
The Impact of Pneumococcal Conjugate Vaccine (PCV) Coverage Heterogeneities on the Changing Epidemiology of Invasive Pneumococcal Disease in Switzerland, 2005–2019

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Case Definition and Regional Assignment
2.3. Statistical Analyses
3. Results
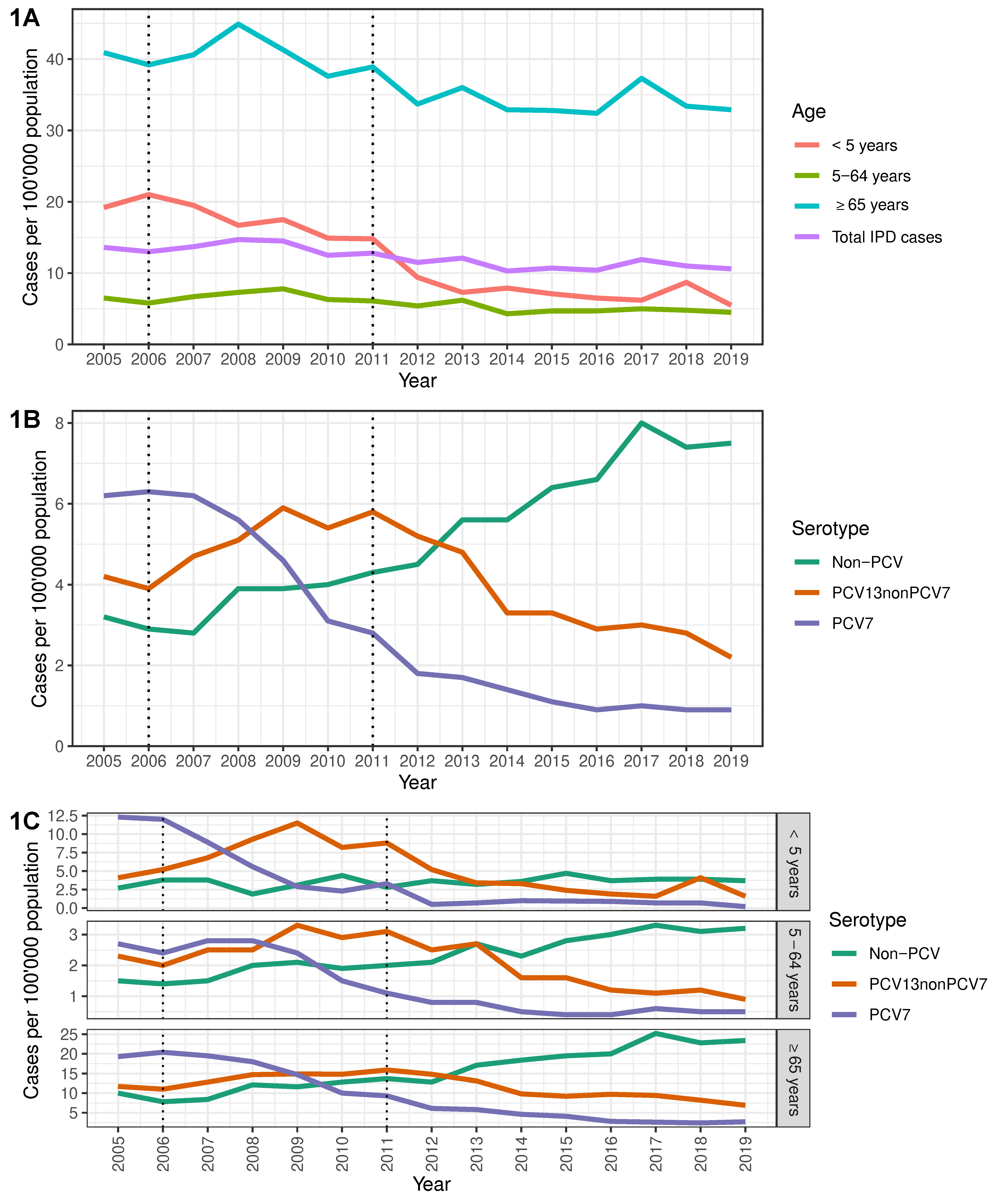
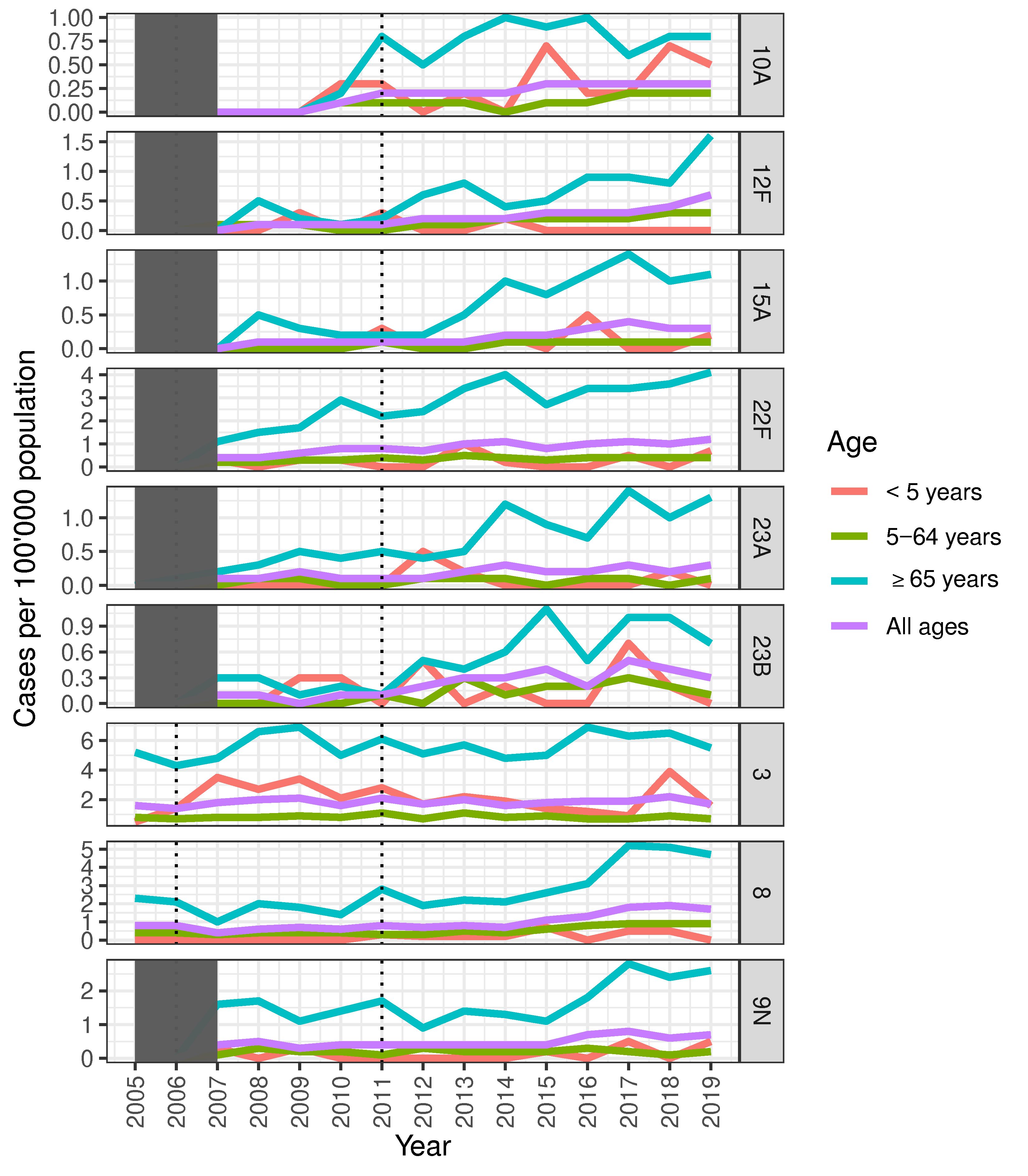
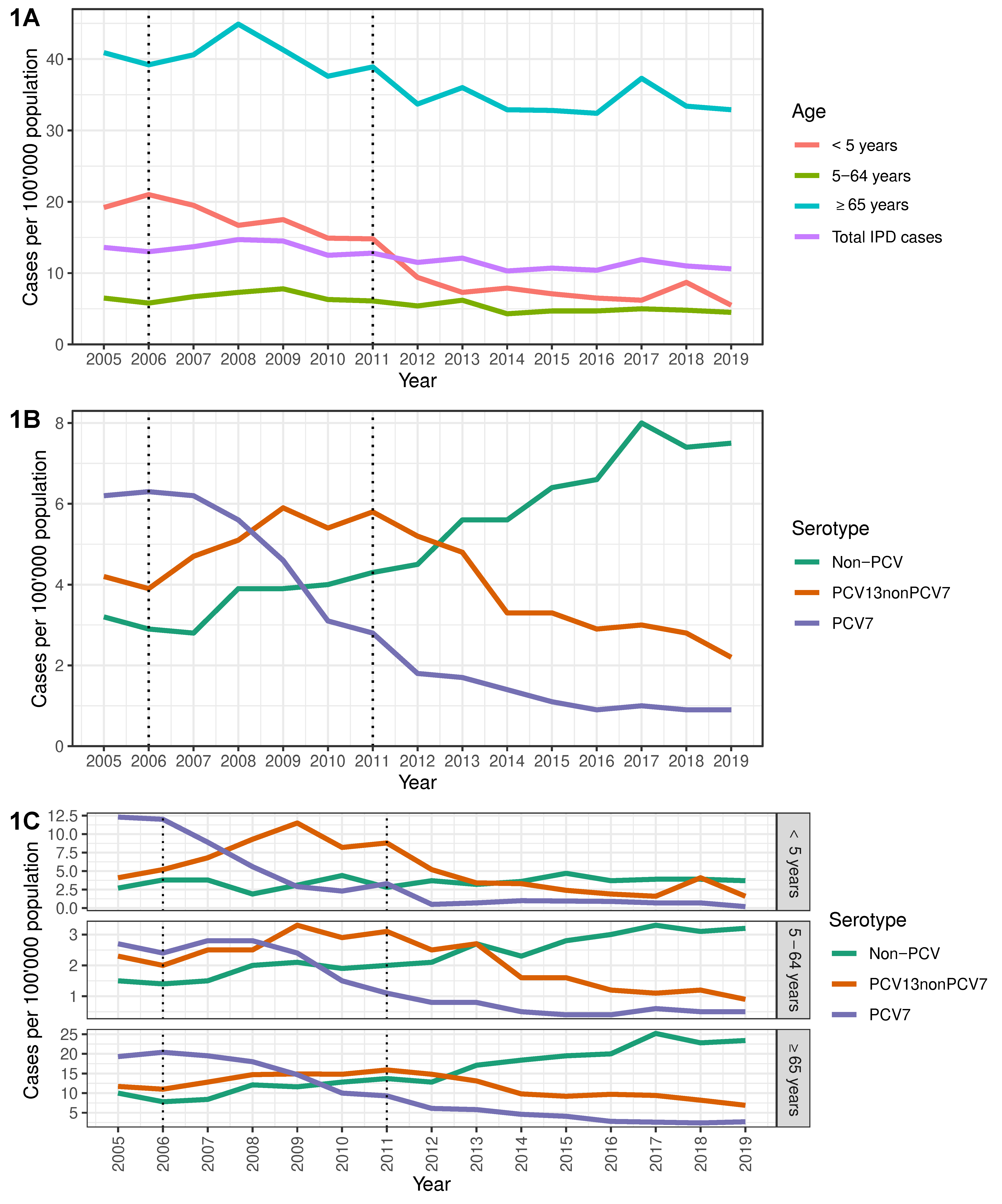
3.1. Characteristics of IPD from 2005–2019
3.2. Overall Impact of PCV on IPD Incidence and Serotype Distribution in Switzerland
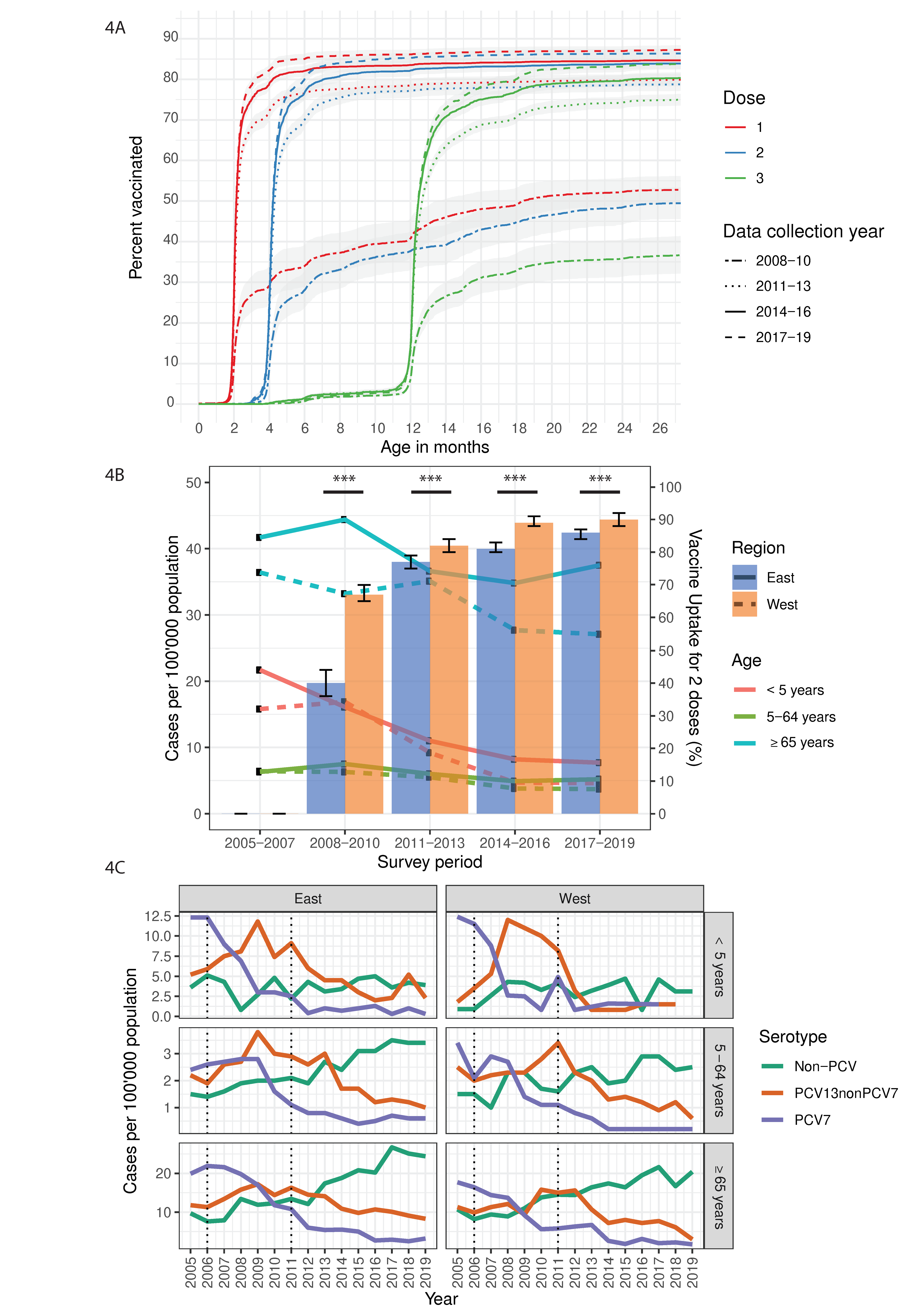
3.3. Overall Impact of PCV on IPD Incidence in Eastern and Western Switzerland
3.4. Pneumococcal Vaccine Coverage in National and Regional Switzerland
3.5. Indirect and Overall Impact of PCV Coverage on IPD Incidence in Age Group Populations in the East and West
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Pneumococcal conjugate vaccine for childhood immunization—WHO position paper. Wkly. Epidemiol. Rec. 2007, 82, 93–104. [Google Scholar]
- Ciruela, P.; Izquierdo, C.; Broner, S.; Muñoz-Almagro, C.; Hernández, S.; Ardanuy, C.; Pallarés, R.; Domínguez, A.; Jané, M.; Esteva, C.; et al. The changing epidemiology of invasive pneumococcal disease after PCV13 vaccination in a country with intermediate vaccination coverage. Vaccine 2018, 36, 7744–7752. [Google Scholar] [CrossRef] [PubMed]
- Hays, C.; Vermee, Q.; Agathine, A.; Dupuis, A.; Varon, E.; Poyart, C.; Ploy, M.-C.; Raymond, J. Demonstration of the herd effect in adults after the implementation of pneumococcal vaccination with PCV13 in children. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 36, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Bundesamt für Gesundheit; Eidgenössische Kommission für Impffragen. Empfehlungen zur Pneumokokkenimpfung bei Kindern unter 5 Jahren. Richtlinien und Empfehlungen (ehemals Supplementum XVII); Bundesamt für Gesundheit: Liebefeld, Switzerland, 2007; pp. 1–16.
- Bundesamt für Gesundheit; Eidgenössische Kommission für Impffragen. Empfehlungen zur Pneumokokkenimpfung bei Kindern unter 5 Jahren: Wechsel vom 7- zum 13-valenten konjugierten Impfstoff. Bull. BAG 2010, 51, 1202–1205. [Google Scholar]
- Jackson, L.A.; Gurtman, A.; Van Cleeff, M.; Jansen, K.U.; Jayawardene, D.; Devlin, C.; Scott, D.A.; Emini, E.A.; Gruber, W.C.; Schmoele-Thoma, B. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine compared to a 23-valent pneumococcal polysaccharide vaccine in pneumococcal vaccine-naive adults. Vaccine 2013, 31, 3577–3584. [Google Scholar] [CrossRef] [Green Version]
- Jackson, L.A.; Gurtman, A.; Rice, K.; Pauksens, K.; Greenberg, R.N.; Jones, T.R.; Scott, D.A.; Emini, E.A.; Gruber, W.C.; Schmoele-Thoma, B. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine in adults 70 years of age and older previously vaccinated with 23-valent pneumococcal polysaccharide vaccine. Vaccine 2013, 31, 3585–3593. [Google Scholar] [CrossRef] [Green Version]
- Harboe, Z.B.; Dalby, T.; Weinberger, D.M.; Benfield, T.; Mølbak, K.; Slotved, H.C.; Suppli, C.H.; Konradsen, H.B.; Valentiner-Branth, P. Impact of 13-Valent Pneumococcal Conjugate Vaccination in Invasive Pneumococcal Disease Incidence and Mortality. Clin. Infect. Dis. 2014, 59, 1066–1073. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, G.A.; Hill, P.C.; Jeffries, D.J.; Hossain, I.; Uchendu, U.; Ameh, D.; Ndiaye, M.; Adeyemi, O.; Pathirana, J.; Olatunji, Y.; et al. Effect of the introduction of pneumococcal conjugate vaccination on invasive pneumococcal disease in The Gambia: A population-based surveillance study. Lancet Infect. Dis. 2016, 16, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Rudnick, W.; Liu, Z.; Shigayeva, A.; Low, D.E.; Green, K.; Plevneshi, A.; Devlin, R.; Downey, J.; Katz, K.; Kitai, I.; et al. Pneumococcal vaccination programs and the burden of invasive pneumococcal disease in Ontario, Canada, 1995–2011. Vaccine 2013, 31, 5863–5871. [Google Scholar] [CrossRef] [PubMed]
- Hauser, C.; Kronenberg, A.; Allemann, A.; Mühlemann, K.; Hilty, M. Serotype/serogroup-specific antibiotic non-susceptibility of invasive and non-invasive Streptococcus pneumoniae, Switzerland, 2004 to 2014. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Achermann, R.; Suter, K.; Kronenberg, A.; Gyger, P.; Mühlemann, K.; Zimmerli, W.; Bucher, H. Antibiotic use in adult outpatients in Switzerland in relation to regions, seasonality and point of care tests. Clin. Microbiol. Infect. 2011, 17, 855–861. [Google Scholar] [CrossRef] [Green Version]
- Riesen, M.; Konstantinoudis, G.; Lang, P.; Low, N.; Hatz, C.; Maeusezahl, M.; Spaar, A.; Bühlmann, M.; Spycher, B.D.; Althaus, C.L. Exploring variation in human papillomavirus vaccination uptake in Switzerland: A multilevel spatial analysis of a national vaccination coverage survey. BMJ Open 2018, 8, e021006. [Google Scholar] [CrossRef] [Green Version]
- Olearo, F.; Albrich, W.C.; Vernaz, N.; Harbarth, S.; Kronenberg, A. Staphylococcus aureus and methicillin resistance in Switzerland: Regional differences and trends from 2004 to 2014. Swiss Med. Wkly. 2016, 146. [Google Scholar] [CrossRef] [Green Version]
- Meichtry, J.; Born, R.; Küffer, M.; Zwahlen, M.; Albrich, W.C.; Brugger, S.D.; Mühlemann, K.; Hilty, M. Serotype epidemiology of invasive pneumococcal disease in Swiss adults: A nationwide population-based study. Vaccine 2014, 32, 5185–5191. [Google Scholar] [CrossRef] [Green Version]
- Lang, P.; Zimmermann, H.; Piller, U.; Steffen, R.; Hatz, C. The Swiss National Vaccination Coverage Survey, 2005–2007. Public Health Rep. 2011, 126, 97–108. [Google Scholar] [CrossRef] [Green Version]
- Naucler, P.; Galanis, I.; Morfeldt, E.; Darenberg, J.; Örtqvist, Å.; Henriques-Normark, B. Comparison of the Impact of Pneumococcal Conjugate Vaccine 10 or Pneumococcal Conjugate Vaccine 13 on Invasive Pneumococcal Disease in Equivalent Populations. Clin. Infect. Dis. 2017, 65, 1780–1790.e1. [Google Scholar] [CrossRef] [Green Version]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–2017: A prospective national observational cohort study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Ouldali, N.; Varon, E.; Levy, C.; Angoulvant, F.; Georges, S.; Ploy, M.-C.; Kempf, M.; Cremniter, J.; Cohen, R.; Bruhl, D.L.; et al. Invasive pneumococcal disease incidence in children and adults in France during the pneumococcal conjugate vaccine era: An interrupted time-series analysis of data from a 17-year national prospective surveillance study. Lancet Infect. Dis. 2021, 21, 137–147. [Google Scholar] [CrossRef]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Lexau, C.; Bennett, N.M.; Petit, S.; Zansky, S.M.; Harrison, L.H.; Reingold, A.; et al. Effect of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: Analysis of multisite, population-based surveillance. Lancet Infect. Dis. 2015, 15, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Lewnard, J.A.; Hanage, W.P. Making sense of differences in pneumococcal serotype replacement. Lancet Infect. Dis. 2019, 19, e213–e220. [Google Scholar] [CrossRef]
- Southern, J.; Andrews, N.; Sandu, P.; Sheppard, C.L.; Waight, P.A.; Fry, N.K.; Van Hoek, A.J.; Miller, E. Pneumococcal carriage in children and their household contacts six years after introduction of the 13-valent pneumococcal conjugate vaccine in England. PLoS ONE 2018, 13, e0195799. [Google Scholar] [CrossRef] [PubMed]
- Fjeldhøj, S.; Laursen, R.P.; Larnkjær, A.; Mølgaard, C.; Fuursted, K.; Krogfelt, K.A.; Slotved, H.-C. Probiotics and carriage of Streptococcus pneumoniae serotypes in Danish children, a double-blind randomized controlled trial. Sci. Rep. 2018, 8, 15258. [Google Scholar] [CrossRef]
- Lindstrand, A.; Galanis, I.; Darenberg, J.; Morfeldt, E.; Naucler, P.; Blennow, M.; Alfvén, T.; Henriques-Normark, B.; Örtqvist, Å. Unaltered pneumococcal carriage prevalence due to expansion of non-vaccine types of low invasive potential 8 years after vaccine introduction in Stockholm, Sweden. Vaccine 2016, 34, 4565–4571. [Google Scholar] [CrossRef] [Green Version]
- Vissers, M.; Wijmenga-Monsuur, A.J.; Knol, M.J.; Badoux, P.; Van Houten, M.A.; Van Der Ende, A.; Sanders, E.A.M.; Rots, N.Y. Increased carriage of non-vaccine serotypes with low invasive disease potential four years after switching to the 10-valent pneumococcal conjugate vaccine in The Netherlands. PLoS ONE 2018, 13, e0194823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galanis, I.; Lindstrand, A.; Darenberg, J.; Browall, S.; Nannapaneni, P.; Sjöström, K.; Morfeldt, E.; Naucler, P.; Blennow, M.; Örtqvist, Å.; et al. Effects of PCV7 and PCV13 on invasive pneumococcal disease and carriage in Stockholm, Sweden. Eur. Respir. J. 2016, 47, 1208–1218. [Google Scholar] [CrossRef]
- Horácio, A.N.; Silva-Costa, C.; Diamantino-Miranda, J.; Lopes, J.P.; Ramirez, M.; Melo-Cristino, J. Portuguese Group for the Study of Streptococcal Infections Population Structure of Streptococcus pneumoniae Causing Invasive Disease in Adults in Portugal before PCV13 Availability for Adults: 2008–2011. PLoS ONE 2016, 11, e0153602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azarian, T.; Mitchell, P.K.; Georgieva, M.; Thompson, C.M.; Ghouila, A.; Pollard, A.J.; Von Gottberg, A.; Du Plessis, M.; Antonio, M.; Kwambana-Adams, B.A.; et al. Global emergence and population dynamics of divergent serotype 3 CC180 pneumococci. PLoS Pathog. 2018, 14, e1007438. [Google Scholar] [CrossRef] [Green Version]
- Asner, S.A.; Agyeman, P.K.A.; Gradoux, E.; Posfay-Barbe, K.M.; Heininger, U.; Giannoni, E.; Crisinel, P.A.; Stocker, M.; Bernhard-Stirnemann, S.; Niederer-Loher, A.; et al. Burden of Streptococcus pneumoniae Sepsis in Children After Introduction of Pneumococcal Conjugate Vaccines: A Prospective Population-based Cohort Study. Clin. Infect. Dis. 2019, 69, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Reinau, D.; Schur, N.; Blozik, E.; Früh, M.; Signorell, A.; Heininger, U.; Schwenkglenks, M.; Meier, C.R. Coverage rates and timeliness of nationally recommended vaccinations in Swiss preschool children: A descriptive analysis using claims data. Vaccine 2020, 38, 1551–1558. [Google Scholar] [CrossRef]
- Hausdorff, W.P.; Siber, G.; Paradiso, P.R. Geographical differences in invasive pneumococcal disease rates and serotype frequency in young children. Lancet 2001, 357, 950–952. [Google Scholar] [CrossRef]
- Kronenberg, A.; Zucs, P.; Droz, S.; Mühlemann, K. Distribution and Invasiveness of Streptococcus pneumoniae Serotypes in Switzerland, a Country with Low Antibiotic Selection Pressure, from 2001 to 2004. J. Clin. Microbiol. 2006, 44, 2032–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Early PCV7 era Incidence a (2005–2007) | Late PCV7 era Incidence a (2008–2010) | Early PCV13 era Incidence a (2011–2013) | Mid PCV13 era Incidence a (2014–2016) | Late PCV13 era Incidence a (2017–2019) | Late PCV7 vs. Early PCV7 IRR b (95% CI) | Early PCV13 vs. Late PCV7 IRR b (95% CI) | Mid PCV13 vs. Early PCV13 IRR b (95% CI) | Late PCV13 vs. Mid PCV13 IRR b (95% CI) | Late PCV13 vs. Early PCV7 IRR b (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|---|
| <5 years | n = 219 | n = 188 | n = 127 | n = 91 | n = 89 | |||||
| PCV7 | 11.1 (9.2–13.2) | 3.6 (2.6–4.8) | 1.5 (0.9–2.3) | 0.6 (0.3–1.2) | 0.5 (0.2–1.1) | 0.32 (0.23–0.46) | 0.42 (0.24–0.72) | 0.42 (0.19–0.98) | 0.85 (0.31–2.34) | 0.05 (0.02–0.10) |
| PCV13nonPCV7 | 5.4 (4.1–6.9) | 9.7 (8.0–11.6) | 5.8 (4.5–7.3) | 2.5 (1.7–3.6) | 2.4 (1.7–3.5) | 1.80 (1.31–2.47) | 0.60 (0.44–0.80) | 0.44 (0.29–0.66) | 0.97 (0.60–1.59) | 0.46 (0.30–0.70) |
| Non-PCV | 3.5 (2.4–4.7) | 3.1 (2.2–4.3) | 3.2 (2.3–4.4) | 4.0 (3.0–5.3) | 3.8 (2.8–5.0) | 0.91 (0.58–1.43) | 1.02 (0.65–1.61) | 1.25 (0.82–1.90) | 0.95 (0.65–1.41) | 1.11 (0.73–1.69) |
| Total cases | 19.9 (17.4–22.7) | 16.4 (14.1–18.9) | 10.5 (8.7–12.4) | 7.2 (5.8–8.8) | 6.8 (5.5–8.4) | 0.82 (0.68–1.0) | 0.64 (0.51–0.80) | 0.68 (0.52–0.90) | 0.95 (0.71–1.27) | 0.34 (0.27–0.44) |
| 5–64 years | n = 1129 | n = 1308 | n = 1103 | n = 879 | n = 936 | |||||
| PCV7 | 2.6 (2.4–2.9) | 2.2 (2.0–2.5) | 0.9 (0.8–1.0) | 0.4 (0.3–0.5) | 0.5 (0.4–0.6) | 0.84 (0.74–0.96) | 0.40 (0.34–0.48) | 0.47 (0.36–0.61) | 1.23 (0.91–1.65) | 0.19 (0.16–0.24) |
| PCV13nonPCV7 | 2.2 (2.0–2.5) | 2.9 (2.7–3.2) | 2.8 (2.5–3.0) | 1.5 (1.3–1.6) | 1.1 (0.9–1.2) | 1.31 (1.15–1.49) | 0.94 (0.84–1.06) | 0.53 (0.46–0.61) | 0.73 (0.61–0.88) | 0.48 (0.41–0.57) |
| Non-PCV | 1.5 (1.3–1.6) | 2.0 (1.8–2.2) | 2.2 (2.0–2.5) | 2.7 (2.5–2.9) | 3.2 (2.9–3.5) | 1.36 (1.16–1.60) | 1.12 (0.97–1.29) | 1.2 (1.06–1.37) | 1.19 (1.06–1.33) | 2.18 (1.89–2.52) |
| Total cases | 6.3 (6.0–6.7) | 7.2 (6.8–7.6) | 5.9 (5.5–6.2) | 4.6 (4.3–4.9) | 4.8 (4.5–5.1) | 1.13 (1.04–1.22) | 0.82 (0.76–0.89) | 0.78 (0.71–0.85) | 1.05 (0.95–1.15) | 0.75 (0.69–0.82) |
| ≥65 years | n = 1471 | n = 1617 | n = 1518 | n = 1467 | n = 1634 | |||||
| PCV7 | 19.7 (18.3–21.2) | 14.3 (13.1–15.5) | 7.0 (6.3–7.9) | 3.8 (3.3–4.5) | 2.6 (2.2–3.1) | 0.72 (0.65–0.81) | 0.50 (0.43–0.57) | 0.55 (0.45–0.66) | 0.68 (0.54–0.85) | 0.13 (0.11–0.16) |
| PCV13nonPCV7 | 11.8 (10.7–13) | 14.8 (13.6–16.1) | 14.6 (13.5–15.8) | 9.6 (8.7–10.5) | 8.2 (7.4–9.0) | 1.25 (1.11–1.42) | 0.98 (0.88–1.10) | 0.66 (0.58–0.74) | 0.85 (0.74–0.98) | 0.69 (0.60–0.79) |
| Non-PCV | 8.7 (7.8–9.7) | 12.1 (11.0–13.2) | 14.6 (13.4–15.8) | 19.3 (18.0–20.6) | 23.8 (22.4–25.2) | 1.39 (1.21–1.60) | 1.20 (1.07–1.36) | 1.32 (1.2–1.47) | 1.23 (1.13–1.34) | 2.73 (2.41–3.09) |
| Total cases | 40.3 (38.2–42.4) | 41.2 (39.2–43.2) | 36.2 (34.4–38.0) | 32.7 (31.1–34.4) | 34.5 (32.9–36.2) | 1.02 (0.95–1.10) | 0.88 (0.82–0.94) | 0.90 (0.84–0.97) | 1.06 (0.98–1.13) | 0.86 (0.80–0.92) |
| All ages | n = 3031 | n = 3237 | n = 2929 | n = 2612 | n = 2871 | |||||
| PCV7 | 6.2 (5.9–6.5) | 4.5 (4.2–4.7) | 2.1 (1.9–2.3) | 1.1 (1.0–1.3) | 0.9 (0.8–1.1) | 0.72 (0.66–0.78) | 0.47 (0.42–0.52) | 0.53 (0.46–0.62) | 0.83 (0.70–0.99) | 0.15 (0.13–0.17) |
| PCV13nonPCV7 | 4.3 (4.0–4.6) | 5.5 (5.2–5.8) | 5.3 (5.0–5.6) | 3.2 (2.9–3.4) | 2.7 (2.5–2.9) | 1.28 (1.18–1.39) | 0.96 (0.88–1.04) | 0.6 (0.55–0.66) | 0.85 (0.76–0.94) | 0.62 (0.56–0.69) |
| Non-PCV | 2.9 (2.7–3.2) | 3.9 (3.7–4.2) | 4.8 (4.5–5.1) | 6.2 (5.9–6.5) | 7.6 (7.3–8.0) | 1.33 (1.21–1.47) | 1.22 (1.12–1.33) | 1.3 (1.2–1.4) | 1.23 (1.15–1.31) | 2.59 (2.37–2.83) |
| Total cases | 13.4 (13.0–13.9) | 13.9 (13.4–14.3) | 12.1 (11.7–12.6) | 10.5 (10.1–10.9) | 11.2 (10.8–11.6) | 1.03 (0.98–1.08) | 0.88 (0.83–0.92) | 0.86 (0.82–0.91) | 1.07 (1.02–1.13) | 0.83 (0.79–0.88) |
| IPD Cases- East | IPD Cases- West | Incidence (per 100′000) East | Incidence (per 100′000) West | IRR- West vs. East | 95% CI | |
|---|---|---|---|---|---|---|
| 2005–2007 (early PCV7 era) | ||||||
| PCV7 | 993 | 408 | 6.2 | 6.1 | 0.98 | 0.88–1.11 |
| PCV13nonPCV7 | 673 | 292 | 4.2 | 4.4 | 1.04 | 0.91–1.19 |
| Non-PCV | 456 | 206 | 2.9 | 3.1 | 1.08 | 0.92–1.28 |
| Total cases | 2122 | 906 | 13.3 | 13.6 | 1.02 | 0.95–1.10 |
| 2008–2010 (late PCV7 era) | ||||||
| PCV7 | 814 | 225 | 5.0 | 3.2 | 0.65 | 0.57–0.76 |
| PCV13nonPCV7 | 924 | 355 | 5.6 | 5.1 | 0.91 | 0.81–1.03 |
| Non-PCV | 634 | 284 | 3.9 | 4.1 | 1.06 | 0.92–1.22 |
| Total cases | 2372 | 864 | 14.4 | 12.5 | 0.86 | 0.80–0.93 |
| 2011–2013 (early PCV13 era) | ||||||
| PCV7 | 365 | 139 | 2.2 | 1.9 | 0.89 | 0.74–1.09 |
| PCV13nonPCV7 | 895 | 376 | 5.3 | 5.2 | 0.99 | 0.88–1.11 |
| Non-PCV | 780 | 374 | 4.6 | 5.2 | 1.13 | 1.00–1.27 |
| Total cases | 2040 | 889 | 12.1 | 12.3 | 1.02 | 0.95–1.11 |
| 2014–2016 (mid-PCV13 era) | ||||||
| PCV7 | 226 | 52 | 1.3 | 0.7 | 0.54 | 0.40–0.72 |
| PCV13nonPCV7 | 585 | 203 | 3.3 | 2.7 | 0.81 | 0.69–0.95 |
| Non-PCV | 1110 | 436 | 6.4 | 5.8 | 0.91 | 0.82–1.02 |
| Total cases | 1921 | 691 | 11 | 9.2 | 0.84 | 0.77–0.91 |
| 2017–2019 (late PCV13 era) | ||||||
| PCV7 | 193 | 44 | 1.1 | 0.6 | 0.53 | 0.38–0.74 |
| PCV13nonPCV7 | 523 | 159 | 2.9 | 2.1 | 0.71 | 0.59–0.85 |
| Non-PCV | 1429 | 514 | 8.0 | 6.7 | 0.84 | 0.76–0.93 |
| Total cases | 2145 | 717 | 12 | 9.3 | 0.78 | 0.72–0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyewole, O.R.-A.; Lang, P.; Albrich, W.C.; Wissel, K.; Leib, S.L.; Casanova, C.; Hilty, M. The Impact of Pneumococcal Conjugate Vaccine (PCV) Coverage Heterogeneities on the Changing Epidemiology of Invasive Pneumococcal Disease in Switzerland, 2005–2019. Microorganisms 2021, 9, 1078. https://doi.org/10.3390/microorganisms9051078
Oyewole OR-A, Lang P, Albrich WC, Wissel K, Leib SL, Casanova C, Hilty M. The Impact of Pneumococcal Conjugate Vaccine (PCV) Coverage Heterogeneities on the Changing Epidemiology of Invasive Pneumococcal Disease in Switzerland, 2005–2019. Microorganisms. 2021; 9(5):1078. https://doi.org/10.3390/microorganisms9051078
Chicago/Turabian StyleOyewole, Oluwaseun Rume-Abiola, Phung Lang, Werner C. Albrich, Kerstin Wissel, Stephen L. Leib, Carlo Casanova, and Markus Hilty. 2021. "The Impact of Pneumococcal Conjugate Vaccine (PCV) Coverage Heterogeneities on the Changing Epidemiology of Invasive Pneumococcal Disease in Switzerland, 2005–2019" Microorganisms 9, no. 5: 1078. https://doi.org/10.3390/microorganisms9051078