

Strategies for Avoiding Typical Drug–Drug Interactions and Drug-Related Problems in Patients with Vascular Diseases
 ,
,
Abstract
1. Introduction
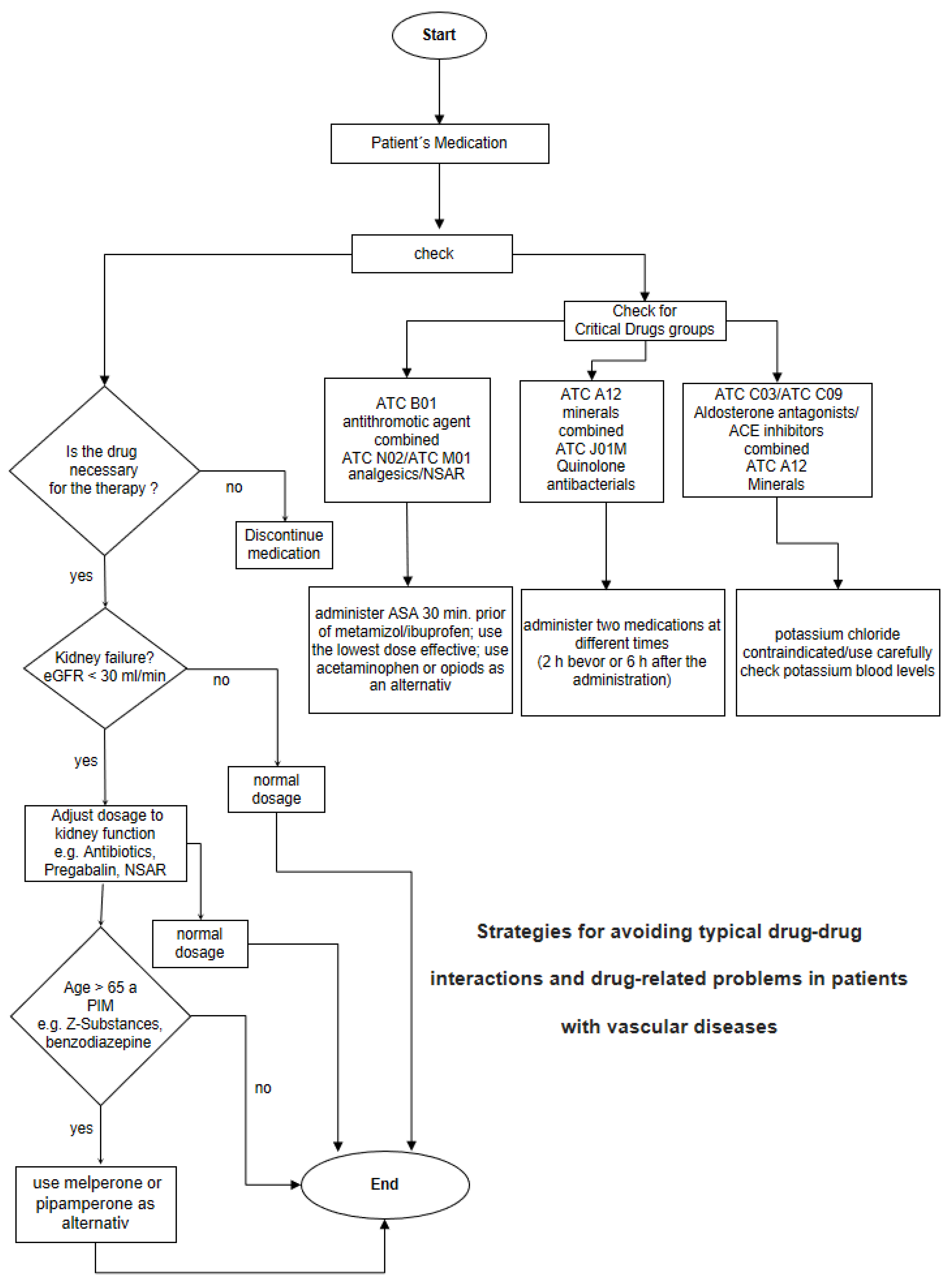
- Interactions;
- Dosing in patients with renal insufficiency, considering the current clearance, which was transferred from the Hospital Information System (HIS);
- Double medical prescriptions;
- Potentially inadequate medication for the elderly;
- Maximum dose.
Statistical Analysis
2. Results
2.1. Contraindicated/High-Risk Combinations
2.2. Clinically Serious Interactions
2.3. Potentially Clinically Relevant Moderate Risks
2.4. Interventions
3. Discussion
3.1. Contraindicated/High-Risk Combinations
3.2. Clinically Serious Interactions
3.3. Potential Clinically Relevant Moderate Risk
3.4. Notes for Medical Professionals
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olinic, D.M.; Spinu, M.; Olinic, M.; Homorodean, C.; Tataru, D.A.; Liew, A.; Schernthaner, G.H.; Stanek, A.; Fowkes, G.; Catalano, M. Epidemiology of peripheral artery disease in Europe: VAS Educational Paper. Int. Angiol. 2018, 37, 327–334. [Google Scholar] [CrossRef]
- Hohn, N.; Langer, S.; Kalder, J.; Jacobs, M.J.; Marx, G.; Eisert, A. Optimizing the pharmacotherapy of vascular surgery patients by medication reconciliation. J. Cardiovasc. Surg. 2014, 55, 175–181. [Google Scholar]
- Pharmaceutical Care Network Europe Association Classification for Drug Related Problems. Available online: https://www.pcne.org/upload/files/417_PCNE_classification_V9-1_final.pdf (accessed on 1 January 2020).
- Strand, L.M.; Morley, P.C.; Cipolle, R.J.; Ramsey, R.; Lamsam, G.D. Drug-related problems: Their structure and function. Dicp 1990, 24, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.F.; Yang, C.S.; Bai, Y.M.; Hu, Z.X.; Zhang, L.L. Drug-Related Problems of Patients in Primary Health Care Institutions: A Systematic Review. Front. Pharmacol. 2021, 12, 698907. [Google Scholar] [CrossRef]
- Schnurrer, J.U.; Frölich, J.C. Zur Häufigkeit und Vermeidbarkeit von tödlichen unerwünschten Arzneimittelwirkungen. Der Internist 2003, 44, 889–895. [Google Scholar] [CrossRef]
- American Geriatrics Society Beers Criteria® Update Expert Panel; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; et al. American Geriatrics Society 2019 Updated AGS Beers Criteria(R) for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Abolbashari, M.; Macaulay, T.E.; Whayne, T.F.; Mukherjee, D.; Saha, S. Polypharmacy in Cardiovascular Medicine: Problems and Promises! Cardiovasc. Hematol. Agents Med. Chem. 2017, 15, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Disdier Moulder, M.P.A.; Hendricks, A.K.; Ou, N.N. Towards appropriate polypharmacy in older cardiovascular patients: How many medications do I have to take? Clin. Cardiol. 2020, 43, 137–144. [Google Scholar] [CrossRef]
- WHO. International Language for Drug Utilization Research. Available online: https://www.whocc.no/ (accessed on 18 November 2021).
- van den Bemt, P.M.; Egberts, T.C.; de Jong-van den Berg, L.T.; Brouwers, J.R. Drug-related problems in hospitalised patients. Drug Saf. 2000, 22, 321–333. [Google Scholar] [CrossRef]
- Olakotan, O.; Mohd Yusof, M.; Ezat Wan Puteh, S. A Systematic Review on CDSS Alert Appropriateness. Stud. Health Technol. Inf. 2020, 270, 906–910. [Google Scholar] [CrossRef]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Elovic, A.; Pourmand, A. Lexicomp App Review. J. Digit. Imaging 2020, 33, 17–20. [Google Scholar] [CrossRef]
- Prescribing Information Inspra. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/021437s013lbl.pdf (accessed on 18 November 2021).
- Company, B.-M.S. Medication Guide Eliquis Apixaban. Available online: https://www.fda.gov/media/84985/download (accessed on 20 December 2021).
- Hartmann, B.C.; Czock, D.; Keller, F. Arzneimitteltherapie bei Patienten mit chronischem Nierenversagen. Dtsch. Ärzteblatt 2010, 37, 647–656. [Google Scholar]
- Davison, S.N.; Curhan, G.C. Management of Chronic Pain in Chronic Kidney Disease. Available online: https://www.uptodate.com/contents/management-of-chronic-pain-in-advanced-chronic-kidney-disease (accessed on 31 July 2021).
- Dixit, M.; Doan, T.; Kirschner, R.; Dixit, N. Significant Acute Kidney Injury Due to Non-steroidal Anti-inflammatory Drugs: Inpatient Setting. Pharmaceuticals 2010, 3, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, T.; Zimmermann, N.; Weber, A.A.; Jessen, G.; Weber, H.; Schror, K.; Holtje, H.D.; Ebel, R. Pyrazolinone analgesics prevent the antiplatelet effect of aspirin and preserve human platelet thromboxane synthesis. J. Thromb. Haemost. 2008, 6, 166–173. [Google Scholar] [CrossRef]
- Li, X.; Fries, S.; Li, R.; Lawson, J.A.; Propert, K.J.; Diamond, S.L.; Blair, I.A.; FitzGerald, G.A.; Grosser, T. Differential impairment of aspirin-dependent platelet cyclooxygenase acetylation by nonsteroidal antiinflammatory drugs. Proc. Natl. Acad. Sci. USA 2014, 111, 16830–16835. [Google Scholar] [CrossRef]
- Pfrepper, C.; Dietze, C.; Remane, Y.; Bertsche, T.; Schiek, S.; Kaiser, T.; Gockel, I.; Josten, C.; Petros, S. Intake of aspirin prior to metamizole does not completely prevent high on treatment platelet reactivity. Eur. J. Clin. Pharm. 2020, 76, 483–490. [Google Scholar] [CrossRef]
- Polzin, A.; Hohlfeld, T.; Kelm, M.; Zeus, T. Impairment of aspirin antiplatelet effects by non-opioid analgesic medication. World J. Cardiol. 2015, 7, 383–391. [Google Scholar] [CrossRef]
- Burnakis, T.G.; Mioduch, H.J. Combined therapy with captopril and potassium supplementation. A potential for hyperkalemia. Arch. Intern. Med. 1984, 144, 2371–2372. [Google Scholar] [CrossRef]
- MacDonald, T.M.; Wei, L. Effect of ibuprofen on cardioprotective effect of aspirin. Lancet 2003, 361, 573–574. [Google Scholar] [CrossRef]
- Catella-Lawson, F.; Reilly, M.P.; Kapoor, S.C.; Cucchiara, A.J.; DeMarco, S.; Tournier, B.; Vyas, S.N.; FitzGerald, G.A. Cyclooxygenase inhibitors and the antiplatelet effects of aspirin. N. Engl. J. Med. 2001, 345, 1809–1817. [Google Scholar] [CrossRef] [PubMed]
- Lehto, P.; Kivisto, K.T.; Neuvonen, P.J. The effect of ferrous sulphate on the absorption of norfloxacin, ciprofloxacin and ofloxacin. Br. J. Clin. Pharm. 1994, 37, 82–85. [Google Scholar] [CrossRef]
- Serebruany, V.L.; Glassman, A.H.; Malinin, A.I.; Atar, D.; Sane, D.C.; Oshrine, B.R.; Ferguson, J.J.; O’Connor, C.M. Selective serotonin reuptake inhibitors yield additional antiplatelet protection in patients with congestive heart failure treated with antecedent aspirin. Eur. J. Heart Fail. 2003, 5, 517–521. [Google Scholar] [CrossRef]
- Dalton, S.O.; Johansen, C.; Mellemkjaer, L.; Norgard, B.; Sorensen, H.T.; Olsen, J.H. Use of selective serotonin reuptake inhibitors and risk of upper gastrointestinal tract bleeding: A population-based cohort study. Arch. Intern. Med. 2003, 163, 59–64. [Google Scholar] [CrossRef]
- van Walraven, C.; Mamdani, M.M.; Wells, P.S.; Williams, J.I. Inhibition of serotonin reuptake by antidepressants and upper gastrointestinal bleeding in elderly patients: Retrospective cohort study. BMJ 2001, 323, 655–658. [Google Scholar] [CrossRef] [PubMed]
- de Abajo, F.J.; Rodriguez, L.A.; Montero, D. Association between selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: Population based case-control study. BMJ 1999, 319, 1106–1109. [Google Scholar] [CrossRef]
- Turner, M.S.; May, D.B.; Arthur, R.R.; Xiong, G.L. Clinical impact of selective serotonin reuptake inhibitors therapy with bleeding risks. J. Intern. Med. 2007, 261, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Dorian, P.; Roberts, R.S.; Gent, M.; Bailin, S.; Fain, E.S.; Thorpe, K.; Champagne, J.; Talajic, M.; Coutu, B.; et al. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: The OPTIC Study: A randomized trial. JAMA 2006, 295, 165–171. [Google Scholar] [CrossRef]
- Ohyama, K.; Nakajima, M.; Suzuki, M.; Shimada, N.; Yamazaki, H.; Yokoi, T. Inhibitory effects of amiodarone and its N-deethylated metabolite on human cytochrome P450 activities: Prediction of in vivo drug interactions. Br. J. Clin. Pharm. 2000, 49, 244–253. [Google Scholar] [CrossRef]
- Amsden, G.W.; Kuye, O.; Wei, G.C. A study of the interaction potential of azithromycin and clarithromycin with atorvastatin in healthy volunteers. J Clin Pharm. 2002, 42, 444–449. [Google Scholar] [CrossRef]
- Mesgarpour, B.; Gouya, G.; Herkner, H.; Reichardt, B.; Wolzt, M. A population-based analysis of the risk of drug interaction between clarithromycin and statins for hospitalisation or death. Lipids Health Dis. 2015, 14, 131. [Google Scholar] [CrossRef] [PubMed]
- Highlights of Prescribing Information Lipitor. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020702s056lbl.pdf (accessed on 10 October 2022).
- Sipe, B.E.; Jones, R.J.; Bokhart, G.H. Rhabdomyolysis causing AV blockade due to possible atorvastatin, esomeprazole, and clarithromycin interaction. Ann Pharm. 2003, 37, 808–811. [Google Scholar] [CrossRef]
- Marot, A.; Morelle, J.; Chouinard, V.A.; Jadoul, M.; Lambert, M.; Demoulin, N. Concomitant use of simvastatin and amiodarone resulting in severe rhabdomyolysis: A case report and review of the literature. Acta Clin. Belg. 2011, 66, 134–136. [Google Scholar]
- Ricaurte, B.; Guirguis, A.; Taylor, H.C.; Zabriskie, D. Simvastatin-amiodarone interaction resulting in rhabdomyolysis, azotemia, and possible hepatotoxicity. Ann. Pharm. 2006, 40, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Widmer, P.; Maibach, R.; Kunzi, U.P.; Capaul, R.; Mueller, U.; Galeazzi, R.; Hoigne, R. Diuretic-related hypokalaemia: The role of diuretics, potassium supplements, glucocorticoids and beta 2-adrenoceptor agonists. Results from the comprehensive hospital drug monitoring programme, berne (CHDM). Eur. J. Clin. Pharm. 1995, 49, 31–36. [Google Scholar] [CrossRef]
- Park, C.G.; Lee, H.; Choi, J.W.; Lee, S.J.; Kim, S.H.; Lim, H.E. Non-concurrent dosing attenuates the pharmacokinetic interaction between amlodipine and simvastatin. Int. J. Clin. Pharm. Ther. 2010, 48, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Klinenberg, J.R.; Miller, F. Effect of corticosteroids on blood salicylate concentration. JAMA 1965, 194, 601–604. [Google Scholar] [CrossRef]
- Singh, N.; Singh, P.N.; Hershman, J.M. Effect of calcium carbonate on the absorption of levothyroxine. JAMA 2000, 283, 2822–2825. [Google Scholar] [CrossRef]
- Zamfirescu, I.; Carlson, H.E. Absorption of levothyroxine when coadministered with various calcium formulations. Thyroid 2011, 21, 483–486. [Google Scholar] [CrossRef]
- FDA. FDA Drug Safety Communication: FDA Warns about Serious Risks and Death When Combining Opioid Pain or Cough Medicines with Benzodiazepines; Requires Its Strongest Warning. Available online: http://www.fda.gov/Drugs/DrugSafety/ucm518473.htm (accessed on 16 December 2021).
- Mekonnen, A.B.; McLachlan, A.J.; Brien, J.A. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: A systematic review and meta-analysis. BMJ Open 2016, 6, e010003. [Google Scholar] [CrossRef]
- Spinewine, A.; Fialova, D.; Byrne, S. The role of the pharmacist in optimizing pharmacotherapy in older people. Drugs Aging 2012, 29, 495–510. [Google Scholar] [CrossRef] [PubMed]
- Lovely, J.K.; Hyland, S.J.; Smith, A.N.; Nelson, G.; Ljungqvist, O.; Parrish, R.H., 2nd. Clinical pharmacist perspectives for optimizing pharmacotherapy within Enhanced Recovery after Surgery (ERAS((R))) programs. Int. J. Surg. 2019, 63, 58–62. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n = 96 (IQR) |
|---|---|
| Gender | |
| Male | 66 (68.8%) |
| Age (years) mean | 73.6 (12.43) |
| Age range | 48–97 |
| Smoker | 18 (18.8%) |
| Former Smoker | 13 (13.5%) |
| Number of DRPs (total) | 277 |
| Interactions | 111 (2) |
| Interventions | 114 (7) |
| Notes for ward doctors | 96 |
| Kidney failure stage 5: eGFR 5 < 15 mL/min | 4 (4.1%) |
| Kidney failure stage 4: eGFR15–29 mL/min | 8 (8.3%) |
| Kidney failure stage 3: eGFR 30–59 mL/min | 30 (31.2%) |
| Kidney failure stage 2: eGFR 60–89 mL/min | 37 (38.5%) |
| Normal kidney function: eGFR > 90 mL/min | 17 (17.7%) |
| Number of medications | 10.5 (4) |
| Polypharmacy > 5 medications | 92 (95.8%) |
| Main indications of hospitalization (ICD-10): | |
| Atherosclerosis of the extremity arteries (I70) | 49 (51%) |
| Embolism and thrombosis of the arteries of the lower extremities (I74) | 10 (10.4%) |
| Diabetes mellitus, Type 2 (E11) | 10 (9.4%) |
| Aortic aneurysm and dissection (I71) | 7 (7.3%) |
| Complications due to prostheses, implants, or grafts in the heart and vessels (T82) | 5 (5.2%) |
| Complications indicative of replantation and amputation (T87) | 4 (4.2%) |
| Other aneurysm and other dissection (I72) | 3 (3.2%) |
| Chronic ischemic heart disease (I25) | 2 (2.1%) |
| Skin abscess, boil, and carbuncles (L02) | 2 (2.1%) |
| Occlusion and stenosis of precerebral arteries without resulting cerebral infarction (I65) | 1 (1.0%) |
| Varices of the lower extremities (I83) | 1 (1.0%) |
| Complications of surgery, not elsewhere classified (T81) | 1 (1.0%) |
| Secondary diagnosis: | |
| Hypertension | 66 (68.8%) |
| Type 1 diabetes | 2 (2.1%) |
| Type 2 diabetes | 50 (52.1%) |
| Peripheral arterial occlusive disease | 43 (44.8%) |
| Cardiac arrhythmia | 26 (27.1%) |
| Renal insufficiency/failure | 26 (27.1%) |
| Hyperlipidemia | 23 (24.0%) |
| Coronary artery disease | 22 (22.9%) |
| Cancer | 18 (18.7%) |
| Pneumonia | 12 (12.5%) |
| COPD | 12 (12.5%) |
| Aneurysm | 9 (9.3%) |
| Heart attack | 8 (8.3%) |
| Heart failure | 8 (8.3%) |
| Anemia | 8 (8.3%) |
| Valvular heart disease | 6 (6.3%) |
| Hypercholesterolemia | 6 (6.3%) |
| Affective disorder | 6 (6.3%) |
| Hypothyroidism | 5 (5.2%) |
| Thrombosis | 4 (4.2%) |
| Gastrointestinal disorders | 4 (4.2%) |
| Embolism | 3 (3.1%) |
| Delirium | 3 (3.1%) |
| Liver disease/insufficiency | 3 (3.1%) |
| TIA | 3 (3.1%) |
| ICD implant | 3 (3.1%) |
| Type 1 diabetes | 2 (2.1%) |
| Coronary artery bypass | 2 (2.1%) |
| Hyperthyroidism | 1 (1%) |
| Blood clotting disorder | 1 (1%) |
| Abdominal surgery | 1 (1%) |
| Aortic valve repair/replacement | 1 (1%) |
| Drug Combinations Involved in Contraindicated/High-Risk Combinations | n | Consequences of This Combination |
|---|---|---|
| eplerenone C03DA04/potassium chloride A12BA01 | 4 | contraindication ➔ discontinuation of potassium chloride |
| apixaban B01AF02/enoxaparin B01AB05 | 1 | contraindication ➔ discontinuation of enoxaparin |
| rivaroxaban B01AX06/enoxaparin B01AB05 | 1 | contraindication ➔ discontinuation of enoxaparin |
| Total | 6 | |
| Drug combinations involved in clinically serious interactions: | ||
| acetylsalicylic acid (ASA) B01AC06/metamizole-natrium N02BB02 | 24 | administer ASA 30 min. prior to metamizole; use the lowest dose effective; use acetaminophen or opioids as an alternative |
| ramipril C09AA05/potassium chloride A12BA01 | 4 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| spironolactone C03DA01/potassium chloride A12BA01 | 3 | increased risk of toxic potassium blood levels;use carefully, check potassium blood levels |
| ASA B01AC06/ibuprofen M01AE01 | 3 | administer ASA 30 min. prior to ibuprofen |
| ciprofloxacin J01MA02/iron (II) glycine sulphate complex B03AA01 | 2 | administer ciprofloxacin 2 h before or 6 h after the iron (II) glycine sulphate complex |
| venlafaxine N06AX16/ASA B01AC06 | 2 | increased risk of gastrointestinal bleeding |
| citalopram N06AB04/ASA B01AC06 | 3 | increased risk of gastrointestinal bleeding |
| potassium chloride A12BA01/lisinopril C09AA03 | 2 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| acarbose A10BF01/glimepiride A10BB12 | 1 | risk of hypoglycemia |
| amiodaron C01BD01/metoprolol C07AB02 | 1 | use carefully under ECG controls |
| atorvastatin C10AA05/valsartan and sacubitril C09DX04 | 1 | increased risk of myopathy and/or rhabdomyolysis use carefully; pay attention to symptoms |
| atorvastatin C10AA05/amiodaron C01BD01 | 2 | inhibitor of the cyto chrome P450 3A4; increased risk of myopathy and/or rhabdomyolysis; pay attention to symptoms |
| atorvastatin C10AA05/clarithromycin J01FA09 | 1 | inhibitor of the cyto chrome P450 3A4; increased risk of myopathy and/or rhabdomyolysis; pay attention to symptoms |
| bisoprolol C07AB07/amiodaron C01BD01 | 1 | use carefully under ECG controls |
| ciprofloxacin J01MA02/citalopram N06AB04 | 1 | use carefully under ECG controls; check potassium blood levels |
| clarithromycin J01FA09/atorvastatin C10AA05 | 1 | increased risk of myopathy and/or rhabdomyolysis; pay attention to symptoms |
| digitoxin C01AA04/torasemide C03CA04 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| duloxetine N06AX21/rivaroxaban B01AX06 | 1 | increased risk of gastrointestinal bleeding; monitor therapy; agents with antiplatelet properties may enhance the anticoagulant effect of rivaroxaban |
| enoxaparin B01AB05/escitalopram N06AB10 | 1 | increased risk of gastrointestinal bleeding |
| eplerenone C03DA04/ramipril C09AA05 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| ibuprofen M01AE01/torasemide C03CA04 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| ibuprofen M01AE01/candesartan and hydrochlorothiazide C09DA26 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| ibuprofen M01AE01/hydrochlorothiazide C03AA03 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| ibuprofen M01AE01/valsartan and amlodipine C09DB01 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| lisinopril and diuretics C09BA03/potassium chloride A12BA01 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| melperone N05AD03/citalopram N06AB04 | 1 | use carefully under ECG controls; check potassium blood levels |
| paroxetine N06AB05/ASA B01AC06 | 1 | increased risk of gastrointestinal bleeding |
| prednisolone H02AB06/hydrochlorothiazide C03AA03 | 1 | increased risk of toxic potassium blood levels; check potassium blood levels |
| ramipril C09AA05/eplerenone C03DA04 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| ramipril and diuretics C09BA05/potassium chloride A12BA01 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| ramipril and diuretics C09BA05/ibuprofen M01AE01 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| sertraline N06AB06/ASA B01AC06 | 2 | increased risk of gastrointestinal bleeding; monitor therapy; agents with antiplatelet properties may enhance the anticoagulant effect of ASA |
| spironolactone C03DA01/ciprofloxacin J01MA02 | 1 | increased risk of toxic potassium blood levels;use carefully, check potassium blood levels |
| valsartan and diuretics C09DA03/ibuprofen M01AE01 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| azithromycin J01FA10/moxifloxacin J01MA14 | 1 | use carefully under ECG controls; check potassium blood levels |
| valsartan and sacubitril C09DX04/potassium chloride A12BA01 | 1 | increased risk of toxic potassium blood levels; use carefully, check potassium blood levels |
| fentanyl N02AB03/clarithromycin J01FA09 | 1 | CYP3A4 inhibitors (strong) may increase the serum concentration of fentanyl, monitoring of opioid side effects (coma, respiratory depression) |
| levodopa in combination with benserazide N04BA11/melperone N05AD03 | 1 | efficacy of levodopa to be verified in the short term |
| magnesium aspartate A12CC05/levothyroxine-natrium H03AA01 | 1 | magnesium should be taken no earlier than 2 h after taking levothyroxine |
| ibuprofen M01AE01/furosemide C03CA01 | 1 | monitoring of diuresis in the first days after starting and stopping NSAIDs |
| Total: | 81 | |
| Drug combinations involved in potential clinically relevant moderate risk combinations: | ||
| prednisolone H02AB06/hydrochlorothiazide C03AA03 | 3 | corticosteroids (systemic) may enhance the hypokalemic effect of thiazide and thiazide-like diuretics; check potassium blood levels |
| prednisolone H02AB06/torasemide C03CA04 | 4 | corticosteroids (systemic) may enhance the hypokalemic effect of loop diuretics; check potassium blood levels |
| prednisolone H02AB06/ASA B01AC06 | 3 | ASA may enhance the adverse/toxic effect of corticosteroids; increased risk of gastrointestinal bleeding |
| amlodipine C08CA01/simvastatin C10AA01 | 2 | inhibitor of the cyto chrome P450 3A4; increased risk of myopathy and/or rhabdomyolysis; pay attention to symptoms |
| levothyroxine-natrium H03AA01/calcium, combinations with vitamin D and/or other drugs A12AX | 2 | amlodipine may increase the serum concentration of simvastatin; increased risk for myopathy and/or rhabdomyolysis; pay attention to symptoms |
| oxycodone N02AA05/pregabalin N03AX16 | 2 | CNS depressants may enhance the CNS depressant effect of oxycodone |
| ASA B01AC06/ verapamil C08DA01 | 1 | increased risk of gastrointestinal bleeding; calcium channel blockers may enhance the antiplatelet effect of ASA |
| enoxaparin B01AB05/clopidogrel B01AC04 | 1 | agents with antiplatelet properties may enhance the anticoagulant effect of enoxaparin; monitor closely for symptoms of bleeding |
| metoprolol C07AB02/amlodipine C08CA01 | 1 | check blood pressure regularly and watch for signs of heart failure |
| levodopa, decarboxylase inhibitor and COMT inhibitor N04BA03/iron (II) glycine sulfate complex B03AA01 | 1 | iron preparations may decrease the serum concentration of levodopa; separating doses of the agents by 2 or more hours |
| metamizole-natrium N02BB02/clopidogrel B01AC04 | 1 | may enhance the antiplatelet effect of other agents with antiplatelet properties |
| metoprolol C07AB02/digitoxin C01AA04 | 1 | bradycardia-causing agents may enhance the bradycardic effect of other bradycardia-causing agents; monitor heart rate and blood pressure more closely |
| calcium carbonate A12AA04/ciprofloxacin J01MA02 | 1 | iron preparations may decrease the serum concentration of levodopa; separating doses of the agents by 2 or more hours |
| ramipril and diuretics C09BA05/clopidogrel B01AC04 | 1 | thiazide diuretics may decrease the excretion of calcium; monitor for toxic effects of calcium if a thiazide diuretic is initiated or the dose is increased |
| Total: | 24 |
| Intervention | n | % |
|---|---|---|
| Apply another drug | 13 | 11.4% |
| Discontinue the drug | 41 | 36.0% |
| Dose reduction/adjustment | 40 | 35.1% |
| Apply medication | 8 | 7.0% |
| Handwritten errors | 12 | 10.5% |
| Total | 114 | 100% |
| Notes for Medical Professionals | n | % |
|---|---|---|
| Monitor laboratory values | 49 | 51.0% |
| Monitor side effects | 17 | 17.7% |
| Potentially inappropriate medications | 18 | 18.8% |
| Application time | 4 | 4.2% |
| Manual transmission errors | 8 | 8.3% |
| Total | 96 | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmelzer, K.P.; Liebetrau, D.; Kämmerer, W.; Meisinger, C.; Hyhlik-Dürr, A. Strategies for Avoiding Typical Drug–Drug Interactions and Drug-Related Problems in Patients with Vascular Diseases. Medicina 2023, 59, 780. https://doi.org/10.3390/medicina59040780
Schmelzer KP, Liebetrau D, Kämmerer W, Meisinger C, Hyhlik-Dürr A. Strategies for Avoiding Typical Drug–Drug Interactions and Drug-Related Problems in Patients with Vascular Diseases. Medicina. 2023; 59(4):780. https://doi.org/10.3390/medicina59040780
Chicago/Turabian StyleSchmelzer, Klaus Peter, Dominik Liebetrau, Wolfgang Kämmerer, Christine Meisinger, and Alexander Hyhlik-Dürr. 2023. "Strategies for Avoiding Typical Drug–Drug Interactions and Drug-Related Problems in Patients with Vascular Diseases" Medicina 59, no. 4: 780. https://doi.org/10.3390/medicina59040780
APA StyleSchmelzer, K. P., Liebetrau, D., Kämmerer, W., Meisinger, C., & Hyhlik-Dürr, A. (2023). Strategies for Avoiding Typical Drug–Drug Interactions and Drug-Related Problems in Patients with Vascular Diseases. Medicina, 59(4), 780. https://doi.org/10.3390/medicina59040780