
Novel Blood Biomarkers for Response Prediction and Monitoring of Stereotactic Ablative Radiotherapy and Immunotherapy in Metastatic Oligoprogressive Lung Cancer
 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Clinical Outcomes
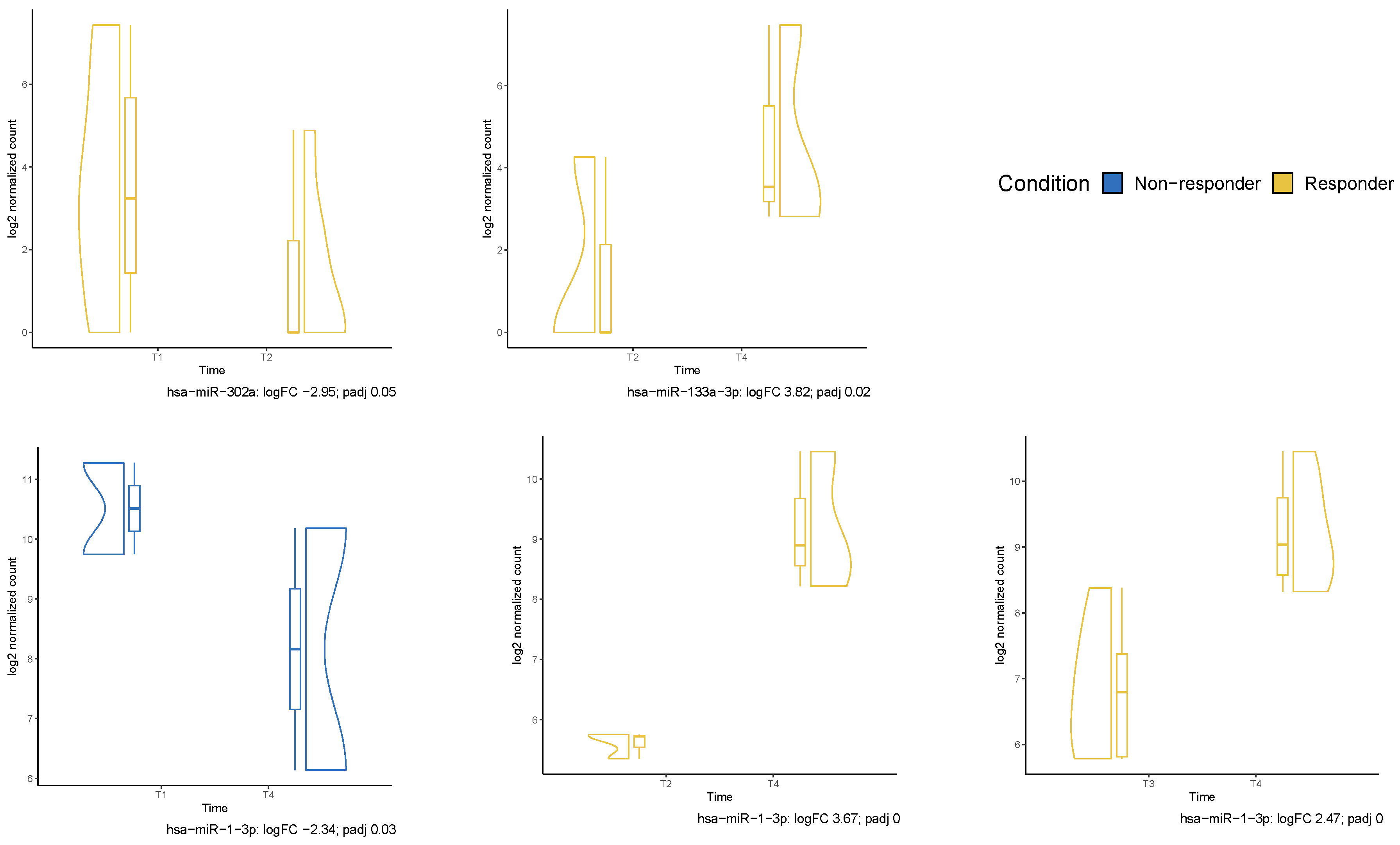
2.3. Liquid Biopsy Assessment
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Clinical Protocol
4.3. Translational Protocol
4.4. Study Endpoints
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bagchi, S.; Yuan, R.; Engleman, E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu. Rev. Pathol. 2021, 16, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.T.; Sun, Z.J. Turning cold tumors into hot tumors by improving T-cell infiltration. Theranostics 2021, 11, 5365–5386. [Google Scholar] [CrossRef] [PubMed]
- Abuodeh, Y.; Venkat, P.; Kim, S. Systematic review of case reports on the abscopal effect. Curr. Probl. Cancer 2016, 40, 25–37. [Google Scholar] [CrossRef]
- Chicas-Sett, R.; Morales-Orue, I.; Castilla-Martinez, J.; Zafra-Martin, J.; Kannemann, A.; Blanco, J.; Lloret, M.; Lara, P.C. Stereotactic Ablative Radiotherapy Combined with Immune Checkpoint Inhibitors Reboots the Immune Response Assisted by Immunotherapy in Metastatic Lung Cancer: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 2173. [Google Scholar] [CrossRef] [PubMed]
- Lievens, Y.; Guckenberger, M.; Gomez, D.; Hoyer, M.; Iyengar, P.; Kindts, I.; Romero, A.M.; Nevens, D.; Palma, D.; Park, C.; et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother. Oncol. 2020, 148, 157–166. [Google Scholar] [CrossRef]
- Popp, I.; Vaes, R.D.; Wieten, L.; Adebahr, S.; Hendriks, L.; Haghighi, E.B.; Degens, J.; Schäfer, H.; Greil, C.; Peeters, S.; et al. Radiotherapy to reinvigorate immunotherapy activity after acquired resistance in metastatic non-small-cell lung cancer: A pooled analysis of two institutions prospective phase II single arm trials. Radiother. Oncol. 2023, 190, 110048. [Google Scholar] [CrossRef]
- Franceschini, D.; De Rose, F.; Cozzi, S.; Franzese, C.; Rossi, S.; Finocchiaro, G.; Toschi, L.; Santoro, A.; Scorsetti, M. The use of radiation therapy for oligoprogressive/oligopersistent oncogene-driven non small cell lung cancer: State of the art. Crit. Rev. Oncol. Hematol. 2020, 148, 102894. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Shao, C. Radiotherapy-Mediated Immunomodulation and Anti-Tumor Abscopal Effect Combining Immune Checkpoint Blockade. Cancers 2020, 12, 2762. [Google Scholar] [CrossRef]
- Chicas-Sett, R.; Zafra, J.; Rodriguez-Abreu, D.; Castilla-Martinez, J.; Benitez, G.; Salas, B.; Hernandez, S.; Lloret, M.; Onieva, J.L.; Barragan, I.; et al. Combination of SABR With Anti-PD-1 in Oligoprogressive Non-Small Cell Lung Cancer and Melanoma: Results of a Prospective Multicenter Observational Study. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 655–665. [Google Scholar] [CrossRef]
- McBride, S.; Sherman, E.; Tsai, C.J.; Baxi, S.; Aghalar, J.; Eng, J.; Zhi, W.I.; McFarland, D.; Michel, L.S.; Young, R.; et al. Randomized Phase II Trial of Nivolumab With Stereotactic Body Radiotherapy Versus Nivolumab Alone in Metastatic Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2021, 39, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Gabos, Z.; Duimering, A.; Debenham, B.; Fairchild, A.; Huang, F.; Rowe, L.; Severin, D.; Giuliani, M.; Bezjak, A.; et al. Stereotactic Ablative Radiotherapy for Oligo-Progressive Cancers: Results of the Randomized Phase II STOP Trial. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, S58. [Google Scholar] [CrossRef]
- Nelson, B.E.; Adashek, J.J.; Sheth, A.A.; Subbiah, V. Predicting the Abscopal Effect: Associated Tumor Histologic Subtypes and Biomarkers. Mol. Cancer Ther. 2023, 22, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Semenkovich, N.; Samson, P.; Badiyan, S.; Vlacich, G.; Stowe, H.; Pellini, B.; Robinson, C.; Chaudhuri, A. Circulating Tumor DNA for Early Risk Stratification of Oligometastatic Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, S29–S30. [Google Scholar] [CrossRef]
- Sánchez-Herrero, E.; Serna-Blasco, R.; Robado de Lope, L.; González-Rumayor, V.; Romero, A.; Provencio, M. Circulating Tumor DNA as a Cancer Biomarker: An Overview of Biological Features and Factors That may Impact on ctDNA Analysis. Front. Oncol. 2022, 12, 943253. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Malapelle, U.; André, F.; Paz-Ares, L.; Schuler, M.; Thomas, D.M.; Vainer, G.; Yoshino, T.; Rolfo, C. Practical Considerations for the Use of Circulating Tumor DNA in the Treatment of Patients With Cancer: A Narrative Review. JAMA Oncol. 2022, 8, 1830–1839. [Google Scholar] [CrossRef]
- Oliver, J.; Onieva, J.L.; Garrido-Barros, M.; Cobo-Dols, M.; Martínez-Gálvez, B.; García-Pelícano, A.I.; Dubbelman, J.; Benítez, J.C.; Martín, J.Z.; Cantero, A.; et al. Fluorometric Quantification of Total Cell-Free DNA as a Prognostic Biomarker in Non-Small-Cell Lung Cancer Patients Treated with Immune Checkpoint Blockade. Cancers 2023, 15, 3357. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.H.; Song, C.; Eom, K.Y.; Kim, I.A.; Kim, J.S. Modulation of CD8(+) T Cell Responses by Radiotherapy-Current Evidence and Rationale for Combination with Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2023, 24, 16691. [Google Scholar] [CrossRef]
- Urabe, F.; Kosaka, N.; Ito, K.; Kimura, T.; Egawa, S.; Ochiya, T. Extracellular vesicles as biomarkers and therapeutic targets for cancer. Am. J. Physiol. Cell Physiol. 2020, 318, C29–C39. [Google Scholar] [CrossRef]
- Yang, Z.; Zhong, W.; Yang, L.; Wen, P.; Luo, Y.; Wu, C. The emerging role of exosomes in radiotherapy. Cell Commun. Signal 2022, 20, 171. [Google Scholar] [CrossRef] [PubMed]
- Wan, Z.; Dong, Y.; Wei, M.; Gao, X.; Yang, G.; Zhang, J.; Liu, L. Exosomes in Tumor Immunotherapy: Mediator, Drug Carrier, and Prognostic Biomarker. Adv. Biosyst. 2020, 4, e2000061. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.J.; Yang, J.T.; Shaverdian, N.; Patel, J.; Shepherd, A.F.; Guttmann, D.; Yeh, R.; Gelblum, D.Y.; Namakydoust, A.; Preeshagul, I.; et al. Standard-of-care systemic therapy with or without stereotactic body radiotherapy in patients with oligoprogressive breast cancer or non-small-cell lung cancer (Consolidative Use of Radiotherapy to Block [CURB] oligoprogression): An open-label, randomised, controlled, phase 2 study. Lancet 2024, 403, 171–182. [Google Scholar] [PubMed]
- Theelen, W.S.M.; Chen, D.; Verma, V.; Hobbs, B.P.; Peulen, H.M.U.; Aerts, J.G.J.V.; Bahce, I.; Niemeijer, A.L.N.; Chang, J.Y.; de Groot, P.M.; et al. Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Respir. Med. 2021, 9, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Eberst, G.; Vernerey, D.; Laheurte, C.; Meurisse, A.; Kaulek, V.; Cuche, L.; Jacoulet, P.; Almotlak, H.; Lahourcade, J.; Gainet-Brun, M.; et al. Prognostic value of CD4+ T lymphopenia in non-small cell lung Cancer. BMC Cancer 2022, 22, 529. [Google Scholar] [CrossRef] [PubMed]
- Gkika, E.; Firat, E.; Adebahr, S.; Graf, E.; Popp, I.; Radicioni, G.; Lo, S.S.; Nestle, U.; Nicolay, N.H.; Niedermann, G.; et al. Systemic immune modulation by stereotactic radiotherapy in early-stage lung cancer. NPJ Precis. Oncol. 2023, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.G.; Hong, M.H.; Kim, K.H.; Seo, I.-H.; Ahn, B.-C.; Pyo, K.-H.; Synn, C.-B.; Yoon, H.I.; Shim, H.S.; Lee, Y.I.; et al. Dynamic changes in circulating PD-1(+)CD8(+) T lymphocytes for predicting treatment response to PD-1 blockade in patients with non-small-cell lung cancer. Eur. J. Cancer 2021, 143, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gao, J.; Li, Y.; Nie, J.; Dai, L.; Hu, W.; Chen, X.; Han, J.; Ma, X.; Tian, G.; et al. Circulating PD-L1 in NSCLC patients and the correlation between the level of PD-L1 expression and the clinical characteristics. Thorac. Cancer 2015, 6, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Padinharayil, H.; Varghese, J.; John, M.C.; Rajanikant, G.K.; Wilson, C.M.; Al-Yozbaki, M.; Renu, K.; Dewanjee, S.; Sanyal, R.; Dey, A.; et al. Non-small cell lung carcinoma (NSCLC): Implications on molecular pathology and advances in early diagnostics and therapeutics. Genes. Dis. 2023, 10, 960–989. [Google Scholar] [CrossRef]
- Bousquets-Muñoz, P.; Díaz-Navarro, A.; Nadeu, F.; Sánchez-Pitiot, A.; López-Tamargo, S.; Shuai, S.; Balbín, M.; Tubio, J.M.C.; Beà, S.; Martin-Subero, J.I.; et al. PanCancer analysis of somatic mutations in repetitive regions reveals recurrent mutations in snRNA U2. NPJ Genom. Med. 2022, 7, 19. [Google Scholar] [CrossRef]
- Uhlen, M.; Karlsson, M.J.; Zhong, W.; Tebani, A.; Pou, C.; Mikes, J.; Lakshmikanth, T.; Forsström, B.; Edfors, F.; Odeberg, J.; et al. A genome-wide transcriptomic analysis of protein-coding genes in human blood cells. Science 2019, 366, eaax9198. [Google Scholar] [CrossRef] [PubMed]
- Zimta, A.A.; Sigurjonsson, O.E.; Gulei, D.; Tomuleasa, C. The Malignant Role of Exosomes as Nanocarriers of Rare RNA Species. Int. J. Mol. Sci. 2020, 21, 5866. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.; Wang, T.; Cao, X.; Sun, M.; Qu, Y. The role of receptor-type protein tyrosine phosphatases in cancer. Precis. Med. Sci. 2023, 12, 48–57. [Google Scholar] [CrossRef]
- Song, Y.; Wang, Z.; He, L.; Sun, F.; Zhang, B.; Wang, F. Dysregulation of Pseudogenes/lncRNA-Hsa-miR-1-3p-PAICS Pathway Promotes the Development of NSCLC. J. Oncol. 2022, 2022, 4714931. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.T.; Xu, W.X.; Li, H.; Xia, M. Emerging roles of MiR-133a in human cancers. J. Cancer 2021, 12, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Braghini, M.R.; Re, O.L.; Romito, I.; Fernandez-Barrena, M.G.; Barbaro, B.; Pomella, S.; Rota, R.; Vinciguerra, M.; Avila, M.A.; Alisi, A. Epigenetic remodelling in human hepatocellular carcinoma. J. Exp. Clin. Cancer Res. 2022, 41, 107. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Wang, G.; Zhang, C.; Liu, Y.; Chen, W.; Wang, H.; Liu, H. LncRNA SBF2-AS1 affects the radiosensitivity of non-small cell lung cancer via modulating microRNA-302a/MBNL3 axis. Cell Cycle 2020, 19, 300–316. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yan, J.; Chen, H.; Zhou, W.; Yang, J. MicroRNA-133a-3p Inhibits Lung Adenocarcinoma Development and Cisplatin Resistance through Targeting GINS4. Cells Tissues Organs. 2024, 213, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Tang, S.; Tang, S.; Zhang, J.; Guo, H.; Qin, C.; Hu, H.; Zhong, C.; Yang, L.; Zhu, Y.; et al. miRNAs in anti-cancer drug resistance of non-small cell lung cancer: Recent advances and future potential. Front. Pharmacol. 2022, 13, 949566. [Google Scholar] [CrossRef]
- de Miguel-Perez, D.; Ortega, F.G.; Tejada, R.G.; Martínez-Única, A.; Peterson, C.B.; Russo, A.; Gunasekaran, M.; Cardona, A.F.; Amezcua, V.; Lorente, J.A.; et al. Baseline extracellular vesicle miRNA-30c and autophagic CTCs predict chemoradiotherapy resistance and outcomes in patients with lung cancer. Biomark. Res. 2023, 11, 98. [Google Scholar] [CrossRef]
- Martin, J.Z.; Onieva, J.; Roman, A.; Garrido, M.; Oliver, J.; Martinez-Galvez, B.; Dubbelman, J.; Mesas, A.; Villatoro, R.; Ramos, I.; et al. Dynamic Exosome Analysis to Predict Response to the Combination of SABR and Immunotherapy in Oligoprogressive Disease. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, e274–e275. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- Spurr, L.F.; Martinez, C.; Kang, W.; Chen, M.; Zha, Y.; Hseu, R.; Gutiontov, S.; Turchan, W.T.; Lynch, C.; Pitroda, S.P.; et al. Concurrent Radiation Immunotherapy Augments Local Immunity Improves Survival in Aneuploid, NSCLC. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, S23. [Google Scholar] [CrossRef]
- US Department of Health and Human Services FaDA, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER). Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics. 2007. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics (accessed on 1 December 2022).
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- McGee, H.M.; Daly, M.E.; Azghadi, S.; Stewart, S.L.; Oesterich, L.; Schlom, J.; Donahue, R.; Schoenfeld, J.D.; Chen, Q.; Rao, S.; et al. Stereotactic Ablative Radiation Therapy Induces Systemic Differences in Peripheral Blood Immunophenotype Dependent on Irradiated Site. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1259–1270. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [PubMed]
- Onieva, J.L.; Cháves, P.; Oliver, J.; Garrido-Barros, M.; Zafra, J.; Sojo, B.; Sánchez, A.; Álvarez, M.; Jiménez, P.; Alba, E.; et al. Abstract 1910: flowTOTAL: A comprehensive bioinformatics workflow for flow cytometry automatic analysis. Cancer Res. 2022, 82 (Suppl. S12), 1910. [Google Scholar] [CrossRef]
- Li, J.; Kho, A.T.; Chase, R.P.; Pantano, L.; Farnam, L.; Amr, S.S.; Tantisira, K.G. COMPSRA: A COMprehensive Platform for Small RNA-Seq data Analysis. Sci. Rep. 2020, 10, 4552. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Formenti, S.C.; Rudqvist, N.-P.; Golden, E.; Cooper, B.; Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Friedman, K.; Ferrari de Andrade, L.; Wucherpfennig, K.W.; et al. Radiotherapy induces responses of lung cancer to CTLA-4 blockade. Nat. Med. 2018, 24, 1845–1851. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Gender | |
| Male | 14 (73.7%) |
| Female | 5 (26.3%) |
| Median age, years (range) | 67 (41–79) |
| ECOG | |
| 0 | 10 (52.6%) |
| 1 | 9 (47.4%) |
| Primary tumor | |
| Lung (non-squamous) | 11 (57.8%) |
| Lung (squamous) | 3 (15.8%) |
| Renal | 3 (15.8%) |
| Bladder | 1 (5.3%) |
| Cervix (squamous) | 1 (5.3%) |
| PD-L1 status (TPS) | |
| <50% | 3 (15.8%) |
| ≥50% | 9 (47.4%) |
| Unknown | 7 (36.8%) |
| Driver mutations | |
| Yes | 1 (5.3%) |
| No | 18 (94.7%) |
| Number of systemic therapy lines before SABR | |
| None | 12 (63.2%) |
| One | 7 (36.8%) |
| Prior radiotherapy | |
| Yes | 8 (42.1%) |
| No | 11 (57.9%) |
| Metastatic stage | |
| Oligometastatic (1–5 lesions) | 9 (47.4%) |
| Polymetastatic (>5 lesions) | 10 (52.6%) |
| Current systemic therapy | |
| ICI only | 15 (78.9%) |
| ICI plus chemotherapy | 4 (21.1%) |
| Primary resistance to ICI | |
| Yes | 4 (21.1%) |
| No | 15 (78.9%) |
| Irradiated tumor sites | |
| Lung | 10 (40%) |
| Nodes | 6 (24%) |
| Bone | 3 (12%) |
| Liver | 2 (8%) |
| Other | 4 (16%) |
| Number of irradiated sites | |
| One | 13 (62%) |
| Two | 6 (28%) |
| SABR dose | |
| 35 Gy/5 fx | 24 (98%) |
| 24 Gy/3 fx | 1 (2%) |
| Partial SABR | |
| Yes | 3 (15.4%) |
| No | 16 (84.2%) |
| Characteristic | Value |
|---|---|
| Gender | |
| Male | 6 (65%) |
| Female | 2 (25%) |
| Median age, years (range) | 68 (38–73) |
| ECOG | |
| 0 | 3 (37.5%) |
| 1 | 5 (62.5%) |
| Primary tumor | |
| Lung (non-squamous) | 4 (50%) |
| Renal | 2 (25%) |
| Colorectal | 1 (12.5%) |
| Liposarcoma | 1 (12.5%) |
| PD-L1 status (TPS) | |
| <50% | 2 (25%) |
| ≥50% | 1 (12.5%) |
| Unknown | 5 (62.5%) |
| Driver mutations | |
| No | 8 (100%) |
| Number of systemic therapy lines before SABR | |
| None | 5 (62.5%) |
| One | 2 (25%) |
| Two or more | 1 (12.5%) |
| Prior radiotherapy | |
| Yes | 4 (50%) |
| No | 4 (50%) |
| Metastatic stage | |
| Oligometastatic (1–5 lesions) | 7 (87.5%) |
| Polymetastatic (>5 lesions) | 1 (12.5%) |
| Irradiated tumor sites | |
| Lung | 6 (60%) |
| Nodes | 2 (20%) |
| Bone | 2 (20%) |
| Number of irradiated sites | |
| One | 6 (75%) |
| Two | 2 (25%) |
| SABR dose | |
| 54 Gy/3 fx | 2 (20%) |
| 50 Gy/5 fx | 4 (40%) |
| 35 Gy/5 fx | 1 (10%) |
| 30 Gy/3 fx | 1 (10%) |
| 27 Gy/3 fx | 1 (10%) |
| 30 Gy/5 fx | 1 (10%) |
| Partial SABR | |
| No | 8 (100%) |
| Endpoint | N (%) | |
|---|---|---|
| Cohort A | Cohort B | |
| Last Objective Response Rate (ORR) | 11/19 patients (57.9%) | 6/8 patients (75%) |
| Complete response | 4 (21.1%) | 3 (37.5%) |
| Partial response | 7 (36.8%) | 3 (37.5%) |
| Stable disease | 1 (5.3%) | 0 |
| Progression disease | 7 (36.8%) | 2 (25%) |
| Abscopal response (AR) at 8 weeks | ||
| Present | 5/14 patients (35.7%) | NA |
| Absent | 9/14 patients (64.3%) | NA |
| Local control (LC) | 22/25 lesions (88%) | 10/10 lesions (100%) |
| Complete response | 12 (48%) | 7 (70%) |
| Partial response | 8 (32%) | 3 (30%) |
| Stable disease | 2 (8%) | 0 |
| Progression disease | 3 (12%) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafra, J.; Onieva, J.L.; Oliver, J.; Garrido-Barros, M.; González-Hernández, A.; Martínez-Gálvez, B.; Román, A.; Ordóñez-Marmolejo, R.; Pérez-Ruiz, E.; Benítez, J.C.; et al. Novel Blood Biomarkers for Response Prediction and Monitoring of Stereotactic Ablative Radiotherapy and Immunotherapy in Metastatic Oligoprogressive Lung Cancer. Int. J. Mol. Sci. 2024, 25, 4533. https://doi.org/10.3390/ijms25084533
Zafra J, Onieva JL, Oliver J, Garrido-Barros M, González-Hernández A, Martínez-Gálvez B, Román A, Ordóñez-Marmolejo R, Pérez-Ruiz E, Benítez JC, et al. Novel Blood Biomarkers for Response Prediction and Monitoring of Stereotactic Ablative Radiotherapy and Immunotherapy in Metastatic Oligoprogressive Lung Cancer. International Journal of Molecular Sciences. 2024; 25(8):4533. https://doi.org/10.3390/ijms25084533
Chicago/Turabian StyleZafra, Juan, Juan Luis Onieva, Javier Oliver, María Garrido-Barros, Andrea González-Hernández, Beatriz Martínez-Gálvez, Alicia Román, Rafael Ordóñez-Marmolejo, Elisabeth Pérez-Ruiz, José Carlos Benítez, and et al. 2024. "Novel Blood Biomarkers for Response Prediction and Monitoring of Stereotactic Ablative Radiotherapy and Immunotherapy in Metastatic Oligoprogressive Lung Cancer" International Journal of Molecular Sciences 25, no. 8: 4533. https://doi.org/10.3390/ijms25084533