratory and Circulatory Morbidity in Colombia 2011–2014: A Multi-City, Time-Series Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1610. [Google Scholar] [CrossRef]
- Santos, U.P.; Garcia, M.L.S.B.; Braga, A.L.F.; Pereira, L.A.A.; Lin, C.A.; de André, P.A.; de André, C.D.S.; da Singer, J.M.; Saldiva, P.H.N. Association between Traffic Air Pollution and Reduced Forced Vital Capacity: A Study Using Personal Monitors for Outdoor Workers. PLoS ONE 2016, 11, e0163225. [Google Scholar] [CrossRef]
- Shah Anoop, S.V.; Lee, K.K.; McAllister, D.A.; Hunter, A.; Nair, H.; Whiteley, W.; Langrish, J.P.; Newby David, E.; Mills Nicholas, L. Short Term Exposure to Air Pollution and Stroke: Systematic Review and Meta-Analysis. BMJ 2015, 350, h1295. [Google Scholar] [CrossRef]
- Alemayehu, Y.A.; Asfaw, S.L.; Terfie, T.A. Exposure to Urban Particulate Matter and Its Association with Human Health Risks. Environ. Sci. Pollut. Res. 2020, 27, 27491–27506. [Google Scholar] [CrossRef]
- Costa Amine Farias; Hoek Gerard; Brunekreef Bert; Ponce de Leon Antônio, C.M. Air Pollution and Deaths among Elderly Residents of São Paulo, Brazil: An Analysis of Mortality Displacement. Environ. Health Perspect. 2017, 125, 349–354. [Google Scholar] [CrossRef]
- Raysoni, A.U.; Armijos, R.X.; Weigel, M.M.; Montoya, T.; Eschanique, P.; Racines, M.; Li, W.-W. Assessment of Indoor and Outdoor PM Species at Schools and Residences in a High-Altitude Ecuadorian Urban Center. Environ. Pollut. 2016, 214, 668–679. [Google Scholar] [CrossRef]
- Edwards, R.D.; Mason, C.N. Spinning the Wheels and Rolling the Dice: Life-Cycle Risks and Benefits of Bicycle Commuting in the U.S. Prev. Med. 2014, 64, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Grøntved, A.; Koivula, R.W.; Johansson, I.; Wennberg, P.; Østergaard, L.; Hallmans, G.; Renström, F.; Franks, P.W. Bicycling to Work and Primordial Prevention of Cardiovascular Risk: A Cohort Study Among Swedish Men and Women. J. Am. Heart Assoc. 2016, 5, e004413. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Sarmiento, O.L.; Stauber, C.; Zarama, R. The Ciclovia and Cicloruta Programs: Promising Interventions to Promote Physical Activity and Social Capital in Bogotá, Colombia. Am. J. Public Health 2012, 103, e23–e30. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, J.; Briggs, D.J. Personal Exposure to Particulate Air Pollution in Transport Microenvironments. Atmos. Environ. 2004, 38, 1–8. [Google Scholar] [CrossRef]
- Kaur, S.; Nieuwenhuijsen, M.J.; Colvile, R.N. Fine Particulate Matter and Carbon Monoxide Exposure Concentrations in Urban Street Transport Microenvironments. Atmos. Environ. 2007, 41, 4781–4810. [Google Scholar] [CrossRef]
- de Nazelle, A.; Fruin, S.; Westerdahl, D.; Martinez, D.; Ripoll, A.; Kubesch, N.; Nieuwenhuijsen, M. A Travel Mode Comparison of Commuters’ Exposures to Air Pollutants in Barcelona. Atmos. Environ. 2012, 59, 151–159. [Google Scholar] [CrossRef]
- SDM Encuestas de Movilidad|Observatorio de Movilidad. Available online: https://observatorio.movilidadbogota.gov.co/encuestas_de_movilidad (accessed on 28 July 2022).
- Ortiz-Durán, E.Y.; Rojas-Roa, N.Y. Estimating air quality change-associated health benefits by reducing PM10 in Bogotá. Rev. Salud Pública 2013, 15, 90–102. [Google Scholar]
- Morales Betancourt, R.; Galvis, B.; Balachandran, S.; Ramos-Bonilla, J.P.; Sarmiento, O.L.; Gallo-Murcia, S.M.; Contreras, Y. Exposure to Fine Particulate, Black Carbon, and Particle Number Concentration in Transportation Microenvironments. Atmos. Environ. 2017, 157, 135–145. [Google Scholar] [CrossRef]
- Malagón-Rojas, J.; Parra-Barrera, E.; Méndez, D. Letter to the Editors: Personal Exposure to PM2.5, Some Considerations for Inhaled Dose Estimation. Environ. Pollut. 2022, 297, 118753. [Google Scholar] [CrossRef]
- Faber, R.; Merkies, R.; Damen, W.; Oirbans, L.; Massa, D.; Kroesen, M.; Molin, E. The Role of Travel-Related Reasons for Location Choice in Residential Self-Selection. Travel Behav. Soc. 2021, 25, 120–132. [Google Scholar] [CrossRef]
- CIEMAT. Percepción Pública de La Contaminación Atmosférica Urbana: Un Análisis Exploratorio; Informes Técnicos Ciemat: Madrid, Spain, 2014. [Google Scholar]
- Gehl, J. Cities for People; ISLAND PRESS: Washington DC, USA, 2010; ISBN 978-1-59726-573-7. [Google Scholar]
- Shiftan, Y.; Kamargianni, M. (Eds.) Preparing for the New Era of Transport Policies: Learning from Experience, 1st ed.; Academic Press: Cambridge, MA, USA, 2018; Volume 1, ISBN 978-0-12-815295-9. [Google Scholar]
- World Health Organization (WHO). WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021; Volume 4, ISBN 978-92-4-003422-8. [Google Scholar]
- Malagón-Rojas, J.N.; Pinzón-Silva, D.C.; Parra, E.L.; Lagos, M.L.F.; Toloza-Perez, Y.G.; Hernández Florez, L.J.; Morales Betancourt, R.; Romero, S.A.; Ríos Cabra, A.P.; Sarmiento, O.L. Assessment of Personal Exposure to Particulate Air Pollution in Different Microenvironments and Traveling by Several Modes of Transportation in Bogotá, Colombia: Protocol for a Mixed Methods Study (ITHACA). JMIR Res. Protoc. 2022, 11, e25690. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, B.J.B.; Ricas, J.; Turato, E.R. Saturation sampling in qualitative health research: Theoretical contributions. Cad. Saúde Pública 2008, 24, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Campbell, A. Translation Equations to Compare ActiGraph GT3X and Actical Accelerometers Activity Counts. BMC Med. Res. Methodol. 2012, 12, 54. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. Accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Lyden, K.; Kozey, S.L.; Staudenmeyer, J.W.; Freedson, P.S. A Comprehensive Evaluation of Commonly Used Accelerometer Energy Expenditure and MET Prediction Equations. Eur. J. Appl. Physiol. 2011, 111, 187–201. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. About the Exposure Factors Handbook; 2015. Available online: https://www.epa.gov/expobox/about-exposure-factors-handbook (accessed on 8 May 2022).
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- LaVange, L.; Davis, S.M.; Hankinson, J.; Enright, P.; Wilson, R.; Barr, R.G.; Aldrich, T.K.; Kalhan, R.; Lemus, H.; Ni, A.; et al. Spirometry Reference Equations from the HCHS/SOL (Hispanic Community Health Study/Study of Latinos). Am. J. Respir. Crit. Care Med. 2017, 196, 993–1003. [Google Scholar] [CrossRef]
- TSI Incorporated SidePak Personal Aerosol Monitor Model AM520/AM520i User Guide 2021. Available online: https://gpcustomer.com/wp-content/uploads/2021/03/TSI_SidePak_AM520_AM520i_User-Manual_021621_V1.pdf (accessed on 8 May 2022).
- TSI Incorporated DustTrak II Aerosol Monitor Model 8530 /8531/8532/8530 EP 2012. Available online: https://tsi.com/getmedia/7c608b93-b6d1-459a-a6a8-2b0e2a55ba91/8530-8531-8532-DustTrak_II-6001893-web?ext=.pdf (accessed on 8 May 2022).
- Aethlabs MicroAeth® AE51 Operating Manual 2016. Available online: https://aethlabs.com/sites/all/content/microaeth/kits/microAeth%20AE51%20Flow%20Calibration%20Kit%20Manual%20Rev%2002%20Updated%20Jul%202016.pdf (accessed on 8 May 2022).
- Ferrero, L.; Bernardoni, V.; Santagostini, L.; Cogliati, S.; Soldan, F.; Valentini, S.; Massabò, D.; Močnik, G.; Gregorič, A.; Rigler, M.; et al. Consistent Determination of the Heating Rate of Light-Absorbing Aerosol Using Wavelength- and Time-Dependent Aethalometer Multiple-Scattering Correction. Sci. Total Environ. 2021, 791, 148277. [Google Scholar] [CrossRef]
- Forero, R.; Nahidi, S.; De Costa, J.; Mohsin, M.; Fitzgerald, G.; Gibson, N.; McCarthy, S.; Aboagye-Sarfo, P. Application of Four-Dimension Criteria to Assess Rigour of Qualitative Research in Emergency Medicine. BMC Health Serv. Res. 2018, 18, 120. [Google Scholar] [CrossRef]
- Samaja, J. Methodological Triangulation (for a Dialectic Understanding of the Approaches Combination). Rev. Cuba. Salud Pública 2018, 44, 431–443. [Google Scholar]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Grassi, S.; Caldiroli, A.; Carnevali, G.S.; Mucci, F.; Iodice, S.; Cantone, L.; Pergoli, L.; Bollati, V. Is There a Link between Air Pollution and Mental Disorders? Environ. Int. 2018, 118, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Petrowski, K.; Bührer, S.; Strauß, B.; Decker, O.; Brähler, E. Examining Air Pollution (PM10), Mental Health and Well-Being in a Representative German Sample. Sci. Rep. 2021, 11, 18436. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Oliva, P.; Zhang, P. Air Pollution and Mental Health: Evidence from China. 2018. Available online: https://www.nber.org/papers/w24686 (accessed on 8 May 2022). [CrossRef]
- Santana, J.C.C.; Miranda, A.C.; Souza, L.; Yamamura, C.L.K.; de Coelho, D.F.; Tambourgi, E.B.; Berssaneti, F.T.; Ho, L.L. Clean Production of Biofuel from Waste Cooking Oil to Reduce Emissions, Fuel Cost, and Respiratory Disease Hospitalizations. Sustainability 2021, 13, 9185. [Google Scholar] [CrossRef]
- Morishita, M.; Thompson, K.C.; Brook, R.D. Understanding Air Pollution and Cardiovascular Diseases: Is It Preventable? Curr. Cardiovasc. Risk Rep. 2015, 9, 30. [Google Scholar] [CrossRef]
- Langrish, J.P.; Li, X.; Wang, S.; Lee, M.M.Y.; Barnes, G.D.; Miller, M.R.; Cassee, F.R.; Boon, N.A.; Donaldson, K.; Li, J.; et al. Reducing Personal Exposure to Particulate Air Pollution Improves Cardiovascular Health in Patients with Coronary Heart Disease. Environ. Health Perspect. 2012, 120, 367–372. [Google Scholar] [CrossRef]
- Langrish, J.P.; Mills, N.L.; Chan, J.K.; Leseman, D.L.; Aitken, R.J.; Fokkens, P.H.; Cassee, F.R.; Li, J.; Donaldson, K.; Newby, D.E.; et al. Beneficial Cardiovascular Effects of Reducing Exposure to Particulate Air Pollution with a Simple Facemask. Part Fibre Toxicol. 2009, 6, 8. [Google Scholar] [CrossRef]
- Zhang, G.; Poslad, S.; Rui, X.; Yu, G.; Fan, Y.; Song, X.; Li, R. Using an Internet of Behaviours to Study How Air Pollution Can Affect People’s Activities of Daily Living: A Case Study of Beijing, China. Sensors 2021, 21, 5569. [Google Scholar] [CrossRef]
- Bédard, A.; Carsin, A.-E.; Fuertes, E.; Accordini, S.; Dharmage, S.C.; Garcia-Larsen, V.; Heinrich, J.; Janson, C.; Johannessen, A.; Leynaert, B.; et al. Physical Activity and Lung Function—Cause or Consequence? PLoS ONE 2020, 15, e0237769. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Macera, C.A.; Addy, C.L.; Sy, F.S.; Wieland, D.; Blair, S.N. Effects of Physical Activity on Exercise Tests and Respiratory Function. Br. J. Sports Med. 2003, 37, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Luzak, A.; Karrasch, S.; Thorand, B.; Nowak, D.; Holle, R.; Peters, A.; Schulz, H. Association of Physical Activity with Lung Function in Lung-Healthy German Adults: Results from the KORA FF4 Study. BMC Pulm. Med. 2017, 17, 215. [Google Scholar] [CrossRef]
- Tainio, M.; de Nazelle, A.J.; Götschi, T.; Kahlmeier, S.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; de Sá, T.H.; Kelly, P.; Woodcock, J. Can Air Pollution Negate the Health Benefits of Cycling and Walking? Prev. Med. 2016, 87, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Bo, Y.; Chan, T.-C.; Zhang, Z.; Lin, C.; Tam, T.; Lau, A.K.H.; Chang, L.; Hoek, G.; Lao, X.Q. Does Fine Particulate Matter (PM2.5) Affect the Benefits of Habitual Physical Activity on Lung Function in Adults: A Longitudinal Cohort Study. BMC Med. 2020, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Heckman, E.J.; O’Connor, G.T. Pulmonary Function Tests for Diagnosing Lung Disease. JAMA 2015, 313, 2278–2279. [Google Scholar] [CrossRef] [PubMed]
- Havet, A.; Hulo, S.; Cuny, D.; Riant, M.; Occelli, F.; Cherot-Kornobis, N.; Giovannelli, J.; Matran, R.; Amouyel, P.; Edmé, J.-L.; et al. Residential Exposure to Outdoor Air Pollution and Adult Lung Function, with Focus on Small Airway Obstruction. Environ. Res. 2020, 183, 109161. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Hao, Y.; Wang, X.; Zheng, C.; Lv, H.; Lu, X.; Wei, H.; Huang, J.; Qin, Y.; et al. Fine Particulate Matter, Temperature, and Lung Function in Healthy Adults: Findings from the HVNR Study. Chemosphere 2014, 108, 168–174. [Google Scholar] [CrossRef]
- Yang, T.; Chen, R.; Gu, X.; Xu, J.; Yang, L.; Zhao, J.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; et al. Association of Fine Particulate Matter Air Pollution and Its Constituents with Lung Function: The China Pulmonary Health Study. Environ. Int. 2021, 156, 106707. [Google Scholar] [CrossRef]
- Desiraju, K.; Agrawal, A. Impulse Oscillometry: The State-of-Art for Lung Function Testing. Lung India 2016, 33, 410. [Google Scholar] [CrossRef]
- Thurston, G.D.; Newman, J.D. Walking to a Pathway for Cardiovascular Effects of Air Pollution. Lancet 2018, 391, 291–292. [Google Scholar] [CrossRef]
- Chaney, R.A.; Sloan, C.D.; Cooper, V.C.; Robinson, D.R.; Hendrickson, N.R.; McCord, T.A.; Johnston, J.D. Personal Exposure to Fine Particulate Air Pollution While Commuting: An Examination of Six Transport Modes on an Urban Arterial Roadway. PLoS ONE 2017, 12, e0188053. [Google Scholar] [CrossRef] [PubMed]
- Franco, J.F.; Segura, J.F.; Mura, I. Air Pollution alongside Bike-Paths in Bogotá-Colombia. Front. Environ. Sci. 2016, 4, 77. [Google Scholar] [CrossRef]
- Peng, L.; Shen, Y.; Gao, W.; Zhou, J.; Pan, L.; Kan, H.; Cai, J. Personal Exposure to PM2.5 in Five Commuting Modes under Hazy and Non-Hazy Conditions. Environ. Pollut. 2021, 289, 117823. [Google Scholar] [CrossRef] [PubMed]
- de Nazelle, A.; Bode, O.; Orjuela, J.P. Comparison of Air Pollution Exposures in Active vs. Passive Travel Modes in European Cities: A Quantitative Review. Environ. Int. 2017, 99, 151–160. [Google Scholar] [CrossRef]
- Cherrie, J.W.; Apsley, A.; Cowie, H.; Steinle, S.; Mueller, W.; Lin, C.; Horwell, C.J.; Sleeuwenhoek, A.; Loh, M. Effectiveness of Face Masks Used to Protect Beijing Residents against Particulate Air Pollution. Occup. Environ. Med. 2018, 75, 446–452. [Google Scholar] [CrossRef]
- Vargas Pinilla, O.C. Ejercicio y entrenamiento en altura: Efectos fisiológicos y protocolos. Rev. Cienc. Salud 2014, 12, 115–130. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Category | Meaning | Questions |
|---|---|---|
| Knowledge of air quality and health | Mental representations preceding cognitive processes developed, socially constructed, and recreated during everyday interactions. |
|
| Attitudes toward exposure | Means the orientation (positive or negative) before an object of the pre-existing social world. Cognitive, affective and behavioral components converge in them. |
|
| Practices related to exposure | They express both the human experience and all those activities that materialize in a direct and daily relationship of people with the world. They are constituted as an action on reality. |
|
| Variable | Minivan | Bicycle | Bus | p | |
|---|---|---|---|---|---|
| Age (years) (mean ± SD) | 32.84 ± 10.35 | 31.75 ± 8.35 | 30.86 ± 8.78 | >0.05 | |
| BMI (mean ± SD) | 22.94 ± 3.46 | 22.95 ± 3.21 | 23.22 ± 3.36 | >0.05 | |
| Sex (% (n)) | Male | 28.3% (n = 30) | 59.26% (n = 48) | 38.05% (n = 43) | >0.05 |
| Female | 71.7% (n = 76) | 40.74% (n = 33) | 61.95% (n = 70) | ||
| Routes (% (n)) | Cali Avenue | 23.58% (n = 25) | 25.93% (n = 21) | 25.66% (n = 29) | >0.05 |
| 116th Street | 26.42% (n = 28) | 25.93% (n = 21) | 23.89% (n = 27) | ||
| South Avenue | 25.47% (n = 27) | 22.22% (n = 18) | 25.66% (n = 29) | ||
| Quinto Centenario Avenue | 24.53% (n = 26) | 25.93% (n = 21) | 24.78% (n = 28) | ||
| Spirometry parameters (mean ± SD) | Pre-FVC | 3.79 ± 3.79 | 4.34 ± 4.34 | 3.87 ± 3.87 | >0.05 |
| Post-FVC | 3.72 ± 0.76 | 4.26 ± 0.86 | 3.88 ± 1.14 | >0.05 | |
| Pre-FEV1 | 3.08 ± 0.66 | 3.55 ± 0.68 | 3.21 ± 0.88 | >0.05 | |
| Post-FEV1 | 3.14 ± 0.62 | 3.53 ± 0.69 | 3.25 ± 0.85 | >0.05 | |
| Pre-FEF25–75% | 3.48 ± 0.93 | 3.69 ± 1.02 | 3.47 ± 1.13 | >0.05 | |
| Post-FEF25–75% | 3.58 ± 0.94 | 3.68 ± 1.02 | 3.63 ± 1.05 | >0.05 | |
| Pre-FEV1/FVC | 82.86 ± 8.20 | 82.20 ± 5.70 | 83.40 ± 6.26 | >0.05 | |
| Post-FEV1/FVC | 83.88 ± 9.47 | 82.92 ± 5.27 | 83.54 ± 9.82 | >0.05 | |
| Aim of the Study | Quantitative Mode | Qualitative Moment | Relationship | Summary of the Triangulation | |
|---|---|---|---|---|---|
| Summary of Results Related to the Objectives | Synthesis of Social Representations | ||||
| Describe the perception of the participants of air pollution in Bogotá. | Most of the participants reported that the quality of the air they breathe on their routes to places of work/study was not good enough (regular 47%, bad 24% and very bad 12%), with a link between air quality and health (72%). According to the perception of the participants, the human systems most frequently affected by air pollution were respiratory (94%), visual (72%), skin (67%), cardiovascular (41%), and gastrointestinal (17%). The participants stated that they use elements to protect against air pollution (62%). The most frequent element was surgical/cloth mask (40%), followed by N95 (7%). Likewise, the participants declared practices such as closing windows (16%); open windows (7%) and hold your breath (10%)” | Knowledge about air quality and its relationship with health. | The perception of air quality was mediated by the sensory experience (visual and olfactory) and the context where the sensation occurred. Recognizing an environment with high levels of contamination, public transport, cargo, and industries as the largest sources of contamination, as well as a high relationship between air pollution and health, which is expressed, on the one hand, in the appearance of respiratory diseases, eye irritation and skin discomfort, and on the other hand, the alteration of mental health expressed in changes in moods and stressful situations | Complementarity relationship between the quantitative-qualitative results. | The integrative analysis of the quantitative and qualitative results showed that the air quality in the city is poor, especially in routes by bus and in the Southern part of the city. |
| Attitudes towards exposure | Two types of attitudes were identified, (1) associated with knowledge, mostly attitudes towards individual protection in order to reduce exposure. (2) attitudes of resignation, habits, naturalization where being exposed is an inevitable condition | ||||
| Practices against exposure | Individual protection practices, mainly through the use of face masks became an element that establishes protection against contamination | ||||
| To estimate changes in lung volumes and respiratory symptoms in users according to the means of transport evaluated. | No differences were observed between pre and post spirometry within the FVC and FEV1 parameters. | Knowledge of air quality and its relationship with health | The respiratory system is recognized as the main affected system by air pollution. Symptoms such as fatigue, shortness of breath, cough, allergic reactions, sore throat, and nasal congestion were identified as manifestations of the contamination. | Neutrality relationship, since qualitative information does not provide results against spirometry alterations. | Social representations do not recognize spirometry alterations as a factor associated with contamination. However, a representation is constructed that relates pollution levels with health effects, especially with effects on the respiratory system. |
| Attitudes towards exposure | The control over the potential exposure to air pollutants was assumed to be an individual responsibility The risk transferred to the person was maximized with the use of personal protection elements. | ||||
| Exposure Practices | The influence of cognitive and affective factors was recognized as a determinant of environmental behaviour and its relationship with health care. This behaviour included individual actions to protect and implement healthy lifestyles | ||||
| To determine the concentration of P.M 2.5 and black carbon in the microenvironments evaluated. | The concentration of PM2.5 in buses was the highest (median 50.67 ug m−3; RI: 306.7), followed by cars (38.49; RI: 182.3), and bicycles. Similarly, the concentrations of CN in buses were the highest (29.94 ug m−3; RI: 116.3); these differed significantly from the concentrations in bicycles (7.83 ug m−3; RI: 26.6) and car (18.54 ug m−3; IR: 68.6) | Relation of complementarity, while the qualitative component allows expanding from the representations of the participants | The air pollutants concentration was variable according to route and mode. Perception of the air pollutants was not influenced by the transport mode or route | ||
| The concentration of PM2.5 and BC as significantly lower in Street 116 compared to Southern avenue, and Cali Avenue. | Attitudes towards exposure | The use of protection elements is claimed, especially against direct and sudden exposure. Although some attitudes suggest a generalized awareness of the presence of air pollution, they also reflect a considerable level of apparent ambivalence, a naturalization that locates and signifies a distancing from the problem and a lack of social participation. | |||
| The mean inhaled dose of PM2.5 and BC doses were significantly higher among men compared to women. There was no association between inhaled PM2.5 and BC dose with route or mode of transport. There was no correlation between the spirometry parameters, age, body mass index, and inhaled dose of PM2.5 and carbon black. There was a positive correlation between travel time and inhaled dose of PM2.5 and BC. | Practices towards exposure | The use of the bicycle is claimed as the ideal means of transport, not only to reduce emissions, but also to improve and maintain optimal health conditions. They also suggest the adaptation of infrastructure and security conditions that allow this practice. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malagón-Rojas, J.N.; Parra-Barrera, E.L.; Toloza-Pérez, Y.G.; Soto, H.; Lagos, L.F.; Mendez, D.; Rico, A.; Almentero, J.E.; Quintana-Cortes, M.A.; Pinzón-Silva, D.C.; et al. Assessment of Factors Influencing Personal Exposure to Air Pollution on Main Roads in Bogota: A Mixed-Method Study. Medicina 2022, 58, 1125. https://doi.org/10.3390/medicina58081125
Malagón-Rojas JN, Parra-Barrera EL, Toloza-Pérez YG, Soto H, Lagos LF, Mendez D, Rico A, Almentero JE, Quintana-Cortes MA, Pinzón-Silva DC, et al. Assessment of Factors Influencing Personal Exposure to Air Pollution on Main Roads in Bogota: A Mixed-Method Study. Medicina. 2022; 58(8):1125. https://doi.org/10.3390/medicina58081125
Chicago/Turabian StyleMalagón-Rojas, Jeadran N., Eliana L. Parra-Barrera, Yesith Guillermo Toloza-Pérez, Hanna Soto, Luisa F. Lagos, Daniela Mendez, Andrea Rico, Julia Edith Almentero, Mónica A. Quintana-Cortes, Diana C. Pinzón-Silva, and et al. 2022. "Assessment of Factors Influencing Personal Exposure to Air Pollution on Main Roads in Bogota: A Mixed-Method Study" Medicina 58, no. 8: 1125. https://doi.org/10.3390/medicina58081125
APA StyleMalagón-Rojas, J. N., Parra-Barrera, E. L., Toloza-Pérez, Y. G., Soto, H., Lagos, L. F., Mendez, D., Rico, A., Almentero, J. E., Quintana-Cortes, M. A., Pinzón-Silva, D. C., García, A., Benavides-Piracón, J. A., Zona-Rubio, D. C., Portilla, C., Wilches-Mogollon, M. A., Romero-Díaz, S. A., Hernández-Florez, L. J., Morales, R., & Sarmiento, O. L. (2022). Assessment of Factors Influencing Personal Exposure to Air Pollution on Main Roads in Bogota: A Mixed-Method Study. Medicina, 58(8), 1125. https://doi.org/10.3390/medicina58081125