Low Serum Levels of (Dihydro-)Ceramides Reflect Liver Graft Dysfunction in a Real-World Cohort of Patients Post Liver Transplantation

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Low Serum Long and Very Long Chain (Dihydro-) Ceramides Associate with History of Graft Rejection and Ischemic Type Biliary Lesions (ITBL)
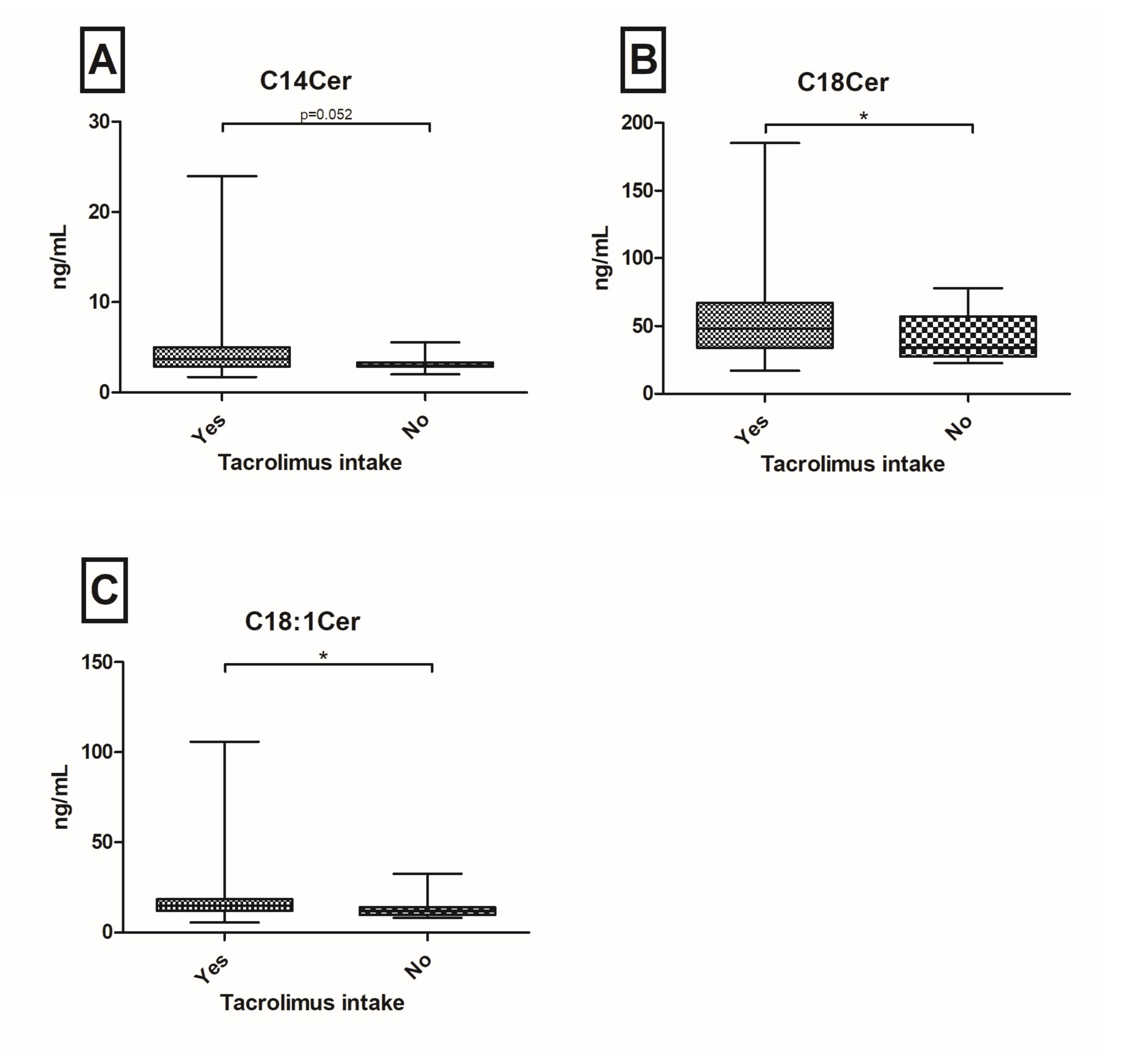
2.3. Tacrolimus Based Immunosuppressive Therapy Associates with Upregulated Serum Cer Levels
2.4. Analyses of Serum Cer’s Concerning Pre-OLT Hepatopathy, HCC, Donors’ Characteristics and Time Between OLT and Blood Withdrawal
3. Discussion
4. Patients and Methods
4.1. Patients’ Selection
4.2. Determination of Sphingolipid Concentrations by High-Performance Liquid Chromatography Tandem Mass Spectrometry
4.3. Statistical Analyses
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Reddy, S.S.; Civan, J.M. From child-pugh to model for end-stage liver disease: Deciding who needs a liver transplant. Med. Clin. North. Am. 2016, 100, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Lankarani, K.B.; Eshraghian, K.; Malek-Hosseini, S.A.; Janghorban, P.; Geramizadeh, B.; Eshraghian, A. Outcomes of liver transplantation for patients with acute liver failure. Arch. Iran. Med. 2013, 16, 64–67. [Google Scholar] [PubMed]
- Lerut, J.; Julliard, O.; Ciccarelli, O.; Lannoy, V.; Gofette, P. Hepatocellular cancer and liver transplantation: A western experience. Recent Results Cancer Res. 2013, 190, 127–144. [Google Scholar] [PubMed]
- Starzl, T.E.; Groth, C.G.; Brettschneider, L.; Penn, I.; Fulginiti, V.A.; Moon, J.B.; Blanchard, H.; Martin, A.J., Jr.; Porter, K.A. Orthotopic homotransplantation of the human liver. Ann. Surg. 1968, 168, 392–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Mahony, C.A.; Goss, J.A. The future of liver transplantation. Tex. Heart Inst. J. 2012, 39, 874–875. [Google Scholar] [PubMed]
- Waits, S.A.; Kim, E.K.; Terjimanian, M.N.; Tishberg, L.M.; Harbaugh, C.M.; Sheetz, K.H.; Sonnenday, C.J.; Sullivan, J.; Wang, S.C.; Englesbe, M.J. Morphometric age and mortality after liver transplant. JAMA Surg. 2014, 149, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Hinz, U.; Hillebrand, N.; Ganten, T.; Gotthardt, D.; Longerich, T.; Schirmacher, P.; Schemmer, P. The meld score predicts the short-term and overall survival after liver transplantation in patients with primary sclerosing cholangitis or autoimmune liver diseases. Langenbecks Arch. Surg. 2014, 399, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, J.; Riaz, D.R.; Shi, G.; Liu, C.; Dai, Y. Outcomes of liver transplantation for nonalcoholic steatohepatitis: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Fung, J.J.; Eliasziw, M.; Todo, S.; Jain, A.; Demetris, A.J.; McMichael, J.P.; Starzl, T.E.; Meier, P.; Donner, A. The pittsburgh randomized trial of tacrolimus compared to cyclosporine for hepatic transplantation. J. Am. Coll. Surg. 1996, 183, 117–125. [Google Scholar] [PubMed]
- Wiesner, R.H. A long-term comparison of tacrolimus (FK506) versus cyclosporine in liver transplantation: A report of the united states FK506 study group. Transplantation 1998, 66, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Batts, K.P. Acute and chronic hepatic allograft rejection: Pathology and classification. Liver Transpl. Surg. 1999, 5, S21–S29. [Google Scholar] [PubMed]
- Pfitzmann, R.; Nussler, N.C.; Hippler-Benscheidt, M.; Neuhaus, R.; Neuhaus, P. Long-term results after liver transplantation. Transpl. Int. 2008, 21, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Benitez, C.; Londono, M.C.; Miquel, R.; Manzia, T.M.; Abraldes, J.G.; Lozano, J.J.; Martinez-Llordella, M.; Lopez, M.; Angelico, R.; Bohne, F.; et al. Prospective multicenter clinical trial of immunosuppressive drug withdrawal in stable adult liver transplant recipients. Hepatology 2013, 58, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- De la Garza, R.G.; Sarobe, P.; Merino, J.; Lasarte, J.J.; D’Avola, D.; Belsue, V.; Delgado, J.A.; Silva, L.; Inarrairaegui, M.; Sangro, B.; et al. Trial of complete weaning from immunosuppression for liver transplant recipients: Factors predictive of tolerance. Liver Transpl. 2013, 19, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Nojima, H.; Freeman, C.M.; Gulbins, E.; Lentsch, A.B. Sphingolipids in liver injury, repair and regeneration. Biol. Chem. 2015, 396, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Grammatikos, G.; Muhle, C.; Ferreiros, N.; Schroeter, S.; Bogdanou, D.; Schwalm, S.; Hintereder, G.; Kornhuber, J.; Zeuzem, S.; Sarrazin, C.; et al. Serum acid sphingomyelinase is upregulated in chronic hepatitis c infection and non alcoholic fatty liver disease. Biochim. Biophys. Acta 2014, 1841, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Grammatikos, G.; Schoell, N.; Ferreiros, N.; Bon, D.; Herrmann, E.; Farnik, H.; Koberle, V.; Piiper, A.; Zeuzem, S.; Kronenberger, B.; et al. Serum sphingolipidomic analyses reveal an upregulation of c16-ceramide and sphingosine-1-phosphate in hepatocellular carcinoma. Oncotarget 2016, 7, 18095–18105. [Google Scholar] [CrossRef] [PubMed]
- Grammatikos, G.; Ferreiros, N.; Waidmann, O.; Bon, D.; Schroeter, S.; Koch, A.; Herrmann, E.; Zeuzem, S.; Kronenberger, B.; Pfeilschifter, J. Serum sphingolipid variations associate with hepatic decompensation and survival in patients with cirrhosis. PLoS ONE 2015, 10, e0138130. [Google Scholar] [CrossRef] [PubMed]
- Dennis, E.A.; Deems, R.A.; Harkewicz, R.; Quehenberger, O.; Brown, H.A.; Milne, S.B.; Myers, D.S.; Glass, C.K.; Hardiman, G.; Reichart, D.; et al. A mouse macrophage lipidome. J. Biol. Chem. 2010, 285, 39976–39985. [Google Scholar] [CrossRef] [PubMed]
- Sims, K.; Haynes, C.A.; Kelly, S.; Allegood, J.C.; Wang, E.; Momin, A.; Leipelt, M.; Reichart, D.; Glass, C.K.; Sullards, M.C.; et al. Kdo2-lipid a, a tlr4-specific agonist, induces de novo sphingolipid biosynthesis in raw264.7 macrophages, which is essential for induction of autophagy. J. Biol. Chem. 2010, 285, 38568–38579. [Google Scholar] [CrossRef] [PubMed]
- Maceyka, M.; Spiegel, S. Sphingolipid metabolites in inflammatory disease. Nature 2014, 510, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Bikman, B.T.; Summers, S.A. Ceramides as modulators of cellular and whole-body metabolism. J. Clin. Investig. 2011, 121, 4222–4230. [Google Scholar] [CrossRef] [PubMed]
- Zabielski, P.; Baranowski, M.; Zendzian-Piotrowska, M.; Blachnio, A.; Gorski, J. Partial hepatectomy activates production of the pro-mitotic intermediates of the sphingomyelin signal transduction pathway in the rat liver. Prostaglandins Other Lipid Mediat. 2007, 83, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Huwiler, A.; Kolter, T.; Pfeilschifter, J.; Sandhoff, K. Physiology and pathophysiology of sphingolipid metabolism and signaling. Biochim. Biophys. Acta 2000, 1485, 63–99. [Google Scholar] [CrossRef]
- Siddique, M.M.; Li, Y.; Chaurasia, B.; Kaddai, V.A.; Summers, S.A. Dihydroceramides: From bit players to lead actors. J. Biol. Chem. 2015, 290, 15371–15379. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Grosch, S.; Schiffmann, S.; Geisslinger, G. Chain length-specific properties of ceramides. Prog. Lipid Res. 2012, 51, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Karahatay, S.; Thomas, K.; Koybasi, S.; Senkal, C.E.; Elojeimy, S.; Liu, X.; Bielawski, J.; Day, T.A.; Gillespie, M.B.; Sinha, D.; et al. Clinical relevance of ceramide metabolism in the pathogenesis of human head and neck squamous cell carcinoma (HNSCC): Attenuation of C(18)-ceramide in HNSCC tumors correlates with lymphovascular invasion and nodal metastasis. Cancer Lett. 2007, 256, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Mesicek, J.; Lee, H.; Feldman, T.; Jiang, X.; Skobeleva, A.; Berdyshev, E.V.; Haimovitz-Friedman, A.; Fuks, Z.; Kolesnick, R. Ceramide synthases 2, 5, and 6 confer distinct roles in radiation-induced apoptosis in hela cells. Cell Signal. 2010, 22, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.L., Jr.; Matsko, C.M.; Lotze, M.T.; Amoscato, A.A. Mass spectrometric identification of increased c16 ceramide levels during apoptosis. J. Biol. Chem. 1999, 274, 30580–30588. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Uchinami, H.; Bielawski, J.; Schwabe, R.F.; Hannun, Y.A.; Brenner, D.A. Roles for C16-ceramide and sphingosine 1-phosphate in regulating hepatocyte apoptosis in response to tumor necrosis factor-alpha. J. Biol. Chem. 2005, 280, 27879–27887. [Google Scholar] [CrossRef] [PubMed]
- Guicciardi, M.E.; Gores, G.J. Apoptosis: A mechanism of acute and chronic liver injury. Gut 2005, 54, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L. Mechanisms of hepatic fibrogenesis. Gastroenterology 2008, 134, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Kolesnick, R. The therapeutic potential of modulating the ceramide/sphingomyelin pathway. J. Clin. Investig. 2002, 110, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Charles, R.; Sandirasegarane, L.; Yun, J.; Bourbon, N.; Wilson, R.; Rothstein, R.P.; Levison, S.W.; Kester, M. Ceramide-coated balloon catheters limit neointimal hyperplasia after stretch injury in carotid arteries. Circ. Res. 2000, 87, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Blackinton, D.; Omar, I.; Kouttab, N.; Myrick, D.; Klostergaard, J.; Wanebo, H. Combined cytotoxic action of paclitaxel and ceramide against the human tu138 head and neck squamous carcinoma cell line. Cancer Chemother. Pharmacol. 2000, 46, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A.; Li, X.K.; Funeshima, N.; Enosawa, S.; Amemiya, H.; Kitajima, M.; Suzuki, S. Immunosuppressive therapy using fty720 combined with tacrolimus in rat liver transplantation. Surgery 2000, 127, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Enosawa, S.; Kakefuda, T.; Amemiya, H.; Hoshino, Y.; Chiba, K. Long-term graft acceptance in allografted rats and dogs by treatment with a novel immunosuppressant, FTY720. Transplant. Proc. 1996, 28, 1375–1376. [Google Scholar] [PubMed]
- Trayssac, M.; Galvani, S.; Auge, N.; Sabbadini, R.; Calise, D.; Mucher, E.; Sallusto, F.; Thomsen, M.; Salvayre, R.; Negre-Salvayre, A. Role of sphingosine-1-phosphate in transplant vasculopathy evoked by anti-hla antibody. Am. J. Transplant. 2015, 15, 2050–2061. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.; Emmler, T.; Schwalm, S.; Ebadi, M.; Heringdorf, D.M.; Nieuwenhuis, B.; Kleuser, B.; Huwiler, A.; Pfeilschifter, J. Glucocorticoids protect renal mesangial cells from apoptosis by increasing cellular sphingosine-1-phosphate. Kidney Int. 2010, 77, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Weiler, N.; Bilge, N.; Troetschler, S.; Vermehren, J.; Schnitzbauer, A.A.; Herrmann, E.; Sarrazin, C.; Zeuzem, S.; Welker, M.W. Conversion from sirolimus to everolimus in long-term liver graft recipients. J. Clin. Pharmacol. 2017, 57, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Banff schema for grading liver allograft rejection: An international consensus document. Hepatology 1997, 25, 658–663.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients (n = 149) |
|---|---|
| Age, years; mean (range) | 56 (21–79) |
| Gender | |
| Female, n (%) | 55 (37%) |
| Male, n (%) | 94 (63%) |
| Body mass index; mean (range) | 26 (16.4–46.5) |
| Blood type A/B/AB/0, n (%) | 57 (38%)/23 (15%)/7 (4.6%)/39 (26%) |
| ALT, IU/L; mean (range) | 30 (7–132) |
| AST, IU/L; mean (range) | 30 (13–100) |
| GGT, IU/L; mean (range) | 89 (8–1525) |
| Bilirubin, mg/dL; mean (range) | 0.8 (0.1–19) |
| Creatinine, mg/dL; mean (range) | 1.3 (0.64–9.76) |
| Triglyceride, mg/dL; mean (range) | 134 (40–411) |
| Cholesterol, mg/dL; mean (range) | 178 (38–331) |
| Albumin, mg/dL; mean (range) | 4.3 (3–4.9) |
| International normalized ratio; mean (range) | 1.07 (0.84–3.38) |
| Tacrolimus though level, ng/ml; mean (range) of 133 patients | 5.9 (2.4–23.1) |
| Aetiology pre-OLT chronic liver disease | |
| Hepatitis B, n (%) | 18 (12%) |
| Hepatitis B/D coinfection, n (%) | 5 (3%) |
| Hepatitis C, n (%) | 34 (22.8%) |
| Hepatitis B/C coinfection, n (%) | 7 (4.7%) |
| Alcohol intake, n (%) | 35 (23%) |
| Non-alcoholic steatohepatitis, n (%) | 1 (0.7%) |
| Primary sclerosing cholangitis, n (%) | 5 (3.6%) |
| Primary biliary cholangitis, n (%) | 4 (2.7%) |
| Cryptogenic, n (%) | 17 (11%) |
| Other, n (%) | 32 (21.5%) |
| HCC pre-OLT, n (%) | 43 (28.9%) |
| CMV-IgG-antibody positive, n (%) | 109 (73%) |
| Graft rejection, n (%) | 29 (19.5%) |
| Ischemic type biliary lesions, n (%) | 15 (10%) |
| Immunosuppressive therapy | |
| Tacrolimus, n (%) | 133 (89%) |
| Mycophenolate-mofetil, n (%) | 79 (53%) |
| Cyclosporine A, n (%) | 8 (5%) |
| mTor-Inhibitors, n (%) | 12 (8%) |
| Steroids, n (%) | 16 (10.7%) |
| Basiliximab, n (%) | 2 (1%) |
| Donors’ gender | |
| Female, n (%) | 50 (33.5%) |
| Male, n (%) | 62 (41.6%) |
| Not applicable, n (%) | 37 (24.8%) |
| Grafts’ age, years; mean (range) | 58 (17–89) |
| AB0-matching: identical/compatible/incompatible, n (%) | 114 (77%)/10 (6.7%)/0 (0%) |
| SL | Patients’ Age at BW | AST | ALT | GGT | Chol | TG | Tacrolimus Though Level | Grafts’ Age at BW | Time Between OLT and BW |
|---|---|---|---|---|---|---|---|---|---|
| Sphingosine | 0.149 | 0.030 | 0.147 | 0.062 | 0.120 | 0.095 | −0.0001 | 0.104 | −00.031 |
| Sphinganine | 0.047 | 0.036 | 0.194 * | 0.049 | 0.082 | 0.065 | −0.039 | 0.114 | −0.031 |
| S1P | −0.014 | 0.069 | 0.171 * | 0.059 | 0.225 ** | 0.114 | 0.027 | −0.111 | −0.014 |
| dhS1P | −0.046 | 0.104 | 0.211 ** | 0.049 | 0.211 ** | 0.165 * | 0.037 | −0.040 | 0.030 |
| C24Cer | 0.214 ** | −0.296 *** | −0.050 | −0.145 | 0.606 *** | 0.429 *** | 0.159 | −0.110 | −0.186 * |
| C16Cer | 0.059 | 0.065 | 0.016 | 0.164 * | 0.205 ** | 0.124 | −0.079 | 0.081 | −0.199 * |
| C14Cer | 0.069 | 0.037 | 0.125 | 0.101 | 0.284 *** | 0.129 | −0.014 | −0.018 | −0.096 |
| C18Cer | 0.308 *** | −0.029 | 0.115 | 0.203 * | 0.427 *** | 0.455 *** | −0.051 | −0.086 | −0.142 |
| C20Cer | 0.306 *** | −0.215 ** | −0.071 | 0.060 | 0.396 *** | 0.418 *** | 0.007 | −0.154 | −0.167 * |
| C18:1Cer | 0.031 | −0.041 | −0.0003 | 0.022 | 0.217 ** | 0.136 | 0.008 | 0.075 | −0.094 |
| C24:1Cer | 0.291 *** | −0.153 | −0.004 | 0.082 | 0.401 *** | 0.444 *** | 0.108 | −0.197 * | −0.208 * |
| C16DHC | −0.010 | 0.142 | 0.076 | 0.137 | 0.039 | 0.040 | −0.082 | 0.106 | −0.072 |
| C18DHC | 0.273 *** | −0.034 | 0.078 | 0.142 | 0.284 *** | 0.377 *** | −0.071 | 0.030 | −0.093 |
| C24DHC | 0.161 | −0.104 | 0.101 | −0.055 | 0.529 *** | 0.313 *** | 0.062 | 0.001 | −0.130 |
| C24:1DHC | 0.199 * | 0.109 | 0.213 ** | 0.186 * | 0.317 *** | 0.272 *** | −0.063 | 0.033 | −0.040 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variable | p Value | OR (95% CI) | p Value | OR (95% CI) |
| Age | 0.919 | 0.997 (0.942–1.055) | ||
| Gender patient | 0.339 | 1.704 (0.572–5.081) | ||
| Gender donor | 0.938 | 0.959 (0.332–2.770) | ||
| ITBL | 0.388 | 1.902 (0.441–8.194) | ||
| HCC pre-OLT | 0.353 | 0.581 (0.185–1.828) | ||
| Tacrolimus intake | 0.207 | 0.296 (0.045–1.965) | ||
| ALT | 0.091 | 0.980 (0.957–1.003) | ||
| AST | 0.138 | 0.973 (0.938–1.009) | ||
| GGT | 0.892 | 1.000 (0.997–1.003) | ||
| Sphingosine-1-phosphate | 0.749 | 0.999 (0.993–1.005) | ||
| Sphinganine | 0.932 | 0.992 (0.823–1.195) | ||
| Sphinganine-1-phosphate | 0.449 | 0.993 (0.973–1.012) | ||
| C18Cer | 0.475 | 1.009 (0.985–1.033) | 0.072 | 0.973 (0.945–1.002) |
| C18:1Cer | 0.571 | 1.016 (0.962–1.072) | ||
| C20Cer | 0.225 | 1.017 (0.990–1.045) | ||
| C24Cer | 0.048 | 1.001 (1.000–1.002) | 0.039 | 1.001 (1.000–1.002) |
| C18DHC | 0.073 | 1.084 (0.992–1.183) | 0.035 | 1.132 (1.009–1.269) |
| C24:1DHC | 0.113 | 1.018 (0.994–1.043) | ||
| Age | 0.311 | 1.032 (0.971–1.097) | ||
| Gender patient | 0.292 | 2.000 (0.551–7.256) | 0.083 | 3.718 (0.842–16.424) |
| Gender donor | 0.863 | 0.894 (0.251–3.190) | ||
| Graft rejection | 0.388 | 1.902 (0.441–8.195) | ||
| HCC pre-OLT | 0.818 | 0.857 (0.230–3.189) | ||
| Tacrolimus intake | 0.933 | 2.741×104 (0.000–3.39×10107) | ||
| ALT | 0.204 | 0.984 (0.959–1.009) | ||
| AST | 0.294 | 0.979 (0.941–1.019) | ||
| GGT | 0.003 | 0.994 (0.989–0.998) | 0.006 | 0.994 (0.989–0.998) |
| C16Cer | 0.931 | 1.001 (0.982–1.020) | ||
| C18DHC | 0.025 | 1.158 (1.019–1.316) | 0.042 | 1.172 (1.006–1.366) |
| C24DHC | 0.082 | 1.024 (0.997–1.052) | ||
| C24:1DHC | 0.375 | 1.012 (0.986–1.040) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mücke, V.T.; Gerharz, J.; Jakobi, K.; Thomas, D.; Ferreirós Bouzas, N.; Mücke, M.M.; Trötschler, S.; Weiler, N.; Welker, M.-W.; Zeuzem, S.; et al. Low Serum Levels of (Dihydro-)Ceramides Reflect Liver Graft Dysfunction in a Real-World Cohort of Patients Post Liver Transplantation. Int. J. Mol. Sci. 2018, 19, 991. https://doi.org/10.3390/ijms19040991
Mücke VT, Gerharz J, Jakobi K, Thomas D, Ferreirós Bouzas N, Mücke MM, Trötschler S, Weiler N, Welker M-W, Zeuzem S, et al. Low Serum Levels of (Dihydro-)Ceramides Reflect Liver Graft Dysfunction in a Real-World Cohort of Patients Post Liver Transplantation. International Journal of Molecular Sciences. 2018; 19(4):991. https://doi.org/10.3390/ijms19040991
Chicago/Turabian StyleMücke, Victoria Therese, Janis Gerharz, Katja Jakobi, Dominique Thomas, Nerea Ferreirós Bouzas, Marcus Maximilian Mücke, Sven Trötschler, Nina Weiler, Martin-Walter Welker, Stefan Zeuzem, and et al. 2018. "Low Serum Levels of (Dihydro-)Ceramides Reflect Liver Graft Dysfunction in a Real-World Cohort of Patients Post Liver Transplantation" International Journal of Molecular Sciences 19, no. 4: 991. https://doi.org/10.3390/ijms19040991