
Expression of Calcitonin Gene-Related Peptide and Calcitonin Receptor-like Receptor in Colorectal Adenocarcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Serum CGRP in Colorectal Patients’ Characteristics
2.2. Histopathological and Immunohistochemical Tumor Analysis: CGRP and CRLR Immunohistochemical Identification and Final Staining Score
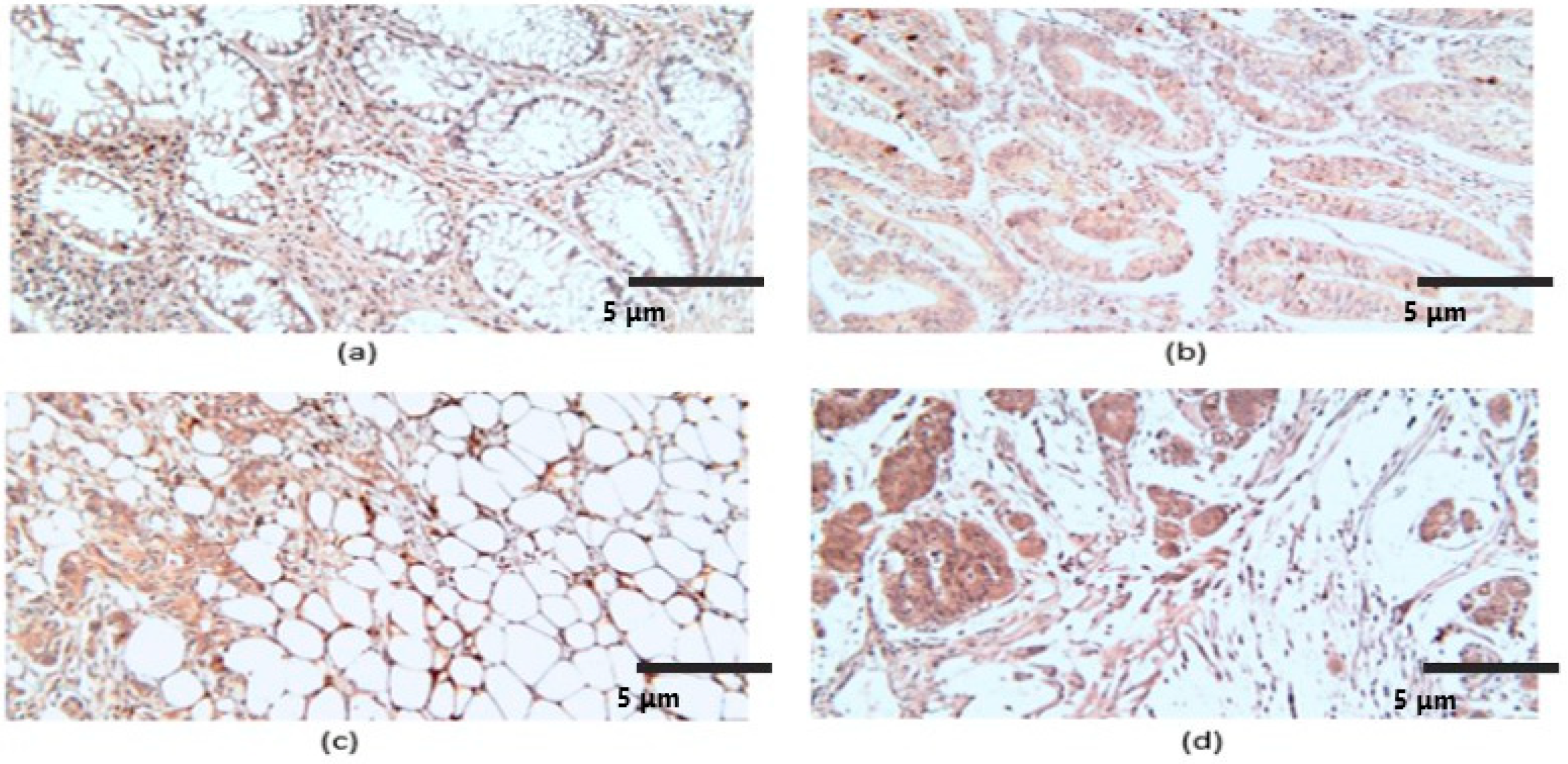
2.2.1. CGRP Histopathological and Immunohistochemical Characteristics
2.2.2. CRLR Histopathological and Immunohistochemical Characteristics
2.3. Comparison between the Immunohistochemical Final Staining Score of CGRP and CRLR according to Patients’ Clinical Data and Tumor Characteristics
3. Discussion
Limitations
4. Materials and Methods
4.1. Patient Selection
4.2. Enzyme-Linked Immunosorbent Assay (ELISA)
4.3. Histopathological (HP) and Immunohistochemical (IHC) Assays
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2017 Colorectal Cancer Collaborators. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 913–933. [Google Scholar] [CrossRef]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Stryjkowska-Góra, A.; Rudzki, S. Title: Risk Factors for the Diagnosis of Colorectal Cancer. Cancer Control 2022, 29, 10732748211056692. [Google Scholar] [CrossRef]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Kaminski, M.F.; Robertson, D.J.; Senore, C.; Rex, D.K. Optimizing the Quality of Colorectal Cancer Screening Worldwide. Gastroenterology 2020, 158, 404–417. [Google Scholar] [CrossRef]
- Carmine Belin, A.; Ran, C.; Edvinsson, L. Calcitonin Gene-Related Peptide (CGRP) and Cluster Headache. Brain Sci. 2020, 10, 30. [Google Scholar] [CrossRef]
- Edvinsson, L.; Ekman, R.; Jansen, I.; Ottosson, A.; Uddman, R. Peptide-containing nerve fibers in human cerebral arteries: Immunocytochemistry, radioimmunoassay and in vitro pharmacology. Ann. Neurol. 1987, 21, 431–437. [Google Scholar] [CrossRef]
- Brain, S.D.; Williams, T.J.; Tippins, J.R.; Morris, H.R.; MacIntyre, I. Calcitonin gene-related peptide is a potent vasodilator. Nature 1985, 313, 54–56. [Google Scholar] [CrossRef]
- Papantoniou, V.; Sotiropoulou, E.; Valsamaki, P.; Tsaroucha, A.; Sotiropoulou, M.; Ptohis, N.; Stipsanelli, A.; Dimitrakakis, K.; Marinopoulos, S.; Tsiouris, S.; et al. Breast density, scinti mammographic (99m)Tc(V)DMSA uptake, and calcitonin gene-related peptide (CGRP) expression in mixed invasive ductal associated with extensive in situ ductal carcinoma (IDC + DCIS) and pure invasive ductal carcinoma (IDC): Correlation with estrogen receptor (ER) status, proliferation index Ki-67, and histological grade. Breast Cancer 2011, 18, 286–291. [Google Scholar]
- Dömötör, A.; Peidl, Z.; Vincze, A.; Hunyady, B.; Szolcsányi, J.; Kereskay, L.; Szekeres, G.; Mózsik, G. Immunohistochemical distribution of vanilloid receptor, calcitonin-gene related peptide, and substance P in the gastrointestinal mucosa of patients with different gastrointestinal disorders. Inflammopharmacology 2005, 13, 161–177. [Google Scholar] [CrossRef]
- Vincze, Á.; Szekeres, G.; Király, Á.; Bódis, B.; Mózsik, G. The immunohistochemical distribution of capsaicin receptor, CGRP, and SP in the human gastric mucosa in patients with different gastric disorders. In Proceedings of the 11th International Conference, Calcutta, India, 22–25 November 2004; Sikiric, P., Seiwerth, P., Mózsik, G., Arakawa, T., Takeuchi, K., Eds.; Ulcer Research: Monduzzi, Bologna, 2004; pp. 149–153. [Google Scholar]
- Mózsik, G.; Peidl, Z.; Szolcsányi, J.; Dömötör, A.; Hideg, K.; Szekeres, G.; Hunyady, B. Participation of vanilloid/capsaicin receptors, substance P and calcitonin gene-related peptide in the omeprazole and omeprazole-like-induced gastric protection. Inflammopharmacology 2005, 13, 95–115. [Google Scholar] [CrossRef]
- Jörk, J.; Nilsson, J.; Hultcrantz, R.; Johansson, C. Growth-regulatory effects of sensory neuropeptides, epidermal growth factor, insulin, and somatostatin on the non-transformed intestinal epithelial cell line IEC-6 and the colon cancer cell line HT 29. Scand. J. Gastroenterol. 1993, 28, 879–884. [Google Scholar]
- Conteas, C.N.; Majumdar, P.N. The effects of gastrin. Epidermal growth factor, and somatostatin on DNA synthesis in a small intestinal crypt cell line (IEC-6). Proc. SOC Exp. Biol. Med. 1989, 184, 307–311. [Google Scholar] [CrossRef]
- Zhu, W.; Sheng, D.; Shao, Y.; Zhang, Q.; Peng, Y. Neuronal calcitonin gene-related peptide promotes prostate tumor growth in the bone microenvironment. Peptides 2021, 135, 170423. [Google Scholar] [CrossRef]
- McLatchie, L.M.; Fraser, N.J.; Main, M.J.; Wise, A.; Brown, J.; Thompson, N.; Solari, R.; Lee, M.G.; Foord, S.M. RAMPs regulate the transport and ligand specificity of the calcitonin-receptor-like receptor. Nature 1998, 393, 333–339. [Google Scholar] [CrossRef]
- Poyner, D.R. Calcitonin gene-related peptide: Multiple actions, multiple receptors. Pharmacol. Ther. 1992, 56, 23–51. [Google Scholar] [CrossRef]
- Muff, R.; Born, W.; Fischer, J.A. Calcitonin, calcitonin gene-related peptide, adrenomedullin, and amylin: Homologous peptides, separate receptors, and overlapping biological actions. Eur. J. Endocrinol. 1995, 133, 17–20. [Google Scholar] [CrossRef]
- Clifton, M.S.; Hoy, J.J.; Chang, J.; Idumalla, P.S.; Fakhruddin, H.; Grady, E.F.; Dada, S.; Corvera, C.U.; Bhargava, A. Role of calcitonin receptor-like receptor in colonic motility and inflammation. Am. J. Physiol.-Gastrointest. Liver Physiol. 2007, 293, G36–G44. [Google Scholar] [CrossRef]
- Logan, M.; Anderson, P.D.; Saab, S.T.; Hameed, O.; Abdulkadir, S.A. RAMP1 is a direct NKX3.1 target gene up-regulated in prostate cancer that promotes tumorigenesis. Am. J. Pathol. 2013, 183, 951–963. [Google Scholar] [CrossRef]
- Wende, B.; Beyer, A.L.; Ruhnke, N.; Kaemmerer, D.; Sänger, J.; Schulz, S.; Lupp, A. Expression of the Calcitonin Receptor-like Receptor (CALCRL) in Normal and Neoplastic Tissues. Int. J. Mol. Sci. 2023, 24, 3960. [Google Scholar] [CrossRef]
- Steenbergh, P.H.; Höppener, J.W.; Zandberg, J.; Lips, C.J.; Jansz, H.S. A second human calcitonin/CGRP gene. FEBS Lett. 1985, 183, 403–407. [Google Scholar] [CrossRef]
- Amara, S.G.; Jonas, V.; Rosenfeld, M.G.; Ong, E.S.; Evans, R.M. Alternative RNA processing in calcitonin gene expression generates mRNAs encoding different polypeptide products. Nature 1982, 298, 240–244. [Google Scholar] [CrossRef]
- Reavis, H.D.; Chen, H.I.; Drapkin, R. Tumor Innervation: Cancer Has Some Nerve. Trends Cancer 2020, 6, 1059–1067. [Google Scholar] [CrossRef]
- Austin, M.; Elliott, L.; Nicolaou, N.; Grabowska, A.; Hulse, R.P. Breast cancer-induced nociceptor aberrant growth and collateral sensory axonal branching. Oncotarget 2017, 8, 76606–76621. [Google Scholar] [CrossRef]
- Pundavela, J.; Roselli, S.; Faulkner, S.; Attia, J.; Scott, R.J.; Thorne, R.F.; Forbes, J.F.; Bradshaw, R.A.; Walker, M.M.; Jobling, P.; et al. Nerve fibers infiltrate the tumor microenvironment and are associated with nerve growth factor production and lymph node invasion in breast cancer. Mol. Oncol. 2015, 9, 1626–1635. [Google Scholar] [CrossRef]
- Wang, P.H.; Song, N.; Shi, L.B.; Zhang, Q.H.; Chen, Z.Y. The relationship between multiple clinicopathological features and nerve invasion in pancreatic cancer. Hepatobiliary Pancreat. Dis. Int. 2013, 12, 546–551. [Google Scholar] [CrossRef]
- Gutierrez, S.; Boada, M.D. Neuropeptide-induced modulation of carcinogenesis in a metastatic breast cancer cell line (MDA-MB-231LUC+). Cancer Cell Int. 2018, 18, 216. [Google Scholar] [CrossRef]
- Dallmayer, M.; Li, J.; Ohmura, S.; Alba Rubio, R.; Baldauf, M.C.; Hölting, T.L.B.; Musa, J.; Knott, M.M.L.; Stein, S.; Cidre-Aranaz, F.; et al. Targeting the CALCB/RAMP1 axis inhibits the growth of Ewing sarcoma. Cell Death Dis. 2019, 10, 116. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, C.; Wang, X.; Ji, T. Calcitonin gene-related peptide: A promising bridge between cancer development and cancer-associated pain in oral squamous cell carcinoma. Oncol. Lett. 2020, 20, 253. [Google Scholar] [CrossRef]
- Han, D. Association of Serum Levels of Calcitonin Gene-related Peptide and Cytokines during Migraine Attacks. Ann. Indian Acad. Neurol. 2019, 22, 277–281. [Google Scholar] [CrossRef]
- Shah, G.V.; Thomas, S.; Muralidharan, A.; Liu, Y.; Hermonat, P.L.; Williams, J.; Chaudhary, J. Calcitonin promotes in vivo metastasis of prostate cancer cells by altering cell signaling, adhesion, and inflammatory pathways. Endocr.-Relat. Cancer 2008, 15, 953–964. [Google Scholar] [CrossRef]
- Warrington, J.I.; Richards, G.O.; Wang, N. The role of the calcitonin peptide family in prostate cancer and bone metastasis. Curr. Mol. Biol. Rep. 2017, 3, 197–203. [Google Scholar] [CrossRef]
- Stepan, A.E.; Ciurea, R.N.; Drăgoescu, P.O.; Florescu, M.M.; Stepan, M.D. Immunoexpression of transcription factors in urothelial bladder carcinomas. Rom. J. Morphol. Embryol. 2017, 58, 863–869. [Google Scholar]
- Stepan, A.E.; Mărgăritescu, C.; Stoica, L.E.; Stepan, M.D.; Simionescu, C.E. Clear cell renal cell carcinomas–epithelial and mesenchymal immunophenotype. Rom. J. Morphol. Embryol. 2018, 59, 1189–1194. [Google Scholar]
- Hay, D.L.; Walker, C.S.; Poyner, D.R. Adrenomedullin and calcitonin gene-related peptide receptors in endocrine-related cancers: Opportunities and challenges. Endocr.-Relat. Cancer 2010, 18, C1–C14. [Google Scholar] [CrossRef]
- Kelley, M.J.; Snider, R.H.; Becker, K.L.; Johnson, B.E. Small cell lung carcinoma cell lines express mRNA for calcitonin and α- and β-calcitonin gene-related peptides. Cancer Lett. 1994, 81, 19–25. [Google Scholar] [CrossRef]
- Suzuki, K.; Kobayashi, Y.; Morita, T. Significance of serum calcitonin gene-related peptide levels in prostate cancer patients receiving hormonal therapy. Urol. Int. 2009, 82, 291–295. [Google Scholar] [CrossRef]
- Pacini, F.; Fugazzola, L.; Basolo, F.; Elisei, R.; Pinchera, A. Expression of calcitonin gene-related peptide in medullary thyroid cancer. J. Endocrinol. Investig. 1992, 15, 539–542. [Google Scholar] [CrossRef]
- Sánchez, M.L.; Rodríguez, F.D.; Coveñas, R. Peptidergic Systems and Cancer: Focus on Tachykinin and Calcitonin/Calcitonin Gene-Related Peptide Families. Cancers 2023, 15, 1694. [Google Scholar] [CrossRef]
- Toda, M.; Suzuki, T.; Hosono, K.; Hayashi, I.; Hashiba, S.; Onuma, Y.; Amano, H.; Kurihara, Y.; Kurihara, H.; Okamoto, H.; et al. Neuronal system-dependent facilitation of tumor angiogenesis and tumor growth by calcitonin gene-related peptide. Proc. Natl. Acad. Sci. USA 2008, 105, 13550–13555. [Google Scholar] [CrossRef]
- Grecu, A.F.; Popa, D.G.; Lungulescu, C.V.; Ciucă, E.M.; Camen, A.; Marinescu, D.; Nica, O.; Busuioc, C.J.; Chen, F.I.; Ciurea, M.E. Histological findings from rat calvaria defect augmented with platelet-rich fibrin by using two consecutive periosteal incisions. Rom. J. Morphol. Embryol. 2019, 60, 111–118. [Google Scholar]
- Dalsgaard, C.J.; Hultgardh Nilsson, A.; Haegerstrand, A.; Nilsson, J. Neuropeptides as growth factors. Possible roles in human diseases. Regul. Pept. 1989, 25, 1–9. [Google Scholar] [PubMed]
- Miller, M.J.; Martínez, A.; Unsworth, E.J.; Thiele, C.J.; Moody, T.W.; Elsasser, T.; Cuttitta, F. Adrenomedullin expression in human tumor cell lines. Its potential role as an autocrine growth factor. J. Biol. Chem. 1996, 271, 23345–23351. [Google Scholar] [PubMed]
- Aggarwal, G.; Ramachandran, V.; Javeed, N.; Arumugam, T.; Dutta, S.; Klee, G.G.; Klee, E.W.; Smyrk, T.C.; Bamlet, W.; Han, J.J.; et al. Adrenomedullin is up-regulated in patients with pancreatic cancer and causes insulin resistance in β cells and mice. Gastroenterology 2012, 143, 1510–1517.e1. [Google Scholar] [CrossRef] [PubMed]
- Qiao, F.; Fang, J.; Xu, J.; Zhao, W.; Ni, Y.; Akuo, B.A.; Zhang, W.; Liu, Y.; Ding, F.; Li, G.; et al. The role of adrenomedullin in the pathogenesis of gastric cancer. Oncotarget 2017, 8, 88464–88474. [Google Scholar] [CrossRef] [PubMed]
- Oehler, M.K.; Norbury, C.; Hague, S.; Rees, M.C.; Bicknell, R. Adrenomedullin inhibits hypoxic cell death by upregulation of Bcl-2 in endometrial cancer cells: A possible promotion mechanism for tumor growth. Oncogene 2001, 20, 2937–2945. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L. CGRP receptor antagonists and antibodies against CGRP and its receptor in migraine treatment. Br. J. Clin. Pharmacol. 2015, 80, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Underwood, E. FDA just approved the first drug to prevent migraines. Here’s the story of its discovery—And its limitations. Science 2018, 18, aae0189. [Google Scholar] [CrossRef]
- Pătraşcu, Ş.; Cercelaru, L.; Graure, G.M.; Firuţ, M.A.; Rotaru, I.; Cârţu, D.; Marinescu, D.; Pătraşcu, A.M.; Radu, R.I.; Mitroi, G.; et al. The histopathological features and their prognostic impact in the postoperative follow-up of colorectal cancer patients. Rom. J. Morphol. Embryol. 2022, 63, 555–561. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Classification of Tumours Editorial Board. In Digestive System Tumors, 5th ed.; International Agency for Research on Cancer (IARC) Press: Lyon, France, 2019; Volume 1. [Google Scholar]
- Andrici, J.; Farzin, M.; Sioson, L.; Clarkson, A.; Watson, N.; Toon, C.W.; Gill, A.J. Mismatch repair deficiency as a prognostic factor in mucinous colorectal cancer. Mod. Pathol. 2016, 29, 266–274. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient and Tumor Characteristics | No. Cases (%) | Serum CGRP Mean (ng/mL) | p-Value | |
|---|---|---|---|---|
| Gender | Male | 40 (74.1) | 7.4 | 0.61 * |
| Female | 14 (25.9) | 6.9 | ||
| Age | ≥69 years old | 30 (55.6) | 7.5 | 0.5 * |
| <69 years old | 24 (44.4) | 7 | ||
| Tumor Grade (G) | G1 | 10 (18.6) | 5.7 | <0.001 ** |
| G2 | 26 (48.1) | 7.6 | ||
| G3 | 18 (33.3) | 7.7 | ||
| Tumor extension (pT) | T1 | 4 (7.4) | 5.6 | <0.001 ** |
| T2 | 11 (20.4) | 6.7 | ||
| T3 | 29 (53.7) | 7.5 | ||
| T4 | 10 (18.5) | 8.8 | ||
| Regional lymph node metastasis (pN) | N0 | 29 (53.7) | 6.6 | 0.003 ** |
| N1 | 10 (18.5) | 8.4 | ||
| N2 | 15 (27.8) | 7.9 | ||
| Distant metastasis (pM) | M0 | 43 (79.6) | 7 | 0.007 * |
| M1a,c | 11 (20.4) | 8.4 | ||
| TNM stage | Control Group | 18 | 0.5 | <0.001 ** |
| I | 12 (22.2) | 5.9 | ||
| II | 16 (29.6) | 7.1 | ||
| III | 15 (27.8) | 7.8 | ||
| IV | 11 (20.4) | 8.4 | ||
| Tumor Characteristics | No. Cases (%) | CGRP FSS (Median) | p-Value | CRLR FSS (Median) | p-Value | |
|---|---|---|---|---|---|---|
| Tumor subtype | Non-mucinous | 42 (77.8) | 4.0 | 0.467 * | 6.0 | 0.537 * |
| Mucinous | 12 (22.2) | 5.0 | 6.0 | |||
| Tumor grade | Low grade (G1–G2) | 36 (66.7) | 4.0 | 0.001 * | 4.0 | <0.0005 * |
| High grade (G3) | 18 (33.3) | 9.0 | 8.5 | |||
| Tumor budding (Bd) | Bd 0 (absent) | 29 (53.7) | 4.0 | 0.081 ** | 4.0 | 0.054 ** |
| Bd 1 | 11 (20.4) | 4.0 | 6.0 | |||
| Bd 2 | 9 (16.7) | 6.0 | 6.0 | |||
| Bd 3 | 5 (9.2) | 9.0 | 9.0 | |||
| Poorly differentiated clusters (PDC) | PDC 0 (absent) | 43 (79.6) | 4.0 | 0.015 * | 4.0 | 0.001 * |
| PDC 1 (present) | 11 (20.4) | 9.0 | 9.0 | |||
| Vascular invasion | VI 0 (absent) | 28 (51.9) | 4.5 | 0.033 * | 4.0 | 0.065 * |
| VI 1 (present) | 26 (48.1) | 6.0 | 6.0 | |||
| Perineural invasion | PI 0 (absent) | 37 (68.5) | 4.0 | 0.013 * | 6.0 | 0.188 * |
| PI 1 (present) | 17 (31.5) | 9.0 | 6.0 | |||
| Tumor extension (pT) | T1 | 4 (7.4) | 1.5 | <0.0005 ** | 1.5 | <0.0005 ** |
| T2 | 11 (20.4) | 3.0 | 4.0 | |||
| T3 | 29 (53.7) | 4.0 | 6.0 | |||
| T4a,b | 10 (18.5) | 8.5 | 9.0 | |||
| Regional lymph node metastasis (pN) | N0 | 29 (53.7) | 4.0 | 0.001 ** | 4.0 | <0.0005 ** |
| N1a,b | 10 (18.5) | 5.0 | 6.0 | |||
| N2a,b | 15 (27.8) | 9.0 | 8.5 | |||
| Distant metastasis (pM) | M0 | 43 (79.6) | 4.0 | 0.007 * | 5.0 | <0.0005 * |
| M1a,c | 11 (20.4) | 6.0 | 10.0 | |||
| Tumor stage | I | 12 (22.2) | 2.0 | 0.001 ** | 2.0 | <0.0005 ** |
| II | 16 (29.6) | 4.0 | 4.0 | |||
| III | 15 (27.8) | 6.0 | 6.0 | |||
| IV | 11 (20.4) | 7.0 | 10.0 | |||
| Patients’ Characteristics | No. Cases (%) | CGRP FSS (Median) | p-Value * | CRLR FSS (Median) | p-Value * | |
|---|---|---|---|---|---|---|
| Gender | Male | 40 (74.1) | 6.0 | 0.776 | 6.0 | 0.642 |
| Female | 14 (25.9) | 2.0 | 3.0 | |||
| Age | ≥69 years old | 30 (55.6) | 4.0 | 0.531 | 4.0 | 0.130 |
| <69 years old | 24 (44.4) | 5.0 | 6.0 | |||
| Parameter | CGRP FSS Low | CGRP FSS High | χ2 Test | p-Value | |
|---|---|---|---|---|---|
| Gender | Male | 12 | 18 | 5.098 | 0.239 |
| Female | 17 | 7 | |||
| Age | ≥69 years old | 18 | 22 | 4.700 | 0.030 |
| <69 years old | 11 | 3 | |||
| TNM stage | I | 10 | 2 | 6.686 | 0.042 |
| II | 8 | 8 | |||
| III | 6 | 9 | |||
| IV | 4 | 7 | |||
| Tumor extension (pT) | T1 + T2 | 10 | 2 | 5.534 | 0.052 |
| T3 | 14 | 16 | |||
| T4 | 5 | 7 | |||
| Regional lymph node metastasis (pN) | N0 | 18 | 13 | 0.5567 | 0.455 |
| N1 + N2 | 11 | 12 | |||
| Distant metastasis (pM) | M0 | 24 | 19 | 0.378 | 0.538 |
| M1 | 5 | 6 | |||
| Tumor grade | G1 | 10 | 1 | 7.700 | 0.021 |
| G2 | 14 | 18 | |||
| G3 | 5 | 6 | |||
| Parameter | CRLR FSS Low | CRLR FSS High | χ2 Test | p-Value | |
|---|---|---|---|---|---|
| Gender | Male | 8 | 22 | 7.001 | 0.008 |
| Female | 15 | 9 | |||
| Age | ≥69 years old | 14 | 26 | 3.637 | 0.046 |
| <69 years old | 9 | 5 | |||
| TNM stage | I | 8 | 4 | 4.434 | 0.218 |
| II | 7 | 9 | |||
| III | 5 | 10 | |||
| IV | 3 | 8 | |||
| Tumor extension (pT) | T1 + T2 | 8 | 4 | 3.695 | 0.157 |
| T3 | 11 | 19 | |||
| T4 | 4 | 8 | |||
| Regional lymph node metastasis (pN) | N0 | 13 | 18 | 0.012 | 0.040 |
| N1 + N2 | 10 | 13 | |||
| Distant metastasis (pM) | M0 | 19 | 24 | 0.219 | 0.639 |
| M1 | 4 | 7 | |||
| Tumor grade | G1 | 8 | 3 | 5.143 | 0.763 |
| G2 | 11 | 21 | |||
| G3 | 4 | 7 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Șerban, R.-E.; Stepan, M.-D.; Florescu, D.N.; Boldeanu, M.-V.; Florescu, M.-M.; Șerbănescu, M.-S.; Ionescu, M.; Streba, L.; Drăgoescu, N.-A.-M.; Christopher, P.; et al. Expression of Calcitonin Gene-Related Peptide and Calcitonin Receptor-like Receptor in Colorectal Adenocarcinoma. Int. J. Mol. Sci. 2024, 25, 4461. https://doi.org/10.3390/ijms25084461
Șerban R-E, Stepan M-D, Florescu DN, Boldeanu M-V, Florescu M-M, Șerbănescu M-S, Ionescu M, Streba L, Drăgoescu N-A-M, Christopher P, et al. Expression of Calcitonin Gene-Related Peptide and Calcitonin Receptor-like Receptor in Colorectal Adenocarcinoma. International Journal of Molecular Sciences. 2024; 25(8):4461. https://doi.org/10.3390/ijms25084461
Chicago/Turabian StyleȘerban, Robert-Emmanuel, Mioara-Desdemona Stepan, Dan Nicolae Florescu, Mihail-Virgil Boldeanu, Mirela-Marinela Florescu, Mircea-Sebastian Șerbănescu, Mihaela Ionescu, Liliana Streba, Nicoleta-Alice-Marinela Drăgoescu, Pavel Christopher, and et al. 2024. "Expression of Calcitonin Gene-Related Peptide and Calcitonin Receptor-like Receptor in Colorectal Adenocarcinoma" International Journal of Molecular Sciences 25, no. 8: 4461. https://doi.org/10.3390/ijms25084461