Alterations in Pharmacokinetics of Gemcitabine and Erlotinib by Concurrent Administration of Hyangsayukgunja-Tang, a Gastroprotective Herbal Medicine

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
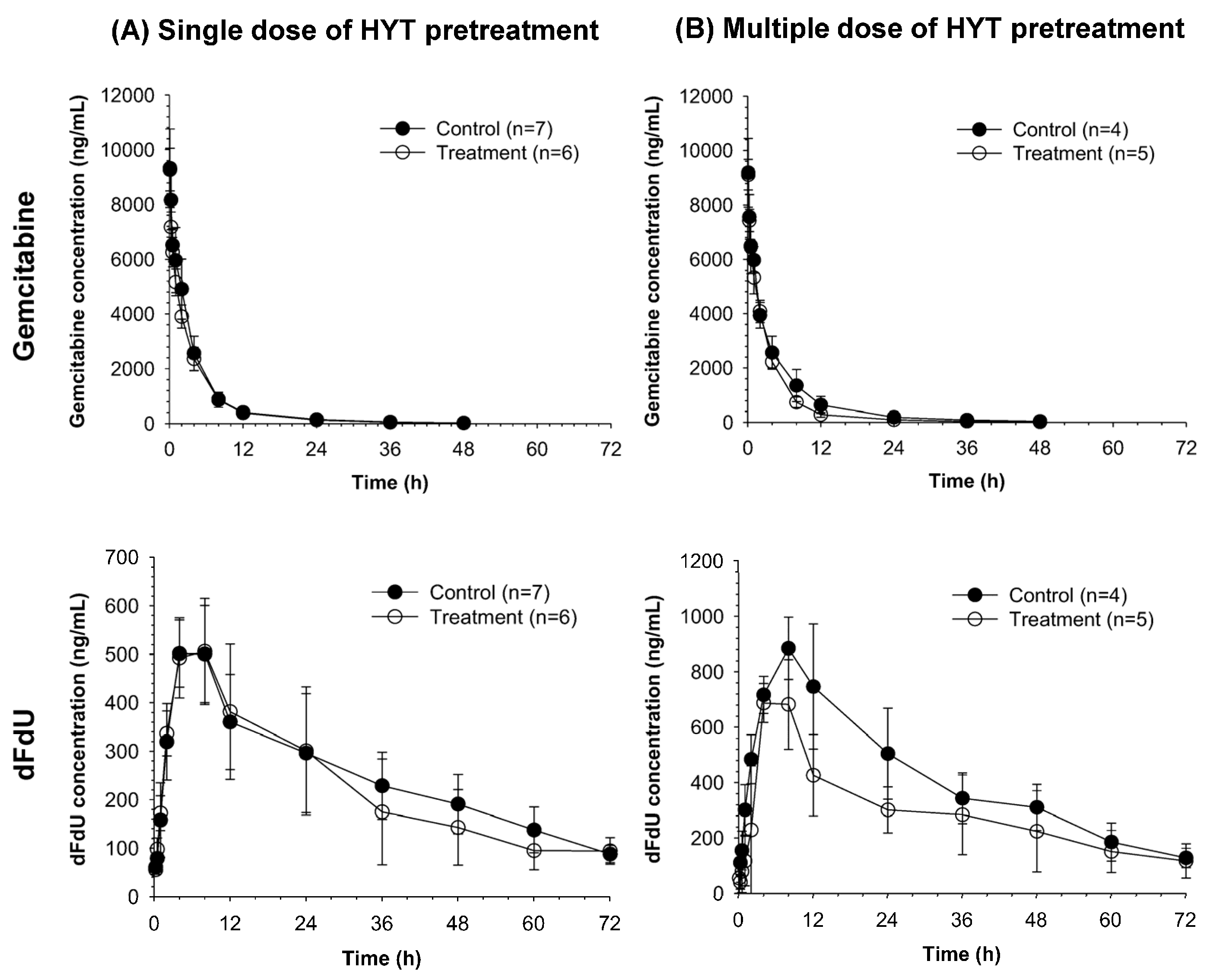
2.1. Pharmacokinetics of Gemcitabine and Its Metabolite dFdU in Rats Pretreated with HYT
2.2. Pharmacokinetics of Erlotinib and Its Metabolites OSI-420 and OSI-413 in Rats Pretreated with HYT
2.3. Pharmacokinetic Modeling
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Animal Study
4.3. LC-MS/MS
4.4. Non-Compartmental Pharmacokinetic Analysis
4.5. Pharmacokinetic Modeling
4.6. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Louvet, C.; Labianca, R.; Hammel, P.; Lledo, G.; Zampino, M.G.; Andre, T.; Zaniboni, A.; Ducreux, M.; Aitini, E.; Taieb, J.; et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: Results of a gercor and giscad phase III trial. J. Clin. Oncol. 2005, 23, 3509–3516. [Google Scholar] [CrossRef] [PubMed]
- Oberstein, P.E.; Olive, K.P. Pancreatic cancer: Why is it so hard to treat? Ther. Adv. Gastroenterol. 2013, 6, 321–337. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A., ІІІ; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [PubMed]
- Hochster, H.S.; Haller, D.G.; de Gramont, A.; Berlin, J.D.; Philip, P.A.; Moore, M.J.; Ajani, J.A. Consensus report of the international society of gastrointestinal oncology on therapeutic progress in advanced pancreatic cancer. Cancer 2006, 107, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Bria, E.; Milella, M.; Gelibter, A.; Cuppone, F.; Pino, M.S.; Ruggeri, E.M.; Carlini, P.; Nistico, C.; Terzoli, E.; Cognetti, F.; et al. Gemcitabine-based combinations for inoperable pancreatic cancer: Have we made real progress? A meta-analysis of 20 phase 3 trials. Cancer 2007, 110, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the national cancer institute of canada clinical trials group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Ansari, D.; Andersson, R.; Wu, D.Q. Does gemcitabine-based combination therapy improve the prognosis of unresectable pancreatic cancer? World J. Gastroenterol. 2012, 18, 4944–4958. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Park, C.M.; Kwon, H.; Lee, K.H. Erlotinib plus gemcitabine versus gemcitabine for pancreatic cancer: Real-world analysis of korean national database. BMC Cancer 2016, 16, 443. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.Y.; Yuan, J.Q.; Di, M.Y.; Zheng, D.Y.; Chen, J.Z.; Ding, H.; Wu, X.Y.; Huang, Y.F.; Mao, C.; Tang, J.L. Gemcitabine plus erlotinib for advanced pancreatic cancer: A systematic review with meta-analysis. PLoS ONE 2013, 8, e57528. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). Assessment Report for Tarceva; EMA: London, UK, 2010. [Google Scholar]
- Hamilton, M.; Wolf, J.L.; Zborowski, D.; Lu, J.; Lum, B.L.; Ding, K.; Clark, G.M.; Rakhit, A.; Seymour, L.; Ptaszynski, A.M.; et al. Tarceva™ (erlotinib) exposure/effects (EE) analysis from a phase III study in advanced nsclc: Effect of smoking on the pk of erlotinib. Cancer Res. 2005, 65, 1451. [Google Scholar]
- Iyer, R.; Bharthuar, A. A review of erlotinib—An oral, selective epidermal growth factor receptor tyrosine kinase inhibitor. Expert Opin. Pharmacother. 2010, 11, 311–320. [Google Scholar] [CrossRef] [PubMed]
- U.S. FDA. FDA Approval for Erlotinib Hydrochloride; FDA: Silver Spring, MD, USA, 2013.
- Bent, S. Herbal medicine in the united states: Review of efficacy, safety, and regulation: Grand rounds at university of California, San Francisco medical center. J. Gen. Intern. Med. 2008, 23, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Brantley, S.J.; Argikar, A.A.; Lin, Y.S.; Nagar, S.; Paine, M.F. Herb-drug interactions: Challenges and opportunities for improved predictions. Drug Metab. Dispos. 2014, 42, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Liu, K. Pharmacokinetic interactions between herbal medicines and prescribed drugs: Focus on drug metabolic enzymes and transporters. Curr. Drug Metab. 2014, 15, 791–807. [Google Scholar] [CrossRef] [PubMed]
- Seo, C.S.; Shin, H.K. Quantitative analysis of Hyangsayukgunja-tang using an ultra-performance liquid chromatography coupled to electrospray ionization tandem mass spectrometry. Korean J. Pharmacogn. 2015, 46, 352–364. [Google Scholar]
- Oriental Medicine Advanced Searching Integrated System (OASIS): Hyangsayukgunja-Tang. Available online: http://oasis.kiom.re.kr/oasis/pres/prdetailView2.jsp?idx=31&selectname=%ED%96%A5%EC%82%AC%EC%9C%A1%EA%B5%B0%EC%9E%90%ED%83%95&srch_menu_nix=null (accessed on 28 August 2017).
- Kong, K.H.; Baik, T.H. The effects of Hyangsayukgunja-tang extract on indomethacin-induced gatric mucosal lesions. J. Intern. Korean Med. 2001, 22, 589–599. [Google Scholar]
- Chang, H.Y.; Kang, Y.H. The effects of hyang-sa-yuk-gun-ja-tang and oh-pe-san on the gastric mucosal repair. J. Dong Guk Orient. Med. 1993, 2, 127–137. [Google Scholar]
- Jeong, Y. Hyangsayukgunja-Tang Increases Appetite and Affects Gut Hormones; Kyung-Hee University: Seoul, Korea, 2011. [Google Scholar]
- Li, X. Study on anti-inflammation and analgesia of Xiangshaliujun granule. J. Luzhou Med. Coll. 2005, 28, 409–411. [Google Scholar]
- Xiao, Y.; Liu, Y.Y.; Yu, K.Q.; Ouyang, M.Z.; Luo, R.; Zhao, X.S. Chinese herbal medicine liu jun zi tang and xiang sha liu jun zi tang for functional dyspepsia: Meta-analysis of randomized controlled trials. Evid. Based Complement. Alternat. Med. 2012, 2012, 936459. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, T.; Li, W. Effects of xiang sha liu jun zi tang and its component on contractile activity of isolated gastric muscle strips in rats. J. Lanzhou Med. Coll. 1999, 25, 1–3. [Google Scholar]
- Jeong, M.J.; Lyu, S.A.; Lee, S.Y. Effects of the hyangsayukgunjatang gamibang on children with abdominal pain. J. Korean Orient. Pediatr. 2007, 21, 57–69. [Google Scholar]
- Ye, H.M.; Lin, N.; Xiao, L.Y. Antioxidant activity of xiangsha liujun pill in hyperlipidemia model rats. China Pharm. 2008, 24, 013. [Google Scholar]
- Gemzar® (Gemcitabine HCL). Available online: https://pi.lilly.com/us/gemzar.pdf (accessed on 28 August 2017).
- Kim, T.H.; Park, G.Y.; Shin, S.; Kwon, D.R.; Seo, W.S.; Shin, J.C.; Choi, J.H.; Joo, S.H.; Weon, K.Y.; Min, B.S.; et al. Pharmacokinetic alteration of baclofen by multiple oral administration of herbal medicines in rats. Evid. Based Complement. Alternat. Med. 2014, 2014, 402126. [Google Scholar] [CrossRef] [PubMed]
- Oga, E.F.; Sekine, S.; Shitara, Y.; Horie, T. Pharmacokinetic herb-drug interactions: Insight into mechanisms and consequences. Eur. J. Drug Metab. Pharmacokinet. 2016, 41, 93–108. [Google Scholar] [CrossRef] [PubMed]
- Ting, C.T.; Cheng, Y.Y.; Tsai, T.H. Herb-drug interaction between the traditional hepatoprotective formulation and sorafenib on hepatotoxicity, histopathology and pharmacokinetics in rats. Molecules 2017, 22, 1034. [Google Scholar] [CrossRef] [PubMed]
- Clinical Research Information Service. Available online: https://cris.nih.go.kr/cris/search/search_result_st01.jsp?seq=4708 (accessed on 28 August 2017).
- Signor, L.; Varesio, E.; Staack, R.F.; Starke, V.; Richter, W.F.; Hopfgartner, G. Analysis of erlotinib and its metabolites in rat tissue sections by maldi quadrupole time-of-flight mass spectrometry. J. Mass Spectrom. 2007, 42, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.; Wolf, J.L.; Rusk, J.; Beard, S.E.; Clark, G.M.; Witt, K.; Cagnoni, P.J. Effects of smoking on the pharmacokinetics of erlotinib. Clin. Cancer Res. 2006, 12, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Shin, H.M. Antioxidant effects of gami hyang sa yuk gun ja tang against gastric mucosal lesions iduced by indomethacin. J. Korean Med. 1998, 19, 165–178. [Google Scholar]
Sample Availability: Samples of the compounds are not available from the authors. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Single Dose | Multiple Doses | |||
|---|---|---|---|---|---|
| Control (n = 7) | HYT (n = 6) | Control (n = 4) | HYT (n = 5) | ||
| Gemcitabine | t1/2 (h) | 7.9 ± 1.2 | 9.8 ± 0.8 * | 12.1 ± 2.1 | 10.6 ± 2.4 |
| C0 (ng/mL) | 10,067.5 ± 2101.4 | 10,562.9 ± 1241.2 | 10,163.2 ± 1938.0 | 10,098.7 ± 820.5 | |
| AUCall (ng·h/mL) | 34,684.2 ± 6088.4 | 30,934.6 ± 4475.8 | 37,842.2 ± 9170.3 | 29,383.8 ± 3473.1 | |
| AUCinf (ng·h/mL) | 34,931.4 ± 6017.6 | 31,222.8 ± 4518.1 | 38,585.6 ± 9292.4 | 29,705.9 ± 3561.8 | |
| Vz/F (L/kg) | 3.4 ± 0.9 | 4.6 ± 1.0 * | 4.9 ± 2.0 | 5.2 ± 1.4 | |
| CL/F (mL/min/kg) | 4.9 ± 1.0 | 5.4 ± 0.8 | 4.5 ± 1.1 | 5.7 ± 0.7 | |
| Vss (L/kg) | 1.7 ± 0.3 | 1.9 ± 0.1 | 2.1 ± 0.3 | 1.9 ± 0.1 | |
| dFdU | t1/2 (h) | 29.2 ± 7.2 | 41.5 ± 28.6 | 24.4 ± 3.9 | 29.6 ± 5.7 |
| Tmax (h) | 6.3 ± 3.1 | 7.3 ± 3.0 | 9.0 ± 2.0 | 5.6 ± 2.2 * | |
| Cmax (ng/mL) | 550.7 ± 68.1 | 538.3 ± 93.9 | 885 ± 112.5 | 722 ± 141.8 | |
| AUCall (ng·h/mL) | 16,597.2 ± 2484 | 16,228.1 ± 5943.2 | 27,104.5 ± 2154.8 | 20,919.8 ± 7518.3 | |
| AUCinf (ng·h/mL) | 22,137.7 ± 5022.7 | 21,221.6 ± 6950.8 | 35,453.2 ± 7118.4 | 25,824.8 ± 9709 | |
| AUCmeta/AUCparent | 0.64 ± 0.14 | 0.67 ± 0.18 | 0.74 ± 0.14 | 0.70 ± 0.17 | |
| Parameter | Single Dose | Multiple Doses | |||
|---|---|---|---|---|---|
| Control (n = 7) | HYT (n = 6) | Control (n = 4) | HYT (n = 5) | ||
| Erlotinib | t1/2 (h) | 5.9 ± 4.0 | 5.3 ± 2.6 | 4.3 ± 1.8 | 6.8 ± 3.5 |
| Tmax (h) | 0.8 ± 0.4 | 1.1 ± 0.5 | 1.0 ± 0.0 | 1.5 ± 0.7 | |
| Cmax (ng/mL) | 2653.8 ± 760.3 | 3092 ± 1142.4 | 2484.5 ± 797.4 | 2449.3 ± 1390 | |
| AUCall (ng·h/mL) | 11,544.5 ± 2210.6 | 13,419.5 ± 2713.9 | 14,218.5 ± 3731.5 | 12,422.6 ± 1026.3 | |
| AUCinf (ng·h/mL) | 11,811.6 ± 2211.8 | 13,517 ± 2678.2 | 14,237.8 ± 3737.1 | 12,509.4 ± 1022.4 | |
| CL/F (mL/min/kg) | 14.5 ± 9.8 | 12.1 ± 7.1 | 9.1 ± 3.2 | 15.7 ± 7.4 | |
| Vz/F (L/kg) | 29.1 ± 5.5 | 25.7 ± 6.5 | 24.7 ± 6.6 | 26.8 ± 2.4 | |
| OSI-420 | t1/2 (h) | 6.8 ± 4.5 | 3.9 ± 2.2 | 3.6 ± 0.8 | 5.9 ± 4.0 |
| Tmax (h) | 2.0 ± 0.0 | 2.3 ± 0.8 | 4.8 ± 3.8 | 3.7 ± 2.8 | |
| Cmax (ng/mL) | 202.3 ± 87.1 | 238.1 ± 88.7 | 167.3 ± 44.7 | 114.7 ± 15.6 * | |
| AUCall (ng·h/mL) | 1553.3 ± 386.7 | 1568.5 ± 393.2 | 1666.5 ± 663.4 | 865 ± 223.8 * | |
| AUCinf (ng·h/mL) | 1598.6 ± 368.3 | 1617.4 ± 410.2 | 1689.9 ± 662 | 955.6 ± 171.5 | |
| AUCmeta/AUCparent | 0.14 ± 0.03 | 0.12 ± 0.02 | 0.12 ± 0.03 | 0.08 ± 0.01 * | |
| OSI-413 | t1/2 (hr) | 7.1 ± 5.8 | 5.8 ± 2.7 | 5.6 ± 1.4 | 5.7 ± 0.9 |
| Tmax (hr) | 2.9 ± 2.3 | 3.3 ± 2.4 | 4.8 ± 3.8 | 3.7 ± 2.8 | |
| Cmax (ng/mL) | 1164.6 ± 493.7 | 1349.3 ± 508.9 | 1039 ± 259.7 | 649.4 ± 115.6 * | |
| AUCall (ng·h/mL) | 10,044.5 ± 3162.8 | 10,300.6 ± 3230.6 | 11,199.6 ± 3637.9 | 5671.4 ± 1018.4 * | |
| AUCinf (ng·h/mL) | 10,196.9 ± 2995.2 | 10,334.4 ± 3228.5 | 11,219.4 ± 3647.3 | 5697.5 ± 1007.6 * | |
| AUCmeta/AUCparent | 0.88 ± 0.28 | 0.83 ± 0.27 | 0.82 ± 0.17 | 0.47 ± 0.07 * | |
| Parameter | Symbol | Unit | Population Mean (BSV) |
|---|---|---|---|
| Absorption rate constant for erlotinib | ka | 1/h | 1.14 (0.81) |
| Absorption lag time for erlotinib | Tlag | h | 0.155 (0.777) |
| Clearance for erlotinib | CLerlotinib/F | L/h/kg | 1.5 (0.148) |
| Fraction of erlotinib clearance for metabolite formation | Fmet | - | 0.1 |
| Clearance for OSI-420 in control group | CLOSI420,con/F | L/h/kg | 0.182 (0.174) |
| Clearance for OSI-420 in HYT pretreatment group | CLOSI420,HYT/F | L/h/kg | 0.35 (0.122) |
| Clearance for OSI-413 in control group | CLOSI413,con/F | L/h/kg | 1.18 (0.257) |
| Clearance for OSI-413 in HYT pretreatment group | CLOSI413,HYT/F | L/h/kg | 2.22 (0.163) |
| Distribution clearance for erlotinib | CLDerlotinib/F | L/h/kg | 2.68 (0.655) |
| Distribution clearance for OSI-420 | CLDOSI420/F | L/h/kg | 4.51 (0.0598) |
| Distribution clearance for OSI-413 | CLDOSI413/F | L/h/kg | 0.943 (0.0244) |
| Central volume of distribution for erlotinib | V1,erlotinib/F | L/kg | 3.97 (0.0473) |
| Peripheral volume of distribution for erlotinib | V2,erlotinib/F | L/kg | 3.91 (0.554) |
| Central volume of distribution for OSI-420 | V1,OSI420/F | L/kg | 0.0278 (0.316) |
| Peripheral volume of distribution for OSI-420 | V2,OSI420/F | L/kg | 1.88 (0.047) |
| Central volume of distribution for OSI-413 | V1,OSI413/F | L/kg | 0.00235 (0.359) |
| Peripheral volume of distribution for OSI-413 | V2,OSI413/F | L/kg | 0.4 (0.0394) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.H.; Shin, S.; Kim, S.; Bulitta, J.B.; Weon, K.-Y.; Joo, S.H.; Ma, E.; Yoo, S.D.; Park, G.-Y.; Kwon, D.R.; et al. Alterations in Pharmacokinetics of Gemcitabine and Erlotinib by Concurrent Administration of Hyangsayukgunja-Tang, a Gastroprotective Herbal Medicine. Molecules 2017, 22, 1515. https://doi.org/10.3390/molecules22091515
Kim TH, Shin S, Kim S, Bulitta JB, Weon K-Y, Joo SH, Ma E, Yoo SD, Park G-Y, Kwon DR, et al. Alterations in Pharmacokinetics of Gemcitabine and Erlotinib by Concurrent Administration of Hyangsayukgunja-Tang, a Gastroprotective Herbal Medicine. Molecules. 2017; 22(9):1515. https://doi.org/10.3390/molecules22091515
Chicago/Turabian StyleKim, Tae Hwan, Soyoung Shin, Sarah Kim, Jürgen B. Bulitta, Kwon-Yeon Weon, Sang Hoon Joo, Eunsook Ma, Sun Dong Yoo, Gi-Young Park, Dong Rak Kwon, and et al. 2017. "Alterations in Pharmacokinetics of Gemcitabine and Erlotinib by Concurrent Administration of Hyangsayukgunja-Tang, a Gastroprotective Herbal Medicine" Molecules 22, no. 9: 1515. https://doi.org/10.3390/molecules22091515