Plants and Surgery: The Protective Effects of Thymoquinone on Hepatic Injury—A Systematic Review of In Vivo Studies

Abstract
:1. Introduction
1.1. Current Treatment Concepts and Hepatotoxicity
Transplantation and IRI
1.2. Natural Remedies and Liver Protection
1.3. Characterization of Nigella sativa Seeds, Its Oil and Its Active Components
1.4. Properties of N. sativa
1.5. Toxicity Studies on N. sativa and Metabolism of TQ
1.6. Objective
2. Results
2.1. Study Protocols and Applied TQ Doses
2.2. Effect of TQ
2.2.1. TQ and Oxidative Stress
2.2.2. TQ and Inflammation
2.2.3. TQ and Fibrosis
2.2.4. TQ and Apoptosis
2.2.5. TQ and Hepatic Malignancy
2.2.6. Summary of the Hepatoprotective Effects of TQ in Tables
3. Summary
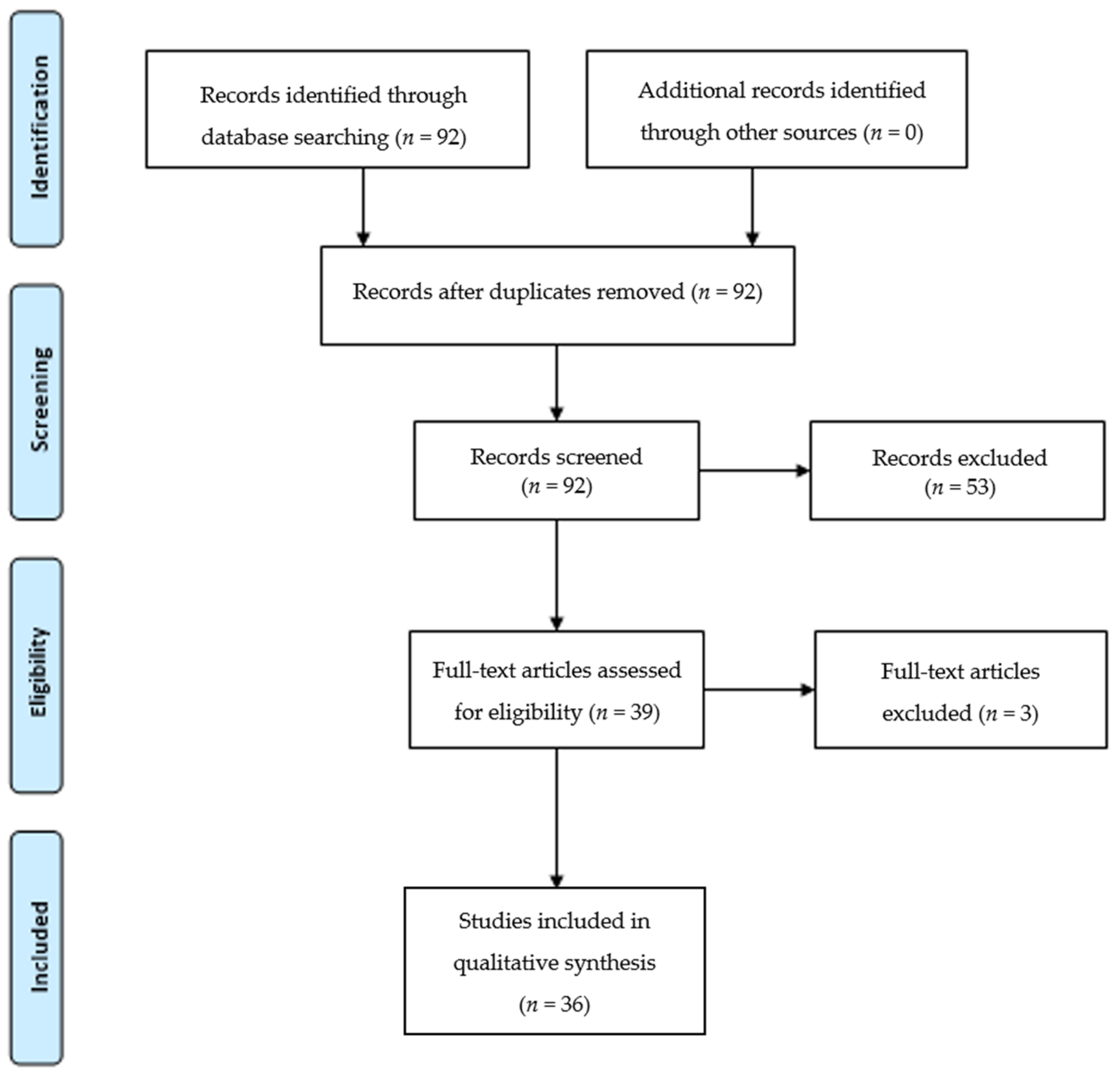
4. Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AFP | α-fetoprotein |
| AgNOR | Argyrophilic nucleolar organizer region |
| ALP | Alkaline phosphatase |
| ALT | Alanine aminotransferase |
| AMPK | Adenosine monophosphate-activated protein kinase |
| AST | Aspartate aminotransferase |
| Bcl-2 | B-cell lymphoma-2 |
| bw | Body weight |
| CAT | Catalase |
| CCA | Cholangiocarcinoma |
| CCI4 | Carbon tetrachloride-induced |
| CD | Conjugated diene |
| CEA | Carcinoembryonic antigen |
| COX-2 | Cyclooxygenase-2 |
| CP | Cyclophosphamide |
| CsA | Cyclosporine A |
| CYP | Cytochrome |
| DHTQ | Dihydrothymoquinone |
| EGF | Epidermal growth factor |
| Gpx | Glutathione peroxidase |
| Gred | Glutathione reductase |
| GSH | Glutathione |
| GSSG | Glutathione disulfide |
| GST | Glutathione S-transferase |
| GTC | Green tea catechin |
| HCC | Hepatocellular carcinoma |
| HDL | High density lipoprotein |
| HP | Hydroxyproline |
| HSC | Hepatic stellate cells |
| Ig | Immunoglobulin |
| IL | Interleukin |
| IL-1β | Interleukin-1 beta |
| iNOS | Inducible nitric oxide synthase |
| ip | intraperitoneal |
| IR | Ischemia/reperfusion |
| IRI | Ischemia/reperfusion injury |
| LD50 | Mean lethal dose |
| LDH | Lactate dehydrogenase |
| LDL | Low density lipoprotein |
| LOOH | Lipid hydroperoxide |
| LPO | Lipid peroxidation |
| LPS | Lipopolysaccharide |
| MCP-1 | Monocyte chemotactic protein-1 |
| MDA | Malondialdehyde |
| MIF | Migration inhibitory factor |
| MnSOD | Manganese superoxide dismutase |
| MPO | Myeloperoxidase |
| MTX | Methotrexate |
| NADH | Nicotinamide adenine dinucleotide |
| NADPH | Nicotinamide adenine dinucleotide phosphate |
| N. sativa | Nigella sativa |
| NASH | Nonalcoholic steatohepatitis induced by high-fat high-cholesterol diet |
| NDEA | N-Nitrosodiethylamine |
| NF-κB | Nuclear factor kappa-B |
| NICD1 | NOTCH1 intracellular Domain |
| NO | Nitric oxide |
| NOSTRIN | Nitric oxide synthase trafficking |
| Nrf2 | Nuclear respiratory factor 2 |
| OH | Hydroxyl radical |
| OSI | Oxidative stress index |
| PCNA | Proliferating cell nuclear antigen |
| PI3K/Akt | Phosphoinositide 3-kinase |
| PON | Paraoxonase |
| R | Reference |
| ROS | Reactive oxygen species |
| SAs | Sodium arsenite |
| sc | subcutaneous |
| SIRT1 | Hepatic sirtuin 1 |
| SOD | Superoxide dismutase |
| SOS | Sinusoidal obstruction syndrome |
| SSAT | Spermidine/spermine N-1-acetyl-transferase |
| TAS | Total antioxidant status |
| TG | Triglycerides |
| TGF-β | Transforming growth factor-β |
| TIMP-1 | Tissue inhibitor of metalloproteinase-1 |
| TNF-α | Tumor necrosis factor-α |
| TOS | Total oxidant status |
| TQ | Thymoquinone |
| VEGF | Vascular endothelial growth factor |
| vLDL | Very low density lipoprotein |
| α-SMA | α-smooth muscle actin |
| γ-GT | Gamma-glutamyl transferase |
References
- Arru, M.; Aldrighetti, L.; Castoldi, R.; Di Palo, S.; Orsenigo, E.; Stella, M.; Pulitano, C.; Gavazzi, F.; Ferla, G.; Di Carlo, V.; et al. Analysis of prognostic factors influencing long-term survival after hepatic resection for metastatic colorectal cancer. World J. Surg. 2008, 32, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Andreou, A.; Vauthey, J.N.; Cherqui, D.; Zimmitti, G.; Ribero, D.; Truty, M.J.; Wei, S.H.; Curley, S.A.; Laurent, A.; Poon, R.T.; et al. Improved long-term survival after major resection for hepatocellular carcinoma: A multicenter analysis based on a new definition of major hepatectomy. J. Gastrointest. Surg. 2013, 17, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.; Lim, H.K.; Rhim, H.; Kim, Y.S.; Yoo, B.C.; Paik, S.W.; Joh, J.W.; Park, C.K. Percutaneous radiofrequency ablation for recurrent hepatocellular carcinoma after hepatectomy: Long-term results and prognostic factors. Ann. Surg. Oncol. 2007, 14, 2319–2329. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Fuster, J.; Bruix, J.; Barcelona-Clinic Liver Cancer, G. The Barcelona approach: Diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004, 10 (Suppl. 1), S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Hoff, P.M.; Ansari, R.; Batist, G.; Cox, J.; Kocha, W.; Kuperminc, M.; Maroun, J.; Walde, D.; Weaver, C.; Harrison, E.; et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: Results of a randomized phase III study. J. Clin. Oncol. 2001, 19, 2282–2292. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Lucidi, V.; Bismuth, H. Hepatic colorectal metastases: Methods of improving resectability. Surg. Clin. N. Am. 2004, 84, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, J. Surgical treatment of hepatocellular carcinoma. J. Chir. (Paris) 1999, 136, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, J.; Kianmanesh, R. Surgical treatment of hepatocellular carcinoma. HPB (Oxford) 2005, 7, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Robinson, S.M.; Wilson, C.H.; Burt, A.D.; Manas, D.M.; White, S.A. Chemotherapy-associated liver injury in patients with colorectal liver metastases: A systematic review and meta-analysis. Ann. Surg. Oncol. 2012, 19, 4287–4299. [Google Scholar] [CrossRef] [PubMed]
- Karoui, M.; Penna, C.; Amin-Hashem, M.; Mitry, E.; Benoist, S.; Franc, B.; Rougier, P.; Nordlinger, B. Influence of preoperative chemotherapy on the risk of major hepatectomy for colorectal liver metastases. Ann. Surg. 2006, 243, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Deleve, L.D. Sinusoidal obstruction syndrome. Gastroenterol. Hepatol. (N. Y.) 2008, 4, 101–103. [Google Scholar]
- DeLeve, L.D.; Shulman, H.M.; McDonald, G.B. Toxic injury to hepatic sinusoids: Sinusoidal obstruction syndrome (veno-occlusive disease). Semin. Liver Dis. 2002, 22, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Sugimoto, K.; Inui, H.; Fukusato, T. Current pharmacological therapies for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J. Gastroenterol. 2015, 21, 3777–3785. [Google Scholar] [CrossRef] [PubMed]
- Guan, L.Y.; Fu, P.Y.; Li, P.D.; Li, Z.N.; Liu, H.Y.; Xin, M.G.; Li, W. Mechanisms of hepatic ischemia-reperfusion injury and protective effects of nitric oxide. World J. Gastrointest. Surg. 2014, 6, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Petrowsky, H.; Hong, J.C.; Busuttil, R.W.; Kupiec-Weglinski, J.W. Ischaemia-reperfusion injury in liver transplantation—From bench to bedside. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Bent, S. Herbal medicine in the United States: Review of efficacy, safety, and regulation: Grand rounds at University of California, San Francisco Medical Center. J. Gen. Intern. Med. 2008, 23, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Li, Y.; Feng, L.; Li, S. Effects of tetrandrine on ischemia/reperfusion injury in mouse liver. Transplant. Proc. 2008, 40, 2163–2166. [Google Scholar] [CrossRef] [PubMed]
- Liang, R.; Nickkholgh, A.; Kern, M.; Schneider, H.; Benzing, S.; Zorn, M.; Buchler, M.W.; Schemmer, P. Green tea extract ameliorates reperfusion injury to rat livers after warm ischemia in a dose-dependent manner. Mol. Nutr. Food Res. 2011, 55, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Sehirli, O.; Ozel, Y.; Dulundu, E.; Topaloglu, U.; Ercan, F.; Sener, G. Grape seed extract treatment reduces hepatic ischemia-reperfusion injury in rats. Phytother. Res. 2008, 22, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, H.; Woolbright, B.L. Current strategies to minimize hepatic ischemia-reperfusion injury by targeting reactive oxygen species. Transplant. Rev. (Orlando) 2012, 26, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Ferriz, J.M.; Vinsova, J. Prodrug design of phenolic drugs. Curr. Pharm. Des. 2010, 16, 2033–2052. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.C.; Hung, C.T.; Chen, Y.S.; Hsueh, C.C.; Hou, C.W.; Lay, H.L. Amelioration of carbon tetrachloride-induced hepatic injury by emulsified Antrodia extract. Iran. J. Basic Med. Sci. 2018, 21, 230–235. [Google Scholar] [PubMed]
- Ahmad, A.; Husain, A.; Mujeeb, M.; Khan, S.A.; Najmi, A.K.; Siddique, N.A.; Damanhouri, Z.A.; Anwar, F. A review on therapeutic potential of Nigella sativa: A miracle herb. Asian Pac. J. Trop. Biomed. 2013, 3, 337–352. [Google Scholar] [CrossRef]
- Mollazadeh, H.; Hosseinzadeh, H. The protective effect of Nigella sativa against liver injury: A review. Iran. J. Basic Med. Sci. 2014, 17, 958–966. [Google Scholar] [PubMed]
- Dajani, E.Z.; Shahwan, T.G.; Dajani, N.E. Overview of the Preclinical Pharmacological Properties of Nigella Sativa (Black Seeds): A Complementary Drug with Historical and Clinical Significance. J. Physiol. Pharmacol. 2016, 67, 801–817. [Google Scholar] [PubMed]
- Pourbakhsh, H.; Taghiabadi, E.; Abnous, K.; Hariri, A.T.; Hosseini, S.M.; Hosseinzadeh, H. Effect of Nigella sativa fixed oil on ethanol toxicity in rats. Iran. J. Basic Med. Sci. 2014, 17, 1020–1031. [Google Scholar] [PubMed]
- Sultan, M.T.; Butt, M.S.; Karim, R.; Zia-Ul-Haq, M.; Batool, R.; Ahmad, S.; Aliberti, L.; De Feo, V. Nigella sativa Fixed and Essential Oil Supplementation Modulates Hyperglycemia and Allied Complications in Streptozotocin-Induced Diabetes Mellitus. Evid. Based Complement. Alternat. Med. 2014, 2014, 826380. [Google Scholar] [CrossRef] [PubMed]
- El-Tahir, K.E.-D.H.; Bakeet, D.M. The black seed Nigella sativa linnaeus-a mine for multi cures: A plea for urgent clinical evaluation of its volatile oil. J. Taibah Univ. Med. Sci. 2006, 1, 1–19. [Google Scholar]
- Khare, C. Encyclopedia of Indian Medicinal Plants; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2004. [Google Scholar]
- Abdel-Sater, K.A. Gastroprotective effects of Nigella Sativa oil on the formation of stress gastritis in hypothyroidal rats. Int. J. Physiol. Pathophysiol. Pharmacol. 2009, 1, 143–149. [Google Scholar] [PubMed]
- Barakat, E.M.; El Wakeel, L.M.; Hagag, R.S. Effects of Nigella sativa on outcome of hepatitis C in Egypt. World J. Gastroenterol. 2013, 19, 2529–2536. [Google Scholar] [CrossRef] [PubMed]
- Ugur, A.R.; Dagi, H.T.; Ozturk, B.; Tekin, G.; Findik, D. Assessment of In vitro Antibacterial Activity and Cytotoxicity Effect of Nigella sativa Oil. Pharmacogn. Mag. 2016, 12 (Suppl. 4), S471–S474. [Google Scholar] [CrossRef] [PubMed]
- Fathy, M.; Nikaido, T. In vivo modulation of iNOS pathway in hepatocellular carcinoma by Nigella sativa. Environ. Health Prev. Med. 2013, 18, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Al-Ali, A.; Alkhawajah, A.A.; Randhawa, M.A.; Shaikh, N.A. Oral and intraperitoneal LD50 of thymoquinone, an active principle of Nigella sativa, in mice and rats. J. Ayub Med. Coll. Abbottabad 2008, 20, 25–27. [Google Scholar] [PubMed]
- Vahdati-Mashhadian, N.; Rakhshandeh, H.; Omidi, A. An investigation on LD50 and subacute hepatic toxicity of Nigella sativa seed extracts in mice. Pharmazie 2005, 60, 544–547. [Google Scholar] [PubMed]
- Zaoui, A.; Cherrah, Y.; Mahassini, N.; Alaoui, K.; Amarouch, H.; Hassar, M. Acute and chronic toxicity of Nigella sativa fixed oil. Phytomedicine 2002, 9, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Badary, O.A.; Al-Shabanah, O.A.; Nagi, M.N.; Al-Bekairi, A.M.; Elmazar, M.M.A. Acute and subchronic toxicity of thymoquinone in mice. Drug Dev. Res. 1998, 44, 56–61. [Google Scholar] [CrossRef]
- El-Dakhakhny, M. Studies on the Egyptian Nigella sativa L. IV. Some pharmacological properties of the seeds’ active principle in comparison to its dihydro compound and its polymer. Arzneimittelforschung 1965, 15, 1227–1229. [Google Scholar] [PubMed]
- Mansour, M.A.; Ginawi, O.T.; El-Hadiyah, T.; El-Khatib, A.S.; Al-Shabanah, O.A.; Al-Sawaf, H.A. Effects of volatile oil constituents of Nigella sativa on carbon tetrachloride-induced hepatotoxicity in mice: Evidence for antioxidant effects of thymoquinone. Res. Commun. Mol. Pathol. Pharmacol. 2001, 110, 239–251. [Google Scholar] [PubMed]
- Laskar, A.A.; Khan, M.A.; Rahmani, A.H.; Fatima, S.; Younus, H. Thymoquinone, an active constituent of Nigella sativa seeds, binds with bilirubin and protects mice from hyperbilirubinemia and cyclophosphamide-induced hepatotoxicity. Biochimie 2016, 127, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Houghton, P.J.; Zarka, R.; de las Heras, B.; Hoult, J.R. Fixed oil of Nigella sativa and derived thymoquinone inhibit eicosanoid generation in leukocytes and membrane lipid peroxidation. Planta Med. 1995, 61, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.A. Protective effects of thymoquinone and desferrioxamine against hepatotoxicity of carbon tetrachloride in mice. Life Sci. 2000, 66, 2583–2591. [Google Scholar] [CrossRef]
- Mohany, M.; El-Feki, M.; Refaat, I.; Garraud, O.; Badr, G. Thymoquinone ameliorates the immunological and histological changes induced by exposure to imidacloprid insecticide. J. Toxicol. Sci. 2012, 37, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Nili-Ahmadabadi, A.; Tavakoli, F.; Hasanzadeh, G.; Rahimi, H.; Sabzevari, O. Protective effect of pretreatment with thymoquinone against Aflatoxin B(1) induced liver toxicity in mice. Daru 2011, 19, 282–287. [Google Scholar] [PubMed]
- Nagi, M.N.; Alam, K.; Badary, O.A.; Al-Shabanah, O.A.; Al-Sawaf, H.A.; Al-Bekairi, A.M. Thymoquinone protects against carbon tetrachloride hepatotoxicity in mice via an antioxidant mechanism. Biochem. Mol. Biol. Int. 1999, 47, 153–159. [Google Scholar] [PubMed]
- Khalife, K.H.; Lupidi, G. Nonenzymatic reduction of thymoquinone in physiological conditions. Free Radic. Res. 2007, 41, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.; Al-Naqeep, G.; Chan, K.W. Nigella sativa thymoquinone-rich fraction greatly improves plasma antioxidant capacity and expression of antioxidant genes in hypercholesterolemic rats. Free Radic. Biol. Med. 2010, 48, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Nagi, M.N.; Almakki, H.A.; Sayed-Ahmed, M.M.; Al-Bekairi, A.M. Thymoquinone supplementation reverses acetaminophen-induced oxidative stress, nitric oxide production and energy decline in mice liver. Food Chem. Toxicol. 2010, 48, 2361–2365. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, W.M. Thymoquinone attenuates toxicity and oxidative stress induced by bisphenol A in liver of male rats. Pak. J. Biol. Sci. 2014, 17, 1152–1160. [Google Scholar] [CrossRef] [PubMed]
- Alenzi, F.Q.; El-Bolkiny Yel, S.; Salem, M.L. Protective effects of Nigella sativa oil and thymoquinone against toxicity induced by the anticancer drug cyclophosphamide. Br. J. Biomed. Sci. 2010, 67, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Al-Malki, A.L.; Sayed, A.A. Thymoquinone attenuates cisplatin-induced hepatotoxicity via nuclear factor kappa-beta. BMC Complement. Altern. Med. 2014, 14, 282. [Google Scholar] [CrossRef] [PubMed]
- Aras, S.; Gerin, F.; Aydin, B.; Ustunsoy, S.; Sener, U.; Turan, B.C.; Armutcu, F. Effects of sodium arsenite on the some laboratory signs and therapeutic role of thymoquinone in the rats. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 658–663. [Google Scholar] [PubMed]
- Aycan, I.O.; Tufek, A.; Tokgoz, O.; Evliyaoglu, O.; Firat, U.; Kavak, G.O.; Turgut, H.; Yuksel, M.U. Thymoquinone treatment against acetaminophen-induced hepatotoxicity in rats. Int. J. Surg. 2014, 12, 213–218. [Google Scholar] [CrossRef] [PubMed]
- El-Sheikh, A.A.; Morsy, M.A.; Abdalla, A.M.; Hamouda, A.H.; Alhaider, I.A. Mechanisms of Thymoquinone Hepatorenal Protection in Methotrexate-Induced Toxicity in Rats. Mediat. Inflamm. 2015, 2015, 859383. [Google Scholar] [CrossRef] [PubMed]
- Farag, M.M.; Ahmed, G.O.; Shehata, R.R.; Kazem, A.H. Thymoquinone improves the kidney and liver changes induced by chronic cyclosporine A treatment and acute renal ischaemia/reperfusion in rats. J. Pharm. Pharmacol. 2015, 67, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, K.M.; El-Amir, Y.O. Protective effects of thymoquinone and avenanthramides on titanium dioxide nanoparticles induced toxicity in Sprague-Dawley rats. Pathol. Res. Pract. 2017, 213, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Helal, G.K. Thymoquinone supplementation ameliorates acute endotoxemia-induced liver dysfunction in rats. Pak. J. Pharm. Sci. 2010, 23, 131–137. [Google Scholar] [PubMed]
- Mabrouk, A.; Bel Hadj Salah, I.; Chaieb, W.; Ben Cheikh, H. Protective effect of thymoquinone against lead-induced hepatic toxicity in rats. Environ. Sci. Pollut. Res. Int. 2016, 23, 12206–12215. [Google Scholar] [CrossRef] [PubMed]
- Suddek, G.M. Protective role of thymoquinone against liver damage induced by tamoxifen in female rats. Can. J. Physiol. Pharmacol. 2014, 92, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.S.; Abd Al Haleem, E.N.; El-Bakly, W.M.; Sherief, M.A. Thymoquinone alleviates nonalcoholic fatty liver disease in rats via suppression of oxidative stress, inflammation, apoptosis. Naunyn Schmiedebergs Arch. Pharmacol. 2016, 389, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Attia, A.; Ragheb, A.; Sylwestrowicz, T.; Shoker, A. Attenuation of high cholesterol-induced oxidative stress in rabbit liver by thymoquinone. Eur. J. Gastroenterol. Hepatol. 2010, 22, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Sayed-Ahmed, M.M.; Aleisa, A.M.; Al-Rejaie, S.S.; Al-Yahya, A.A.; Al-Shabanah, O.A.; Hafez, M.M.; Nagi, M.N. Thymoquinone attenuates diethylnitrosamine induction of hepatic carcinogenesis through antioxidant signaling. Oxid. Med. Cell. Longev. 2010, 3, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.Y.; Li, G.P.; Yang, P.; Xi, Z. Protective effect of thymoquinone on cholestatic rats with liver injury. Genet. Mol. Res. 2015, 14, 12247–12253. [Google Scholar] [CrossRef] [PubMed]
- Oguz, S.; Kanter, M.; Erboga, M.; Erenoglu, C. Protective effects of thymoquinone against cholestatic oxidative stress and hepatic damage after biliary obstruction in rats. J. Mol. Histol. 2012, 43, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elbaset, M.; Arafa, E.A.; El Sherbiny, G.A.; Abdel-Bakky, M.S.; Elgendy, A.N. Thymoquinone mitigate ischemia-reperfusion-induced liver injury in rats: A pivotal role of nitric oxide signaling pathway. Naunyn Schmiedebergs Arch. Pharmacol. 2017, 390, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.S.; Kamel, R.; Sherief, M.A. Effect of thymoquinone on hepatorenal dysfunction and alteration of CYP3A1 and spermidine/spermine N-1-acetyl-transferase gene expression induced by renal ischaemia-reperfusion in rats. J. Pharm. Pharmacol. 2011, 63, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Cikman, O.; Taysi, S.; Gulsen, M.T.; Demir, E.; Akan, M.; Diril, H.; Kiraz, H.A.; Karaayvaz, M.; Tarakcioglu, M. The radio-protective effects of caffeic acid phenethyl ester and thymoquinone in rats exposed to total head irradiation. Wien. Klin. Wochenschr. 2015, 127, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Elbarbry, F.; Ragheb, A.; Marfleet, T.; Shoker, A. Modulation of hepatic drug metabolizing enzymes by dietary doses of thymoquinone in female New Zealand White rabbits. Phytother. Res. 2012, 26, 1726–1730. [Google Scholar] [CrossRef] [PubMed]
- Nagi, M.N.; Almakki, H.A. Thymoquinone supplementation induces quinone reductase and glutathione transferase in mice liver: Possible role in protection against chemical carcinogenesis and toxicity. Phytother. Res. 2009, 23, 1295–1298. [Google Scholar] [CrossRef] [PubMed]
- Galaly, S.R.; Ahmed, O.M.; Mahmoud, A.M. Thymoquinone and curcumin prevent gentamicin-induced liver injury by attenuating oxidative stress, inflammation and apoptosis. J. Physiol. Pharmacol. 2014, 65, 823–832. [Google Scholar] [PubMed]
- Bai, T.; Yang, Y.; Wu, Y.L.; Jiang, S.; Lee, J.J.; Lian, L.H.; Nan, J.X. Thymoquinone alleviates thioacetamide-induced hepatic fibrosis and inflammation by activating LKB1-AMPK signaling pathway in mice. Int. Immunopharmacol. 2014, 19, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Ghazwani, M.; Zhang, Y.; Gao, X.; Fan, J.; Li, J.; Li, S. Anti-fibrotic effect of thymoquinone on hepatic stellate cells. Phytomedicine 2014, 21, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Bai, T.; Yao, Y.L.; Zhang, D.Q.; Wu, Y.L.; Lian, L.H.; Nan, J.X. Upregulation of SIRT1-AMPK by thymoquinone in hepatic stellate cells ameliorates liver injury. Toxicol. Lett. 2016, 262, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, A.H.; BaSalamah, M.A.; Idris, S.; Ahmad, J.; Refaat, B. The fibrolytic potentials of vitamin D and thymoquinone remedial therapies: Insights from liver fibrosis established by CCl4 in rats. J. Transl. Med. 2016, 14, 281. [Google Scholar] [CrossRef] [PubMed]
- Ke, X.; Zhao, Y.; Lu, X.; Wang, Z.; Liu, Y.; Ren, M.; Lu, G.; Zhang, D.; Sun, Z.; Xu, Z.; et al. TQ inhibits hepatocellular carcinoma growth in vitro and in vivo via repression of Notch signaling. Oncotarget 2015, 6, 32610–32621. [Google Scholar] [CrossRef] [PubMed]
- Raghunandhakumar, S.; Paramasivam, A.; Senthilraja, S.; Naveenkumar, C.; Asokkumar, S.; Binuclara, J.; Jagan, S.; Anandakumar, P.; Devaki, T. Thymoquinone inhibits cell proliferation through regulation of G1/S phase cell cycle transition in N-nitrosodiethylamine-induced experimental rat hepatocellular carcinoma. Toxicol. Lett. 2013, 223, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ning, Z.H.; Tai, H.W.; Long, S.; Qin, W.C.; Su, L.M.; Zhao, Y.H. Relationship between lethal toxicity in oral administration and injection to mice: Effect of exposure routes. Regul. Toxicol. Pharmacol. 2015, 71, 205–212. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Constituent | % Range |
|---|---|
| Carbohydrates | 33–34 |
| Oil | 31–35.5 |
| Protein | 16–19.9 |
| Fibre | 4.5–6.5 |
| Moisture | 5–7 |
| Saponins | 0.013 |
| Country | n |
|---|---|
| Saudi Arabia | 13 |
| China | 4 |
| Tunisia | 1 |
| Canada | 1 |
| Egypt | 7 |
| India | 2 |
| Malaysia | 1 |
| Iran | 1 |
| Turkey | 4 |
| USA | 2 |
| Model | n | % | Corresponding Summary Table |
|---|---|---|---|
| Toxic liver injury | 23 | 64 | Table 4 |
| Steatosis | 3 | 6 | Table 5 |
| Tumor | 3 | 8 | Table 6 |
| Cholestasis | 2 | 6 | Table 7 |
| IRI | 2 | 6 | Table 8 |
| Healthy liver | 2 | 6 | Table 9 |
| Irradiation | 1 | 3 | Table 10 |
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [56] | · MTX · Single dose (20 mg/kg ip) day 3 · Rat | · Dilatation and congestion of portal vein | · 10 mg/kg/d · po · 10 days | · Normal hepatic architecture | · ↓ TNF-α, COX-2 | · ↓ caspase 3 · ↓ NF-kB expression | · ↑ GSH · ↓ MDA, NO, iNOS | |||
| [54] | · SAs · 14 days · Rat | · Elevation of liver enyzmes · ↓ albumin | · 10 mg/kg bw · po · 14 days | · ↓ AST, ALT · ↑ albumin | · ↓ IL-6, MCP-1 and MIF | · ↓ NO | · ↓ TG, creatinine, cholesterol | |||
| [72] | · Gentamicin · 21 days (every 2nd day) · Rat | · Hydropic degeneration of hepatocytes, fatty changes, inflammatory cell infiltration, congestion of portal vein · Elevation of liver enyzmes, decrease of proteins | · 20 mg/kg bw · po · 21 days (every 2nd day) | · Normal hepatic architecture · ↓ AST, ALT, LDH, total bilirubin level · improvement of serum total protein, albumin and albumin/ globulin ratio | · ↓ TNF-α | · Caspase 3 and Bax expression reduced to normal · ↑ Bcl-2 | ||||
| [53] | · Cisplatin · Single injection (12 mg/kg ip) at day 28 · Rat | · Elevation of liver parameters · Vacuolar degeneration and hepatocellular necrosis | · 10 mg/kg/d · po · 28 days pretreatment + 28 days after Cisplatin | · Normal hepatic architecture · ↓ AST, ALT, ALP, γ-GT, total bilirubin, LDH | · ↓ TNF-α and IL-1β | · ↓ NF-kB expression | · ↑ Gpx, GSH, SOD, GST, CAT · ↓ MDA, NO | |||
| [61] | · Tamoxifen · 10 days (45 mg/kg/d ip) · Rat | · Elevation of liver parameters | · 50 mg/kg/d · po · 20 days, starting 10 days before intoxication | · ↓ AST, ALT, LDH, total bilirubin and γ-GT | · ↓ TNF-α | · Normalizing SOD activity · ↓ GSH, LPO | ||||
| [44] | · Imidacloprid · 28 days (0.21 mg/kg bw po) · Rat | · Congestion of central vein and blood sinusoids, widely distributed pyknotic nuclei and leukocyte infiltration · Elevation of liver enzymes | · 1 mg/kg · ip · 28 days (every 7th day) | · Improved hepatic architecture · ↓ AST, ALT, ALP | · ↑ phagocyte activity, chemokinesis, chemotaxis, total levels of Ig | · Inhibition of LPO | ||||
| [59] | · LPS · Single dose at day 6 · Rat | · Infiltration of inflammatory cells along with necrotic Damages · Elevation of liver enzymes | · 10 mg/kg/d · po · 7 days | · Reduced infiltration of inflammatory cells and necrotic damage · ↓ total bilirubin, ALP, γGT | · ↓ TNF-α | · ↓ caspase 3 | · normalization of GSH level · ↓ MDA | |||
| [75] | · Ethanol · 10 days 5% Vol., at day 11 5 g/kg po · Rat | · Hepatocyte enlargement, steatosis, inflammation · Elevation of liver enzymes | · 20 & 40 mg/kg · po · 10 days | · Reduction of histological changes · ↓ ALT, AST | · Enhancement of sirtuin 1 (SIRT1) expression | · Activation of LKB1 and AMPK phosphorylation · Inhibition of TGF-ß induced HSC activation | · ↓ TG | |||
| [40] | · CCI4 · Single injection (15 µL/kg ip) · Mouse | · Elevation of liver enyzmes | · 4, 8, 12.5, 25 & 50 mg/kg · ip · pretreatment 1 h before CCI4 injection | · ↓ AST, ALT, LDH | · ↓ MDA · ↑ nonprotein sulfhydryl (-SH) concentration | |||||
| [74] | · CCI4 · Single dose on day 6 · Mouse | · Not specified histological changes | · 25 mg/kg/d · po · 7 days | · Significant resistance to liver damage (not specified) | · Inactivation of NF-κB pathway | · Inhibition of upregulation of COL1A1 mRNA expression · Inhibition of HSCs · ↓ α-SMA | ||||
| [76] | · CCI4 · 3 µL/g twice weekly for 49 days · Rat | · Cellular infiltration and fibrous septa · Elevation of liver enyzmes | · 35 mg/kg/d · po · 3x/week from day 63 to 119 | · Less histological changes · ↓ ALT, AST | · ↓ TGF-ß1, IL-6, IL-22, TGF-ßRII, IL-6R, IL-22RA1+2, IL-10RA, IL-10RB · ↑ MMP9 mRNA | |||||
| [43] | · CCI4 · Single injection (20 µL/kg ip) · Mouse | · Elevation of liver enyzmes | · 16 mg/kg/d · po · 1 day (5 days before CCI4 injection) | · ↓ ALT, AST, LDH | · ↑ total SH content · ↓ MDA · Inhibition of LPO | |||||
| [46] | · CCI4 · Single injection (20 µL/kg ip) · Mouse | · Elevation of ALT | · 100 mg/kg · po · 1 day | · ↓ ALT | · Inhibition of LPO | |||||
| [73] | · Thiocetamide · 3x/week for 35 days · Mouse | · Necrosis, collagen deposition and infiltration of inflammatory cells in liver interstitial · Elevation of liver enyzmes | · 10 & 40 mg/kg · po · 35 days | · Less liver damage, inflammatory cell infiltration, collagen-I and α-SMA positive cells · ↓ ALT, AST | · ↓ protein and mRNA expression of α-SMA, collagen-I, TIMP-1 · AMK phosphorylation | |||||
| [52] | · Cyclophos- Phamide · 2 injections (200 mg/kg ip) · Rat | · Elevation of liver parameters | · 10 mg/kg/d · po · 12 days (every 2nd day) | · ↓ ALT, AST, bilirubin, γ-GT | · ↓ LPO | · ↓ urea, creatinine, TG, LDL, cholesterol | ||||
| [41] | · Cyclophos-phamide · Single dose (250 mg/kg ip) · Mouse | · Severe hemorrhage, necrosis, dilatation of blood vessels · Elevation of liver parameters | · 5 & 10 mg/kg/d · ip · 3 days | · Less hemorrhage and necrosis · ↓ ALT, AST, bilirubin | · ↑ SOD, CAT | |||||
| [45] | · Aflatoxin B · Single dose (2 mg/kg ip) · Mouse | · Inflammation, necrosis and hyperlasia of Kupffer cells, infiltration of mononuclear cells, dilatation of sinusoids and disruption of hepatocytes · Elevation of liver enyzmes | · 4, 5, 9 & 18 mg/kg · ip · 3 days pretreatment | · Improvement of histological changes · ↓ AST, ALT, ALP | · ↓ MDA · recovering GSH content | |||||
| [60] | · Lead · 35 days · Rat | · Degenerative changes in liver cell architecture · Elevation of liver paramters | · 5 mg/kg/d · po · 35 days | · Prevention of histological changes · ↓ ALT, AST, ALP, γ-GT | · ↑ TAS level | |||||
| [58] | · Titanium-dioxide nanoparticles · 42 days · Rat | · Congestion, necrosis and mononuclear infiltration · Elevation of liver enzymes | · 20 mg/kg · po · 42 days | · ↓ ALT | · ↓TNFα | · ↓ oxidative stress, DNA damage · ↑ TAS and GSH levels | ||||
| [55] | · Acet-Aminophen · Single dose (500 mg/kg po) · Rat | · Hepatic cell necrosis and toxicity · Elevation of liver enyzmes | · 15 mg/kg/d · po · 1 day | · Less necrosis · ↓ ALT, AST | · ↑ Gpx · ↓ GSSG & SOD activity, serum and tissue MDA levels | |||||
| [50] | · Acet-Aminophen · Single injection (500 mg/kg ip) · Mouse | · Elevation of ALT | · 0.5, 1 & 2 mg/kg/d · po · 5 days | · ↓ ALT | · ↓ lipid peroxide, GSH | · ↓ total nitrate/ nitrite, ATP | ||||
| [51] | · Bisphenol A · 28 days · Rat | · Elevation of liver parameters | · 10 mg/kg · po · 35 days | · ↓ AST, ALT, ALP, γ-GT and level of total bilirubin | · ↓ LPO · normalization of TAS, GSH, Gpx, GST, SOD, CAT | · ↓ total cholesterol · ↓ TG, LDL and vLDL · ↑ HDL | ||||
| [57] | · Chronic CsA treatment · 28 days · Rat | · Central vein congestion, hepatocyte vaculation, portal inflammation and fibrosis with bile ductular proliferation and focal necrosis · Elevation of liver enyzmes | · 10 mg/kg · po · 28 days | · Mild congestion of central vein and sinuses with minimal fibrotic spots · ↓ AST, ALT | · ↑ GSH, SOD · ↓ MDA | |||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [49] | · Hyper-Cholesterolemia (cholesterol diet) · 56 days · Rat | · Elevation of liver parameters | · 20, 50 & 100 mg/kg bw · po · 56 days | · ↓ ALT, γ-GT | · inhibition of OH · ↑ SOD1, CAT, Gpx | · ↓ plasma total cholesterol, LDL cholesterol, creatinine, urea | ||||
| [62] | · NASH (cholesterol diet) · 42 days · Rat | · Focal hepatic necrosis, vacuolation of hepatocytes associated with portal infiltration with inflammatory cells · Elevation of liver enyzmes | · 10 & 20 mg/kg/d · po · 42 days | · TQ 10 mg/kg/day: few inflammatory cells infiltration in between the few fatty changed hepatocytes · TQ 20 mg/kg/day: slight congestion of hepatic sinusoids and minimal vacuolation of sporadic hepatocytes · ↓ AST, ALT | · ↓ TNF-α · ↑ IL-10 | · ↓ Bax · ↑ Bcl-2 | · ↓ matrix metallo-proteinase-2 | · ↓ MDA | · ↓ TG · ↑ HDL | |
| [63] | · Hyper-cholesterolemia · 56 days · Rabbit | · Severe steatosis involving > 66% of hepatocytes, hepatocellular ballooning, mild mixed inflammation · Elevation of liver enyzmes | · 10 & 20 mg/kg/d · po · 56 days | · Reduction of steatosis and inflammation · ↓ AST, ALT | · ↓ protein carbonyl, MDA | · ↓ HDL, LDL, total/HDL-cholesterol | ||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti- Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [77] | · HCC (induced by injection of Hep3B cells sc) · Tumor volume ~150 mm3 · Mouse | · Growth of tumor nodules | · 5 & 20 mg/kg/d · sc · 31 days | · ↓ tumor volume | · ↑ expression of p21protein · inhibition of NICD1 and Bcl-2 | |||||
| [78] | · HCC (induced by NDEA) · Preventive: 16 weeks; Curative: 11 weeks · Rat | · Growth of tumor nodules · Loss of architecture with pleomorphism of nuclei · Elevated liver tumor markers and liver parameters | · 20 mg/kg bw · po · Preventive: 3x/week for 2 weeks prior experiment; Curative: 3x/week for last 5 weeks | · Reduced incidence of tumor nodules · Normal architecture, minimal inflammatory and few neoplastically transformed hepatocytes · ↓ liver tumor markers (AFP & CEA) · ↓ ALT, AST, LDH, ALP, γ-GT, total bilirubin | · ↓ AgNOR · Regulating G1/s phase cell cycle transition | |||||
| [64] | · HCC (induced by NDEA) · Single dose NDEA (200 mg/kg ip) · Rat | · Signs of severe hepatic injury (total score: 14) · Elevation of liver parameters | · 4 mg/kg/d · po · 7 days (5 days before, 2 days after NDEA) | · Mild hepatic injury (total score: 6) · ↓ ALT, ALP, total bilirubin | · ↓ thiobarbituric acid reactive substance · ↑ GSH, GPx, GST, CAT | · ↓ total nitrate/ nitrite | ||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [65] | · Bile duct ligation · Rat | · Hepatic necrosis and fibrosis | · 25 & 50 mg/kg · po · 2 weeks (start 3 days prior to ligation) | · Less necrosis and fibrosis | · ↓ HP and MDA · ↑ SOD and Gpx | |||||
| [66] | · Bile duct ligation · Rat | · Bile duct proliferation and fibrosis | · 50 mg/kg · po · 2 weeks (start 3 days prior to ligation) | · Attenuation of histological changes | · ↓ tissue hydroxyproline and MDA · ↑ SOD and Gpx | |||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [67] | · Occlusion of hepatic pedicule · 30 min · Rat | · Congestion of central vein, dilatation of interstitial spaces, activation of Kupffer cells, hepatocytes with pyknotic nuclei, cytoplasmic degeneration, and inflammatory cell infiltration · Elevation of liver enzymes | · 20 mg/kg/d · po · 10 days | · Moderate congestion of central vein, slight dilation of blood sinusoids · ↓ AST, ALT | · ↓ MPO | · ↓ NO, eNOS, iNOS, NOSTRIN · ↑ GSH | ||||
| [68] | · Occlusion of renal artery · 30 min · Rat | · Elevation of ALT | · 10 mg/kg bw · po · 10 days | · ↓ ALT | · ↓ MDA, SSAT mRNA expression · ↑ GST, SOD | · ↓CYP3A1 | ||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [71] | · Mouse | · 1, 2 & 4 mg/kg/d · po · 5 days | · ↑ GST, quinone reductase | |||||||
| [70] | · Rabbit | · 10 & 20 mg/kg/d · po · 56 days | · ↑ GST, Gred and Gpx | · ↓ CYP1A, CYP2A4 | ||||||
| Injury Model | TQ | Effect of TQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | · Model · Duration of Induction · Species | Toxic Effect | · Dose · Route of Administration · Duration of Treatment | Reduction of Hepatic Damage | Anti-Inflammatory | Anti-/Pro-Apoptotic | Antifibrotic | Anti-Carcinogenic | Anti-Oxidative | Others |
| [69] | · 5 Gy gamma · Single dose · Rat | · Not analyzed | · 50 mg/kg/d · ip · 10 days (start 30 min prior irradiation) | · ↓ TOS, OSI, LOOH · ↑ PON | ||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tekbas, A.; Huebner, J.; Settmacher, U.; Dahmen, U. Plants and Surgery: The Protective Effects of Thymoquinone on Hepatic Injury—A Systematic Review of In Vivo Studies. Int. J. Mol. Sci. 2018, 19, 1085. https://doi.org/10.3390/ijms19041085
Tekbas A, Huebner J, Settmacher U, Dahmen U. Plants and Surgery: The Protective Effects of Thymoquinone on Hepatic Injury—A Systematic Review of In Vivo Studies. International Journal of Molecular Sciences. 2018; 19(4):1085. https://doi.org/10.3390/ijms19041085
Chicago/Turabian StyleTekbas, Aysun, Jutta Huebner, Utz Settmacher, and Uta Dahmen. 2018. "Plants and Surgery: The Protective Effects of Thymoquinone on Hepatic Injury—A Systematic Review of In Vivo Studies" International Journal of Molecular Sciences 19, no. 4: 1085. https://doi.org/10.3390/ijms19041085