Different Original and Biosimilar TNF Inhibitors Similarly Reduce Joint Destruction in Rheumatoid Arthritis—A Network Meta-Analysis of 36 Randomized Controlled Trials

 and
and
Abstract
:1. Introduction
2. Results
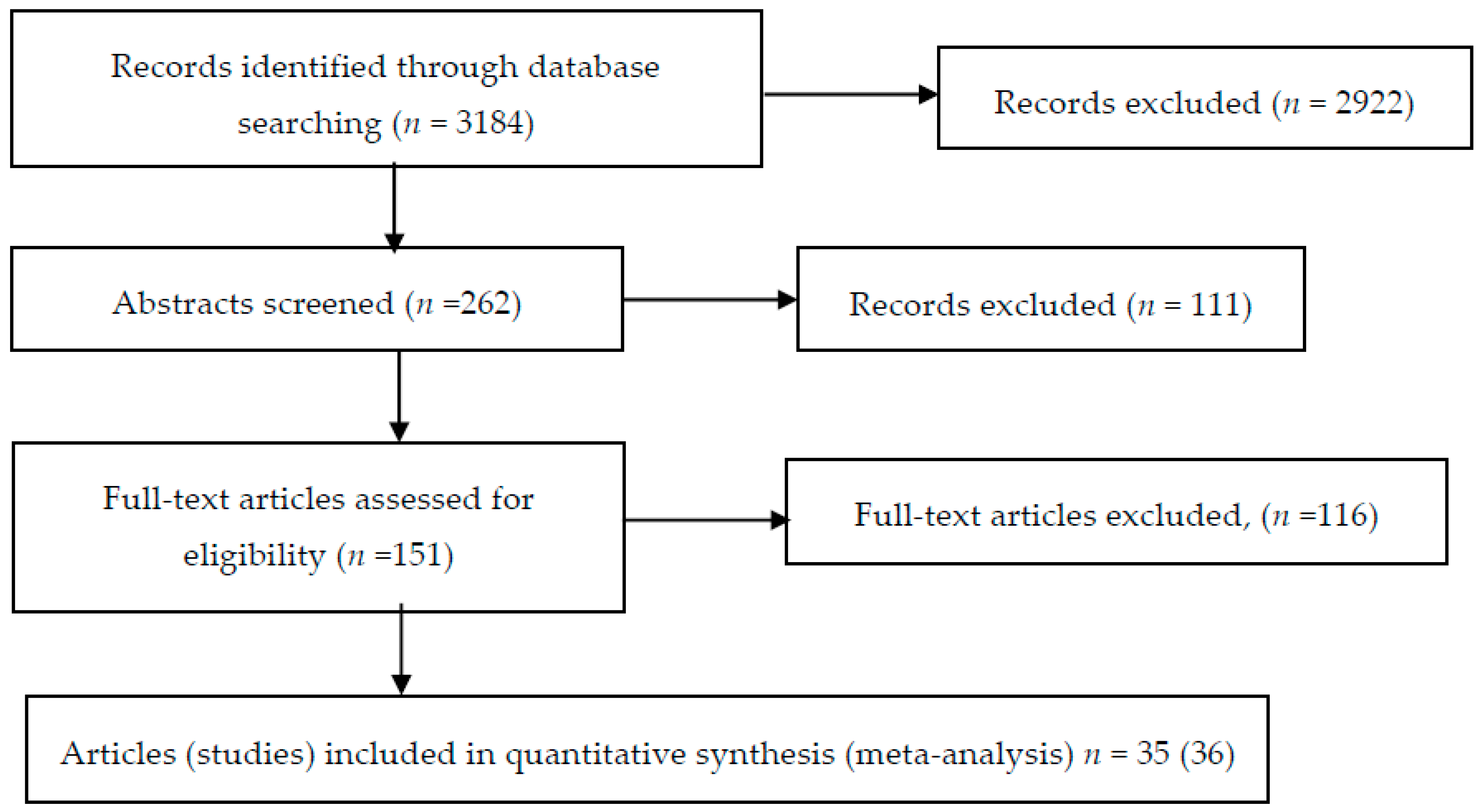
2.1. Result of the Search
2.2. Description of Included Studies
2.3. Risk of Bias in Included Studies
2.4. Trial Network
2.5. Treatment Effects
2.6. Additional Analyses
2.7. Inconsistency Checks
2.8. Model Fitness and Comparison
3. Discussion
3.1. Limitations
3.2. Strengths
4. Materials and Methods
4.1. Types of Studies
4.2. Types of Participants
4.3. Types of Interventions
4.4. Type of Outcome
4.5. Search Method for Identification of Studies
4.6. Study Selection
4.7. Data Extraction and Management
4.8. Assessment of Risk of Bias in Included Studies
4.9. Measure of Treatment Effect
4.10. Missing Data
4.11. Data Synthesis
4.12. Model Specification and Parameter Estimation
Author Contributions
Funding
Conflicts of Interest
References
- Lim, H.; Lee, S.; Lee, H.; Lee, J.; Son, J.; Shin, W.; Heo, Y.S. Structural Biology of the TNFα Antagonists Used in the Treatment of Rheumatoid Arthritis. Int. J. Mol. Sci. 2018, 19, 768. [Google Scholar] [CrossRef] [PubMed]
- Hassell, A.B.; Davis, M.J.; Fowler, P.D.; Clarke, S.; Fisher, J.; Shadforth, M.F.; Jones, P.W.; Dawes, P.T. The relationship between serial measures of disease activity and outcome in rheumatoid arthritis. Q. J. Med. 1993, 86, 601–607. [Google Scholar] [PubMed]
- Graudal, N.; Tarp, U.; Jurik, A.G.; Galløe, A.M.; Garred, P.; Milman, N.; Graudal, H.K. Inflammatory patterns in rheumatoid arthritis estimated by the number of swollen and tender joints, the erythrocyte sedimentation rate, and hemoglobin: Long-term course and association to radiographic progression. J. Rheumatol. 2000, 27, 47–57. [Google Scholar] [PubMed]
- Graudal, N. The natural history and prognosis of rheumatoid arthritis: Association of radiographic outcome with process variables, joint motion and immune proteins. Scand. J. Rheumatol. Suppl. 2004, 118, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.J.; Maini, R.N.; Feldmann, M.; Kalden, J.R.; Antoni, C.; Smolen, J.S.; Leeb, B.; Breedveld, F.C.; Macfarlane, J.D.; Bijl, H. Randomised double-blind comparison of chimeric monoclonal antibody to tumour necrosis factor alpha (cA2) versus placebo in rheumatoid arthritis. Lancet 1994, 344, 1105–1110. [Google Scholar] [CrossRef]
- Murray, K.M.; Dahl, S.L. Recombinant human tumor necrosis factor receptor (p75) Fc fusion protein (TNFR:Fc) in rheumatoid arthritis. Ann. Pharmacother. 1997, 31, 1335–1338. [Google Scholar] [CrossRef]
- Graudal, N.; Jürgens, G. Similar effects of disease-modifying antirheumatic drugs, glucocorticoids, and biologic agents on radiographic progression in rheumatoid arthritis: Meta-analysis of 70 randomized placebo-controlled or drug-controlled studies, including 112 comparisons. Arthritis Rheum. 2010, 62, 2852–2863. [Google Scholar] [CrossRef]
- Graudal, N.; Hubeck-Graudal, T.; Tarp, S.; Christensen, R.; Jürgens, G. Effect of combination therapy on joint destruction in rheumatoid arthritis: A network meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e106408. [Google Scholar] [CrossRef]
- Lunn, D.J.; Thomas, A.; Best, N.; Spiegelhalter, D. WinBUGS—A Bayesian modelling framework: Concepts, structure, and extensibility. Stat. Comput. 2000, 10, 325–337. [Google Scholar] [CrossRef]
- Aaltonen, K.J.; Virkki, L.M.; Malmivaara, A.; Konttinen, Y.T.; Nordström, D.C.; Blom, M. Systematic Review and Meta-Analysis of the Efficacy and Safety of Existing TNF Blocking Agents in Treatment of Rheumatoid Arthritis. PLoS ONE 2012, 7, e30275. [Google Scholar] [CrossRef]
- Schmitz, S.; Adams, R.; Walsh, C.D.; Barry, M.; FitzGerald, O. A mixed treatment comparison of the efficacy of anti-TNF agents in rheumatoid arthritis for methotrexate non-responders demonstrates differences between treatments: A Bayesian approach. Ann. Rheum. Dis. 2012, 71, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Sharp, J.T. Scoring radiographic abnormalities in rheumatoid arthritis. Radiol. Clin. North Am. 1996, 34, 233–241. [Google Scholar] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Hannonen, P.; Möttönen, T.; Hakola, M.; Oka, M. Sulfasalazine in early rheumatoid arthritis. A 48-week double-blind, prospective, placebo-controlled study. Arthritis Rheum. 1993, 36, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Kalden, J.R.; Scott, D.L.; Rozman, B.; Kvien, T.K.; Larsen, A.; Loew-Friedrich, I.; Oed, C.; Rosenburg, R. Efficacy and safety of leflunomide compared with placebo and sulphasalazine in active rheumatoid arthritis: A double-blind, randomised, multicentre trial. European Leflunomide Study Group. Lancet 1999, 353, 259–266. [Google Scholar] [CrossRef]
- Strand, V.; Cohen, S.; Schiff, M.; Weaver, A.; Fleischmann, R.; Cannon, G.; Fox, R.; Moreland, L.; Olsen, N.; Furst, D.; et al. Treatment of active rheumatoid arthritis with leflunomide compared with placebo and methotrexate. Leflunomide Rheumatoid Arthritis Investigators Group. Arch. Intern. Med. 1999, 159, 2542–2550. [Google Scholar] [CrossRef]
- Dougados, M.; Combe, B.; Cantagrel, A.; Goupille, P.; Olive, P.; Schattenkirchner, M.; Meusser, S.; Paimela, L.; Rau, R.; Zeidler, H.; et al. Combination therapy in early rheumatoid arthritis: A randomised, controlled, double blind 52 week clinical trial of sulphasalazine and methotrexate compared with the single components. Ann. Rheum. Dis. 1999, 58, 220–225. [Google Scholar] [CrossRef]
- Lipsky, P.E.; van der Heijde, D.M.; St Clair, E.W.; Furst, D.E.; Breedveld, F.C.; Kalden, J.R.; Smolen, J.S.; Weisman, M.; Emery, P.; Feldmann, M.; et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group. N. Engl. J. Med. 2000, 343, 1594–1602. [Google Scholar] [CrossRef]
- Bathon, J.M.; Martin, R.W.; Fleischmann, R.M.; Tesser, J.R.; Schiff, M.H.; Keystone, E.C.; Genovese, M.C.; Wasko, M.C.; Moreland, L.W.; Weaver, A.L.; et al. A comparison of etanercept and methotrexate in patients with early rheumatoid arthritis. N. Engl. J. Med. 2000, 343, 1586–1593. [Google Scholar] [CrossRef]
- Choy, E.H.S.; Scott, D.L.; Kingsley, G.H.; Williams, P.; Wojtulewski, J.; Papasavvas, G.; Henderson, E.; Macfarlane, D.; Erhardt, C.; Young, A.; et al. Treating rheumatoid arthritis early with disease modifying drugs reduces joint damage: A randomised double blind trial of sulphasalazine vs diclofenac sodium. Clin. Exp. Rheumatol. 2002, 20, 351–358. [Google Scholar]
- Klareskog, L.; van der Heijde, D.; de Jager, J.P.; Gough, A.; Kalden, J.; Malaise, M.; Martín Mola, E.; Pavelka, K.; Sany, J.; Settas, L.; et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: Double-blind randomised controlled trial. Lancet 2004, 363, 675–681. [Google Scholar] [CrossRef]
- St Clair, E.W.; van der Heijde, D.M.F.M.; Smolen, J.S.; Maini, R.N.; Bathon, J.M.; Emery, P.; Keystone, E.; Schiff, M.; Kalden, J.R.; Wang, B.; et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: A randomized, controlled trial. Arthritis Rheum. 2004, 50, 3432–3443. [Google Scholar] [CrossRef] [PubMed]
- Keystone, E.C.; Kavanaugh, A.F.; Sharp, J.T.; Tannenbaum, H.; Hua, Y.; Teoh, L.S.; Fischkoff, S.A.; Chartash, E.K. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti-tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: A randomized, placebo-controlled, 52-week trial. Arthritis Rheum. 2004, 50, 1400–1411. [Google Scholar] [PubMed]
- Taylor, P.C.; Steuer, A.; Gruber, J.; Cosgrove, D.O.; Blomley, M.J.K.; Marsters, P.A.; Wagner, C.L.; McClinton, C.; Maini, R.N. Comparison of ultrasonographic assessment of synovitis and joint vascularity with radiographic evaluation in a randomized, placebo-controlled study of infliximab therapy in early rheumatoid arthritis. Arthritis Rheum. 2004, 50, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Goekoop-Ruiterman, Y.P.M.; de Vries-Bouwstra, J.K.; Allaart, C.F.; van Zeben, D.; Kerstens, P.J.S.M.; Hazes, J.M.W.; Zwinderman, A.H.; Ronday, H.K.; Han, K.H.; Westedt, M.L.; et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): A randomized, controlled trial. Arthritis Rheum. 2005, 52, 3381–3390. [Google Scholar] [CrossRef] [PubMed]
- Breedveld, F.C.; Weisman, M.H.; Kavanaugh, A.F.; Cohen, S.B.; Pavelka, K.; van Vollenhoven, R.; Sharp, J.; Perez, J.L.; Spencer-Green, G.T. The PREMIER study: A multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 2006, 54, 26–37. [Google Scholar]
- Emery, P.; Breedveld, F.C.; Hall, S.; Durez, P.; Chang, D.J.; Robertson, D.; Singh, A.; Pedersen, R.D.; Koenig, A.S.; Freundlich, B. Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): A randomised, double-blind, parallel treatment trial. Lancet 2008, 372, 375–382. [Google Scholar] [CrossRef]
- Keystone, E.; van der Heijde, D.; Mason, D.; Landewé, R.; Vollenhoven, R.V.; Combe, B.; Emery, P.; Strand, V.; Mease, P.; Desai, C.; et al. Certolizumab pegol plus methotrexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: Findings of a fifty-two-week, phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum. 2008, 58, 3319–3329. [Google Scholar] [CrossRef]
- Smolen, J.; Landewé, R.B.; Mease, P.; Brzezicki, J.; Mason, D.; Luijtens, K.; van Vollenhoven, R.F.; Kavanaugh, A.; Schiff, M.; Burmester, G.R.; et al. Efficacy and safety of certolizumab pegol plus methotrexate in active rheumatoid arthritis: The RAPID 2 study a randomised controlled trial. Ann. Rheum. Dis. 2009, 68, 797–804. [Google Scholar] [CrossRef]
- Takeuchi, T.; Miyasaka, N.; Inoue, K.; Abe, T.; Koike, T. RISING study Impact of trough serum level on radiographic and clinical response to infliximab plus methotrexate in patients with rheumatoid arthritis: Results from the RISING study. Mod. Rheumatol. 2009, 19, 478–487. [Google Scholar] [CrossRef]
- Emery, P.; Fleischmann, R.; van der Heijde, D.; Keystone, E.C.; Genovese, M.C.; Conaghan, P.G.; Hsia, E.C.; Xu, W.; Baratelle, A.; Beutler, A.; et al. The effects of golimumab on radiographic progression in rheumatoid arthritis: Results of randomized controlled studies of golimumab before methotrexate therapy and golimumab after methotrexate therapy. Arthritis Rheum. 2011, 63, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Harigai, M.; Takeuchi, T.; Yamanaka, H.; Ishiguro, N.; Yamamoto, K.; Miyasaka, N.; Koike, T.; Kanazawa, M.; Oba, T.; et al. Golimumab in combination with methotrexate in Japanese patients with active rheumatoid arthritis: Results of the GO-FORTH study. Ann. Rheum. Dis. 2012, 71, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Fleischmann, R.M.; Emery, P.; Kupper, H.; Redden, L.; Guerette, B.; Santra, S.; Smolen, J.S. Clinical, functional and radiographic consequences of achieving stable low disease activity and remission with adalimumab plus methotrexate or methotrexate alone in early rheumatoid arthritis: 26-week results from the randomised, controlled OPTIMA study. Ann. Rheum. Dis. 2013, 72, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Tada, M.; Koike, T.; Okano, T.; Sugioka, Y.; Wakitani, S.; Fukushima, K.; Sakawa, A.; Uehara, K.; Inui, K.; Nakamura, H. Comparison of joint destruction between standard- and low-dose etanercept in rheumatoid arthritis from the Prevention of Cartilage Destruction by Etanercept (PRECEPT) study. Rheumatology (Oxford) 2012, 51, 2164–2169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, T.; Son, Y.; Ozaki, Y.; Nomura, S.; Iida, H. Clinical and radiographic results from a 2-year comparison of once-weekly versus twice-weekly administration of etanercept in biologics-naive patients with rheumatoid arthritis. Mod. Rheumatol. 2012, 22, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Weinblatt, M.E.; Bingham, C.O.; Mendelsohn, A.M.; Kim, L.; Mack, M.; Lu, J.; Baker, D.; Westhovens, R. Intravenous golimumab is effective in patients with active rheumatoid arthritis despite methotrexate therapy with responses as early as week 2: Results of the phase 3, randomised, multicentre, double-blind, placebo-controlled GO-FURTHER trial. Ann. Rheum. Dis. 2013, 72, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Miyasaka, N.; Zang, C.; Alvarez, D.; Fletcher, T.; Wajdula, J.; Yuasa, H.; Vlahos, B. A phase 3 randomized, double-blind, multicenter comparative study evaluating the effect of etanercept versus methotrexate on radiographic outcomes, disease activity, and safety in Japanese subjects with active rheumatoid arthritis. Mod. Rheumatol. 2013, 23, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Harigai, M.; Tanaka, Y.; Yamanaka, H.; Ishiguro, N.; Yamamoto, K.; Miyasaka, N.; Koike, T.; Kanazawa, M.; Oba, T.; et al. Golimumab monotherapy in Japanese patients with active rheumatoid arthritis despite prior treatment with disease-modifying antirheumatic drugs: Results of the phase 2/3, multicentre, randomised, double-blind, placebo-controlled GO-MONO study through 24 weeks. Ann. Rheum. Dis. 2013, 72, 1488–1495. [Google Scholar]
- Nam, J.L.; Villeneuve, E.; Hensor, E.M.A.; Conaghan, P.G.; Keen, H.I.; Buch, M.H.; Gough, A.K.; Green, M.J.; Helliwell, P.S.; Keenan, A.M.; et al. Remission induction comparing infliximab and high-dose intravenous steroid, followed by treat-to-target: A double-blind, randomised, controlled trial in new-onset, treatment-naive, rheumatoid arthritis (the IDEA study). Ann. Rheum. Dis. 2014, 73, 75–85. [Google Scholar] [CrossRef]
- Yamanaka, H.; Ishiguro, N.; Takeuchi, T.; Miyasaka, N.; Mukai, M.; Matsubara, T.; Uchida, S.; Akama, H.; Kupper, H.; Arora, V.; et al. Recovery of clinical but not radiographic outcomes by the delayed addition of adalimumab to methotrexate-treated Japanese patients with early rheumatoid arthritis: 52-week results of the HOPEFUL-1 trial. Rheumatology (Oxford) 2014, 53, 904–913. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, K.; Takeuchi, T.; Yamanaka, H.; Ishiguro, N.; Tanaka, Y.; Eguchi, K.; Watanabe, A.; Origasa, H.; Iwai, K.; Sakamaki, Y.; et al. Efficacy and safety of certolizumab pegol without methotrexate co-administration in Japanese patients with active rheumatoid arthritis: The HIKARI randomized, placebo-controlled trial. Mod. Rheumatol. 2014, 24, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Yamamoto, K.; Takeuchi, T.; Yamanaka, H.; Ishiguro, N.; Eguchi, K.; Watanabe, A.; Origasa, H.; Shoji, T.; Miyasaka, N.; et al. Long-term efficacy and safety of certolizumab pegol in Japanese rheumatoid arthritis patients with an inadequate response to methotrexate: 52-week results from an open-label extension of the J-RAPID study. Mod. Rheumatol. 2014, 24, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Atsumi, T.; Yamamoto, K.; Takeuchi, T.; Yamanaka, H.; Ishiguro, N.; Tanaka, Y.; Eguchi, K.; Watanabe, A.; Origasa, H.; Yasuda, S.; et al. The first double-blind, randomised, parallel-group certolizumab pegol study in methotrexate-naive early rheumatoid arthritis patients with poor prognostic factors, C-OPERA, shows inhibition of radiographic progression. Ann. Rheum. Dis. 2016, 75, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Hørslev-Petersen, K.; Hetland, M.L.; Ørnbjerg, L.M.; Junker, P.; Pødenphant, J.; Ellingsen, T.; Ahlquist, P.; Lindegaard, H.; Linauskas, A.; Schlemmer, A.; et al. Clinical and radiographic outcome of a treat-to-target strategy using methotrexate and intra-articular glucocorticoids with or without adalimumab induction: A 2-year investigator-initiated, double-blinded, randomised, controlled trial (OPERA). Ann. Rheum. Dis. 2016, 75, 1645–1653. [Google Scholar] [CrossRef] [PubMed]
- Yoo, D.H.; Racewicz, A.; Brzezicki, J.; Yatsyshyn, R.; Arteaga, E.T.; Baranauskaite, A.; Abud-Mendoza, C.; Navarra, S.; Kadinov, V.; Sariego, I.G.; et al. A phase III randomized study to evaluate the efficacy and safety of CT-P13 compared with reference infliximab in patients with active rheumatoid arthritis: 54-week results from the PLANETRA study. Arthritis Res. Ther. 2016, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Emery, P.; Bingham, C.O.; Burmester, G.R.; Bykerk, V.P.; Furst, D.E.; Mariette, X.; van der Heijde, D.; van Vollenhoven, R.; Arendt, C.; Mountian, I.; et al. Certolizumab pegol in combination with dose-optimised methotrexate in DMARD-naïve patients with early, active rheumatoid arthritis with poor prognostic factors: 1-year results from C-EARLY, a randomised, double-blind, placebo-controlled phase III study. Ann. Rheum. Dis. 2017, 76, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Emery, P.; Vencovský, J.; Sylwestrzak, A.; Leszczynski, P.; Porawska, W.; Baranauskaite, A.; Tseluyko, V.; Zhdan, V.M.; Stasiuk, B.; Milasiene, R.; et al. 52-week results of the phase 3 randomized study comparing SB4 with reference etanercept in patients with active rheumatoid arthritis. Rheumatology (Oxford) 2017, 56, 2093–2101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolen, J.S.; Choe, J.-Y.; Prodanovic, N.; Niebrzydowski, J.; Staykov, I.; Dokoupilova, E.; Baranauskaite, A.; Yatsyshyn, R.; Mekic, M.; Porawska, W.; et al. Safety, immunogenicity and efficacy after switching from reference infliximab to biosimilar SB2 compared with continuing reference infliximab and SB2 in patients with rheumatoid arthritis: Results of a randomised, double-blind, phase III transition study. Ann. Rheum. Dis. 2018, 77, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Chichester, UK, 2008; ISBN 978-0-470-71218-4. [Google Scholar]
- Valente, T.W. Social Networks and Health: Models, Methods, and Applications; Oxford University Press: Oxford, UK, 2010; ISBN 978-0-19-530101-4. [Google Scholar]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P.A. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Shealy, D.J.; Cai, A.; Staquet, K.; Baker, A.; Lacy, E.R.; Johns, L.; Vafa, O.; Gunn, G.; Tam, S.; Sague, S.; et al. Characterization of golimumab, a human monoclonal antibody specific for human tumor necrosis factor α. MAbs 2010, 2, 428–439. [Google Scholar] [CrossRef]
- Khan, N.A.; Singh, M.; Spencer, H.J.; Torralba, K.D. Randomized controlled trials of rheumatoid arthritis registered at ClinicalTrials.gov: What gets published and when. Arthritis Rheum. 2014, 66, 2664–2674. [Google Scholar]
- Graudal, N.A.; Jurik, A.G.; de Carvalho, A.; Graudal, H.K. Radiographic progression in rheumatoid arthritis: A long-term prospective study of 109 patients. Arthritis Rheum. 1998, 41, 1470–1480. [Google Scholar] [CrossRef]
- Ropes, M.W.; Bennett, G.A.; Cobb, S.; Jacox, R.; Jessar, R.A. 1958 Revision of diagnostic criteria for rheumatoid arthritis. Bull. Rheum. Dis. 1958, 9, 175–176. [Google Scholar] [PubMed]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Van Valkenhoef, G.; Lu, G.; de Brock, B.; Hillege, H.; Ades, A.E.; Welton, N.J. Automating network meta-analysis. Res. Synth. Methods 2012, 3, 285–299. [Google Scholar] [CrossRef]
- Ranganath, V.K.; Yoon, J.; Khanna, D.; Park, G.S.; Furst, D.E.; Elashoff, D.A.; Jawaheer, D.; Sharp, J.T.; Gold, R.H.; Keystone, E.C.; et al. Comparison of composite measures of disease activity in an early seropositive rheumatoid arthritis cohort. Ann. Rheum. Dis. 2007, 66, 1633–1640. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, H.A.; Pincus, T. Reduced joint counts in controlled clinical trials in rheumatoid arthritis. Arthritis Rheum. 1994, 37, 470–475. [Google Scholar] [CrossRef]
- Wasserman, L. All of Statistics: A Concise Course in Statistical Inference; Springer: New York, NY, USA, 2010; ISBN 978-1-4419-2322-6. [Google Scholar]
- Sturtz, S.; Liggers, U.; Geiman, A. R2WinBUGS: A package for running WinBUGS from R. J. Stat. Softw. 2005, 12, 1–16. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Making 2013, 33, 607–617. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Welton, N.J.; Ades, A.E. Evidence synthesis for decision making 3: Heterogeneity-subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Making 2013, 33, 618–640. [Google Scholar] [CrossRef] [PubMed]
- Van Valkenhoef, G.; Kuiper, J. Gemtc: Network Meta-Analysis Using Bayesian Methods: R Package Version 0.8-2. 2016. Available online: https://CRAN.R-project.org/package=gemtc (accessed on 30 August 2019).
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Vehtari, A.; Rubin, D.B. Bayesian Data Analysis; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]



{kind=link}
{kind=link}
| Ref. | TD/C | GC. mg | DIR | RP | IOC | N | SD, weeks | DD, years | Age, years | F% | RF% | DAS28 | HAQ | RS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [14] | Su/Pl | 0.4 | No | IS | Yes | 73 | 52 | 0.5 | 51.3 | 64.0 | 66.7 | 5.6 | 1.4 | 2.0 |
| [15] | Su/Pl | 1.3 | No | S | No | 137 | 24 | 6.6 | 58.9 | 72.5 | 81.5 | 6.8 | 1.1 | 57.6 |
| [16] | Mt/Pl | 2.7 | No | S | No | 221 | 52 | 6.7 | 54.0 | 72.8 | 59.8 | 6.4 | 1.3 | 24.1 |
| [17] | Mt/Su | 0.0 | No | IS | No | 95 | 52 | 1.2 | 51.0 | 72.5 | 68.5 | 5.5 | 1.3 | 7.2 |
| [18] | In/Mt | 3.2 | Yes | IS | Yes | 135 | 54 | 10.5 | 52.5 | 80.5 | 80.5 | 6.7 | 1.8 | 80.5 |
| [19] | Et/Mt | 2.8 | No | IS | Yes | 390 | 52 | 1.0 | 49.5 | 75.0 | 88.5 | 6.9 | 1.4 | 12.1 |
| [20] | Su/Pl | 0.0 | No | IS | Yes | 83 | 52 | 0.5 | 57.1 | 75.0 | 56.0 | 5.2 | 1.2 | 3.9 |
| [21] | Et/Mt | 3.1 | Yes | IS | UC | 424 | 52 | 6.6 | 53.1 | 78.0 | 73.0 | 5.6 | 1.4 | 32.2 |
| [22] | In/Mt | 1.9 | No | S | No | 532 | 54 | 0.9 | 50.5 | 73.0 | 71.0 | 6.7 | 1.5 | 11.5 |
| [23] | Ad/Mt | 2.6 | Yes | IS | Yes | 368 | 52 | 11.0 | 56.7 | 74.3 | 85.4 | 6.1 | 1.5 | 66.5 |
| [24] | In/Mt | 2.5 | Yes | S | No | 24 | 54 | 1.5 | 53.3 | 75.5 | 100.0 | 5.3 | 1.4 | 18.0 |
| [25] | In/Mt | 0.0 | No | S | Yes | 234 | 52 | 0.6 | 54.0 | 67.0 | 65.5 | 5.5 | 1.4 | 7.2 |
| [26] | Ad/Mt | 2.2 | No | IS | Yes | 531 | 52 | 0.8 | 52.1 | 75.7 | 79.9 | 6.4 | 1.6 | 20.4 |
| [27] | Et/Mt | 2.5 | No | S | No | 476 | 52 | 0.8 | 51.4 | 73.5 | 68.5 | 6.5 | 1.7 | 6.0 |
| [28] | Cz/Mt | 1.7 | Yes | IS | No | 592 | 52 | 6.2 | 51.8 | 83.2 | 81.2 | 7.0 | 1.7 | 41.1 |
| [29] | Cz/Mt | 2.8 | Yes | IS | No | 373 | 24 | 5.9 | 51.9 | 84.0 | 77.9 | 6.8 | 1.6 | 43.1 |
| [30] | In/In | 3.4 | Yes | IS | No | 178 | 40 | 7.8 | 49.3 | 80.8 | 87.0 | 6.2 | 1.2 | 48.5 |
| [31] | Go/Mt | 3.3 | No | IS | No | 280 | 52 | 3.5 | 48.4 | 84.1 | 81.5 | 5.1 | 1.6 | 20.1 |
| [31] | Go/Mt | 4.8 | Yes | IS | No | 234 | 52 | 6.2 | 51.5 | 80.5 | 82.4 | 6.1 | 1.4 | 37.1 |
| [32] | Go/Mt | 2.5 | Yes | IS | Yes | 165 | 24 | 8.8 | 50.8 | 84.0 | 79.9 | 5.6 | 1.0 | 56.1 |
| [33] | Ad/Mt | 2.2 | No | IS | No | 1022 | 26 | 0.4 | 50.6 | 74.0 | 88.0 | 6.0 | 1.6 | 11.5 |
| [34] | Et/Et | 4.4 | Yes | IS | UC | 62 | 52 | 9.2 | 60.7 | 80.0 | 81.4 | 4.8 | 1.0 | 159.9 |
| [35] | Et/Et | 3.8 | No | IS | No | 63 | 104 | 10.9 | 60.6 | 85.7 | 75.0 | 4.4 | 1.4 | 54.0 |
| [36] | Go/Mt | 2.5 | Yes | IS | No | 592 | 24 | 7.0 | 51.7 | 81.1 | 100.0 | 6.0 | 1.6 | 49.0 |
| [37] | Et/Mt | 3.0 | Yes | S | No | 361 | 52 | 3.0 | 51.0 | 79.9 | 75.6 | 5.8 | 1.1 | 44.1 |
| [38] | Go/Mt | 2.5 | Yes | IS | Yes | 206 | 24 | 8.7 | 52.7 | 81.1 | NR | 5.9 | 1.1 | 50.0 |
| [39] | In/Mt | 1.6 | No | S | No | 112 | 26 | 0.1 | 53.3 | 68.7 | 54.9 | 4.3 | 1.4 | 7.6 |
| [40] | Ad/Mt | 1.6 | No | IS | No | 331 | 26 | 0.3 | 54.0 | 81.3 | 84.4 | 6.6 | 1.2 | 13.7 |
| [41] | Cz/Su.Pl | 3.6 | Yes | S | No | 114 | 24 | 5.8 | 55.4 | 77.2 | 89.5 | 6.3 | 1.2 | 46.1 |
| [42] | Cz/Mt | 3.1 | Yes | S | No | 146 | 24 | 5.9 | 53.1 | 83.2 | 88.0 | 6.4 | 1.2 | 53.8 |
| [43] | Cz/Mt | 0.9 | No | IS | UC | 315 | 24 | 0.3 | 49.2 | 81.0 | 96.2 | 5.5 | 1.1 | 5.6 |
| [44] | Ad/Mt | 0.9 | No | IS | Yes | 173 | 52 | 0.2 | 55.2 | 66.0 | 72.0 | 5.6 | 1.1 | 4.4 |
| [45] | In/In | 2.5 | Yes | IS | UC | 336 | 54 | NR | 50.0 | 82.7 | 73.5 | 5.9 | 1.6 | 66.6 |
| [46] | Cz/Mt | 1.6 | No | IS | No | 691 | 52 | 0.3 | 50.8 | 77.9 | 96.8 | 6.8 | 1.7 | 7.9 |
| [47] | Et/Et | 2.5 | Yes | IS | Yes | 478 | 52 | 6.1 | 51.9 | 84.3 | 78.6 | 6.5 | 1.5 | 41.1 |
| [48] | In/In | 2.5 | Yes | S | No | 422 | 54 | 6.5 | 52.1 | 80.1 | 72.5 | 6.5 | 1.5 | 38.0 |
| Treatment # | Unadjusted | DAS28 * | HAQ * | Baseline RS * | Glucocorti-Coid Dose * | Incomplete Outcome | Randomi-Zation Procedure |
|---|---|---|---|---|---|---|---|
| Coefficient | — | −0.0 (−0.2, 0.1) | 0.0 (−0.1, 0.2) | −0.3 (−0.4, 0.1) | −0.1 (−0.2, 0.1) | −0.1 (−0.3, 0.2) | 0.2 (−0.1, 0.6) |
| Ad40 | −0.1 (−0.8, 0.5) | −0.1 (−0.8, 0.5) | −0.1 (−0.8, 0.5) | −0.2 (−0.8, 0.3) | −0.2 (−0.8, 0.4) | −0.1 (−0.8, 0.5) | −0.4 (−1.1, 0.4) |
| Ad20x2Mt | −0.4 (−0.8, 0.0) | −0.4 (−0.8, 0.0) | −0.4 (−0.8, 0.0) | −0.3 (−0.6, 0.0) | −0.4 (−0.8, 0.0) | −0.3 (−0.8, 0.1) | −0.6 (−1.2, −0.1) |
| Ad40Mt | −0.5 (−0.7, −0.3) | −0.5 (−0.7, −0.3) | −0.5 (−0.7, 0.3) | −0.6 (−0.8, 0.4) | −0.5 (−0.8, 0.3) | −0.5 (−0.7, 0.2) | −0.7 (−1.2, −0.3) |
| Cz100Mt | −0.2 (−0.9, 0.3) | −0.2 (−0.8, 0.4) | −0.3 (−0.9, 0.3) | −0.3 (−0.8, 0.2) | −0.3 (−0.9, 0.3) | −0.2 (−0.9, 0.4) | −0.4 (−1.2, 0.2) |
| Cz200 | −1.1 (−2.1, −0.2) | −1.1 (−2.1, −0.1) | −1.1 (−2.1, 0.1) | −1.3 (−2.1, 0.4) | −1.1 (−2.1, 0.1) | −1.1 (−2.1, 0.1) | −1.1 (−2.1, −0.2) |
| Cz200Mt | −0.5 (−0.7, −0.3) | −0.4 (−0.7, −0.2) | −0.5 (−0.8, 0.3) | −0.6 (−0.8, 0.4) | −0.5 (−0.8, 0.3) | −0.5 (−0.7, 0.2) | −0.7 (−1.1, −0.3) |
| Cz400Mt | −0.5 (−0.9, −0.3) | −0.5 (−0.8, −0.2) | −0.6 (−0.9, 0.3) | −0.6 (−0.9, 0.4) | −0.6 (−0.9, 0.3) | −0.5 (−0.9, 0.3) | −0.8 (−1.2, −0.3) |
| Et20 | −0.2 (−0.6, 0.1) | −0.2 (−0.6, 0.1) | −0.2 (−0.6, 0.1) | −0.3 (−0.6, 0.0) | −0.2 (−0.6, 0.1) | −0.2 (−0.6, 0.2) | −0.4 (−0.8, 0.0) |
| Et25Mt | −0.5 (−1.1, 0.0) | −0.5 (−1.1, 0.0) | −0.6 (−1.2, 0.0) | −0.7 (−1.2, 0.3) | −0.5 (−1.1, 0.0) | −0.5 (−1.2, 0.1) | −0.6 (−1.3, −0.0) |
| Et50 | −0.5 (−0.8, −0.2) | −0.5 (−0.8, −0.2) | −0.5 (−0.8, 0.2) | −0.6 (−0.9, 0.3) | −0.4 (−0.8, 0.2) | −0.4 (−0.8, 0.1) | −0.6 (−1.0, −0.2) |
| SB4Et50Mt | −0.7 (−1.2, −0.2) | −0.7 (−1.2, −0.2) | −0.7 (−1.3, −0.2) | −0.9 (−1.2, −0.5) | −0.7 (−1.2, 0.2) | −0.7 (−1.2, −0.1) | −0.8 (−1.3, −0.3) |
| Et50Mt | −0.6 (−0.9, −0.3) | −0.6 (−0.9, −0.3) | −0.7 (−1.0, −0.3) | −0.8 (−1.1, −0.5) | −0.6 (−0.9, 0.3) | −0.6 (−0.9, −0.3) | −0.7 (−1.1, −0.4) |
| Go100 | −0.1 (−0.4, 0.2) | −0.1 (−0.5, 0.2) | −0.1 (−0.5, 0.2) | −0.2 (−0.4, 0.1) | −0.0 (−0.4, 0.3) | −0.1 (−0.4, 0.2) | −0.4 (−0.9, 0.1) |
| Go50Mt | −0.2 (−0.5, 0.1) | −0.2 (−0.5, 0.1) | −0.2 (−0.5, 0.1) | −0.2 (−0.4, 0.0) | −0.1 (−0.5, 0.2) | −0.2 (−0.5, 0.1) | −0.4 (−0.9, 0.0) |
| Go100Mt | −0.4 (−0.6, −0.1) | −0.4 (−0.7, −0.1) | −0.4 (−0.6, −0.1) | −0.4 (−0.6, −0.2) | −0.3 (−0.6, 0.0) | −0.3 (−0.6, −0.1) | −0.6 (−1.1, −0.1) |
| Go130Mt | −0.5 (−0.9, −0.1) | −0.5 (−1.0, −0.1) | −0.6 (−1.1, −0.1) | −0.4 (−0.8, −0.1) | −0.5 (−1.0, 0.1) | −0.5 (−1.0, −0.1) | −0.7 (−1.3, −0.2) |
| SB2In3Mt | −0.9 (−1.4, −0.4) | −0.9 (−1.4, −0.4) | −0.9 (−1.5, −0.4) | −1.0 (−1.4, −0.7) | −0.9 (−1.4, 0.4) | −0.9 (−1.4, −0.4) | −0.9 (−1.4, −0.4) |
| CTPIn3Mt | −0.8 (−1.3, −0.3) | −0.8 (−1.4, −0.3) | −0.8 (−1.4, −0.3) | −0.9 (−1.4, −0.5) | −0.8 (−1.4, 0.3) | −0.8 (−1.4, −0.2) | −0.8 (−1.4, −0.3) |
| In3Mt | −0.9 (−1.2, −0.6) | −0.9 (−1.2, −0.6) | −0.9 (−1.2, −0.6) | −1.0 (−1.3, −0.8) | −0.9 (−1.2, 0.6) | −0.9 (−1.2, −0.6) | −0.9 (−1.2, −0.6) |
| In6Mt | −0.8 (−1.2, −0.5) | −0.8 (−1.2, −0.5) | −0.9 (−1.2, −0.5) | −0.9 (−1.2, −0.7) | −0.9 (−1.2, 0.5) | −0.8 (−1.2, −0.5) | −0.9 (−1.2, −0.5) |
| In10Mt | −1.0 (−1.4, −0.7) | −1.0 (−1.4, −0.7) | −1.1 (−1.5, −0.7) | −1.1 (−1.4, −0.8) | −1.1 (−1.5, 0.7) | −1.0 (−1.4, −0.6) | −1.1 (−1.5, −0.7) |
| In20Mt | −1.3 (−1.8, −0.9) | −1.3 (−1.8, −0.9) | −1.4 (−1.9, −0.9) | −1.4 (−1.8, −1.0) | −1.3 (−1.8, 0.9) | −1.3 (−1.8, −0.8) | −1.4 (−1.9, −0.9) |
| Sulfasalazin | −0.7 (−1.2, −0.1) | −0.7 (−1.2, −0.1) | −0.7 (−1.2, −0.0) | −0.8 (−1.3, −0.3) | −0.7 (−1.3, 0.1) | −0.7 (−1.2, −0.1) | −0.7 (−1.3, −0.1) |
| Placebo | 0.4 (−0.0, 0.8) | 0.4 (−0.0, 0.8) | 0.4 (−0.0, 0.8) | 0.2 (−0.1, 0.6) | 0.4 (−0.0, 0.8) | 0.4 (−0.1, 0.8) | 0.4 (−0.1, 0.8) |
| σ ** | 0.2 (0.1, 0.3) | 0.2 (0.1, 0.3) | 0.2 (0.1, 0.3) | 0.1 (0.0, 0.2) | 0.2 (0.1, 0.3) | 0.2 (0.1, 0.3) | 0.2 (0.1, 0.3) |
| Dbar † | −117.4 | −117.4 | −119.7 | −119.5 | −117.4 | −118.2 | −119.1 |
| DIC | −43.0 | −42.1 | −44.0 | −50.4 | −42.3 | −42.6 | −43.4 |
| pD | 74.3 | 75.3 | 75.7 | 69.0 | 75.0 | 75.5 | 75.8 |
| Treatment # | Four-Covariate Metaregression | RS Covariate Metaregression | Unadjusted Model |
|---|---|---|---|
| Random Eff. | Random Eff. | Random Eff. | |
| DAS28* | 0.0 (−0.1, 0.1) | - | - |
| Incomplete outcome | 0.1 (−0.1, 0.3) | - | - |
| Glucocorticoid dose* | 0.1 (−0.1, 0.3) | - | - |
| Relative base RS* | −0.3 (−0.5, −0.2) | −0.3 (−0.4, 0.1) | - |
| Ad40 | −0.2 (−0.8, 0.3) | −0.2 (−0.8, 0.3) | −0.1 (−0.8, 0.5) |
| Ad20x2Mt | −0.3 (−0.7, 0.0) | −0.3 (−0.6, 0.0) | −0.4 (−0.8, 0.0) |
| Ad40Mt | −0.6 (−0.9, −0.4) | −0.6 (−0.8, 0.4) | −0.5 (−0.7, −0.3) |
| Cz100Mt | −0.3 (−0.9, 0.2) | −0.3 (−0.8, 0.2) | −0.2 (−0.9, 0.3) |
| Cz200 | −1.3 (−2.2, −0.4) | −1.3 (−2.1, 0.4) | −1.1 (−2.1, −0.1) |
| Cz200Mt | −0.6 (−0.8, −0.4) | −0.6 (−0.8, 0.4) | −0.5 (−0.7, −0.3) |
| Cz400Mt | −0.6 (−0.9, −0.4) | −0.6 (−0.9, 0.4) | −0.5 (−0.8, −0.3) |
| Et20 | −0.5 (−0.9, −0.1) | −0.3 (−0.6, 0.0) | −0.2 (−0.6, 0.1) |
| Et25Mt | −0.9 (−1.4, −0.3) | −0.7 (−1.2, 0.3) | −0.5 (−1.1, 0.0) |
| Et50 | −0.8 (−1.1, −0.4) | −0.6 (−0.9, 0.3) | −0.5 (−0.8, −0.2) |
| SB4Et50Mt | −1.0 (−1.4, −0.6) | −0.9 (−1.2, −0.5) | −0.7 (−1.2, −0.2) |
| Et50Mt | −0.9 (−1.3, −0.6) | −0.8 (−1.1, −0.5) | −0.6 (−0.9, −0.3) |
| Go100 | −0.4 (−0.8, 0.0) | −0.2 (−0.4, 0.1) | −0.1 (−0.4, 0.2) |
| Go50Mt | −0.4 (−0.8, −0.0) | −0.2 (−0.4, 0.0) | −0.2 (−0.5, 0.1) |
| Go100Mt | −0.6 (−0.9, −0.2) | −0.4 (−0.6, −0.2) | −0.4 (−0.6, −0.1) |
| Go130Mt | −0.4 (−0.7, −0.1) | −0.4 (−0.8, −0.1) | −0.5 (−1.0, −0.1) |
| SB2In3Mt | −1.0 (−1.4, −0.6) | −1.0 (−1.4, −0.7) | −0.9 (−1.4, −0.4) |
| CTPIn3Mt | −0.9 (−1.4, −0.5) | −0.9 (−1.4, −0.5) | −0.8 (−1.3, −0.3) |
| In3Mt | −1.0 (−1.3, −0.7) | −1.0 (−1.3, −0.8) | −0.9 (−1.2, −0.6) |
| In6Mt | −0.9 (−1.3, −0.7) | −0.9 (−1.2, −0.7) | −0.8 (−1.2, −0.5) |
| In10Mt | −1.1 (−1.5, −0.8) | −1.1 (−1.4, −0.8) | −1.0 (−1.4, −0.7) |
| In20Mt | −1.4 (−1.8, −1.0) | −1.4 (−1.8, −1.0) | −1.3 (−1.8, −0.9) |
| Sulfasalazin | −0.8 (−1.4, −0.3) | −0.8 (−1.3, −0.3) | −0.7 (−1.2, −0.1) |
| Placebo | 0.2 (−0.2, 0.5) | 0.2 (−0.1, 0.6) | 0.4 (−0.0, 0.8) |
| σ ** | 0.1 (0.0, 0.2) | 0.1 (0.0, 0.2) | 0.2 (0.1, 0.3) |
| Dbar † | −119.4 | −119.5 | −117.4 |
| DIC | −47.6 | −50.4 | −43.0 |
| pD | 71.8 | 69.0 | 74.3 |
| Comparison | Consistency Effect | Direct Effect | Indirect Effect | p-Value |
|---|---|---|---|---|
| Et50Mt vs. Et50 | −0.2 (−0.5, 0.2) | −0.2 (−0.7, 0.2) | 0.1 (−0.5, 0.7) | 0.42 |
| Mt vs. Et20 | 0.2 (−0.1, 0.6) | 0.3 (−0.1, 0.7) | 0.1 (−0.5, 0.8) | 0.71 |
| Mt vs. In10Mt | 1.0 (0.7, 1.4) | 1.5 (0.8, 2.2) | 0.8 (0.4, 1.3) | 0.12 |
| Mt vs. In3Mt | 0.9 (0.6, 1.2) | 0.8 (0.5, 1.1) | 2.1 (0.7, 3.5) | 0.08 |
| Mt vs. In6Mt | 0.8 (0.5, 1.2) | 0.9 (0.5, 1.3) | 0.6 (−0.0, 1.3) | 0.40 |
| In6Mt vs. In3Mt | 0.1 (−0.2, 0.3) | 0.1 (−0.2, 0.3) | −1.2 (−2.6, 0.2) | 0.08 |
| Pl vs. Mt | 0.4 (−0.0, 0.8) | 0.3 (−0.1, 0.7) | 1.1 (−0.3, 2.6) | 0.28 |
| Su vs. Mt | −0.7 (−1.2, −0.1) | 0.0 (−1.3, 1.4) | −0.8 (−1.4, −0.2) | 0.28 |
| Su vs. Pl | −1.0 (−1.5, −0.6) | −1.1 (−1.6, −0.7) | −0.3 (−1.7, 1.2) | 0.28 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graudal, N.; Kaas-Hansen, B.S.; Guski, L.; Hubeck-Graudal, T.; Welton, N.J.; Jürgens, G. Different Original and Biosimilar TNF Inhibitors Similarly Reduce Joint Destruction in Rheumatoid Arthritis—A Network Meta-Analysis of 36 Randomized Controlled Trials. Int. J. Mol. Sci. 2019, 20, 4350. https://doi.org/10.3390/ijms20184350
Graudal N, Kaas-Hansen BS, Guski L, Hubeck-Graudal T, Welton NJ, Jürgens G. Different Original and Biosimilar TNF Inhibitors Similarly Reduce Joint Destruction in Rheumatoid Arthritis—A Network Meta-Analysis of 36 Randomized Controlled Trials. International Journal of Molecular Sciences. 2019; 20(18):4350. https://doi.org/10.3390/ijms20184350
Chicago/Turabian StyleGraudal, Niels, Benjamin Skov Kaas-Hansen, Louise Guski, Thorbjørn Hubeck-Graudal, Nicky J. Welton, and Gesche Jürgens. 2019. "Different Original and Biosimilar TNF Inhibitors Similarly Reduce Joint Destruction in Rheumatoid Arthritis—A Network Meta-Analysis of 36 Randomized Controlled Trials" International Journal of Molecular Sciences 20, no. 18: 4350. https://doi.org/10.3390/ijms20184350