
Discrepancies in Composition and Biological Effects of Different Formulations of Chondroitin Sulfate

Abstract
:1. Introduction
2. Chondroitin Sulfate
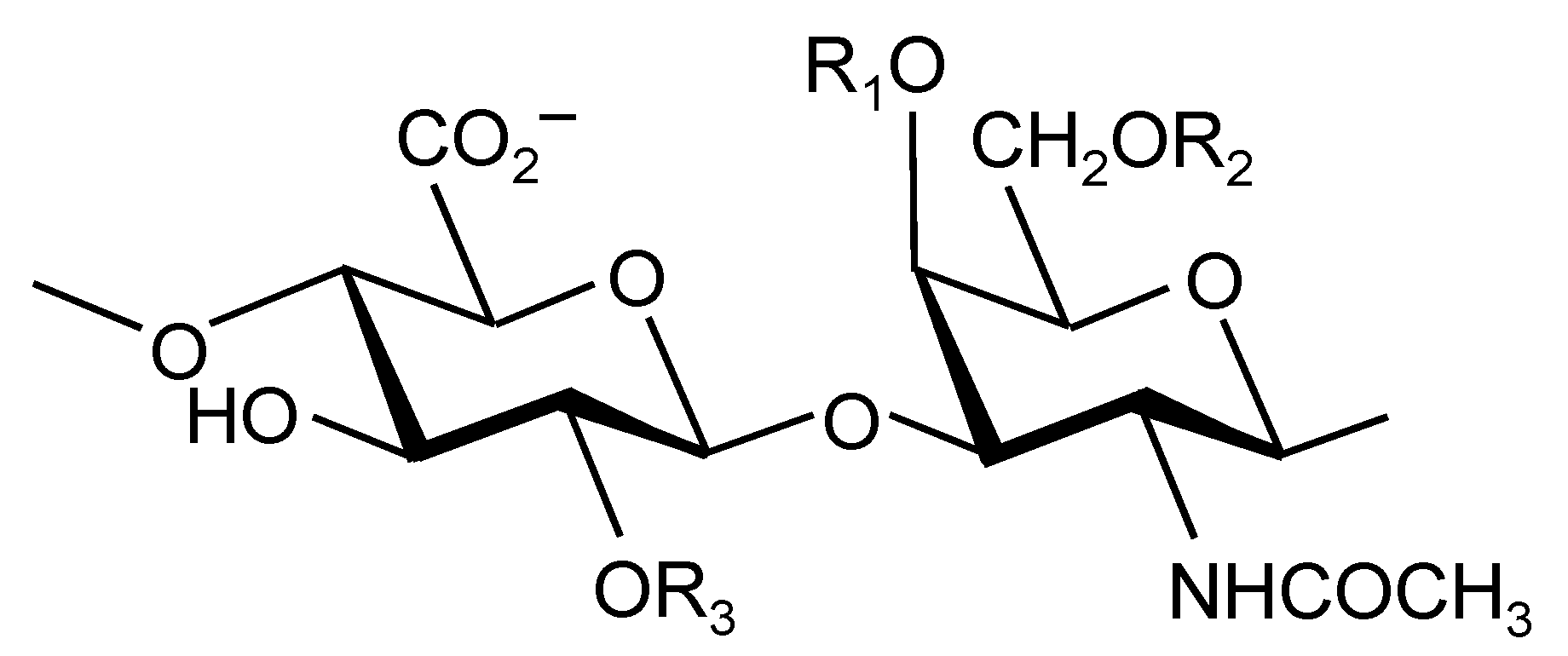
2.1. Structure

2.2. Production
2.3. Regulation
2.4. Content
2.5. Composition and Chemical Properties

{kind=link}
{kind=link}
| Characteristic | CS1 | CS2 | CS3 |
|---|---|---|---|
| Species | Porcine | Bovine | Bovine |
| Chondroitin sulfate content (%) | 90.4 | 96.2 | 99.9 |
| Molecular weight a (kDa) | 12.9 | 13.8 | 15.1 |
| Protein (%) | 7.4 | 3.3 | ND |
| Intrinsic viscosity (m3/kg) | 0.034 | 0.036 | 0.040 |
| Chlorides (%) | 0.70 | 0.02 | 0.34 |
| Free sulfates (%) | 0.75 | 0.05 | 0.14 |
| Oxalate (%) | 0.021 | ND | 0.01 |
| Sodium (%) | 7.10 | 6.75 | 7.05 |
| Non-sulfated chondroitin (%) | 5.9 | 5.1 | 5.7 |
| Chondroitin-4-sulfate (%) | 78.3 | 72.7 | 62.8 |
| Chondroitin-6-sulfate (%) | 15.8 | 21.3 | 31.5 |
| Chondroitin-2,6-disulfate (%) | ND | 0.4 | ND |
| Chondroitin-4,6-disulfate (%) | ND | 0.5 | ND |
2.6. Absorption, Bioavailability and Bioequivalence
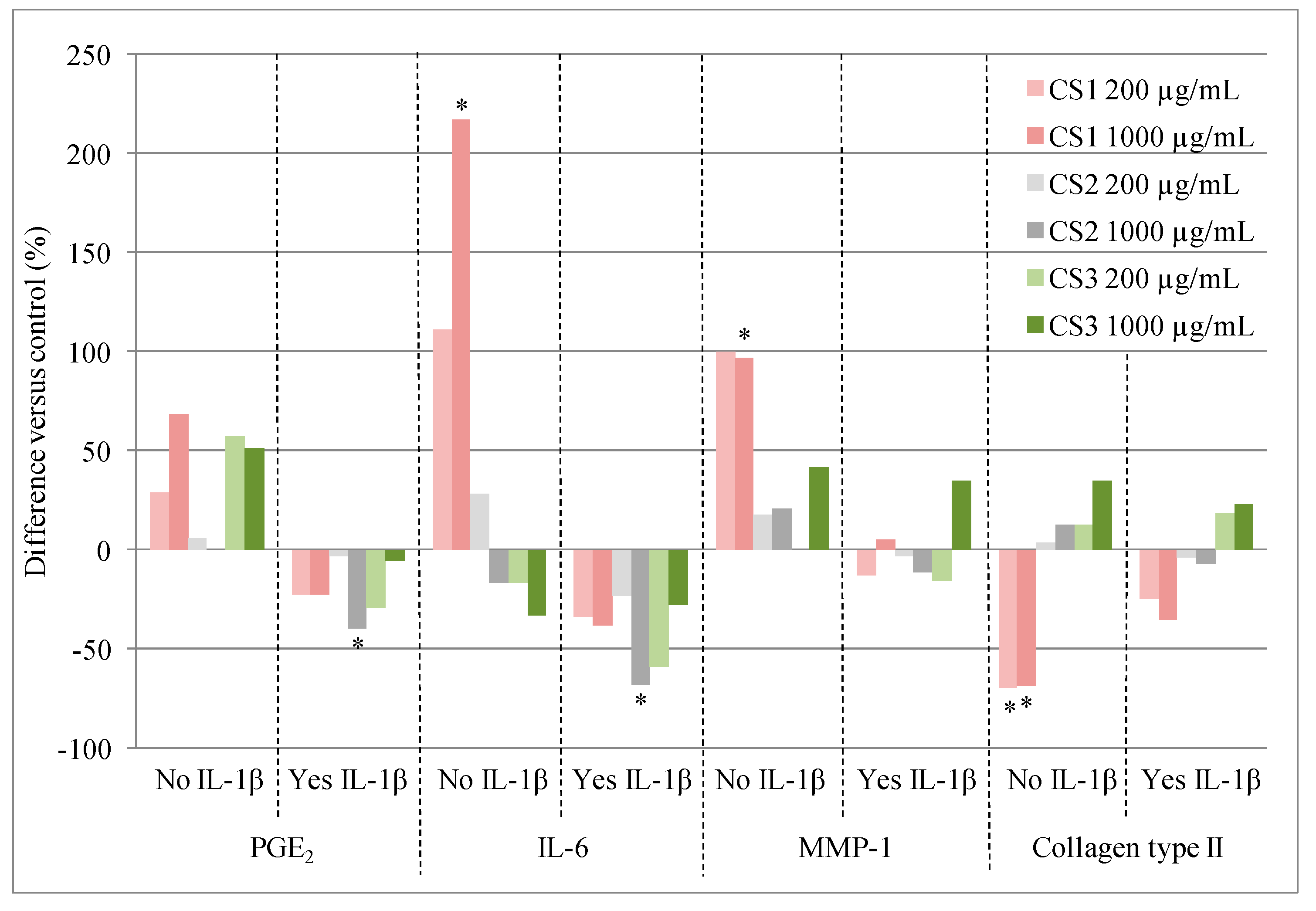
2.7. Biological Effects

2.8. Clinical Effects
2.9. Safety
3. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Conaghan, P.G.; Kloppenburg, M.; Schett, G.; Bijlsma, J.W. Osteoarthritis research priorities: A report from a EULAR ad hoc expert committee. Ann. Rheum. Dis. 2014, 73, 1442–1445. [Google Scholar]
- Bhatia, D.; Bejarano, T.; Novo, M. Current interventions in the management of knee osteoarthritis. J. Pharm. Bioallied Sci. 2013, 5, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Pereira, D.; Peleteiro, B.; Araujo, J.; Branco, J.; Santos, R.A.; Ramos, E. The effect of osteoarthritis definition on prevalence and incidence estimates: A systematic review. Osteoarthr. Cartil. 2011, 19, 1270–1285. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.; Chevalier, X.; Henrotin, Y.; Hunter, D.J.; Uebelhart, D. Symptom and structure modification in osteoarthritis with pharmaceutical-grade chondroitin sulfate: What’s the evidence? Curr. Med. Res. Opin. 2013, 29, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Doherty, M.; Arden, N.; Bannwarth, B.; Bijlsma, J.; Gunther, K.P.; Hauselmann, H.J.; Herrero-Beaumont, G.; Jordan, K.; Kaklamanis, P.; et al. EULAR evidence based recommendations for the management of hip osteoarthritis: Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis. 2005, 64, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Bruyere, O.; Cooper, C.; Pelletier, J.P.; Branco, J.; Luisa Brandi, M.; Guillemin, F.; Hochberg, M.C.; Kanis, J.A.; Kvien, T.K.; Martel-Pelletier, J.; et al. An algorithm recommendation for the management of knee osteoarthritis in Europe and internationally: A report from a task force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin. Arthritis Rheum. 2014, 44, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E.; Brandt, K.; Hawker, G.; Peeva, E.; Schreyer, E.; Tsuji, W.; Hochberg, M.C. OARSI-FDA initiative: Defining the disease state of osteoarthritis. Osteoarthr. Cartil. 2011, 19, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Lajeunesse, D.; Pelletier, J.P. Etiopathogenesis of osteoarthritis. In Arthritis and Allied Conditions. A Textbook of Rheumatology; Koopman, W.J., Moreland, L.W., Eds.; Lippincott, Williams & Wilkins: Baltimore, MA, USA, 2005; pp. 2199–2226. [Google Scholar]
- Osago, H.; Shibata, T.; Hara, N.; Kuwata, S.; Kono, M.; Uchio, Y.; Tsuchiya, M. Quantitative analysis of glycosaminoglycans, chondroitin/dermatan sulfate, hyaluronic acid, heparan sulfate, and keratan sulfate by liquid chromatography-electrospray ionization-tandem mass spectrometry. Anal. Biochem. 2014, 467, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Anower-E-Khuda, M.F.; Kimata, K. Human blood glycosaminoglycans: Isolation and analysis. Methods Mol. Biol. 2015, 1229, 95–103. [Google Scholar] [PubMed]
- Bannuru, R.R.; Vaysbrot, E.E.; Sullivan, M.C.; McAlindon, T.E. Relative efficacy of hyaluronic acid in comparison with NSAIDs for knee osteoarthritis: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 43, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Yamada, S.; Haslam, S.M.; Morris, H.R.; Dell, A.; Sugahara, K. Novel tetrasaccharides isolated from squid cartilage chondroitin sulfate E contain unusual sulfated disaccharide units GlcA(3-O-sulfate)beta1–3GalNAc(6-O-sulfate) or GlcA(3-O-sulfate)beta1–3GalNAc. J. Biol. Chem. 1997, 272, 19656–19665. [Google Scholar] [CrossRef] [PubMed]
- Sugahara, K.; Tanaka, Y.; Yamada, S.; Seno, N.; Kitagawa, H.; Haslam, S.M.; Morris, H.R.; Dell, A. Novel sulfated oligosaccharides containing 3-O-sulfated glucuronic acid from king crab cartilage chondroitin sulfate K. Unexpected degradation by chondroitinase ABC. J. Biol. Chem. 1996, 271, 26745–26754. [Google Scholar] [CrossRef] [PubMed]
- Volpi, N. Quality of different chondroitin sulfate preparations in relation to their therapeutic activity. J. Pharm. Pharmacol. 2009, 61, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Tat, S.K.; Pelletier, J.P.; Mineau, F.; Duval, N.; Martel-Pelletier, J. Variable effects of 3 different chondroitin sulfate compounds on human osteoarthritic cartilage/chondrocytes: Relevance of purity and production process. J. Rheumatol. 2010, 37, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Volpi, N. Analytical aspects of pharmaceutical grade chondroitin sulfates. J. Pharm. Sci. 2007, 96, 3168–3180. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, J.G.; Fye, C.L.; Williams, D.W.; Reda, D.J.; Harris, C.L.; Clegg, D.O. Chondroitin product selection for the glucosamine/chondroitin arthritis intervention trial. J. Am. Pharm. Assoc. 2006, 46, 14–24. [Google Scholar] [CrossRef]
- Tat, S.K.; Pelletier, J.P.; Vergés, J.; Lajeunesse, D.; Montell, E.; Fahmi, H.; Lavigne, M.; Martel-Pelletier, J. Chondroitin and glucosamine sulfate in combination decrease the pro-resorptive properties of human osteoarthritis subchondral bone osteoblasts: A basic science study. Arthritis Res. Ther. 2007, 9, R117. [Google Scholar] [CrossRef] [PubMed]
- Lauder, R.M. Chondroitin sulphate: A complex molecule with potential impacts on a wide range of biological systems. Complement. Ther. Med. 2009, 17, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Calamia, V.; Fernandez-Puente, P.; Mateos, J.; Lourido, L.; Rocha, B.; Montell, E.; Vergés, J.; Ruiz-Romero, C.; Blanco, F.J. Pharmacoproteomic study of three different chondroitin sulfate compounds on intracellular and extracellular human chondrocyte proteomes. Mol. Cell. Proteomics 2012, 11, M111.013417. [Google Scholar] [CrossRef] [PubMed]
- Co-ordination Group for Mutual Recognition and Decentralised Procedures—Human (CMDh). Overview of Biological Active Substances of Non-Recombinant Origin. Available online: http://www.hma.eu/fileadmin/dateien/Human_Medicines/CMD_h_/procedural_guidance/Compilation_Biological_Active_Substance_non-recombinant_origin.pdf (accessed on 21 November 2014).
- Adebowale, A.O.; Cox, D.S.; Liang, Z.; Eddington, N.D. Chondroitin sulfate content in marketed products and the Caco-2 permeability of chondroitin sulfate raw materials. JANA 2000, 3, 37–44. [Google Scholar]
- Sakai, S.; Otake, E.; Toida, T.; Goda, Y. Identification of the origin of chondroitin sulfate in “health foods”. Chem. Pharm. Bull (Tokyo) 2007, 55, 299–303. [Google Scholar] [CrossRef]
- Malavaki, C.J.; Asimakopoulou, A.P.; Lamari, F.N.; Theocharis, A.D.; Tzanakakis, G.N.; Karamanos, N.K. Capillary electrophoresis for the quality control of chondroitin sulfates in raw materials and formulations. Anal. Biochem. 2008, 374, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Volpi, N. Oral bioavailability of chondroitin sulfate (Condrosulf) and its constituents in healthy male volunteers. Osteoarthr. Cartil. 2002, 10, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Ronca, F.; Palmieri, L.; Panicucci, P.; Ronca, G. Anti-inflammatory activity of chondroitin sulfate. Osteoarthr. Cartil. 1998, 6, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Barthe, L.; Woodley, J.; Lavit, M.; Przybylski, C.; Philibert, C.; Houin, G. In vitro intestinal degradation and absorption of chondroitin sulfate, a glycosaminoglycan drug. Arzneim.-Forsch. 2004, 54, 286–292. [Google Scholar]
- Vergés, J.; Castaneda-Hernandez, G. On the bioavailability of oral chondroitin sulfate formulations: Proposed criteria for bioequivalence studies. Proc. West Pharmacol. Soc. 2004, 47, 50–53. [Google Scholar] [PubMed]
- Murrieta, F.J.F.; Castaneda, G.; Medina Santillan, R. Biodisponibilidad y Bioequivalencia en los Medicamentos Genericos: Bases clínicas, analiticas y estadísticas; Medina Santillan, R., Ed.; Asclepios XXI: Puebla, Mexico, 2002; p. 80. [Google Scholar]
- Du Souich, P.; Vergés, J. Simple approach to predict the maximal effect elicited by a drug when plasma concentrations are not available or are dissociated from the effect, as illustrated with chondroitin sulfate data. Clin. Pharmacol. Ther. 2001, 70, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Monfort, J.; Pelletier, J.P.; Garcia-Giralt, N.; Martel-Pelletier, J. Biochemical basis of the effect of chondroitin sulphate on osteoarthritis articular tissues. Ann. Rheum. Dis. 2008, 67, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Du Souich, P. Absorption, distribution and mechanism of action of SYSADOAS. Pharmacol. Ther. 2014, 142, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Au, R.Y.; Phan, P.V.; Au, A.Y.; Frondoza, C.G. Effect of different chondroitin sulfate raw materials on pro-inflammatory gene expression in chondrocytes and monocytes. In Proceediongs of the 6th Symposium of ICRSl; San Diego, CA, USA: 8–11 January 2006.
- Cantley, M.D.; Rainsford, K.D.; Haynes, D.R. Comparison of the ability of chondroitin sulfate derived from bovine, fish and pigs to suppress human osteoclast activity in vitro. Inflammopharmacology 2013, 21, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Kwan Tat, S.; Pelletier, J.P.; Lajeunesse, D.; Fahmi, H.; Lavigne, M.; Martel-Pelletier, J. The differential expression of osteoprotegerin (OPG) and receptor activator of nuclear factor kappaB ligand (RANKL) in human osteoarthritic subchondral bone osteoblasts is an indicator of the metabolic state of these disease cells. Clin. Exp. Rheumatol. 2008, 26, 295–304. [Google Scholar] [PubMed]
- Miyazaki, T.; Miyauchi, S.; Tawada, A.; Anada, T.; Suzuki, O. Effect of chondroitin sulfate-E on the osteoclastic differentiation of RAW264 cells. Dent. Mater. J. 2010, 29, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Leeb, B.F.; Schweitzer, H.; Montag, K.; Smolen, J.S. A metaanalysis of chondroitin sulfate in the treatment of osteoarthritis. J. Rheumatol. 2000, 27, 205–211. [Google Scholar] [PubMed]
- McAlindon, T.E.; LaValley, M.P.; Gulin, J.P.; Felson, D.T. Glucosamine and chondroitin for treatment of osteoarthritis: A systematic quality assessment and meta-analysis. JAMA 2000, 283, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Richy, F.; Bruyere, O.; Ethgen, O.; Cucherat, M.; Henrotin, Y.; Reginster, J.Y. Structural and symptomatic efficacy of glucosamine and chondroitin in knee osteoarthritis: A comprehensive meta-analysis. Arch. Intern. Med. 2003, 163, 1514–1522. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Zhan, M.; Langenberg, P. The rate of decline of joint space width in patients with osteoarthritis of the knee: A systematic review and meta-analysis of randomized placebo-controlled trials of chondroitin sulfate. Curr. Med. Res. Opin. 2008, 24, 3029–3035. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Structure-modifying effects of chondroitin sulfate in knee osteoarthritis: An updated meta-analysis of randomized placebo-controlled trials of 2-year duration. Osteoarthr. Cartil. 2010, 18 (Suppl. 1), S28–S31. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Woo, J.H.; Choi, S.J.; Ji, J.D.; Song, G.G. Effect of glucosamine or chondroitin sulfate on the osteoarthritis progression: A meta-analysis. Rheumatol. Int. 2010, 30, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Maheu, E.; Cucherat, M. Symptom-modifying effect of chondroitin sulfate in knee osteoarthritis: A meta-analysis of randomized placebo-controlled trials performed with Structum®. Open Rheumatol. J. 2012, 6, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Wildi, L.M.; Raynauld, J.P.; Martel-Pelletier, J.; Beaulieu, A.; Bessette, L.; Morin, F.; Abram, F.; Dorais, M.; Pelletier, J.P. Chondroitin sulphate reduces both cartilage volume loss and bone marrow lesions in knee osteoarthritis patients starting as early as 6 months after initiation of therapy: A randomised, double-blind, placebo-controlled pilot study using MRI. Ann. Rheum. Dis. 2011, 70, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Raynauld, J.-P.; Martel-Pelletier, J.; Dorais, M.; Haraoui, B.; Choquette, D.; Abram, F.; Beaulieu, A.; Bessette, L.; Morin, F.; Wildi, L.M.; et al. Total knee replacement as a knee osteoarthritis outcome: Predictors derived from a 4-year long-term observation following a randomized clinical trial using chondroitin sulfate. Cartilage 2013, 4, 291–226. [Google Scholar] [CrossRef]
- Prieto-Alhambra, D.; Morros, R.; Arden, N. Association between chondroitin sulphate use and the risk of total knee artrhoplasty in osteoarthitis patients: A propensity-score matched cohort study. Basic Clin. Pharmacol. Toxicol. 2013, 113, 34. [Google Scholar]
- Reichenbach, S.; Sterchi, R.; Scherer, M.; Trelle, S.; Burgi, E.; Burgi, U.; Dieppe, P.A.; Juni, P. Meta-analysis: Chondroitin for osteoarthritis of the knee or hip. Ann. Intern. Med. 2007, 146, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Wandel, S.; Juni, P.; Tendal, B.; Nuesch, E.; Villiger, P.M.; Welton, N.J.; Reichenbach, S.; Trelle, S. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: Network meta-analysis. BMJ 2010, 341, c4675. [Google Scholar] [CrossRef] [PubMed]
- Henrotin, Y.E. Interpretation of metaanalyses: Pitfalls should be more widely recognized. J. Rheumatol. 2012, 39, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Rainsford, K.D. Importance of pharmaceutical composition and evidence from clinical trials and pharmacological studies in determining effectiveness of chondroitin sulphate and other glycosaminoglycans: A critique. J. Pharm. Pharmacol. 2009, 61, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Clegg, D.O.; Reda, D.J.; Harris, C.L.; Klein, M.A.; O’Dell, J.R.; Hooper, M.M.; Bradley, J.D.; Bingham, C.O., 3rd; Weisman, M.H.; Jackson, C.G.; et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N. Engl. J. Med. 2006, 354, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Hathcock, J.N.; Shao, A. Risk assessment for glucosamine and chondroitin sulfate. Regul. Toxicol. Pharmacol. 2007, 47, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, T.K.; Viswanathan, K.; Ganguly, T.; Elankumaran, S.; Smith, S.; Pelzer, K.; Lansing, J.C.; Sriranganathan, N.; Zhao, G.; Galcheva-Gargova, Z.; et al. Contaminated heparin associated with adverse clinical events and activation of the contact system. N. Engl. J. Med. 2008, 358, 2457–2467. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, M.; Beccati, D.; Shriver, Z.; Naggi, A.; Viswanathan, K.; Bisio, A.; Capila, I.; Lansing, J.C.; Guglieri, S.; Fraser, B.; et al. Oversulfated chondroitin sulfate is a contaminant in heparin associated with adverse clinical events. Nat. Biotechnol. 2008, 26, 669–675. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martel-Pelletier, J.; Farran, A.; Montell, E.; Vergés, J.; Pelletier, J.-P. Discrepancies in Composition and Biological Effects of Different Formulations of Chondroitin Sulfate. Molecules 2015, 20, 4277-4289. https://doi.org/10.3390/molecules20034277
Martel-Pelletier J, Farran A, Montell E, Vergés J, Pelletier J-P. Discrepancies in Composition and Biological Effects of Different Formulations of Chondroitin Sulfate. Molecules. 2015; 20(3):4277-4289. https://doi.org/10.3390/molecules20034277
Chicago/Turabian StyleMartel-Pelletier, Johanne, Aina Farran, Eulàlia Montell, Josep Vergés, and Jean-Pierre Pelletier. 2015. "Discrepancies in Composition and Biological Effects of Different Formulations of Chondroitin Sulfate" Molecules 20, no. 3: 4277-4289. https://doi.org/10.3390/molecules20034277
APA StyleMartel-Pelletier, J., Farran, A., Montell, E., Vergés, J., & Pelletier, J.-P. (2015). Discrepancies in Composition and Biological Effects of Different Formulations of Chondroitin Sulfate. Molecules, 20(3), 4277-4289. https://doi.org/10.3390/molecules20034277