
Long-Term Effects of Rifaximin on Patients with Hepatic Encephalopathy: Its Possible Effects on the Improvement in the Blood Ammonia Concentration Levels, Hepatic Spare Ability and Refractory Ascites
 , , , ,
, , , ,
Abstract
:1. Introduction
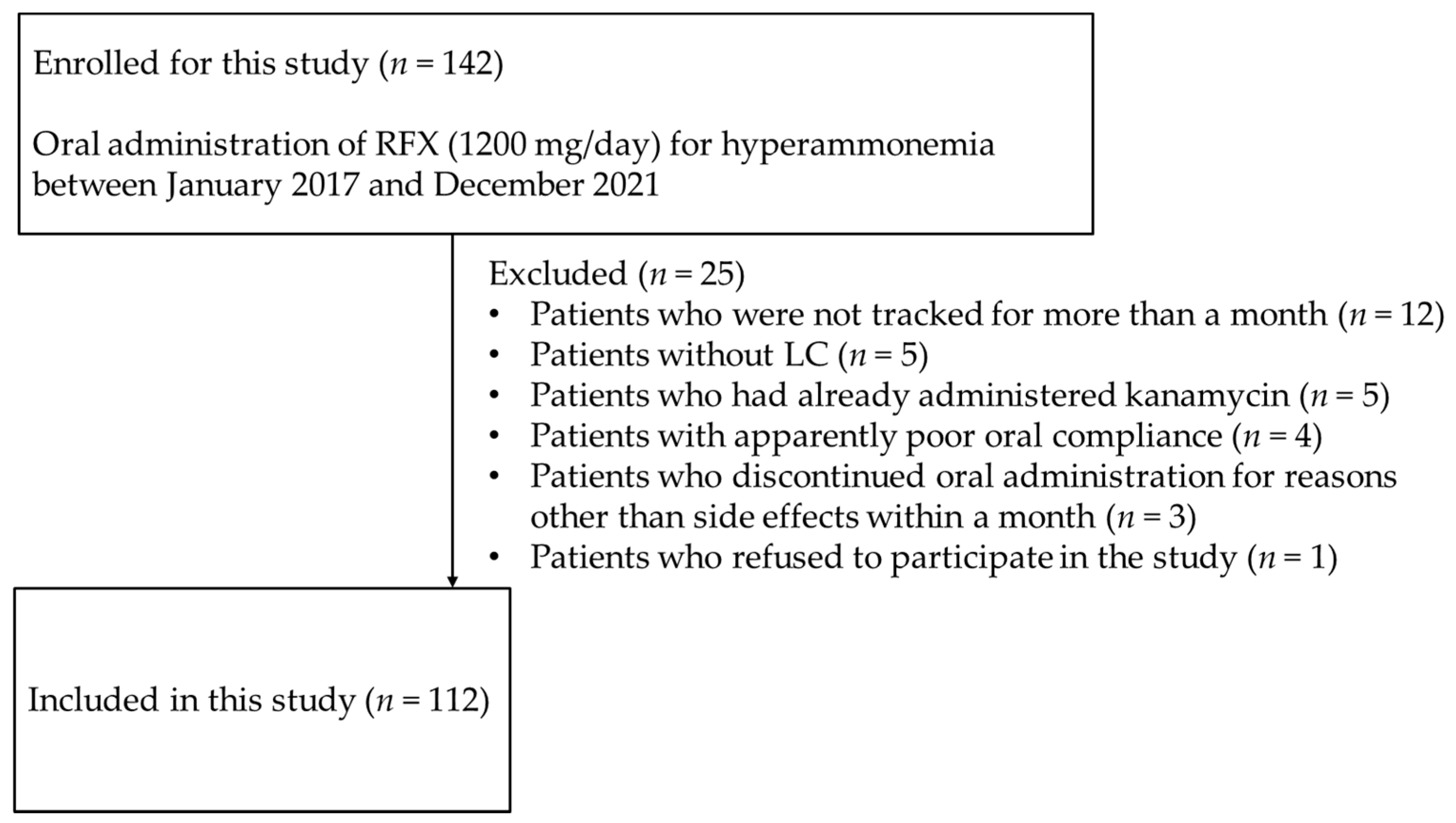
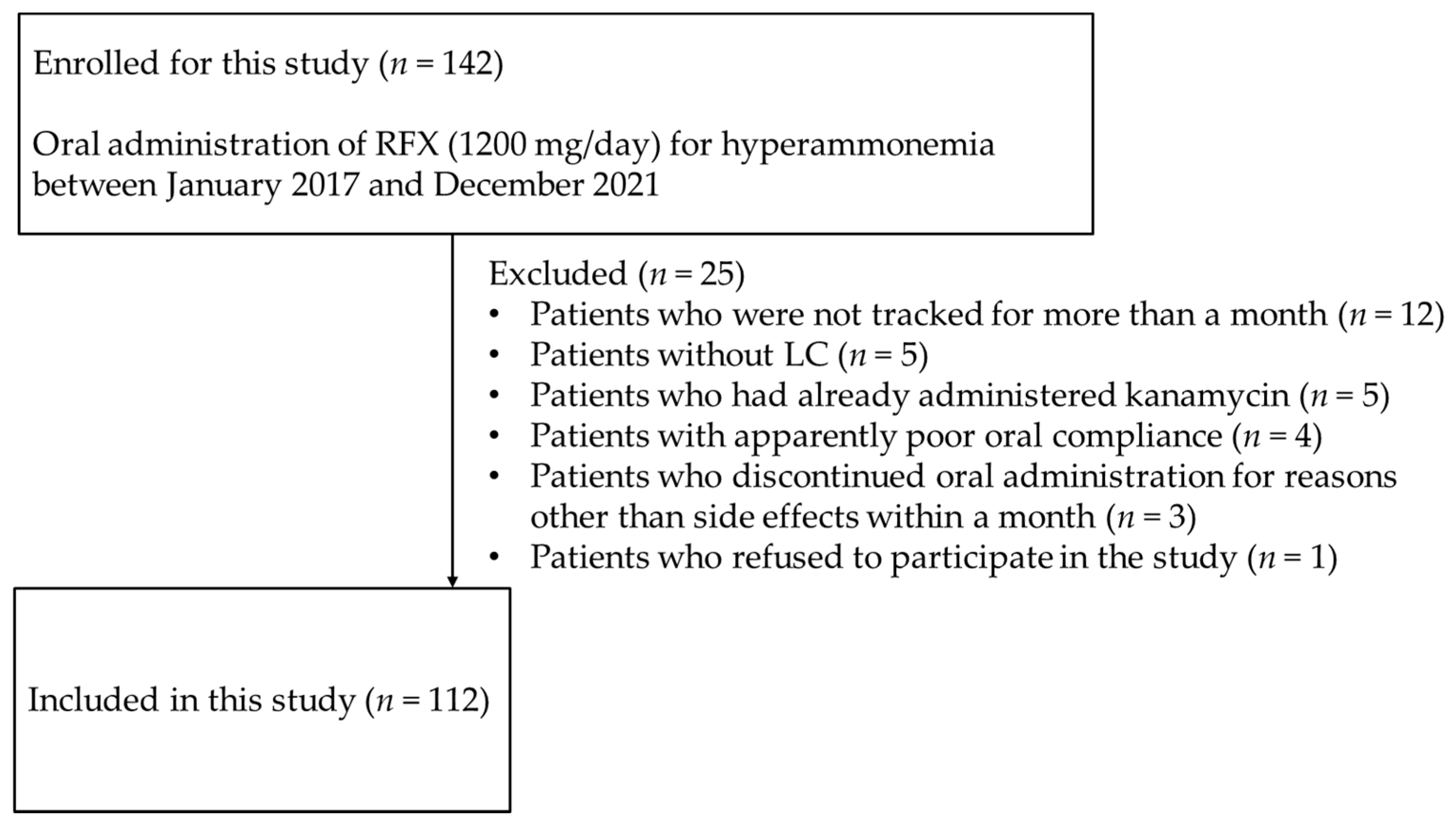
2. Materials and Methods
2.1. Statistical Analyses
2.2. Ethical Statement
3. Results
3.1. Clinical Characteristics of the Study Population
3.2. Long-Term Effects of Administration of RFX on Hyperammonemia and HE
3.3. Secondary Therapeutic Effects
3.4. Adverse Events
3.5. Relationship between RFX Administration and the RAAS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poordad, F.F. Review article: The burden of hepatic encephalopathy. Aliment. Pharmacol. Ther. 2007, 25, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, J.; Chung, C.; Blei, A.T. Brain edema in acute liver failure. A window to the pathogenesis of hepatic encephalopathy. Ann. Hepatol. 2003, 2, 12–22. [Google Scholar] [CrossRef]
- Dbouk, N.; McGuire, B.M. Hepatic encephalopathy: A review of its pathophysiology and treatment. Curr. Treat. Options Gastroenterol. 2006, 9, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yang, F.; Lu, H.; Wang, B.; Chen, Y.; Lei, D.; Wang, Y.; Zhu, B.; Li, L. Characterization of fecal microbial communities in patients with liver cirrhosis. Hepatology 2011, 54, 562–572. [Google Scholar] [CrossRef]
- Qin, N.; Yang, F.; Li, A.; Prifti, E.; Chen, Y.; Shao, L.; Guo, J.; le Chatelier, E.; Yao, J.; Wu, L.; et al. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014, 513, 59–64. [Google Scholar] [CrossRef]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- American Association for the Study of Liver Diseases; European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guidelines by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef]
- Gerard, L.; Garey, K.W.; DuPont, H.L. Rifaximin: A non-absorbable rifamycin antibiotic for use in non-systemic gastrointestinal infections. Expert Rev. Anti Infect. Ther. 2005, 3, 201–211. [Google Scholar] [CrossRef]
- Debbia, E.A.; Maioli, E.; Roveta, S.; Marchese, A. Effects of rifaximin on bacterial virulence mechanisms at supra- and sub-inhibitory concentrations. J. Chemother. 2008, 20, 186–194. [Google Scholar] [CrossRef]
- Jiang, Z.D.; DuPont, H.L. Rifaximin: In vitro and in vivo antibacterial activity—A review. Chemotherapy 2005, 51, 67–72. [Google Scholar] [CrossRef]
- Suzuki, K.; Endo, R.; Takikawa, Y.; Moriyasu, F.; Aoyagi, Y.; Moriwaki, H.; Terai, S.; Sakaida, I.; Sakai, Y.; Nishiguchi, S.; et al. Efficacy and safety of rifaximin in Japanese patients with hepatic encephalopathy: A phase II/III, multicenter, randomized, evaluator-blinded, active-controlled trial and a phase III, multicenter, open trial. Hepatol. Res. 2018, 48, 411–423. [Google Scholar] [CrossRef]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Moriyasu, F.; Aoyagi, Y.; Moriwaki, H.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [Google Scholar] [CrossRef]
- Mullen, K.D.; Sanyal, A.J.; Bass, N.M.; Poordad, F.F.; Sheikh, M.Y.; Frederick, R.T.; Bortey, E.; Forbes, W.P. Rifaximin is safe and well tolerated for long-term maintenance of remission from overt hepatic encephalopathy. Clin. Gastroenterol. Hepatol. 2014, 12, 1390–1397.e2. [Google Scholar] [CrossRef]
- Kang, S.H.; Lee, Y.B.; Lee, J.H.; Nam, J.Y.; Chang, Y.; Cho, H.; Yoo, J.-J.; Cho, Y.Y.; Cho, E.J.; Yu, S.J.; et al. Rifaximin treatment is associated with reduced risk of cirrhotic complications and prolonged overall survival in patients experiencing hepatic encephalopathy. Aliment. Pharmacol. Ther. 2017, 46, 845–855. [Google Scholar] [CrossRef]
- Hudson, M.; Schuchmann, M. Long-term management of hepatic encephalopathy with lactulose and/or rifaximin: A review of the evidence. Eur. J. Gastroenterol. Hepatol. 2019, 31, 434–450. [Google Scholar] [CrossRef]
- Vlachogiannakos, J.; Viazis, N.; Vasianopoulou, P.; Vafiadis, I.; Karamanolis, D.G.; Ladas, S.D. Long-term administration of rifaximin improves the prognosis of patients with decompensated alcoholic cirrhosis. J. Gastroenterol. Hepatol. 2013, 28, 450–455. [Google Scholar] [CrossRef]
- Nishida, S.; Hamada, K.; Nishino, N.; Fukushima, D.; Koyanagi, R.; Horikawa, Y.; Shiwa, Y.; Saitoh, S. Efficacy of long-term rifaximin treatment for hepatic encephalopathy in the Japanese. World J. Hepatol. 2019, 11, 531–541. [Google Scholar] [CrossRef]
- Ishikawa, T.; Endo, S.; Imai, M.; Azumi, M.; Nozawa, Y.; Sano, T.; Iwanaga, A.; Honma, T.; Yoshida, T. Changes in the body composition and nutritional status after long-term rifaximin therapy for hyperammonemia in Japanese patients with hepatic encephalopathy. Intern. Med. 2020, 59, 2465–2469. [Google Scholar] [CrossRef]
- Hiramine, Y.; Uto, H.; Mawatari, S.; Kanmura, S.; Imamura, Y.; Hiwaki, T.; Saishoji, A.; Kakihara, A.; Maenohara, S.; Tokushige, K.; et al. Efficacy of rifaximin, a poorly absorbed rifamycin antimicrobial agent, for hepatic encephalopathy in Japanese patients. Hepatol. Res. 2021, 51, 445–460. [Google Scholar] [CrossRef]
- Suzuki, H.; Sezaki, H.; Suzuki, F.; Kasuya, K.; Sano, T.; Fujiyama, S.; Kawamura, Y.; Hosaka, T.; Akuta, N.; Saitoh, S.; et al. Real-world effects of long-term rifaximin treatment for Japanese patients with hepatic encephalopathy. Hepatol. Res. 2019, 49, 1406–1413. [Google Scholar] [CrossRef]
- Neff, G.; Zachry, W., III. Systematic review of the economic burden of overt hepatic encephalopathy and pharmacoeconomic impact of rifaximin. Pharmacoeconomics 2018, 36, 809–822. [Google Scholar] [CrossRef]
- Oey, R.C.; Buck, L.E.M.; Erler, N.S.; van Buuren, H.R.; de Man, R.A. The efficacy and safety of rifaximin-α: A 2-year observational study of overt hepatic encephalopathy. Therap. Adv. Gastroenterol. 2019, 12, 1756284819858256. [Google Scholar] [CrossRef]
- Lyon, K.C.; Likar, E.; Martello, J.L.; Regier, M. Retrospective cross-sectional pilot study of rifaximin dosing for the prevention of recurrent hepatic encephalopathy. J. Gastroenterol. Hepatol. 2017, 32, 1548–1552. [Google Scholar] [CrossRef]
- Goyal, O.; Sidhu, S.S.; Kishore, H. Minimal hepatic encephalopathy in cirrhosis- how long to treat? Ann. Hepatol. 2017, 16, 115–122. [Google Scholar] [CrossRef]
- Bruyneel, M.; Sersté, T.; Libert, W.; van den Broecke, S.; Ameye, L.; Dachy, B.; Mulkay, J.-P.; Moreno, C.; Gustot, T. Improvement of sleep architecture parameters in cirrhotic patients with recurrent hepatic encephalopathy with the use of rifaximin. Eur. J. Gastroenterol. Hepatol. 2017, 29, 302–308. [Google Scholar] [CrossRef]
- Ahire, K.; Sonawale, A. Comparison of rifaximin plus lactulose with the lactulose alone for the treatment of hepatic encephalopathy. J. Assoc. Physicians India 2017, 65, 42–46. [Google Scholar]
- Lv, X.Y.; Ding, H.G.; Zheng, J.F.; Fan, C.L.; Li, L. Rifaximin improves survival in cirrhotic patients with refractory ascites: A real-world study. World J. Gastroenterol. 2020, 26, 199–218. [Google Scholar] [CrossRef]
- Hanafy, A.S.; Hassaneen, A.M. Rifaximin and midodrine improve clinical outcome in refractory ascites including renal function, weight loss and short-term survival. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1455–1461. [Google Scholar] [CrossRef]
- Kimer, N.; Pedersen, J.S.; Busk, T.M.; Gluud, L.L.; Hobolth, L.; Krag, A.; Møller, S.; Bendtsen, F.; Copenhagen Rifaximin (CoRif) Study Group. Rifaximin has no effect on hemodynamics in decompensated cirrhosis: A randomized, double-blind, placebo-controlled trial. Hepatology 2017, 65, 592–603. [Google Scholar] [CrossRef]
- Lim, Y.L.; Kim, M.Y.; Jang, Y.O.; Baik, S.K.; Kwon, S.O. Rifaximin and propranolol combination therapy is more effective than propranolol monotherapy for the reduction of portal pressure: An open randomized controlled pilot study. Gut Liver 2017, 11, 702–710. [Google Scholar] [CrossRef]
- Dong, T.; Aronsohn, A.; Gautham Reddy, K.; Te, H.S. Rifaximin decreases the incidence and severity of acute kidney injury and hepatorenal syndrome in cirrhosis. Dig. Dis. Sci. 2016, 61, 3621–3626. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W.; Arroyo, V.; Bernardi, M.; Epstein, M.; Henriksen, J.H.; Rodés, J. Peripheral arterial vasodilation hypothesis: A proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 1988, 8, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, J.H.; Møller, S. Cardiac and systemic haemodynamic complications of liver cirrhosis. Scand. Cardiovasc. J. 2009, 43, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Heller, J.; Kristeleit, H.; Brensing, K.A.; Woitas, R.P.; Spengler, U.; Sauerbruch, T. Nitrite and nitrate levels in patients with cirrhosis of the liver: Influence of kidney function and fasting state. Scand. J. Gastroenterol. 1999, 34, 297–302. [Google Scholar]
- Bataller, R.; Ginès, P.; Nicolás, J.M.; Görbig, M.N.; Garcia-Ramallo, E.; Gasull, X.; Bosch, J.; Arroyo, V.; Rodés, J. Angiotensin II induces contraction and proliferation of human hepatic stellate cells. Gastroenterology 2000, 118, 1149–1156. [Google Scholar] [CrossRef]
- Ikura, Y.; Ohsawa, M.; Shirai, N.; Sugama, Y.; Fukushima, H.; Suekane, T.; Hirayama, M.; Ehara, S.; Naruko, T.; Ueda, M. Expression of angiotensin II type one receptor in human cirrhotic livers: Its relation to fibrosis and portal hypertension. Hepatol. Res. 2005, 32, 107–116. [Google Scholar] [CrossRef]
- Paternostro, R.; Reiberger, T.; Mandorfer, M.; Schwarzer, R.; Schwabl, P.; Bota, S.; Ferlitsch, M.; Trauner, M.; Peck-Radosavljevic, M.; Ferlitsch, A. Plasma renin concentration represents an independent risk factor for mortality and is associated with liver dysfunction in patients with cirrhosis. J. Gastroenterol. Hepatol. 2017, 32, 184–190. [Google Scholar] [CrossRef]
- Tandon, P.; Abraldes, J.G.; Berzigotti, A.; Garcia-Pagan, J.C.; Bosch, J. Renin-angiotensin-aldosterone inhibitors in the reduction of portal pressure: A systematic review and meta-analysis. J. Hepatol. 2010, 53, 273–282. [Google Scholar] [CrossRef]
- Kim, G.; Kim, J.; Lim, Y.L.; Kim, M.Y.; Baik, S.K. Renin-angiotensin system inhibitors and fibrosis in chronic liver disease: A systematic review. Hepatol. Int. 2016, 10, 819–828. [Google Scholar] [CrossRef]
- Pelusi, S.; Petta, S.; Rosso, C.; Borroni, V.; Fracanzani, A.L.; Dongiovanni, P.; Craxi, A.; Bugianesi, E.; Fargion, S.; Valenti, L. Renin-angiotensin system inhibitors, type 2 diabetes and fibrosis progression: An observational study in patients with nonalcoholic fatty liver disease. PLoS ONE 2016, 11, e0163069. [Google Scholar] [CrossRef]
- Aihara, Y.; Yoshiji, H.; Noguchi, R.; Kaji, K.; Namisaki, T.; Shirai, Y.; Douhara, A.; Moriya, K.; Kawaratani, H.; Fukui, H. Direct renin inhibitor, aliskiren, attenuates the progression of non-alcoholic steatohepatitis in the rat model. Hepatol. Res. 2013, 43, 1241–1250. [Google Scholar] [CrossRef]
- Noguchi, R.; Kaji, K.; Namisaki, T.; Moriya, K.; Kitade, M.; Takeda, K.; Kawaratani, H.; Okura, Y.; Aihara, Y.; Furukawa, M.; et al. Serum angiotensin-converting enzyme level for evaluating significant fibrosis in chronic hepatitis B. World J. Gastroenterol. 2017, 23, 6705–6714. [Google Scholar] [CrossRef]
- Kaji, K.; Takaya, H.; Saikawa, S.; Furukawa, M.; Sato, S.; Kawaratani, H.; Kitade, M.; Moriya, K.; Namisaki, T.; Akahane, T.; et al. Rifaximin ameliorates hepatic encephalopathy and endotoxemia without affecting the gut microbiome diversity. World J. Gastroenterol. 2017, 23, 8355–8366. [Google Scholar] [CrossRef]
- Kalambokis, G.N.; Mouzaki, A.; Rodi, M.; Pappas, K.; Fotopoulos, A.; Xourgia, X.; Tsianos, E.V. Rifaximin improves systemic hemodynamics and renal function in patients with alcohol-related cirrhosis and ascites. Clin. Gastroenterol. Hepatol. 2012, 10, 815–818. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Suzuki, F.; Imamura, M.; Murashima, N.; Yanase, M.; Mine, T.; Fujisawa, M.; Sato, I.; Yoshiji, H.; Okita, K.; et al. Rifaximin-altered gut microbiota components associated with liver/neuropsychological functions in patients with hepatic encephalopathy: An exploratory data analysis of phase II/III clinical trials. Hepatol. Res. 2019, 49, 404–418. [Google Scholar] [CrossRef]
- Schulz, C.; Schütte, K.; Vilchez-Vargas, R.; Vasapolli, R.; Malfertheiner, P. Long-term effect of rifaximin with and without lactulose on the active bacterial assemblages in the proximal small bowel and faeces in patients with minimal hepatic encephalopathy. Dig. Dis. 2019, 37, 161–169. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 112 |
|---|---|
| Sex (male/female) | 75/37 |
| Age (in years, expressed as mean ± SD) | 65.1 ± 11.6 |
| Etiology | |
| Alcohol consumption | 47 (42.0%) |
| Viral hepatitis | 27 (24.1%) |
| NASH | 14 (12.5%) |
| Alcohol consumption and viral hepatitis | 7 (6.3%) |
| Alcohol consumption and autoimmune hepatitis | 1 (0.9%) |
| Others | 16 (14.3%) |
| Child–Pugh classification | |
| Class A | 6 (5.4%) |
| Class B | 56 (50.0%) |
| Class C | 50 (44.6%) |
| Child–Pugh score (mean ± SD) | 9.54 ± 2.1 |
| MELD score | 12.9 ± 4.43 |
| MELD sodium score | 13.4 ± 4.98 |
| Blood ammonia concentration, NH3 (μg/dL) (mean ± SD) | 117.0 ± 61.3 |
| Prothrombin time, PT (%) (mean ± SD) | 59.4 ± 15.3 |
| Prothrombin time-international normalized ratio, PT-INR (mean ± SD) | 1.36 ± 0.23 |
| Serum albumin concentration, Alb (g/dL) (mean ± SD) | 2.87 ± 0.57 |
| Total-bilirubin, T-bil (mg/dL) (mean ± SD) | 3.30 ± 0.45 |
| Blood urea nitrogen, BUN (mg/dL) (mean ± SD) | 16.3 ± 6.82 |
| Serum creatinine concentration, Cr (mg/dL) (mean ± SD) | 0.94 ± 0.69 |
| Estimated glomerular filtration rate, eGFR (mL/min/1.73 m2) (mean ± SD) | 69.6 ± 23.4 |
| Serum sodium concentration, Na (mEq/L) (mean ± SD) | 139.2 ± 3.04 |
| West-Haven grade | |
| Minimal or I | 50 (44.6%) |
| II | 38 (33.9%) |
| III | 22 (19.6%) |
| IV | 2 (1.8%) |
| HCC | |
| Presence | 40 (35.7%) |
| Absence | 72 (64.3%) |
| History of HCC treatment | |
| Presence | 42 (37.5%) |
| Absence | 70 (62.5%) |
| History of gastrointestinal variceal treatment | |
| Presence | 59 (52.7%) |
| Absence | 53 (47.3%) |
| Administration of diuretics | |
| Loop diuretics | 43 (38.4%) |
| Anti-aldosterone diuretics | 56 (50.0%) |
| Administration of NSBBs | 11 (9.8%) |
| Pretreatment Drug | Number of Patients |
|---|---|
| Oral BCAA preparations | 78 |
| Synthetic disaccharides | 47 |
| Intestinal regulators and laxatives | 38 |
| Carnitine preparations | 30 |
| Zinc preparations | 10 |
| Satisfactory Control n = 39 | Poor Control n = 42 | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| HR 95% CI | p-Value | HR 95% CI | p-Value | |||
| Sex | ||||||
| Male | 27 | 30 | ||||
| Female | 12 | 12 | 0.83 | |||
| Age | 66.8 ± 1.9 | 64.1 ± 1.8 | 0.32 | |||
| Etiology | ||||||
| Alcohol | 17 | 27 | ||||
| Not alcohol | 22 | 15 | 0.06 | 0.40 | ||
| CP score | 8.74 ± 0.30 | 9.90 ± 0.29 | 20.4 2.29–243 | <0.01 ** | 62.7 1.5–4526 | 0.028 * |
| MELD score | 11.7 ± 0.69 | 13.3 ± 0.68 | 0.10 | 0.92 | ||
| MELD sodium score | 12.1 ± 0.76 | 13.9 ± 0.74 | 0.10 | 0.83 | ||
| NH3 | 123 ± 9.9 | 124 ± 9.5 | 0.96 | |||
| Alb | 3.00 ± 0.08 | 2.85 ± 0.08 | 0.21 | |||
| T-bil | 2.07 ± 0.67 | 3.59 ± 0.65 | 0.11 | 0.98 | ||
| BUN | 15.8 ± 1.14 | 16.6 ± 1.11 | 0.65 | |||
| Cr | 0.91 ± 0.10 | 0.90 ± 0.10 | 0.93 | |||
| eGFR | 72.8 ± 3.48 | 66.9 ± 3.39 | 0.22 | |||
| OHE | ||||||
| Presence | 24 | 21 | ||||
| Absence | 15 | 21 | 0.29 | |||
| HCC | ||||||
| Presence | 16 | 12 | ||||
| Absence | 23 | 30 | 0.24 | |||
| History of EGV treatment | ||||||
| Presence | 18 | 26 | ||||
| Absence | 21 | 16 | 0.16 | 0.13 | ||
| Administration of anti-aldosterone diuretics | ||||||
| Presence | 15 | 22 | ||||
| Absence | 24 | 20 | 0.21 | |||
| Renin | 40.9 ± 18.5 | 127.9 ± 17.8 | 26.6 3.46–551 | <0.01 ** | 48.4 4.6–1483 | <0.01 ** |
| Aldosterone | 264.4 ± 89.8 | 307.2 ± 80.4 | 0.72 | |||
| Renin Levels | Satisfactory Control | Poor Control |
|---|---|---|
| Less than 41 pg/mL | 32 | 14 |
| 41 pg/mL or higher | 7 | 28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yokoyama, K.; Fukuda, H.; Yamauchi, R.; Higashi, M.; Miyayama, T.; Higashi, T.; Uchida, Y.; Shibata, K.; Tsuchiya, N.; Fukunaga, A.; et al. Long-Term Effects of Rifaximin on Patients with Hepatic Encephalopathy: Its Possible Effects on the Improvement in the Blood Ammonia Concentration Levels, Hepatic Spare Ability and Refractory Ascites. Medicina 2022, 58, 1276. https://doi.org/10.3390/medicina58091276
Yokoyama K, Fukuda H, Yamauchi R, Higashi M, Miyayama T, Higashi T, Uchida Y, Shibata K, Tsuchiya N, Fukunaga A, et al. Long-Term Effects of Rifaximin on Patients with Hepatic Encephalopathy: Its Possible Effects on the Improvement in the Blood Ammonia Concentration Levels, Hepatic Spare Ability and Refractory Ascites. Medicina. 2022; 58(9):1276. https://doi.org/10.3390/medicina58091276
Chicago/Turabian StyleYokoyama, Keiji, Hiromi Fukuda, Ryo Yamauchi, Masashi Higashi, Takashi Miyayama, Tomotaka Higashi, Yotaro Uchida, Kumiko Shibata, Naoaki Tsuchiya, Atsushi Fukunaga, and et al. 2022. "Long-Term Effects of Rifaximin on Patients with Hepatic Encephalopathy: Its Possible Effects on the Improvement in the Blood Ammonia Concentration Levels, Hepatic Spare Ability and Refractory Ascites" Medicina 58, no. 9: 1276. https://doi.org/10.3390/medicina58091276