
Extrapolating the Coffee and Caffeine (1,3,7-Trimethylxanthine) Effects on Exercise and Metabolism—A Concise Review


Abstract
:1. Introduction
2. Coffee and Caffeine Outcomes
2.1. Caffeine Action Mechanisms
2.2. Caffeine Metabolism and Pharmacokinetics Differences between Populations
2.3. Coffee x Caffeine Effects on Physical Performance

{kind=link}
| Author(s), Year, Reference Number | Caffeine Dose | Timing | Characteristic of Study/Participants | Results |
|---|---|---|---|---|
| Lieberman et al., 2002 [12] | Caffeine in doses of 100, 200, or 300 mg. | The experiment commenced on Sunday night, and at the following Wednesday night at 9:30, either caffeine or placebo was administered. | Double-blind, placebo-controlled study. A total of 68 U.S. Navy Sea–Air–Land trainees, randomly allocated to receive either 100, 200, or 300 mg caffeine or placebo capsules, after 72 h of sleep deprivation and sustained exposure to other stressors. | Caffeine (200 and 300 mg) yielded statistically significant enhancements in visual vigilance, choice reaction time, repeated acquisition, self-reported fatigue, and sleepiness. Most pronounced effects were observed in assessments related to vigilance, reaction time, and overall alertness. |
| Ruiz-Moreno et al., 2020 [24] | 3 mg of caffeine per kg of body mass. | 60 min before the onset of exercise. | Randomized double-blind, placebo-controlled study; 12 healthy participants undertook two acute experimental trials after ingesting of caffeine (3 mg/kg) or a placebo. Trials consisted of 1 h of uninterrupted cycling at Fatmax. Energy expenditure, fat oxidation rate, and carbohydrate oxidation rate were continuously evaluated by indirect calorimetry. | Caffeine augmented the total fat oxidized during the trial and reduced the amount of carbohydrate oxidized and the mean self-perception of fatigue in comparison to the placebo. |
| San Juan et al., 2019 [25] | 6 mg of caffeine per kg of body mass. | 75 min before the start of the session. | Randomized double-blind, placebo-controlled study evaluated the effects of caffeine supplementation on anaerobic performance, neuromuscular efficiency and fatigue in upper and lower extremities in 8 Olympic-level boxers. The athletes performed 2 test bouts after the ingestion of caffeine or placebo. | Caffeine supplementation improved anaerobic performance without affecting electromiography activity and fatigue levels in the lower limbs. Other observed benefits were improved neuromuscular efficiency in some muscles and reaction speed. |
| Foskett et al., 2009 [26] | 6 mg of caffeine per kg of body mass. | 60 min before exercise. | Randomized double-blind, placebo-controlled study. A total of 12 male soccer athletes participated in two 90 min sessions of soccer-specific intermittent running, with intervals dedicated to assessments of their soccer skill. | Participants incurred a significantly reduced amount of penalty time (added for erros) in the caffeine trial, resulting in a notably diminished total duration of this particular trial. The ingestion of caffeine led to enhancements in players’ passing accuracy and jump performance, with no adverse impact observed on other performance indicators. |
| Jodra et al., 2020 [27] | 6 mg of caffeine per kg of body mass. | 60 min before exercise. | Randomized double-blind, placebo-controlled. 8 elite athletes (senior boxing national team) were examined alongside 10 trained recreational athletes the immediate effects of caffeine on anaerobic performance, mood, and perceived effort in both group. During two separate experimental conditions, involving either caffeine supplementation or a placebo, the athletes underwent a Wingate test. | Caffeine supplementation improved anaerobic performance in both groups. The ergogenic effect of caffeine on several mood dimensions and subjective evaluation was superior in the elite athletes. |
| Domínguez et al., 2021 [28] | 6 mg of caffeine per kg of body mass. | 75 min before exercise. | Randomized double-blind, placebo-controlled study examined 15 male resistance training experience volunteers. A total of 60 min after supplement ingestion, participants filled two questionnaires, measuring subjective vitality and mood state. Participants’ performance was evaluated through a Wingate test, which was followed by measurements of rate of general perceived exertion, muscular and cardiovascular level. | Caffeine supplementation improved some components of mood assessed by POMS (tension and vigor dimensions) and subjective vitality profiles, which were succeeded by a enhanced maximum power, average power, and lower time needed to reach maximum power during the Wingate test. Caffeine supplementation yields positive effects both in psychological and physical aspects in trained volunteers. |
| Clarke et al., 2019 [29] | 0.09g of coffee per kg providing 3 mg of caffeine per kg of body mass. | 60 min before exercise. | Randomized double-blind, placebo-controlled study. 38 recreationally active participants executed a 5 km cycling time trial on a cycle ergometer after ingestion of 0.09 g·kg−1 coffee, a placebo or control (water). Coffee intake significantly augmented salivary caffeine levels. | Coffee ingestion achieving 3 mg·kg−1 of caffeine, increased salivary caffeine levels and augmented 5 km cycling time trial performance in men and women by a similar degree (lowering by approximately 9 s and 6 s following coffee ingestion compared with placebo and control, respectively). |
| Loureiro et al., 2021 [30] | The total caffeine provided with the three doses of coffee + milk treatment was 8 mg per kg of body mass. | Three doses of coffee + milk at times 0, 60 and 120 min after exercise (recovery time). | Randomized double-blind, placebo-controlled study. 14 endurance-trained men executed an exhaustive cycle ergometer exercise depleting muscle glycogen. In the following morning, subjects performed a second cycling protocol followed by a 4-h recovery, whilst they received either test beverage (coffee + milk) or control (milk) and a breakfast meal, in a simple randomization model. Blood samples and muscle biopsies were realized at the onset and by the end of recovery. | The ingestion of coffee + milk resulted in greater muscle glycogen recovery, greater glucose and insulin total AUC compared with just milk. The inclusion of coffee to a beverage with adequate quantities of carbohydrates augmented muscular glycogen resynthesis, the glycemic and insulinemic response during the 4 h recovery after exhaustive cycling exercise. |
2.4. Caffeine Thermogenic and Insulin Sensitivity Effect (Acute x Chronic)
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denoeud, F.; Carretero-Paulet, L.; Dereeper, A.; Droc, G.; Guyot, R.; Pietrella, M.; Lashermes, P. The coffee genome provides insight into the convergent evolution of caffeine biosynthesis. Science 2014, 345, 1181. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.A.; Boozer, C.N.; Geliebter, A. Coffee, diabetes, and weight control. Am. J. Clin. Nutr. 2006, 84, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Tse, S.Y.H. Cholinomimetic compound distinct from caffeine contained in coffee. II: Muscarinic actions. J. Pharm. Sci. 1992, 81, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Dulloo, A.G.; Geissler, C.A.; Horton, T.; Collins, A.; Miller, D.S. Normal caffeine consumption: Influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers. Am. J. Clin. Nutr. 1989, 49, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, G.; Herbst, K.L.; Dhuli, K.; Kiani, A.K.; Michelii, S.; Bertelli, M. Dietary supplements for lipedema. J. Prev. Med. Hyg. 2022, 63 (Suppl. S3), E169. [Google Scholar] [PubMed]
- Daly, J.W.; Fredholm, B.B. Mechanisms of action of caffeine on the nervous system. Coffee Tea Choc. Brain 2004, 2, 1–11. [Google Scholar]
- Carek, P.J.; Dickerson, L.M. Current concepts in the pharmacological management of obesity. Drugs 1999, 57, 883–904. [Google Scholar] [CrossRef] [PubMed]
- Varillas-Delgado, D.; Aguilar-Navarro, M.; Muñoz, A.; López-Samanés, Á.; Ruiz-Moreno, C.; Posada-Ayala, M.; Gutiérrez-Hellín, J. Effect of 3 and 6 mg/kg of caffeine on fat oxidation during exercise in healthy active females. Biol. Sport 2023, 40, 827–834. [Google Scholar] [CrossRef]
- Davis, J.M.; Zhao, Z.; Stock, H.S.; Mehl, K.A.; Buggy, J.; Hand, G.A. Central nervous system effects of caffeine and adenosine on fatigue. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R399–R404. [Google Scholar] [CrossRef]
- Casiglia, E.S.; Bongiovi, C.D.; Paleari, S.; Petucco, M.; Boni, G.; Colangeli, G.; Pessina, A.C. Hemodynamic effects of coffee and caffeine in regular volunteers: A placebo controlled clinical study. J. Intern. Med. 1991, 229, 501–504. [Google Scholar] [CrossRef]
- Stuart, G.R.; Hopkins, W.G.; Cook, C.; Cairns, S.P. Multiple effects of caffeine on simulated high-intensity team-sport performance. Med. Sci. Sports Exerc. 2005, 37, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, H.R.; Tharion, W.J.; Shukitt-Hale, B.; Speckman, K.L.; Tulley, R. Effects of caffeine, sleep loss, and stress on cognitive performance and mood during U.S. Navy SEAL training. Sea-Air-Land. Psychopharmacology 2002, 164, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Herz, R. The relationship between caffeine contracture of intact muscle and the effect of caffeine on reticulum. J. Gen. Physiol. 1968, 52, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.S.; Coleman, C.; Shelton, R.; Heemstra, L.A.; Novak, C.M. Caffeine enhances activity thermogenesis and energy expenditure in rats. Clin. Exp. Pharmacol. Physiol. 2019, 46, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Sachse, C.; Brockmöller, J.; Bauer, S.; Roots, I. Functional significance of a C→ A polymorphism in intron 1 of the cytochrome P450 CYP1A2 gene tested with caffeine. Brit. J. Clin. Pharm. 1999, 47, 445–449. [Google Scholar] [CrossRef]
- Kamimori, G.H.; Somani, S.M.; Knowlton, R.G.; Perkins, R.M. The effects of obesity and exercise on the pharmacokinetics of caffeine in lean and obese volunteers. Euro. J. Clin. Pharm. 1987, 31, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Southward, K.; Rutherfurd-Markwick, K.; Badenhorst, C.; Ali, A. The Role of Genetics in Moderating the Inter-Individual Differences in the Ergogenicity of Caffeine. Nutrients 2018, 10, 1352. [Google Scholar] [CrossRef]
- Guest, N.; Corey, P.; Vescovi, J.; El-Sohemy, A. Caffeine, CYP1A2 Genotype, and Endurance Performance in Athletes. Med. Sci. Sports Exerc. 2018, 50, 1570–1578. [Google Scholar] [CrossRef]
- Larsson, S.C.; Woolf, B.; Gill, D. Appraisal of the causal effect of plasma caffeine on adiposity, type 2 diabetes, and cardiovascular disease: Two sample mendelian randomisation study. BMJ Med. 2023, 2, 1–8. [Google Scholar] [CrossRef]
- Aguilar-Navarro, M.; Gloria Muñoz, G.; Salinero, J.; Muñoz-Guerra, J.; Fernández-Álvarez, M.; Plata, M.D.M.; Del Coso, J. Urine caffeine concentration in doping control samples from 2004 to 2015. Nutrients 2019, 11, 286. [Google Scholar] [CrossRef]
- Graham, T.E.; Hibbert, E.; Sathasivam, P. Metabolic and exercise endurance effects of coffee and caffeine ingestion. J. Appl. Phys. 1998, 85, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Costill, D.L.; Dalsky, G.P.; Fink, W.J. Effects of caffeine ingestion on metabolism and exercise performance. Med. Sci. Sports 1978, 10, 155–158. [Google Scholar] [PubMed]
- Arnaud, M.J. Pharmacokinetics and metabolism of natural methylxanthines in animal and man. Methylxanthines 2011, 33–91. [Google Scholar] [CrossRef]
- Ruiz-Moreno, C.; Gutiérrez-Hellín, J.; Amaro-Gahete, F.J.; González-García, J.; Giráldez-Costas, V.; Del Coso, J. Caffeine increases whole-body fat oxidation during 1 h of cycling at Fatmax. Euro. J. Nutr. 2020, 60, 2077–2085. [Google Scholar] [CrossRef] [PubMed]
- San Juan, A.F.; López-Samanes, Á.; Jodra, P.; Valenzuela, P.L.; Rueda, J.; Domínguez, R. Caffeine Supplementation Improves Anaerobic Performance and Neuromuscular Efficiency and Fatigue in Olympic-Level Boxers. Nutrients 2019, 11, 2120. [Google Scholar] [CrossRef] [PubMed]
- Foskett, A.; Ali, A.; Gant, N. Caffeine enhances cognitive function and skill performance during simulated soccer activity. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 410–423. [Google Scholar] [CrossRef]
- Jodra, P.; Lago-Rodríguez, A.; Sánchez-Oliver, A.J.; López-Samanes, A.; Pérez-López, A.; Veiga-Herreros, P.; Domínguez, R. Effects of caffeine supplementation on physical performance and mood dimensions in elite and trained-recreational athletes. J. Int. Soc. Sports Nutr. 2020, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, R.; Veiga-Herreros, P.; Sánchez-Oliver, A.J.; Montoya, J.J.; Ramos-Álvarez, J.J.; Miguel-Tobal, F.; Jodra, P. Acute Effects of Caffeine Intake on Psychological Responses and High-Intensity Exercise Performance. Int. J. Environ. Res. Public Health 2021, 18, 584. [Google Scholar] [CrossRef]
- Clarke, N.D.; Kirwan, N.A.; Richardson, D.L. Coffee Ingestion Improves 5 km Cycling Performance in Men and Women by a Similar Magnitude. Nutrients 2019, 11, 2575. [Google Scholar] [CrossRef]
- Loureiro, L.M.R.; Dos Santos Neto, E.; Molina, G.E.; Amato, A.A.; Arruda, S.F.; da Costa, T.H.M. Coffee Increases Post-Exercise Muscle Glycogen Recovery in Endurance Athletes: A Randomized Clinical Trial. Nutrients 2021, 13, 3335. [Google Scholar] [CrossRef]
- Liguori, A.; Hughes, J.R.; Grass, J.A. Absorption and subjective effects of caffeine from coffee, cola and capsules. Pharmacol. Biochem. Behav. 1997, 58, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, A.B.; Randell, R.K.; Jeukendrup, A.E. The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS ONE 2013, 8, e59561. [Google Scholar] [CrossRef] [PubMed]
- Trexler, E.T.; Smith-Ryan, A.E.; Roelofs, E.J.; Hirsch, K.R.; Mock, M.G. Effects of coffee and caffeine anhydrous on strength and sprint performance. Eur. J. Sport Sci. 2016, 16, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.L.; Clarke, N.D. Effect of Coffee and Caffeine Ingestion on Resistance Exercise Performance. J. Strength Cond. Res. 2016, 30, 2892–2900. [Google Scholar] [CrossRef] [PubMed]
- Carlström, M.; Larsson, S. Coffee consumption and reduced risk of developing type 2 diabetes: A systematic review with meta-analysis. Nutr. Rev. 2018, 76, 395–417. [Google Scholar] [CrossRef] [PubMed]
- Reis, C.E.G.; Dórea, J.G.; da Costa, T.H.M. Effects of coffee consumption on glucose metabolism: A systematic review of clinical trials. J. Tradit. Complement. Med. 2018, 9, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Akash, M.S.; Rehman, K.; Chen, S. Effects of coffee on type 2 diabetes mellitus. Nutrition 2014, 30, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Hudson, R.; Kilpatrick, K.; Graham, T.; Ross, R. Caffeine ingestion is associated with reductions in glucose uptake independent of obesity and type 2 diabetes before and after exercise training. Diabetes Care 2005, 28, 566–572. [Google Scholar] [CrossRef]
- Hoppe, J. Ueber die Wirkungen des Coffein. Deutsch. Klin. 1857, 9, 181. [Google Scholar]
- Smith, E. Experimental Inquiries Into the Chemical and Other Phenomena of Respiration and Their Modifications by Various Physical Agencies. Philos. Trans. 1859, 149, 681. [Google Scholar]
- Greenberg, J.A.; Axen, K.V.; Schnoll, R.; Boozer, C.N. Coffee, tea and diabetes: The role of weight loss and caffeine. Int. J. Obes. Relat. Metab. Disord. 2005, 29, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M.; Hu, F.B. Coffee consumption and risk of type 2 diabetes: A systematic review. JAMA 2005, 294, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M. Coffee and type 2 diabetes: From beans to beta-cells. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.; Lu, Y.; Bowman, L.L.; Qian, Y.; Castranova, V.; Ding, M. Inhibition of AP-1, NF-kappa B and MAPKs and induction of phase 2 detoxifying enzyme activity by chlorogenic acid. J. Biol. Chem. 2005, 280, 27888–27895. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; van Dam, R.M.; Qi, L.; Hu, F.B. Coffee consumption and markers of inflammation and endothelial dysfunction in healthy and diabetic women. Am. J. Clin. Nutr. 2006, 84, 888–893. [Google Scholar] [CrossRef]
- Wedick, N.M.; Brennan, A.M.; Sun, Q.; Hu, F.B.; Mantzoros, C.S.; van Dam, R.M. Effects of caffeinated and decaffeinated coffee on biological risk factors for type 2 diabetes: A randomized controlled trial. Nutr. J. 2011, 10, 93. [Google Scholar] [CrossRef]
- Kolb, H.; Martin, S.; Kempf, K. Coffee and Lower Risk of Type 2 Diabetes: Arguments for a Causal Relationship. Nutrients 2021, 13, 1144. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef]
- Pickering, R.J. Oxidative Stress and Inflammation in Cardiovascular Diseases. Antioxidants 2021, 10, 171. [Google Scholar] [CrossRef]
- Dludla, P.V.; Nkambule, B.B.; Jack, B.; Mkandla, Z.; Mutize, T.; Mazibuko-Mbeje, S.E. Inflammation and Oxidative Stress in an Obese State and the Protective Effects of Gallic Acid. Nutrients 2018, 11, 23. [Google Scholar] [CrossRef]
- Guest, N.S.; VanDusseldorp, T.A.; Nelson, M.T.; Grgic, J.; Schoenfeld, B.J.; Campbell, B.I. International Society of Sports Nutrition Position Stand: Caffeine and Exercise Performance. J. Int. Soc. Sports Nutr. 2021, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- de Souza, J.G.; Del Coso, J.; Fonseca, F.d.S.; Silva, B.V.C.; de Souza, D.B.; da Silva Gianoni, R.L.; Filip-Stachnik, A.; Serrão, J.C.; Claudino, J.G. Risk or Benefit? Side Effects of Caffeine Supplementation in Sport: A Systematic Review. Eur. J. Nutr. 2022, 61, 3823–3834. [Google Scholar] [CrossRef] [PubMed]
- Dludla, P.V.; Cirilli, I.; Marcheggiani, F.; Silvestri, S.; Orlando, P.; Tiano, L. Potential Benefits of Coffee Consumption on Improving Biomarkers of Oxidative Stress and Inflammation in Healthy Individuals and Those at Increased Risk of Cardiovascular Disease. Molecules 2023, 28, 6440. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Castrejón-Téllez, V.; Soto, M.E.; Rubio-Ruiz, M.E.; Manzano-Pech, L.; Guarner-Lans, V. Oxidative Stress, Plant Natural Antioxidants, and Obesity. Int. J. Mol. Sci. 2021, 22, 1786. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, R.P.; Lima, F.D.; Carvalho, N.R.; Bresciani, G.; Royes, L.F. Caffeine effects on systemic metabolism, oxidative- inflammatory pathways, and exercise performance. Nutr. Res. 2020, 80, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.; Kempf, K.; Martin, S. Health Effects of Coffee: Mechanism Unraveled? Nutrients 2020, 12, 1842. [Google Scholar] [CrossRef] [PubMed]
- Lonati, E.; Carrozzini, T.; Bruni, I.; Mena, P.; Botto, L.; Cazzaniga, E.; Del Rio, D.; Labra, M.; Palestini, P.; Bulbarelli, A. Coffee- Derived Phenolic Compounds Activate Nrf2 Antioxidant Pathway in I/R Injury In Vitro Model: A Nutritional Approach Preventing Age Related-Damages. Molecules 2022, 27, 1049. [Google Scholar] [CrossRef]
- Boettler, U.; Sommerfeld, K.; Volz, N.; Pahlke, G.; Teller, N.; Somoza, V.; Lang, R.; Hofmann, T.; Marko, D. Coffee constituents as modulators of Nrf2 nuclear translocation and ARE (EpRE)-dependent gene expression. J. Nutr. Biochem. 2011, 22, 426–440. [Google Scholar] [CrossRef]
- Sánchez-Medina, A.; Redondo-Puente, M.; Dupak, R.; Bravo Clemente, L.; Goya, L.; Sarriá, B. Colonic Coffee Phenols Metabolites, Dihydrocaffeic, Dihydroferulic, and Hydroxyhippuric Acids Protect Hepatic Cells from TNF-α-Induced Inflammation and Oxidative Stress. Int. J. Mol. Sci. 2023, 24, 1440. [Google Scholar] [CrossRef]
- Harpaz, E.; Tamir, S.; Weinstein, A.; Weinstein, Y. The effect of caffeine on energy balance. J. Basic Clin. Physiol. Pharmacol. 2017, 28, 1–10. [Google Scholar] [CrossRef]
- Hossein, S.; Javad, S.; Ajami, M.; Mohseni-Bandpei, A. Caffeine treat- ment prevented from weight regain after calorie shifting diet induced weight loss. Iran. J. Pharm. Res. 2014, 13, 707–718. [Google Scholar]
- Nordestgaard, A.T.; Thomsen, M.; Nordestgaard, B.G. Coffee intake and risk of obesity, metabolic syndrome and type 2 diabetes: A Mendelian randomization study. Int. J. Epidem. 2015, 44, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Bhupathiraju, S.N.; Satija, A.; van Dam, R.M.; Hu, F.B. Long-term coffee consumption and risk of cardiovascular disease: A systematic review and a doseresponse meta-analysis of prospective cohort studies. Circulation 2014, 129, 643–659. [Google Scholar] [CrossRef]
- Nordestgaard, A.T.; Stender, S.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. Coffee intake protects against symptomatic gallstone disease in the general population: A Mendelian randomization study. J. Intern. Med. 2020, 287, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Li, S. Dose-response meta-analysis on coffee, tea and caffeine consumption with risk of Parkinson’s disease. Geriatr. Gerontol. Int. 2014, 14, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Lucas, M.; O’Reilly, E.J.; Pan, A.; Mirzaei, F.; Willett, W.C.; Ascherio, A. Coffee, caffeine, and risk of completed suicide: Results from three prospective cohorts of American adults. World J. Biol. Psychiatry 2014, 15, 377–386. [Google Scholar] [CrossRef]
- Gardener, S.L.; Rainey-Smith, S.R.; Villemagne, V.L.; Fripp, J.; Doré, V.; Bourgeat, P. Higher Coffee Consumption Is Associated with Slower Cognitive Decline and Less Cerebral Aβ-Amyloid Accumulation over 126 Months: Data from the Australian Imaging, Biomarkers, and Lifestyle Study. Front. Aging Neurosci. 2021, 13, 744872. [Google Scholar] [CrossRef]
- Lipton, R.B.; Diener, H.C.; Robbins, M.S.; Garas, S.Y.; Patel, K. Caffeine in the management of patients with headache. J. Headache Pain 2017, 18, 107. [Google Scholar] [CrossRef]
- Gutiérrez-Hellín, J.; Varillas-Delgado, D. Energy Drinks and Sports Performance, Cardiovascular Risk, and Genetic Associations; Future Prospects. Nutrients 2021, 13, 715. [Google Scholar] [CrossRef]
- Cappelletti, S.; Piacentino, D.; Sani, G.; Aromatario, M. Caffeine: Cognitive and physical performance enhancer or psychoactive drug? Curr. Neuropharmacol. 2015, 13, 71–88. [Google Scholar] [CrossRef]
- Nawrot, P.; Jordan, S.; Eastwood, J.; Rotstein, J.; Hugenholtz, A.; Feeley, M. Effects of caffeine on human health. Food Addit. Contam. 2003, 20, 1–30. [Google Scholar] [CrossRef] [PubMed]

| Action Mechanisms of Caffeine | References |
|---|---|
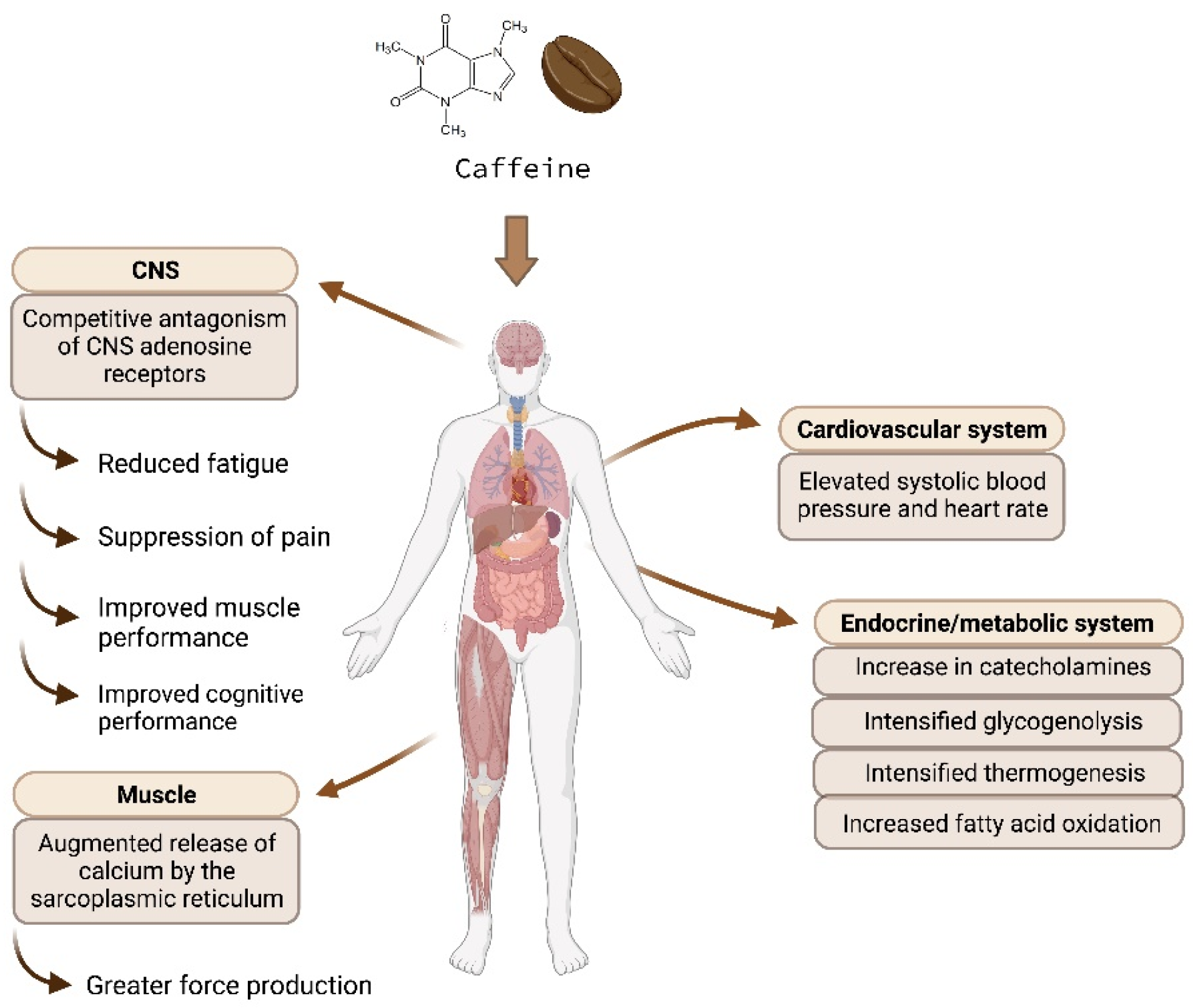
| Increased fatty acid oxidation rate. | Varillas-Delgado et al., 2023 [8] |
| Competitive antagonism of CNS adenosine receptors, resulting in diminished tiredness, pain suppression, and enhanced muscular function. | Davis et al., 2003 [9] |
| Elevated systolic blood pressure and heart rate by blocking adenosine receptors. | Casiglia et al., 1991 [10] |
| Greater catecholamines levels lead to CNS stimulation and intensified glycogenolysis. | Stuart et al., 2005 [11] |
| Improved cognitive performance. | Lieberman et al., 2002 [12] |
| Augmented release of calcium by the sarcoplasmic reticulum and greater force production. | Weber and Herz, 1968 [13] |
| Thermogenesis and higher energy expenditure. | Clark, 2019 [14] |
| Reduced risk of cardiovascular diseases | An inverse association has been observed between coffee consumption and coronary artery disease, stroke, and death from cardiovascular causes. | Ding et al., 2014 [63] |
| Reduced risk of gallstones | Coffee consumption has been associated with a reduced risk of symptomatic gallstone disease. | Nordestgaard et al., 2019 [64] |
| Reduced risk of Parkinson’s disease | There is a decreased Parkinson’s disease risk with caffeine consumption. | Qi and Li, 2014 [65] |
| Reduced risk of depression and suicide | Prospective studies support an association between caffeine consumption and lower risk of suicide. | Lucas et al., 2014 [66] |
| Reduced risk of cognitive decline | Higher coffee consumption was associated with slower cognitive decline in cognitively normal elderly. | Gardener et al., 2021 [67] |
| Headache | Caffeine is an adjuvant for the acute treatment of headache in combination with analgesics. | Lipton et al., 2017 [68] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Starling-Soares, B.; Pereira, M.; Renke, G. Extrapolating the Coffee and Caffeine (1,3,7-Trimethylxanthine) Effects on Exercise and Metabolism—A Concise Review. Nutrients 2023, 15, 5031. https://doi.org/10.3390/nu15245031
Starling-Soares B, Pereira M, Renke G. Extrapolating the Coffee and Caffeine (1,3,7-Trimethylxanthine) Effects on Exercise and Metabolism—A Concise Review. Nutrients. 2023; 15(24):5031. https://doi.org/10.3390/nu15245031
Chicago/Turabian StyleStarling-Soares, Bernardo, Marcela Pereira, and Guilherme Renke. 2023. "Extrapolating the Coffee and Caffeine (1,3,7-Trimethylxanthine) Effects on Exercise and Metabolism—A Concise Review" Nutrients 15, no. 24: 5031. https://doi.org/10.3390/nu15245031