Elevated Peripheral Blood Plasma Concentrations of Tie-2 and Angiopoietin 2 in Patients with Neuroendocrine Tumors


Abstract
:Background
Methods
Results
Conclusions
1. Introduction
2. Results and Discussion
2.1. Patients
2.1.1. Angiogenic Factors Levels in Patients with NETs and Healthy Controls
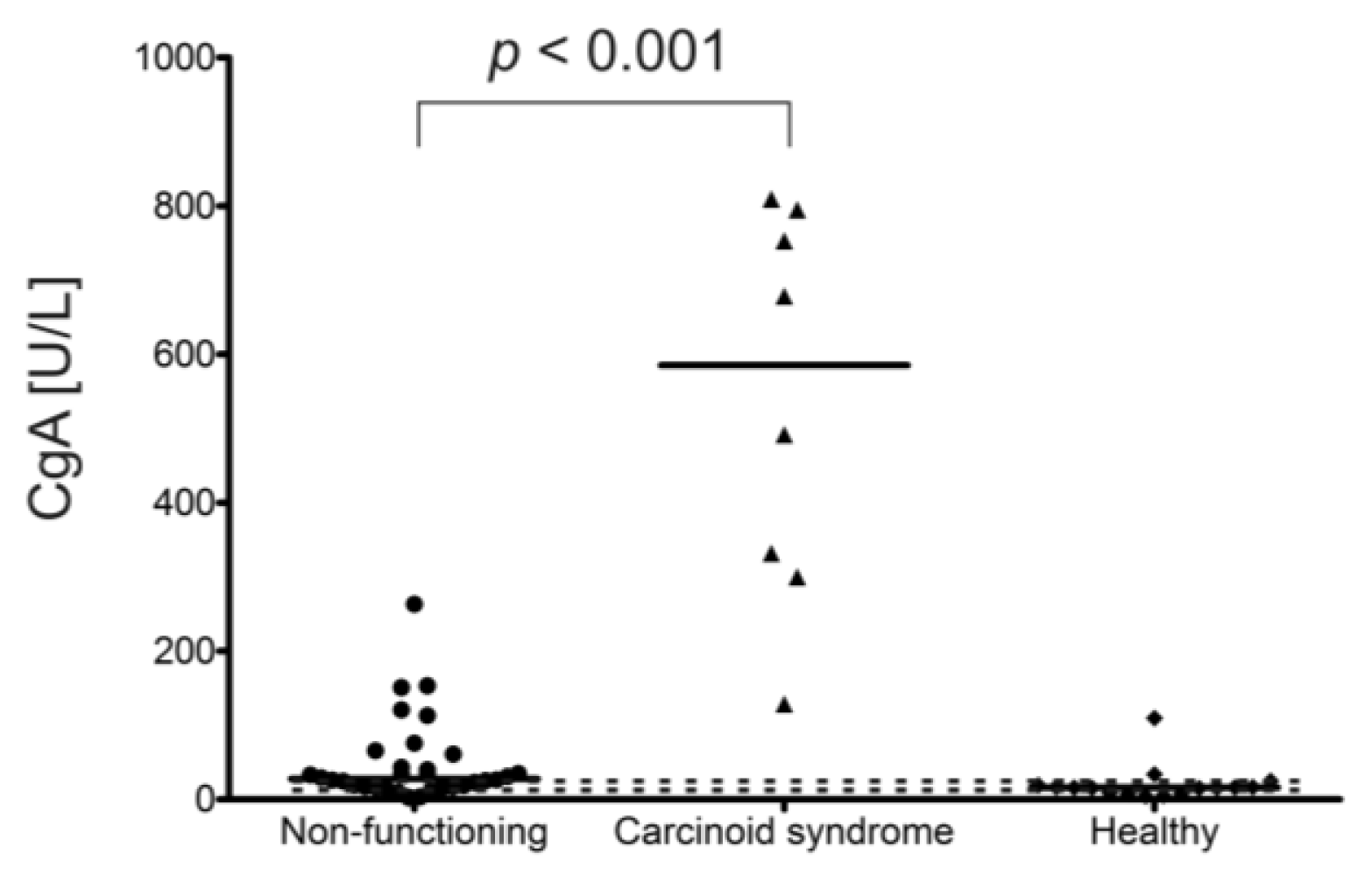
2.1.2. Angiogenic Factors Levels in Patients with Carcinoid Syndrome in Comparison to Non-Functioning NETs
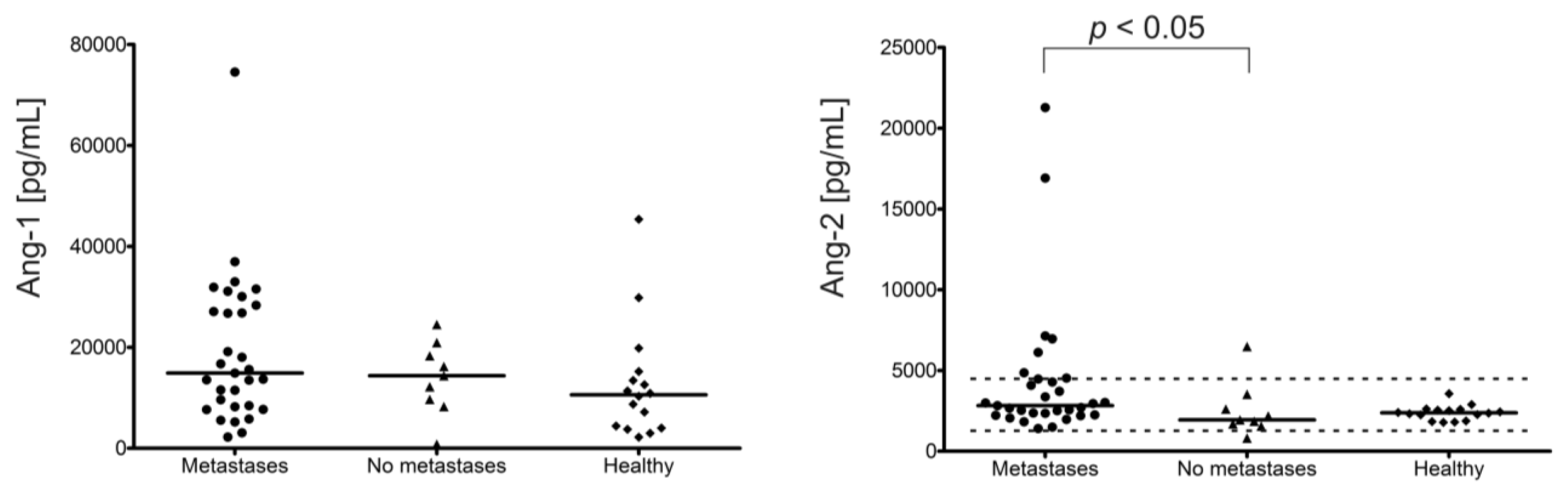
2.1.3. Angiogenic Factors Levels and Stage of Disease
2.1.4. Angiogenic Factor Level and NET Types
2.1.5. Changes in Angiogenic Factors Levels in Selected NET Patients, Who Had Two Blood Samples Taken
2.1.6. Discussion
3. Materials and Methods
3.1. Patients
3.2. ELISAs
3.3. Statistical Analysis
4. Conclusions
Acknowledgments
- Conflict of InterestThe authors declare no conflict of interest.
References
- Stepien, H.M.; Kołomecki, K.; Pasieka, Z.; Komorowski, J.; Stepień, T.; Kuzdak, K. Angiogenesis of endocrine gland tumours—New molecular targets in diagnostics and therapy. Eur. J. Endocrinol 2002, 146, 143–151. [Google Scholar]
- Turner, H.E.; Harris, A.L.; Melmed, S; Wass, J.A. Angiogenesis in endocrine tumors. Endocr. Rev. 2003, 24, 600–632. [Google Scholar]
- Fiedler, U.; Krissl, T.; Koidl, S.; Weiss, C.; Koblizek, T.; Deutsch, U.; Martiny-Baron, G.; Marmé, D.; Augustin, H.G. Angiopoietin-1 and angiopoietin-2 share the same binding domains in the Tie-2 receptor involving the first Ig-like loop and the epidermal growth factor-like repeats. J. Biol. Chem 2003, 278, 1721–1727. [Google Scholar]
- Hu, B.; Cheng, S.Y. Angiopoietin-2: development of inhibitors for cancer therapy. Curr. Oncol. Rep 2009, 11, 111–116. [Google Scholar]
- O’Reilly, M.S.; Boehm, T.; Shing, Y.; Fukai, N.; Vasios, G.; Lane, W.S.; Flynn, E.; Birkhead, J.R.; Olsen, B.R.; Folkman, J. Endostatin: An endogenous inhibitor of angiogenesis and tumor growth. Cell 1997, 88, 277–285. [Google Scholar]
- Bergers, G.; Javaherian, K.; Lo, K.M.; Folkman, J.; Hanahan, D. Effects of angiogenesis inhibitors on multistage carcinogenesis in mice. Science 1999, 284, 808–812. [Google Scholar]
- Kuroi, K.; Tanaka, C.; Toi, M. Circulating levels of endostatin in cancer patients. Oncol. Rep 2001, 8, 405–409. [Google Scholar]
- Schuch, G.; Kisker, O.; Atala, A.; Soker, S. Pancreatic tumor growth is regulated by the balance between positive and negative modulators of angiogenesis. Angiogenesis 2002, 5, 181–190. [Google Scholar]
- Feldman, A.L.; Alexander, H.R., Jr; Yang, J.C.; Linehan, W.M.; Eyler, R.A.; Miller, M.S.; Steinberg, S.M.; Libutti, S.K. Prospective analysis of circulating endostatin levels in patients with renal cell carcinoma. Cancer 2002, 95, 1637–1643. [Google Scholar]
- Schips, L.; Dalpiaz, O.; Lipsky, K.; Langner, C.; Rehak, P.; Puerstner, P.; Pummer, K.; Zigeuner, R. Serum levels of vascular endothelial growth factor (VEGF) and endostatin in renal cell carcinoma patients compared to a control group. Eur. Urol 2007, 51, 168–173. [Google Scholar]
- Fisher, L.W.; Fedarko, N.S. Six genes expressed in bones and teeth encode the current members of the SIBLING family of proteins. Connect. Tissue Res 2003, 44, 33–40. [Google Scholar]
- Rittling, S.R.; Chambers, A.F. Role of osteopontin in tumour progression. Br. J. Cancer 2004, 90, 1877–1881. [Google Scholar]
- Sharp, J.A.; Sung, V.; Slavin, J.; Thompson, E.W.; Henderson, M.A. Tumor cells are the source of osteopontin and bone sialoprotein expression in human breast cancer. Lab. Invest 1999, 79, 869–877. [Google Scholar]
- Creaney, J.; Yeoman, D.; Musk, A.W.; de Klerk, N.; Skates, S.J.; Robinson, B.W. Plasma versus serum levels of osteopontin and mesothelin in patients with malignant mesothelioma—Which is best? Lung Cancer 2011, 74, 55–60. [Google Scholar]
- Detjen, K.M.; Rieke, S.; Deters, A.; Schulz, P.; Rexin, A.; Vollmer, S.; Hauff, P.; Wiedenmann, B.; Pavel, M.; Scholz, A. Angiopoietin-2 promotes disease progression of neuroendocrine tumors. Clin. Cancer Res 2010, 16, 420–429. [Google Scholar]
- Figueroa-Vega, N.; Díaz, A.; Adrados, M.; Alvarez-Escolá, C.; Paniagua, A.; Aragonés, J.; Martín-Pérez, E.; Leskela, S.; Moreno-Otero, R.; González-Amaro, R.; et al. The association of the angiopoietin/Tie-2 system with the development of metastasis and leukocyte migration in neuroendocrine tumors. In Endocr. Relat. Cancer; 2010; Volume 17, pp. 897–908. [Google Scholar]
- Srirajaskanthan, R.; Dancey, G.; Hackshaw, A.; Luong, T.; Caplin, M.E.; Meyer, T. Circulating angiopoietin-2 is elevated in patients with neuroendocrine tumours and correlates with disease burden and prognosis. Endocr. Relat. Cancer 2009, 16, 967–976. [Google Scholar]
- Polikarpova, S.B.; Lyubimova, N.V.; Smirnova, E.A.; Britvin, T.A.; Ogereliev, A.S.; Davidov, M.I. Serum angiogenic factors in patients with neuroendocrine tumors of abdominal organs. Bull. Exp. Biol. Med 2009, 148, 634–637. [Google Scholar]
- Klement, G.L.; Yip, T.T.; Cassiola, F.; Kikuchi, L.; Cervi, D.; Podust, V.; Italiano, J.E.; Wheatley, E.; Abou-Slaybi, A.; Bender, E.; et al. Platelets actively sequester angiogenesis regulators. Blood 2009, 113, 2835–2842. [Google Scholar]
- Adams, J.; Carder, P.J.; Downey, S.; Forbes, M.A.; MacLennan, K.; Allgar, V.; Kaufman, S.; Hallam, S.; Bicknell, R.; Walker, J.J.; et al. Vascular endothelial growth factor (VEGF) in breast cancer: comparison of plasma, serum, and tissue VEGF and microvessel density and effects of tamoxifen. Cancer Res 2000, 60, 2898–2905. [Google Scholar]
- Colleoni, M.; Rocca, A.; Sandri, M.T.; Zorzino, L.; Masci, G.; Masci, G.; Nolè, F.; Peruzzotti, G.; Robertson, C.; Orlando, L.; et al. Low-dose oral methotrexate and cyclophosphamide in metastatic breast cancer: Antitumor activity and correlation with vascular endothelial growth factor levels. Ann. Oncol 2002, 13, 73–80. [Google Scholar]
- Holmes, C.E.; Huang, J.C.; Pace, T.R.; Howard, A.B.; Muss, H.B. Tamoxifen and aromatase inhibitors differentially affect vascular endothelial growth factor and endostatin levels in women with breast cancer. Clin. Cancer Res 2008, 14, 3070–3076. [Google Scholar]
- Kulke, M.H.; Siu, L.L.; Tepper, J.E.; Fisher, G.; Jaffe, D.; Haller, D.G.; Ellis, L.M.; Benedetti, J.K.; Bergsland, E.K.; Hobday, T.J.; et al. Future directions in the treatment of neuroendocrine tumors: consensus report of the National Cancer Institute. Neuroendocrine Tumor clinical trials planning meeting. J. Clin. Oncol 2011, 29, 934–943. [Google Scholar]
- Villaume, K.; Blanc, M.; Gouysse, G.; Walter, T.; Couderc, C.; Nejjari, M.; Vercherat, C.; Cordier-Bussat, M.; Roche, C.; Scoazec, J.Y. VEGF secretion by neuroendocrine tumor cells is inhibited by octreotide and by inhibitors of the PI3K/AKT/mTOR pathway. Neuroendocrinology 2010, 91, 268–278. [Google Scholar]
- Melen-Mucha, G.; Lawnicka, H.; Kierszniewska-Stepien, D.; Komorowski, J.; Stepien, H. The place of somatostatin analogs in the diagnosis and treatment of the neuoroendocrine glands tumors. Recent Pat. Anticancer Drug Discov 2006, 1, 237–254. [Google Scholar]
- Statistica 9, version 9; StatSoft Inc.: Tulsa, OK, USA, 2009.
- Graph Pad Prism, trial version; GraphPad Software Inc.: La Jolla, CA, USA, 2010.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Age—median (range) | 61 years (31–80) |
| Male—number of patients (median of age; range) | 17 (57 years; 32–80) |
| Female—number of patients (median of age; range) | 19 (66 years;31–76) |
| Patients with metastatic disease—number of patients (%) | 27 (75%) |
| Patients without metastases—number of patients (%) | 9 (25%) |
| Patients with carcinoid syndrome—number of patients (%) | 7 (19%) |
| Patients with non-functioning NETs—number of patients (%) | 29 (81%) |
| Type of NETs—number of patients (%) | |
| foregut | 11 (31%) |
| midgut | 12 (33%) |
| hindgut | 6 (17%) |
| unknown or others | 7 (19%) |
| Localization of the primary tumor—number of patients (%) | |
| lung | 6 (17%) |
| thymus | 1 (3%) |
| pancreas | 2 (6%) |
| stomach | 2 (6%) |
| small intestine and appendix | 12 (33%) |
| rectum | 6 (17%) |
| unknown or others | 7 (19%) |
| Concurrent SST analogs—number of patients (%) | 14 (39%) |
| Patient | Time of Two Blood Samplings & Changes | CgA (U/L) | Tie-2 ng/mL | Ang-2 (pg/mL) | Ang-1 (pg/mL) | End ng/mL | OPN ng/mL | VEGF (pg/mL) |
|---|---|---|---|---|---|---|---|---|
| ♀ 69-year-old metastatic nonfunctioning midgut NET (small intestine) | 1/before the first injection of 20 mg octreotide LAR (Novartis) | 34.8 | 64 | 16921 | 13571 | 208 | 123 | ND |
| 2/one month later, before the second injection | ND | 43 | 3024 | 8228 | 160 | 123 | ND | |
| changes | ↓30% | ↓80% | ↓40% | ↓20% | 0% | |||
| ♂ 57-year-old metastatic midgut NET with carcinoid syndrome | 1/before the first injection of 90 mg lanreotide autogel (Ipsen) | 492 | 37 | 2062 | 13671 | 296 | 65 | ND |
| 2/after 7 months of therapy (90 mg every 4 weeks) with well-controlled symptoms | 678.5 | 42 | 4086 | 5231 | 232 | 52.5 | ND | |
| changes | ↑40% | ↑10% | ↑100% | ↓60% | ↓20% | ↓20% | ||
| ♂ 47-year-old metastatic non-functioning NET of the left kidney | 1/good clinical status, 2 months before the first dose of 20 mg octreotide LAR (Novartis) | 75.7 | 38 | 3708 | 27102 | 92 | 14 | 370.6 |
| 2/poor clinical status, just before death, after 1 year and 1 month of octreotide therapy (20 mg every 4 weeks) and after many resections of metastatic foci | 60.8 | 25 | 3376 | 28362 | 100 | 13 | 314.3 | |
| changes | ↓19% | ↓34% | ↓9% | ↑5% | ↑8% | ↓7% | ↓13% | |
| ♂ 57-year-old metastatic nonfunctioning rectal NET and gastric GIST | 1/just before GIST removal on octreotide therapy | 11.1 | 48 | 1406 | 2217 | 144 | 6 | ND |
| 2/after almost 2 years passed, without new GIST foci and with partial regression of NET metastatic foci, continuously treated with octreotide LAR for 3 years and 6 months (Novartis) 20 mg i.m. every 4 weeks | 13.2 | 43.5 | 2823 | 7701 | 240 | 63 | ND | |
| changes | ↑19% | ↓10% | ↑100% | ↑350% | ↑160% | ↑1000% | ND | |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Melen-Mucha, G.; Niedziela, A.; Mucha, S.; Motylewska, E.; Lawnicka, H.; Komorowski, J.; Stepien, H. Elevated Peripheral Blood Plasma Concentrations of Tie-2 and Angiopoietin 2 in Patients with Neuroendocrine Tumors. Int. J. Mol. Sci. 2012, 13, 1444-1460. https://doi.org/10.3390/ijms13021444
Melen-Mucha G, Niedziela A, Mucha S, Motylewska E, Lawnicka H, Komorowski J, Stepien H. Elevated Peripheral Blood Plasma Concentrations of Tie-2 and Angiopoietin 2 in Patients with Neuroendocrine Tumors. International Journal of Molecular Sciences. 2012; 13(2):1444-1460. https://doi.org/10.3390/ijms13021444
Chicago/Turabian StyleMelen-Mucha, Gabriela, Agata Niedziela, Slawomir Mucha, Ewelina Motylewska, Hanna Lawnicka, Jan Komorowski, and Henryk Stepien. 2012. "Elevated Peripheral Blood Plasma Concentrations of Tie-2 and Angiopoietin 2 in Patients with Neuroendocrine Tumors" International Journal of Molecular Sciences 13, no. 2: 1444-1460. https://doi.org/10.3390/ijms13021444
APA StyleMelen-Mucha, G., Niedziela, A., Mucha, S., Motylewska, E., Lawnicka, H., Komorowski, J., & Stepien, H. (2012). Elevated Peripheral Blood Plasma Concentrations of Tie-2 and Angiopoietin 2 in Patients with Neuroendocrine Tumors. International Journal of Molecular Sciences, 13(2), 1444-1460. https://doi.org/10.3390/ijms13021444