Expression of Phospho-ELK1 and Its Prognostic Significance in Urothelial Carcinoma of the Upper Urinary Tract


Abstract
:1. Introduction
2. Results
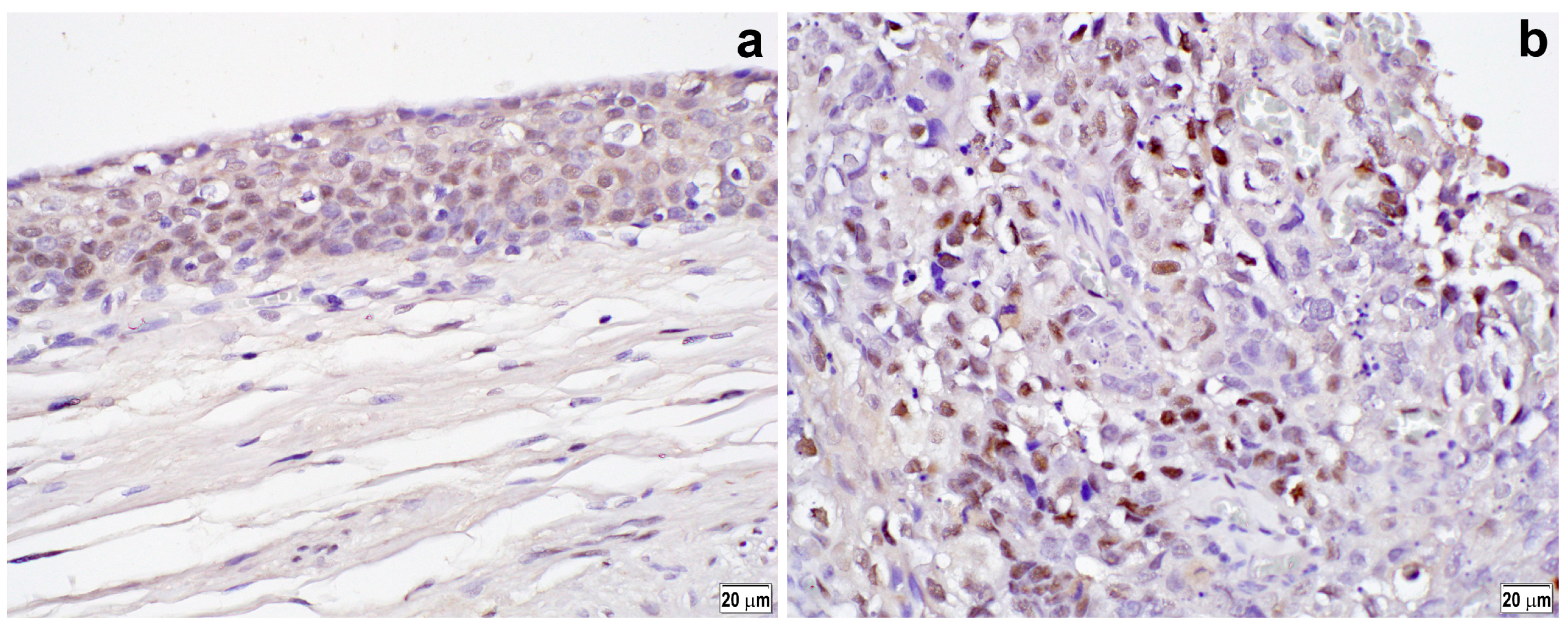
2.1. Immunoreactivity in Benign and Tumor Tissues
2.2. Immunoreactivity and Clinicopathological Features
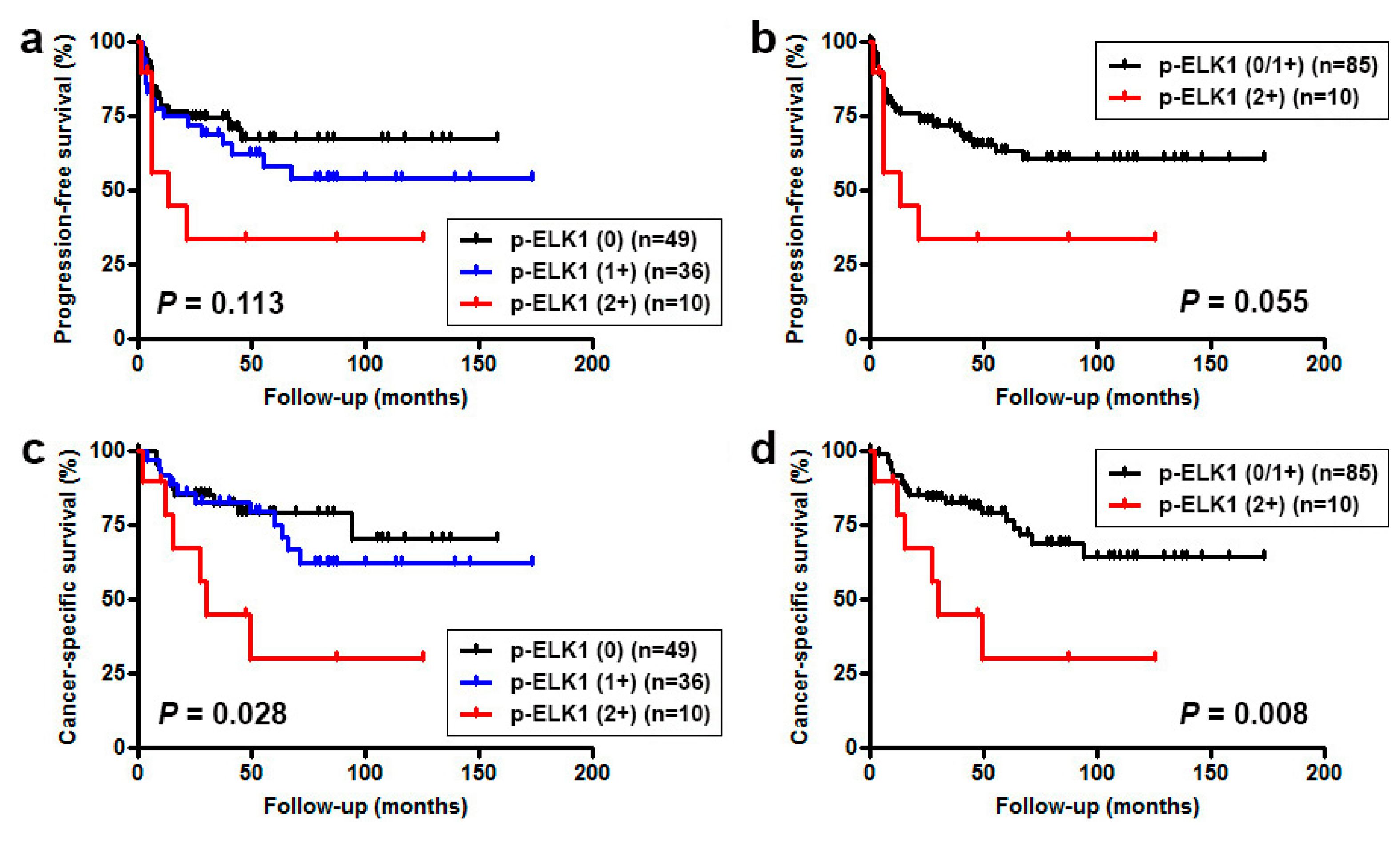
2.3. Immunoreactivity and Prognostic Significance
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. Immunohistochemistry
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Oya, M.; Kikuchi, E.; Committee for Establishment of Clinical Practice Guideline for Management of Upper Tract Urothelial Carcinoma and Japanese Urological Association. Evidenced-based clinical practice guideline for upper tract urothelial carcinoma (summary–Japanese Urological Association, 2014 edition). Int. J. Urol. 2015, 22, 3–13. [Google Scholar] [PubMed]
- Rouprêt, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Böhle, A.; Van Rhijn, B.W.; Kaasinen, E.; et al. European Association of Urology guidelines on upper urinary tract urothelial cell carcinoma: 2015 Update. Eur. Urol. 2015, 68, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Chromecki, T.F.; Bensalah, K.; Remzi, M.; Verhoest, G.; Cha, E.K.; Scherr, D.S.; Novara, G.; Karakiewicz, P.I.; Shariat, S.F. Prognostic factors for upper urinary tract urothelial carcinoma. Nat. Rev. Urol. 2011, 8, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Burger, M.; Margulis, V.; Matin, S.F.; Novara, G.; Roupret, M.; Shariat, S.F.; Wood, C.G.; Zigeuner, R. Prognostic factors in upper urinary tract urothelial carcinomas: A comprehensive review of the current literature. Eur. Urol. 2012, 62, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Krabbe, L.M.; Heitplatz, B.; Preuss, S.; Hutchinson, R.C.; Woldu, S.L.; Singla, N.; Boegemann, M.; Wood, C.G.; Karam, J.A.; Weizer, A.Z.; et al. Prognostic value of PD-1 and PD-L1 expression in patients with high grade upper tract urothelial carcinoma. J. Urol. 2017, 198, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Hipskind, R.A.; Rao, V.N.; Mueller, C.G.; Reddy, E.S.; Nordheim, A. Ets-related protein Elk-1 is homologous to the c-fos regulatory factor p62TCF. Nature 1991, 354, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.; Bamier, J.V.; Guibert, B.; Pagès, C.; Besson, M.J.; Hipskind, R.A.; Caboche, J. Glutamate induces phosphorylation of Elk-1 and CREB, along with c-fos activation, via an extracellular signal-regulated kinase-dependent pathway in brain slices. Mol. Cell. Biol. 1999, 19, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.D.; Jeong, S.J.; Wang, G.; Park, J.J.; Lim, D.S.; Kim, B.H.; Cho, Y.I.; Kim, C.S.; Jeong, M.J. Secretory leukocyte protease inhibitor is associated with MMP-2 and MMP-9 to promote migration and invasion in SNU638 gastric cancer cells. Int. J. Mol. Med. 2011, 28, 527–534. [Google Scholar] [PubMed]
- Ahmad, N.; Wang, W.; Nair, R.; Kapila, S. Relaxin induces matrix-metalloproteinases-9 and -13 via RXFP1: Induction of MMP-9 involves the PI3K, ERK, Akt and PKC-ζ pathways. Mol. Cell. Endocrinol. 2012, 363, 46–61. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Ide, H.; Kashiwagi, E.; Patterson, J.D.; Inoue, S.; Shareef, H.K.; Aljarah, A.K.; Zheng, Y.; Baras, A.S.; Miyamoto, H. Silodosin inhibits the growth of bladder cancer cells and enhances the cytotoxic activity of cisplatin via ELK1 inactivation. Am. J. Cancer Res. 2015, 5, 2959–2968. [Google Scholar] [PubMed]
- Kawahara, T.; Shareef, H.K.; Aljarah, A.K.; Ide, H.; Li, Y.; Kashiwagi, E.; Netto, G.J.; Zheng, Y.; Miyamoto, H. ELK1 is up-regulated by androgen in bladder cancer cells and promotes tumor progression. Oncotarget 2015, 6, 29860–29876. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Mizushima, T.; Miyamoto, H. Role of the androgen receptor in urothelial cancer. Mol. Cell. Endocrinol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Patki, M.; Chari, V.; Sivakumaran, S.; Gonit, M.; Trumbly, R.; Ratnam, M. The ETS domain transcription factor ELK1 directs a critical component of growth signaling by the androgen receptor in prostate cancer cells. J. Biol. Chem. 2013, 288, 11047–11065. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, E.; Fujita, K.; Yamaguchi, S.; Fushimi, H.; Ide, H.; Inoue, S.; Mizushima, T.; Reis, L.O.; Sharma, R.; Netto, G.J.; et al. Expression of steroid hormone receptors and its prognostic significance in urothelial carcinoma of the upper urinary tract. Cancer Biol. Ther. 2016, 17, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Shao, N.; Chai, Y.; Cui, J.Q.; Wang, N.; Aysola, K.; Reddy, E.S.; Rao, V.N. Induction of apoptosis by Elk-1 and ΔElk-1 proteins. Oncogene 1998, 17, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Mut, M.; Lule, S.; Demir, O.; Kumaz, I.A.; Vural, I. Both mitogen-activated protein kinase (MAPK)/extracellular-signal-regulated kinases (ERK) 1/2 and phosphatidylinositide-3-OH kinase (PI3K)/Akt pathways regulate activation of E-twenty-six (ETS)-like transcription factor 1 (Elk-1) in U138 glioblastoma cells. Int. J. Biochem. Cell Biol. 2012, 44, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Aljarah, A.K.; Shareef, H.K.; Inoue, S.; Ide, H.; Patterson, J.D.; Kashiwagi, E.; Han, B.; Li, Y.; Zheng, Y.; et al. Silodosin inhibits prostate cancer cell growth via ELK1 inactivation and enhances the cytotoxic activity of gemcitabine. Prostate 2016, 76, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Mizushima, T.; Fujita, K.; Meliti, A.; Ide, H.; Yamaguchi, S.; Fushimi, H.; Netto, G.J.; Nonomura, N.; Miyamoto, H. GATA3 immunohistochemistry in urothelial carcinoma of the upper urinary tract as a urothelial marker as well as a prognosticator. Hum. Pathol. 2017, 64, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Jalalizadeh, M.; Inoue, S.; Fujita, K.; Ide, H.; Mizushima, T.; Yamaguchi, S.; Fushimi, H.; Nonomura, N.; Miyamoto, H. ZKSCAN3 expression in urothelial carcinoma of the upper urinary tract and its impact on patient outcomes. Integr. Cancer Sci. Ther. 2017, 4, 1000241. [Google Scholar] [CrossRef]
- Miyamoto, H.; Izumi, K.; Yao, J.L.; Li, Y.; Yang, Q.; McMahon, L.A.; Gonzalez-Roibon, N.; Hicks, D.G.; Tacha, D.; Netto, G.J. GATA binding protein 3 is down-regulated in bladder cancer yet strong expression is an independent predictor of poor prognosis in invasive tumor. Hum. Pathol. 2012, 43, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Yao, J.L.; Chaux, A.; Zheng, Y.; Hsu, I.; Izumi, K.; Chang, C.; Messing, E.M.; Netto, G.J.; Yeh, S. Expression of androgen and oestrogen receptors and its prognostic significance in urothelial neoplasm of the urinary bladder. BJU Int. 2012, 109, 1716–1726. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, H.; Kawahara, T.; Zheng, Y.; Netto, G.J.; Miyamoto, H. Reduced glucocorticoid receptor expression predicts bladder tumor recurrence and progression. Am. J. Clin. Pathol. 2014, 142, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Inoue, S.; Ide, H.; Kashiwagi, E.; Ohtake, S.; Mizushima, T.; Li, P.; Li, Y.; Zheng, Y.; Uemura, H.; et al. ZKSCAN3 promotes bladder cancer cell proliferation, migration, and invasion. Oncotarget 2016, 7, 53599–53610. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Inoue, S.; Fujita, K.; Mizushima, T.; Ide, H.; Yamaguchi, S.; Fushimi, H.; Nonomura, N.; Miyamoto, H. NFATc1 expression as a prognosticator in urothelial carcinoma of the upper urinary tract. Transl. Oncol. 2017, 10, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Munari, E.; Fujita, K.; Faraj, S.; Chaux, A.; Gonzalez-Roibon, N.; Hicks, J.; Meeker, A.; Nonomura, N.; Netto, G.J. Dysregulation of mammalian target of rapamycin pathway in upper tract urothelial carcinoma. Hum. Pathol. 2013, 44, 2668–2676. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Tissue | n | p-ELK1 Expression | P Value | ||||
|---|---|---|---|---|---|---|---|
| 0 (%) | 1+ (%) | 2+ (%) | 3+ (%) | 0 vs. 1+/2+/3+ | 0/1+ vs. 2+/3+ | ||
| Normal | 83 | 62 (74.7) | 17 (20.5) | 4 (4.8) | 0 (0) | 0.002 | 0.265 |
| Tumor | 99 | 52 (52.5) | 37 (37.4) | 10 (10.1) | 0 (0) | ||
| Parameter | n | p-ELK1 Expression | p Value | |||
|---|---|---|---|---|---|---|
| 0 (%) | 1+ (%) | 2+ (%) | 0 vs. 1+/2+ | 0/1+ vs. 2+ | ||
| Age (mean ± SD; years) | 99 | 70.0 ± 9.5 | 71.9 ± 7.3 | 68.5 ± 10.9 | 0.199 | 0.659 |
| Gender | 0.849 | 0.736 | ||||
| Male | 60 | 28 (46.7) | 25 (41.7) | 7 (11.7%) | ||
| Female | 39 | 24 (61.5) | 12 (30.8) | 3 (7.7) | ||
| Laterality | 0.548 | 0.323 | ||||
| Right | 43 | 21 (48.8) | 16 (37.2) | 6 (14.0) | ||
| Left | 56 | 31 (55.4) | 21 (37.5) | 4 (7.1) | ||
| Tumor site | 0.151 a | 0.096 a | ||||
| Renal pelvis | 45 | 27 (60.0) | 16 (35.6) | 2 (4.4) | ||
| Ureter | 50 | 22 (44.0) | 20 (40.0) | 8 (16.0) | ||
| Both | 4 | 3 (75.0) | 1 (25.0) | 0 (0) | ||
| Tumor grade | 0.273 | 1.000 | ||||
| Low-grade | 15 | 10 (66.7) | 4 (26.7) | 1 (6.7) | ||
| High-grade | 84 | 42 (50.0) | 33 (39.3) | 9 (10.7) | ||
| Pathologic stage | 0.065 b | 0.085 b | ||||
| pTa | 19 | 13 (68.4) | 5 (26.3) | 1 (5.3) | ||
| pT1 | 18 | 11 (61.1) | 7 (38.9) | 0 (0) | ||
| NMI (pTa + pT1) | 37 | 24 (64.9) | 12 (32.4) | 1 (2.7) | ||
| pT2 | 8 | 1 (12.5) | 6 (75.0) | 1 (12.5) | ||
| pT3 | 48 | 26 (54.2) | 16 (33.3) | 6 (12.5) | ||
| pT4 | 6 | 1 (16.7) | 3 (50.0) | 2 (33.3) | ||
| MI (pT2 + pT3 + pT4) | 62 | 28 (45.2) | 25 (40.3) | 9 (14.5) | ||
| Concurrent CIS | 0.768 | 0.616 | ||||
| No | 86 | 46 (53.5) | 32 (37.2) | 8 (9.3) | ||
| Yes | 13 | 6 (46.2) | 5 (38.5) | 2 (15.4) | ||
| Hydronephrosis | 0.445 c | 1.000 c | ||||
| No | 61 | 33 (54.1) | 25 (41.0) | 3 (4.9) | ||
| Yes | 20 | 13 (65.0) | 6 (30.0) | 1 (5.0) | ||
| Unknown | 18 | 6 (33.3) | 6 (33.3) | 6 (33.3) | ||
| Lymphovascular invasion | 0.227 | 0.014 | ||||
| No | 59 | 34 (57.6) | 23 (39.0) | 2 (3.4) | ||
| Yes | 40 | 18 (45.0) | 14 (35.0) | 8 (20.0) | ||
| Lymph node involvement | 0.357 d | 0.109 d | ||||
| pN0 | 84 | 41 (48.8) | 36 (42.9) | 7 (8.3) | ||
| pN1-3 | 12 | 8 (66.7) | 1 (8.3) | 3 (25.0) | ||
| pNx | 3 | 3 (100) | 0 (0) | 0 (0) | ||
| Patients | n | AR | ERα | ERβ | GR | PR | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CC | P | CC | P | CC | P | CC | P | CC | P | ||
| All cases | 99 | 0.171 | 0.091 | 0.076 | 0.454 | 0.103 | 0.312 | 0.176 | 0.081 | 0.054 | 0.594 |
| Male | 60 | 0.247 | 0.058 | 0.175 | 0.181 | 0.082 | 0.535 | 0.096 | 0.466 | 0.055 | 0.678 |
| Female | 39 | −0.105 | 0.525 | −0.048 | 0.770 | 0.199 | 0.224 | 0.262 | 0.107 | 0.137 | 0.407 |
| Parameter | Progression-Free Survival | Cancer-Specific Survival | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||||||
| HR | 95% CI | P | HR | 95% CI | P | HR | 95% CI | P | HR | 95% CI | P | |
| Tumor grade | 3.858 | 0.923–16.123 | 0.064 | 3.304 | 0.715–12.877 | 0.132 | 6.411 | 0.868–47.372 | 0.036 | 4.953 | 0.661–37.086 | 0.119 |
| pT stage a | 10.975 | 3.848–31.306 | <0.001 | 7.750 | 2.575–23.329 | <0.001 | 17.213 | 4.055–73.070 | <0.001 | 10.118 | 2.241–45.680 | 0.003 |
| LVI | 5.701 | 2.775–11.711 | <0.001 | 2.483 | 1.125–5.481 | 0.024 | 6.712 | 2.827–15.934 | <0.001 | 2.350 | 0.888–6.222 | 0.085 |
| pN stage | 4.232 | 1.738–10.308 | 0.001 | 2.494 | 0.891–6.981 | 0.082 | 4.379 | 1.762–10.884 | 0.001 | 1.603 | 0.605–4.244 | 0.343 |
| p-ELK1 b | 2.291 | 0.948–5.540 | 0.066 | 0.666 | 0.244–1.820 | 0.428 | 3.179 | 1.279–7.901 | 0.013 | 1.131 | 0.431–2.964 | 0.802 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, S.; Ide, H.; Fujita, K.; Mizushima, T.; Jiang, G.; Kawahara, T.; Yamaguchi, S.; Fushimi, H.; Nonomura, N.; Miyamoto, H. Expression of Phospho-ELK1 and Its Prognostic Significance in Urothelial Carcinoma of the Upper Urinary Tract. Int. J. Mol. Sci. 2018, 19, 777. https://doi.org/10.3390/ijms19030777
Inoue S, Ide H, Fujita K, Mizushima T, Jiang G, Kawahara T, Yamaguchi S, Fushimi H, Nonomura N, Miyamoto H. Expression of Phospho-ELK1 and Its Prognostic Significance in Urothelial Carcinoma of the Upper Urinary Tract. International Journal of Molecular Sciences. 2018; 19(3):777. https://doi.org/10.3390/ijms19030777
Chicago/Turabian StyleInoue, Satoshi, Hiroki Ide, Kazutoshi Fujita, Taichi Mizushima, Guiyang Jiang, Takashi Kawahara, Seiji Yamaguchi, Hiroaki Fushimi, Norio Nonomura, and Hiroshi Miyamoto. 2018. "Expression of Phospho-ELK1 and Its Prognostic Significance in Urothelial Carcinoma of the Upper Urinary Tract" International Journal of Molecular Sciences 19, no. 3: 777. https://doi.org/10.3390/ijms19030777