
P16 and HPV Genotype Significance in HPV-Associated Cervical Cancer—A Large Cohort of Two Tertiary Referral Centers

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Clinicopathologic Characteristics
2.2. HPV Genotypes, Genera and p16 Expression
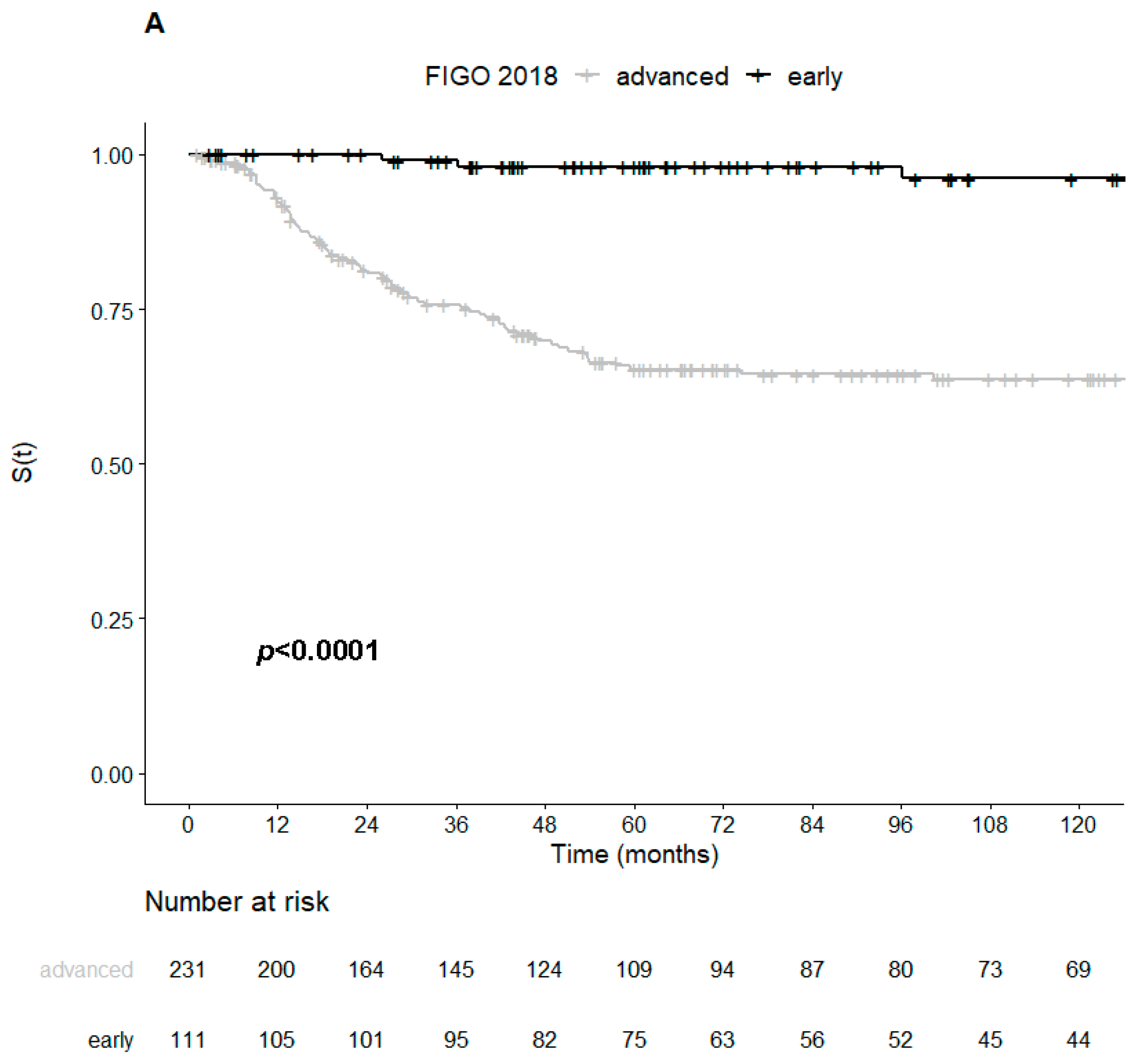
2.3. Survival and Prognostic Variables
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Clinical Management and Treatment
4.3. Histopathological Evaluation
4.4. HPV DNA Detection and Genotyping
4.5. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Darragh, T.M.; Colgan, T.J.; Cox, J.T.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The lower anogenital squamous terminology standardization project for HPV-associated lesions: Background and consensus recommendations from the college of American pathologists and the American society for colposcopy and cervical pathology. Int. J. Gynecol. Pathol. 2013, 32, 76–115. [Google Scholar] [CrossRef] [Green Version]
- Ordi, J.; Puig-Tintoré, L.M.; Torne, A.; Sanz, S.; Esteve, R.; Romagosa, C.; Cardesa, A. Contribución de la detección del virus del papiloma humano de alto riesgo al estudio de las lesiones premalignas y malignas del cérvix uterino. Med. Clin. 2003, 121, 441–445. [Google Scholar] [CrossRef]
- Zur Hausen, H.; Schneider, A. The role of papillomavirus in human anogenital cancer. In The Papovaviridiae: The Papillomaviruses; Salzmann, N., Howley, P., Eds.; Springer: Boston, MA, USA, 1987; Volume 2, pp. 1014–1019. [Google Scholar]
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Szymonowicz, K.A.; Chen, J. Biological and clinical aspects of HPV-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- International Human Papillomavirus Reference Clones, Stockholm: Karolinska Institutet. Available online: https://www.hpvcenter.se/human_reference_clones/ (accessed on 27 December 2020).
- Arbyn, M.; Tommasino, M.; Depuydt, C.; Dillner, J. Are 20 human papillomavirus types causing cervical cancer? J. Pathol. 2014, 234, 431–435. [Google Scholar] [CrossRef]
- Kaliff, M.; Sorbe, B.; Mordhorst, L.B.; Helenius, G.; Karlsson, M.G.; Lillsunde-Larsson, G. Findings of multiple HPV genotypes in cervical carcinoma are associated with poor cancer-specific survival in a Swedish cohort of cervical cancer primarily treated with radiotherapy. Oncotarget 2018, 9, 18786–18796. [Google Scholar] [CrossRef] [PubMed]
- Hang, D.; Jia, M.; Ma, H.; Zhou, J.; Feng, X.; Lyu, Z.; Yin, J.; Cui, H.; Yin, Y.; Jin, G.; et al. Independent prognostic role of human papillomavirus genotype in cervical cancer. BMC Infect. Dis. 2017, 17, 391. [Google Scholar] [CrossRef] [Green Version]
- Clifford, G.M.; Smith, J.S.; Plummer, M.; Muñoz, N.; Franceschi, S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br. J. Cancer. 2003, 88, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Castle, P.E.; Lorincz, A.T.; Wacholder, S.; Sherman, M.; Scott, D.R.; Rush, B.B.; Glass, A.G.; Schiffman, M. The elevated 10-Year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J. Natl. Cancer Inst. 2005, 97, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Nicolás, I.; Marimon, L.; Barnadas, E.; Saco, A.; Rodríguez-Carunchio, L.; Fusté, P.; Martí, C.; Rodriguez-Trujillo, A.; Torne, A.; Del Pino, M.; et al. HPV-negative tumors of the uterine cervix. Mod. Pathol. 2019, 32, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- de Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 32, 1189–1196. [Google Scholar] [CrossRef]
- Li, N.; Franceschi, S.; Howell-Jones, R.; Snijders, P.J.F.; Clifford, G.M. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: Variation by geographical region, histological type and year of publication. Int. J. Cancer 2011, 128, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.O.; Lee, Y.H.; Han, H.S.; Lee, H.J.; Park, J.Y.; Hong, D.G.; Lee, Y.S.; Cho, Y.L. Prognostic value of pre-treatment human papilloma virus DNA status in cervical cancer. Gynecol. Oncol. 2018, 148, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Okuma, K.; Yamashita, H.; Yokoyama, T.; Nakagawa, K.; Kawana, K. Undetected human papillomavirus DNA and uterine cervical carcinoma: Association with cancer recurrence. Strahlenther. Onkol. 2016, 192, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Riou, G.; Bourhis, J.; Favre, M.; Orth, G.; Jeannel, D.; Le Doussal, V. Association between poor prognosis in early-stage invasive cervical carcinomas and non-detection of HPV DNA. Lancet 1990, 335, 1171–1174. [Google Scholar] [CrossRef]
- Higgins, G.D.; Uzelin, D.M.; Phillips, G.E.; Davy, M.; Roder, D.; Burrell, C.J. Increased age and mortality associated with cervical carcinomas negative for human papillomavirus RNA. Lancet 1991, 338, 910–913. [Google Scholar] [CrossRef]
- Rodríguez-Carunchio, L.; Soveral, I.; Steenbergen, R.D.M.; Torné, A.; Martinez, S.; Fusté, P.; Pahisa, J.; Marimon, L.; Ordi, J.; Del Pino, M. HPV-negative carcinoma of the uterine cervix: A distinct type of cervical cancer with poor prognosis. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 119–127. [Google Scholar] [CrossRef]
- Saco, A.; Carrilho, C.; Focchi, G.R.A.; Kong, C.S.; Mills, A.M.; Park, K.J.; Regauer, S. WHO Classification of Tumours of Female Genital Tract, 5th ed.; WHO: Geneva, Switzerland, 2020; Volume 4, pp. 347–350. [Google Scholar]
- Carozzi, F.; Confortini, M.; Palma, P.D.; Del Mistro, A.; Gillio-Tos, A.; De Marco, L.; Giorgi-Rossi, P.; Pontenani, G.; Rosso, S.; Sani, C.; et al. Use of p16-INK4A overexpression to increase the specificity of human papillomavirus testing: A nested substudy of the NTCC randomised controlled trial. Lancet Oncol. 2008, 9, 937–945. [Google Scholar] [CrossRef]
- Lin, J.; Albers, A.E.; Qin, J.; Kaufmann, A.M. Prognostic Significance of Overexpressed p16INK4ain Patients with Cervical Cancer: A Meta-Analysis. PLoS ONE 2014, 9, e106384. [Google Scholar] [CrossRef]
- Cao, H.; Wang, S.; Zhang, Z.; Lou, J. Prognostic value of overexpressed p16INK4a in vulvar cancer: A meta-analysis. PLoS ONE 2016, 11, e0152459. [Google Scholar] [CrossRef]
- Nwachukwu, C.R.; Harris, J.P.; Chin, A.; Von Eyben, R.; Giaretta, S.; Shaffer, J.L.; Hiniker, S.M.; Kapp, D.S.; Folkins, A.K.; Kidd, E.A. Prognostic Significance of P16 Expression and P53 Expression in Primary Vaginal Cancer. Int. J. Gynecol. Pathol. 2019, 38, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, H.; Xiu, Y.; Cheng, H.; Gu, M.; Song, N. Prognostic significance of P16INK4a expression in penile squamous cell carcinoma: A meta-analysis with trial sequential analysis. BioMed Res. Int. 2018, 2018, 8345893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langendijk, J.A.; Psyrri, A. The prognostic significance of p16 overexpression in oropharyngeal squamous cell carcinoma: Implications for treatment strategies and future clinical studies. Ann. Oncol. 2010, 21, 1931–1934. [Google Scholar] [CrossRef]
- Nicolás, I.; Saco, A.; Barnadas, E.; Marimon, L.; Rakislova, N.; Fusté, P.; Rovirosa, A.; Gaba, L.; Buñesch, L.; Gil-Ibañez, B.; et al. Prognostic implications of genotyping and p16 immunostaining in HPV-positive tumors of the uterine cervix. Mod. Pathol. 2020, 33, 128–137. [Google Scholar] [CrossRef]
- Pilch, H.; Gunzel, S.; Schaffer, U.; Tanner, B.; Brockerhoff, P.; Maeurer, M.; Hockel, M.; Hommel, G.; Knapstein, P.G. The presence of HPV DNA in cervical cancer: Correlation with clinico-pathologic parameters and prognostic significance: 10 years experience at-the Department of Obstetrics and Gynecology of the Mainz University. Int. J. Gynecol. Cancer 2001, 11, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.D.; Kim, C.H.; Cho, M.K.; Kim, J.W.; Cho, H.Y.; Kim, Y.H.; Choi, H.S.; Kim, S.M. HPV-18 is a poor prognostic factor, unlike the HPV viral load, in patients with stage IB-IIA cervical cancer undergoing radical hysterectomy. Gynecol. Oncol. 2011, 121, 546–550. [Google Scholar] [CrossRef]
- Wang, C.-C.; Lai, C.-H.; Huang, H.-J.; Chao, A.; Chang, C.-J.; Chang, T.-C.; Chou, H.-H.; Hong, J.-H. Clinical effect of human papillomavirus genotypes in patients with cervical cancer undergoing primary radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1111–1120. [Google Scholar] [CrossRef]
- Okonogi, N.; Kobayashi, D.; Suga, T.; Imai, T.; Wakatsuki, M.; Ohno, T.; Kato, S.; Nakano, T.; Kamada, T. Human papillomavirus genotype affects metastatic rate following radiotherapy in patients with uterine cervical cancer. Oncol. Lett. 2018, 15, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felix, A.; Esteves, S.; Martins, L.; Esteves, G.; Alemany, L.; Bosch, X. Does HPV16 status influence outcome in HPV positive cervical carcinomas? Virchows Arch. 2018, 473, S1–S340. [Google Scholar]
- Okonogi, N.; Kobayashi, D.; Suga, T.; Imai, T.; Wakatsuki, M.; Ohno, T.; Kato, S.; Nakano, T.; Kamada, T. HPV types in cervical cancer tissue in South Africa: A head-to-head comparison by mRNA and DNA tests. Medicine 2017, 96, e8752. [Google Scholar]
- Chen, W.; Sun, H.; Molijn, A.; Zeng, L.; Kang, L.; Jenkins, D.; Zhang, S.; Cui, J.; Wu, Z.; Pirog, E.; et al. The variable characteristics of human papillomavirus in squamous cell carcinoma and adenocarcinoma of Cervix in China. J. Low. Genit. Tract. Dis. 2018, 22, 355–361. [Google Scholar] [CrossRef]
- Van Muyden, R.C.P.A.; Ter Harmsel, B.W.A.; Smedts, F.M.M.; Hermans, J.; Kuijpers, J.C.; Raikhlin, N.T.; Petrov, S.; Lebedev, A.; Ramaekers, F.C.; Trimbos, J.B.; et al. Detection and typing of human papillomavirus in cervical carcinomas in Russian women: A prognostic study. Cancer 1999. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Tenjimbayashi, Y.; Tasaka, N.; Akiyama, A.; Sakurai, M.; Minaguchi, T.; Oki, A.; Satoh, T.; Yoshikawa, H. Human papillomavirus genotype and prognosis of cervical cancer: Favorable survival of patients with HPV16-positive tumors. Papillomavirus Res. 2018, 6, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Poetsch, M.; Hemmerich, M.; Kakies, C.; Kleist, B.; Wolf, E.; Dorp, F.V.; Hakenberg, O.W.; Protzel, C. Alterations in the tumor suppressor gene p16 INK4A are associated with aggressive behavior of penile carcinomas. Virchows Arch. 2011, 458, 221–229. [Google Scholar] [CrossRef]
- Poetsch, M.; Schuart, B.J.; Schwesinger, G.; Kleist, B.; Protzel, C. Screening of microsatellite markers in penile cancer reveals differences between metastatic and nonmetastatic carcinomas. Mod Pathol. 2007, 20, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Corn, P.G.; Baylin, S.B.; Herman, J.G. A gene hypermethylation profile of human cancer. Cancer Res. 2001, 60, 3225–3229. [Google Scholar]
- Banister, C.E.; Liu, C.; Pirisi, L.; Creek, K.E.; Buckhaults, P.J. Identification and characterization of HPV-independent cervical cancers. Oncotarget 2017, 8, 13375–13386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rakislova, N.; Clavero, O.; Alemany, L.; Saco, A.; Quirós, B.; Lloveras, B.; Alejo, M.; Pawlita, M.; Quint, W.; Del Pino, M.; et al. Histological characteristics of HPV-associated and -independent squamous cell carcinomas of the vulva: A study of 1,594 cases. Int. J. Cancer. 2017, 141, 2517–2527. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; AlQatari, M.; Sultan, K.; Ye, F.; Gao, D.; Sigel, K.; Zhang, D.; Kalir, T. Using p16 immunohistochemistry to classify morphologic cervical intraepithelial neoplasia: Correlation of ambiguous staining patterns with HPV subtypes and clinical outcome. Hum. Pathol. 2017, 66, 144–151. [Google Scholar] [CrossRef]
- Karamitopoulou, E.; Zlobec, I.; Koumarianou, A.; Patsouris, E.S.; Peros, G.; Lugli, A. Expression of p16 in lymph node metastases of adjuvantly treated stage III colorectal cancer patients identifies poor prognostic subgroups a retrospective: Analysis of biomarkers in matched primary tumor and lymph node metastases. Cancer 2010, 116, 4474–4486. [Google Scholar] [CrossRef] [PubMed]
- Saadallah-Kallel, A.; Abdelmaksoud-Dammak, R.; Triki, M.; Charfi, S.; Khabir, A.; Sallemi-Boudawara, T.; Mokdad-Gargouri, R. Clinical and prognosis value of the CIMP status combined with MLH1 or p16 INK4a methylation in colorectal cancer. Med. Oncol. 2017, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kanthiya, K.; Khunnarong, J.; Tangjitgamol, S.; Puripat, N.; Tanvanich, S. Expression of the p16 and Ki67 in cervical squamous intraepithelial lesions and cancer. Asian Pacific J. Cancer Prev. 2016, 17, 3201–3206. [Google Scholar]
- Huang, K.; Li, L.A.; Meng, Y.G.; Fu, X.Y. P16 expression in patients with cervical cancer and its prognostic significance: Meta-analysis of published literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 183, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Holm, R.; Kraus, I.; Skomedal, H.; Langerod, A.; Kristensen, G.B.; Lyng, H. Human Papillomavirus DNA and E6/E7 mRNA Status in Relation to Survival of Patients Treated for Cervical Squamous Cell Carcinoma. Open Virol. J. 2008, 2, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleter, B.; Van Doorn, L.-J.; Schrauwen, L.; Molijn, A.; Sastrowijoto, S.; Ter Schegget, J.; Lindeman, J.; Ter Harmsel, B.; Burger, M.; Quint, W. Development and clinical evaluation of a highly sensitive PCR-reverse hybridization line probe assay for detection and identification of anogenital human papillomavirus. J. Clin. Microbiol. 1999, 37, 2508–2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 11 January 2021).
- Therneau, T.M. A Package for Survival Analysis in S, version 2.38; 2015. Available online: https://CRAN.R-project.org/package=survival (accessed on 11 January 2021).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, USA, 2000; ISBN 0-387-98784-3. [Google Scholar]
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. Drawing Survival Curves using “ggplot2.”, CRAN. R package version 0.4.6; 2019. Available online: https://CRAN.R-project.org/package=survminer (accessed on 11 January 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Type of HPV infection (n = 348) | |
| Single | 288 (82.8%) |
| Multiple | 43 (12.4%) |
| Unknown (HPVX) | 17 (4.9%) |
| HPV type | |
| Single infection (n = 288) | |
| HPV16 | 203 (70.5%) |
| HPV18 | 28 (9.7%) |
| HPV33 | 12 (4.2%) |
| HPV45 | 8 (2.8%) |
| HPV35 | 7 (2.4%) |
| Others * | 30 (10.4%) |
| Multiple infection (n = 43) | |
| HPV16, HPV18 | 13 (30.2%) |
| HPV16, HPV33 | 9 (20.9%) |
| Other double infections ** | 14 (32.6%) |
| Triple infections *** | 6 (14.0%) |
| Quadruple infection **** | 1 (2.3%) |
| HPV genera (n = 348) | |
| α-9 | 254 (73.0%) |
| α-7 | 48 (13.8%) |
| α-7 and α-9 | 21 (6.0%) |
| Non-α-7/α-9 | 8 (2.3%) |
| Unknown (HPVX) | 17 (4.9%) |
| Variables | Overall Sample (n = 348) | p16 Positive (n = 330) | p16 Negative (n = 18) | p-Value |
|---|---|---|---|---|
| Age, years old | ||||
| median (min–max) | 47.5 (22–89) | 47 (22–87) | 58.5 (35–89) | 0.04 |
| Histology, n (%) | ||||
| SCC | 280 (80%) | 266 (81%) | 14 (78%) | 0.82 |
| ADC | 64 (19%) | 60 (18%) | 4 (22%) | |
| Other | 4 (1%) | 4 (1%) | 0 | |
| FIGO stage 2018, n (%) | ||||
| Early (IA1 to IB1) | 111 (32%) | 109 (33%) | 2 (11%) | 0.05 |
| Advanced (IB2 to IV) | 237 (68%) | 221 (67%) | 16 (89%) | |
| Lymph node metastases, n (%) | ||||
| No | 256 (74%) | 243 (74%) | 13 (72%) | 0.89 |
| Yes | 92 (26%) | 87 (26%) | 5 (28%) | |
| HPV genotype, n (%) | ||||
| HPV16 | 241 (69%) | 230 (70%) | 11 (61%) | 0.44 |
| Other | 107 (31%) | 100 (30%) | 6 (39%) | |
| Center, n (%) | ||||
| IPOLFG | 158 (45%) | 148 (45%) | 10 (56%) | 0.37 |
| HCB | 190 (55%) | 182 (55%) | 8 (44%) | |
| Variables | Mortality | Relapse | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| HPV genotype | ||||||
| Other | 1 | 1 | ||||
| HPV16 | 0.58 | 0.37–0.92 | 0.0198 | 0.63 | 0.43–0.92 | 0.0174 |
| P16 | ||||||
| Negative | 1 | 1 | ||||
| Positive | 0.37 | 0.17–0.79 | 0.0106 | 0.52 | 0.24–1.13 | 0.0991 |
| HPV genera | ||||||
| α-7 | 1 | 1 | ||||
| α-9 | 0.54 | 0.31–0.95 | 0.032 | 0.57 | 0.35–0.94 | 0.0286 |
| α-7 and α-9 | 0.77 | 0.28–2.11 | 0.612 | 0.82 | 0.35–1.93 | 0.649 |
| Other | 0.95 | 0.28–3.26 | 0.935 | 0.71 | 0.21–2.38 | 0.5764 |
| FIGO stage 2018 | ||||||
| Early | 0.07 | 0.02–0.22 | <0.001 | 0.21 | 0.11-0.38 | <0.001 |
| Advanced | 1 | 1 | ||||
| Variables | Mortality | Relapse | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| HPV genotype | ||||||
| Other | 1 | 1 | ||||
| HPV16 | 0.71 | 0.42–1.11 | 0.141 | 0.71 | 0.47–1.08 | 0.086 |
| P16 | ||||||
| Negative | 1 | 1 | ||||
| Positive | 0.5 | 0.22–1.10 | 0.085 | 0.65 | 0.30–1.40 | 0.271 |
| FIGO stage 2018 | ||||||
| Early | 0.08 | 0.02–0.25 | <0.001 | 0.21 | 0.11–0.39 | <0.001 |
| Advanced | 1 | 1 | ||||
| Age | ||||||
| Per additional year | 1.01 | 0.99–1.02 | 0.209 | 1.00 | 0.98–1.01 | 0.634 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Mata, S.; Ferreira, J.; Nicolás, I.; Esteves, S.; Esteves, G.; Lérias, S.; Silva, F.; Saco, A.; Cochicho, D.; Cunha, M.; et al. P16 and HPV Genotype Significance in HPV-Associated Cervical Cancer—A Large Cohort of Two Tertiary Referral Centers. Int. J. Mol. Sci. 2021, 22, 2294. https://doi.org/10.3390/ijms22052294
da Mata S, Ferreira J, Nicolás I, Esteves S, Esteves G, Lérias S, Silva F, Saco A, Cochicho D, Cunha M, et al. P16 and HPV Genotype Significance in HPV-Associated Cervical Cancer—A Large Cohort of Two Tertiary Referral Centers. International Journal of Molecular Sciences. 2021; 22(5):2294. https://doi.org/10.3390/ijms22052294
Chicago/Turabian Styleda Mata, Sara, Joana Ferreira, Inmaculada Nicolás, Susana Esteves, Gonçalo Esteves, Sofia Lérias, Fernanda Silva, Adela Saco, Daniela Cochicho, Mário Cunha, and et al. 2021. "P16 and HPV Genotype Significance in HPV-Associated Cervical Cancer—A Large Cohort of Two Tertiary Referral Centers" International Journal of Molecular Sciences 22, no. 5: 2294. https://doi.org/10.3390/ijms22052294