
Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol

 ,
,  ,
,  and
and 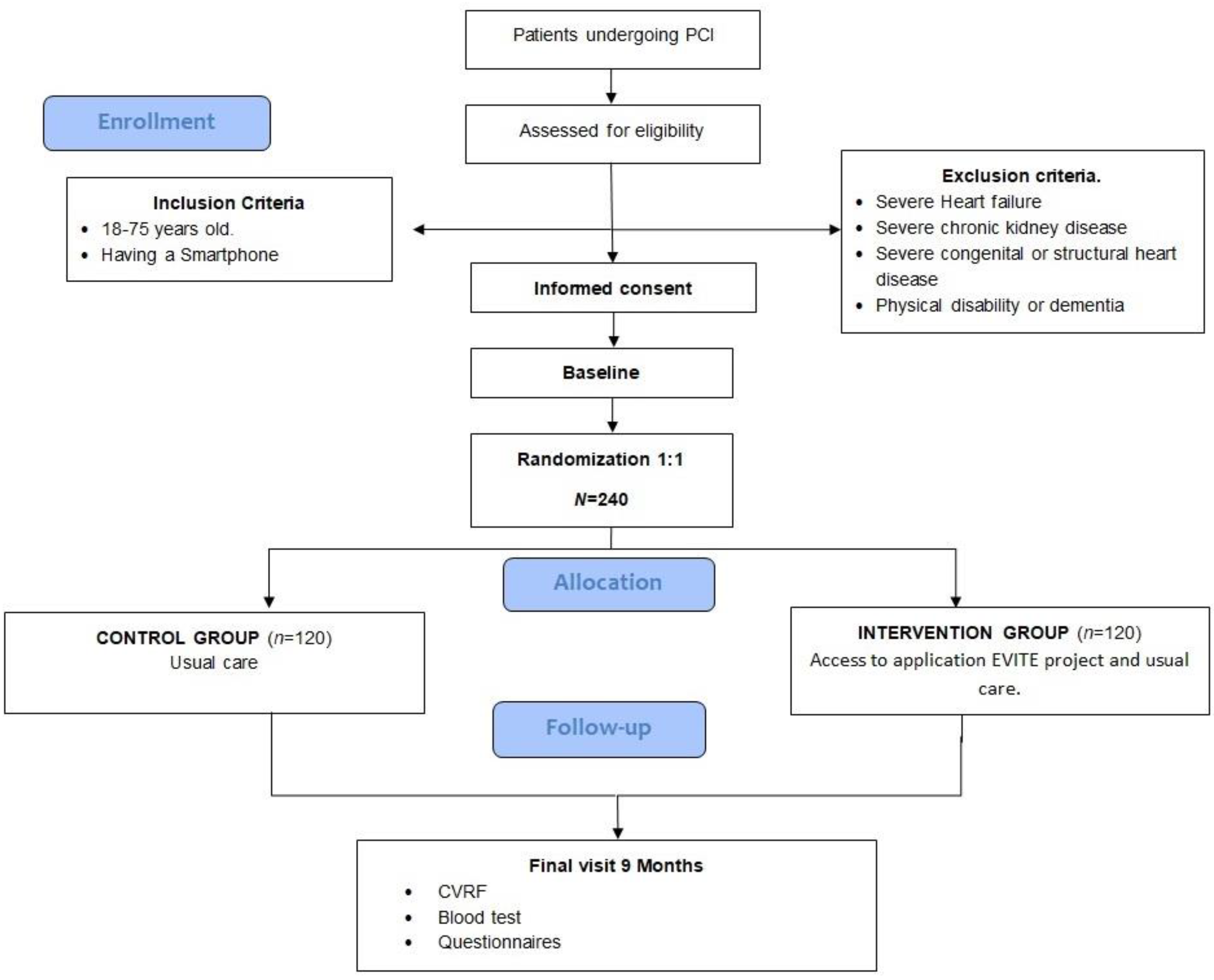{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Improvements in the pattern of diet and food consumption, physical activity and smoking habits.
- The objective measures of cardiovascular risk such as body mass index (BMI), waist circumference, blood pressure, and low-density lipoprotein (LDL) cholesterol.
- Acquiring knowledge about cardiovascular diseases (CVD), the risk factors, and a healthy lifestyle.
- The patients’ level of anxiety, quality of life, and well-being.
- The participants’ commitment to using the application and the level of self-monitoring of CVRFs.
- The participants’ satisfaction regarding the usability of the application.
- Use of health services, emergency visits, and readmissions of the participants throughout the study.
2. Materials and Methods
2.1. Design
2.2. Randomization and Blinding
2.3. Study Sample
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Sample Size
2.5. Recruitment
2.6. Intervention
2.7. Technical Data of the Website and Application
2.8. Application Contents
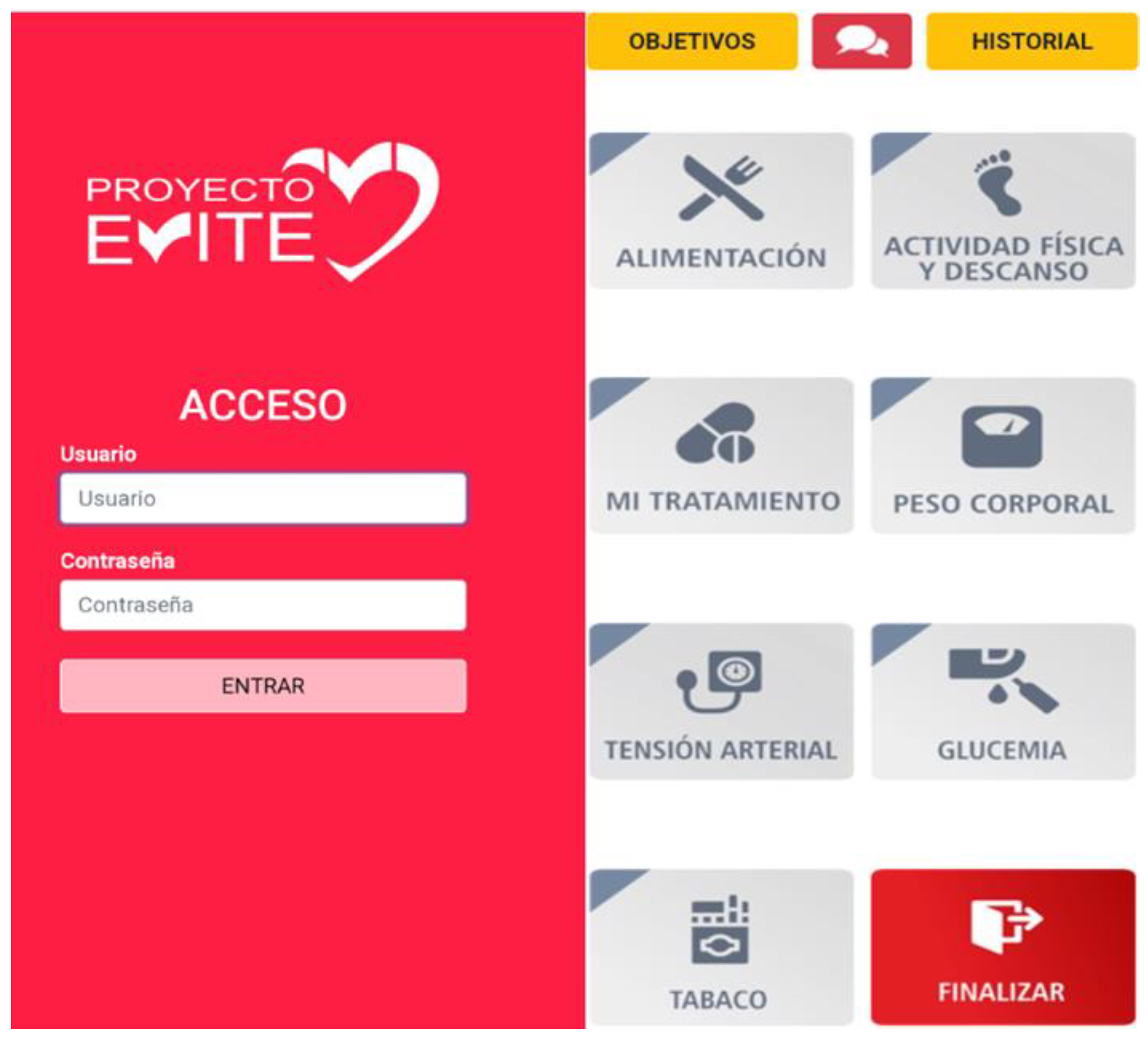
2.9. Components of the Application
- Nutrition (Figure 3). The food eaten in each meal (breakfast, lunch, tea, and dinner) is recorded using a drop-down list from which the food, and the amount consumed are selected (a portion, half portion or quarter portion). This is preferably recorded daily, or at least once a week.
- Physical activity and rest (Figure 3). The patient can select from a drop-down list the type of activity performed during the day, the duration, and the total number of steps each day. Additionally, they record the number of hours of sleep from the previous night and the minutes they are seated or having a siesta.
- Treatment (Figure 3). The participant accesses a screen with a personalized list with their daily treatment (name of medication, dose and timetable) and indicates the medication is taken, which is recorded. Medication cannot be recorded in advance.
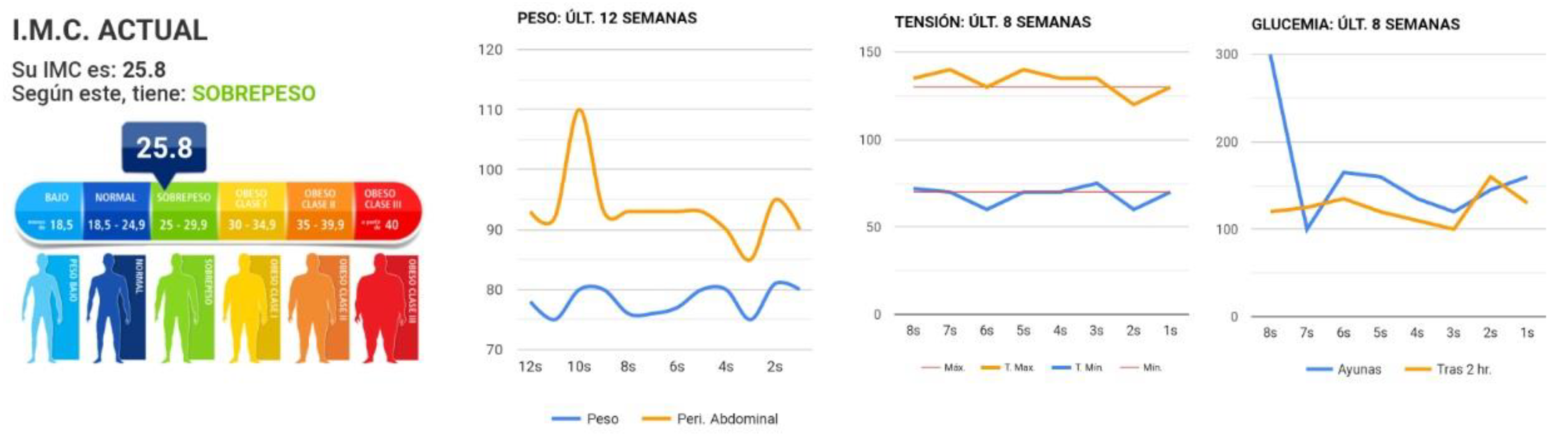
- Body weight (Figure 4). The participant records their body weight and waist circumference every week. The application calculates their BMI and classifies the value as normal, overweight, or obese, following the WHO BMI classification for adults [42]. The size in cm is recorded at the beginning when the application is activated.
- Blood pressure (Figure 4). The participants record their systolic and diastolic blood pressure as well as their heart rate every week.
- Blood glucose in patients with diabetes mellitus (Figure 4). Twice a week, the patients record their fasting blood glucose and levels two hours after consuming food.
- Tobacco in smokers (Figure 4). Record the number of cigarettes smoked in a week.
2.10. Training Session about the Application for Patient and Carer
2.11. Ethical Considerations
3. Results
3.1. Variables Collected in the Initial and Final Evaluations
3.2. Variables Recorded during the Intervention Using the Online Application
3.2.1. Primary Outcome Variables
3.2.2. Secondary Outcome Variables
3.3. Statistical Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Fact Sheets 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 March 2021).
- O’Keeffe, C.; Kabir, Z.; O’Flaherty, M.; Walton, J.; Capewell, S.; Perry, I.J. Modelling the impact of specific food policy options on coronary heart disease and stroke deaths in Ireland. BMJ Open 2013, 3, e002837. [Google Scholar] [CrossRef] [Green Version]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, A.R.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2018, 40, 87–165. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Holmes, D.R. Drug-Eluting Coronary-Artery Stents. N. Engl. J. Med. 2013, 368, 254–265. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Candil, J.; Díaz-Castro, Ó.; Barrabés, J.A.; De La Villa, B.G.; Peris, V.B.; Palop, R.L.; Fernández-Ortiz, A.; Martinez-Selles, M. Actualización en cardiopatía isquémica y cuidados críticos cardiológicos. Rev. Esp. Cardiol. 2013, 66, 198–204. [Google Scholar] [CrossRef]
- Andrés, E.; Cordero, A.; Magán, P.; Alegría, E.; León, M.; Luengo, E.; Botaya, R.M.; Ortiz, L.G.; Casasnovas, J.A. Mortalidad a largo plazo y reingreso hospitalario tras infarto agudo de miocardio: Un estudio de seguimiento de ocho años. Rev. Esp. Cardiol. 2012, 65, 414–420. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Abreu, A.; Albus, C.; Ambrosetti, M.; Brotons, C.; Catapano, A.L.; Corra, U.; Cosyns, B.; Deaton, C.; Graham, I.; et al. Update on cardiovascular prevention in clinical practice: A position paper of the European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2020, 27, 181–205. [Google Scholar] [CrossRef] [Green Version]
- Marquina, C.; Zomer, E.; Vargas-Torres, S.; Zoungas, S.; Ofori-Asenso, R.; Liew, D.; Ademi, Z. Novel Treatment Strategies for Secondary Prevention of Cardiovascular Disease: A Systematic Review of Cost-Effectiveness. PharmacoEconomics 2020, 38, 1095–1113. [Google Scholar] [CrossRef] [PubMed]
- Shields, E.G.; Wells, A.; Doherty, P.; Heagerty, A.; Buck, D.; Davies, L.M. Cost-effectiveness of cardiac rehabilitation: A systematic review. Heart 2018, 104, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- De Smedt, D.; Kotseva, K.; De Bacquer, D.; Wood, D.; De Backer, G.; Dallongeville, J.; Seppo, L.; Pająk, A.; Reiner, Z.; Vanuzzo, D.; et al. Cost-effectiveness of optimizing prevention in patients with coronary heart disease: The EUROASPIRE III health economics project. Eur. Heart J. 2012, 33, 2865–2872. [Google Scholar] [CrossRef]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) * Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar] [CrossRef] [Green Version]
- Wood, D.; Kotseva, K.; Connolly, S.; Jennings, C.; Mead, A.; Jones, J.; Holden, A.; De Bacquer, D.; Collier, T.; De Backer, G.; et al. Nurse-coordinated multidisciplinary, family-based cardiovascular disease prevention programme (EUROACTION) for patients with coronary heart disease and asymptomatic individuals at high risk of cardiovascular disease: A paired, cluster-randomised controlled trial. Lancet 2008, 371, 1999–2012. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-Y.; Choi, K.-C.; Ho, K.-M.; Yu, S.-F. Effectiveness of nurse-led patient-centered care behavioral risk modification on secondary prevention of coronary heart disease: A systematic review. Int. J. Nurs. Stud. 2018, 84, 28–39. [Google Scholar] [CrossRef]
- Allen, J.K.; Dennison-Himmelfarb, C.R.; Szanton, S.L.; Bone, L.R.; Hill, M.N.; Levine, D.M.; West, M.; Barlow, A.E.L.; Lewis-Boyer, L.; Donnelly-Strozzo, M.; et al. Community Outreach and Cardiovascular Health (COACH) Trial: A randomized, controlled trial of nurse practitioner/community health worker cardiovascular disease risk reduction in urban community health centers. Cardiovasc. Qual. Outcomes 2011, 4, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorstad, H.T.; Von Birgelen, C.; Alings, A.M.W.; Liem, A.; Van Dantzig, J.M.; Jaarsma, W.; Lok, D.J.A.; Kragten, H.J.A.; De Vries, K.; De Milliano, P.A.R.; et al. Effect of a nurse-coordinated prevention programme on cardiovascular risk after an acute coronary syndrome: Main results of the RESPONSE randomised trial. Heart 2013, 99, 1421–1430. [Google Scholar] [CrossRef] [Green Version]
- Han, E.; Quek, R.Y.C.; Tan, S.M.; Singh, S.R.; Shiraz, F.; Gea-Sánchez, M.; Legido-Quigley, H. The role of community-based nursing interventions in improving outcomes for individuals with cardiovascular disease: A systematic review. Int. J. Nurs. Stud. 2019, 100, 103415. [Google Scholar] [CrossRef]
- International Telecommunication Union. Measuring the Information Society Report. Available online: http://www.itu.int/en/ITU-D/Statistics/Documents/publications/mis2014/MIS2014_without_Annex_4.Pdf (accessed on 6 March 2021).
- International Telecommunication Union. Digital Trends in Europe 2021. Society Report. Available online: https://www.itu.int/pub/D-IND (accessed on 6 March 2021).
- Burke, L.E.; Ma, J.; Azar, K.M.; Bennett, G.G.; Peterson, E.D.; Zheng, Y.; Riley, W.J.; Stephens, J.; Shah, S.H.; Suffoletto, B.; et al. Current Science on Consumer Use of Mobile Health for Cardiovascular Disease Prevention: A scientific statement from the American Heart Association. Circulation 2015, 132, 1157–1213. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Feldman, D.I.; Blumenthal, R.S.; Jones, S.R.; Post, W.S.; McKibben, R.A.; Michos, E.D.; Ndumele, C.E.; Ratchford, E.V.; Coresh, J.; et al. mActive: A Randomized Clinical Trial of an Automated mHealth Intervention for Physical Activity Promotion. J. Am. Heart Assoc. 2015, 4, e002239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, C.K.; Redfern, J.; Hillis, G.S.; Thakkar, J.; Santo, K.; Hackett, M.; Jan, S.; Graves, N.; De Keizer, L.; Barry, T.; et al. Effect of Lifestyle-Focused Text Messaging on Risk Factor Modification in Patients with Coronary Heart Disease. JAMA 2015, 314, 1255–1263. [Google Scholar] [CrossRef]
- Thakkar, J.; Kurup, R.; Laba, T.-L.; Santo, K.; Thiagalingam, A.; Rodgers, A.; Woodward, M.; Redfern, J.; Chow, C.K. Mobile Telephone Text Messaging for Medication Adherence in Chronic Disease. JAMA Intern. Med. 2016, 176, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Gandapur, Y.; Kianoush, S.; Kelli, H.M.; Misra, S.; Urrea, B.; Blaha, M.J.; Graham, G.; Marvel, F.A.; Martin, S.S. The role of mHealth for improving medication adherence in patients with cardiovascular disease: A systematic review. Eur. Heart J. Qual. Care Clin. Outcomes 2016, 2, 237–244. [Google Scholar] [CrossRef]
- Treskes, R.W.; Van Winden, L.A.M.; Van Keulen, N.; Van Der Velde, E.T.; Beeres, S.L.M.A.; Atsma, D.E.; Schalij, M.J. Effect of Smartphone-Enabled Health Monitoring Devices vs Regular Follow-up on Blood Pressure Control Among Patients After Myocardial Infarction: A randomized clinical trial. JAMA Netw. Open 2020, 3, e202165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunde, P.; Bye, A.; Bergland, A.; Grimsmo, J.; Jarstad, E.; Nilsson, B.B. Long-term follow-up with a smartphone application improves exercise capacity post cardiac rehabilitation: A randomized controlled trial. Eur. J. Prev. Cardiol. 2020, 27, 1782–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, N.; Bodegard, J.; Jerström, S.; Åkesson, J.; Brorsson, H.; Alfredsson, J.; Albertsson, P.A.; Karlsson, J.-E.; Varenhorst, C. Effects of interactive patient smartphone support app on drug adherence and lifestyle changes in myocardial infarction patients: A randomized study. Am. Heart J. 2016, 178, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, S.; Chen, S.; Hong, L.; Sun, K.; Gong, E.; Li, C.; Yan, L.L.; Schwalm, J.-D. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Coorey, G.M.; Neubeck, L.; Mulley, J.; Redfern, J. Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. Eur. J. Prev. Cardiol. 2018, 25, 505–521. [Google Scholar] [CrossRef]
- Su, J.J.; Yu, D.S.F.; Paguio, J.T. Effect of eHealth cardiac rehabilitation on health outcomes of coronary heart disease patients: A systematic review and meta-analysis. J. Adv. Nurs. 2019, 76, 754–772. [Google Scholar] [CrossRef]
- Agarwal, S.; LeFevre, A.; Lee, J.; L’Engle, K.; Mehl, G.; Sinha, C.; Labrique, A. Guidelines for reporting of health interventions using mobile phones: Mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ 2016, 352, i1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish Men. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; I. Covas, M.; Marrugat, J. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish Women. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C.; Norcross, J.C. In search of how people change: Applications to addictive behaviors. Am. Psychol. 1992, 47, 1102–1114. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.; Rollnick, S. Motivational Interviewing: Preparing People for Change, 3rd ed.; Guilford Publicatins, Inc.: New York, NY, USA, 2013. [Google Scholar]
- Bartrina, J.A. Guías alimentarias para la población española (SENC, 2016); la nueva pirámide de la alimentación saludable. Nutr. Hosp. 2016, 33, 1–48. [Google Scholar]
- Robinson, T.N. Stealth interventions for obesity prevention and control: Motivating behavior change. In Obesity Prevention: The Role of Brain and Society on Individual Behavior; Dubé, L., Bechara, A., Dagher, A., Drewnowski, A., Lebel, J., James, P., Yada, R.Y., Eds.; Academic Press: New York, NY, USA, 2010; Chapter 25; pp. 319–327. [Google Scholar]
- Locke, E.A.; Bandura, A. Social Foundations of Thought and Action: A Social-Cognitive View. Acad. Manag. Rev. 1987, 12, 169. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic Report of a WHO Consultation on Obesity; Technical Report Series; World Health Organization: Geneva, Switzerland, 2000; ISBN 92412089. [Google Scholar]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardio-Thorac. Surg. 2012, 41, 734–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagerström, K.-O. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict. Behav. 1978, 3, 235–241. [Google Scholar] [CrossRef]
- Córdoba, R.; Martin, C.F.; Casas, R.; Barberá, C.; Botaya, M.; Hernandez, A.C.; Jané, C. Valor de los cuestionarios breves en la predicción del abandono del tabaco en atención primaria. Atención Primaria 2000, 25, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Spanish Food Composition Database. Ministry of Science and Innovation. Spanish Agency for Food Safety and Nutrition. Ministry of Health, Social Services and Equality. Available online: https://www.bedca.net/bdpub/ (accessed on 6 March 2021).
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a Self-reported Measure of Medication Adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Alm-Roijer, C.; Fridlund, B.; Stagmo, M.; Erhardt, L. Knowing Your Risk Factors for Coronary Heart Disease Improves Adherence to Advice on Lifestyle Changes and Medication. J. Cardiovasc. Nurs. 2006, 21, E24–E31. [Google Scholar] [CrossRef] [PubMed]
- Cosco, T.D.; Doyle, F.; Watson, R.; Ward, M.; McGee, H. Mokken scaling analysis of the Hospital Anxiety and Depression Scale in individuals with cardiovascular disease. Gen. Hosp. Psychiatry 2012, 34, 167–172. [Google Scholar] [CrossRef]
- Dempster, M. Measuring the health related quality of life of people with ischaemic heart disease. Heart 2000, 83, 641–644. [Google Scholar] [CrossRef] [PubMed]
- WHO-Five Well-Being Index. Available online: http://www.who-5.org/ (accessed on 6 April 2021).
- King, A.C.; Hekler, E.B.; Grieco, L.A.; Winter, S.J.; Sheats, J.L.; Buman, M.; Banerjee, B.; Robinson, T.N.; Cirimele, J. Harnessing Different Motivational Frames via Mobile Phones to Promote Daily Physical Activity and Reduce Sedentary Behavior in Aging Adults. PLoS ONE 2013, 8, e62613. [Google Scholar] [CrossRef] [PubMed] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Jiménez, M.Á.; Calle-Pérez, G.; Gutiérrez-Barrios, A.; Gheorghe, L.; Solano-Mulero, A.M.; Rodríguez-Martín, A.; Tur, J.A.; Vázquez-García, R.; Santi-Cano, M.J. Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol. Nutrients 2021, 13, 1818. https://doi.org/10.3390/nu13061818
Bernal-Jiménez MÁ, Calle-Pérez G, Gutiérrez-Barrios A, Gheorghe L, Solano-Mulero AM, Rodríguez-Martín A, Tur JA, Vázquez-García R, Santi-Cano MJ. Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol. Nutrients. 2021; 13(6):1818. https://doi.org/10.3390/nu13061818
Chicago/Turabian StyleBernal-Jiménez, María Ángeles, Germán Calle-Pérez, Alejandro Gutiérrez-Barrios, Livia Gheorghe, Ana María Solano-Mulero, Amelia Rodríguez-Martín, Josep A. Tur, Rafael Vázquez-García, and María José Santi-Cano. 2021. "Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol" Nutrients 13, no. 6: 1818. https://doi.org/10.3390/nu13061818
APA StyleBernal-Jiménez, M. Á., Calle-Pérez, G., Gutiérrez-Barrios, A., Gheorghe, L., Solano-Mulero, A. M., Rodríguez-Martín, A., Tur, J. A., Vázquez-García, R., & Santi-Cano, M. J. (2021). Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol. Nutrients, 13(6), 1818. https://doi.org/10.3390/nu13061818