
Profile of Lipoprotein Subclasses in Chinese Primary Open-Angle Glaucoma Patients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Features of Study Subjects
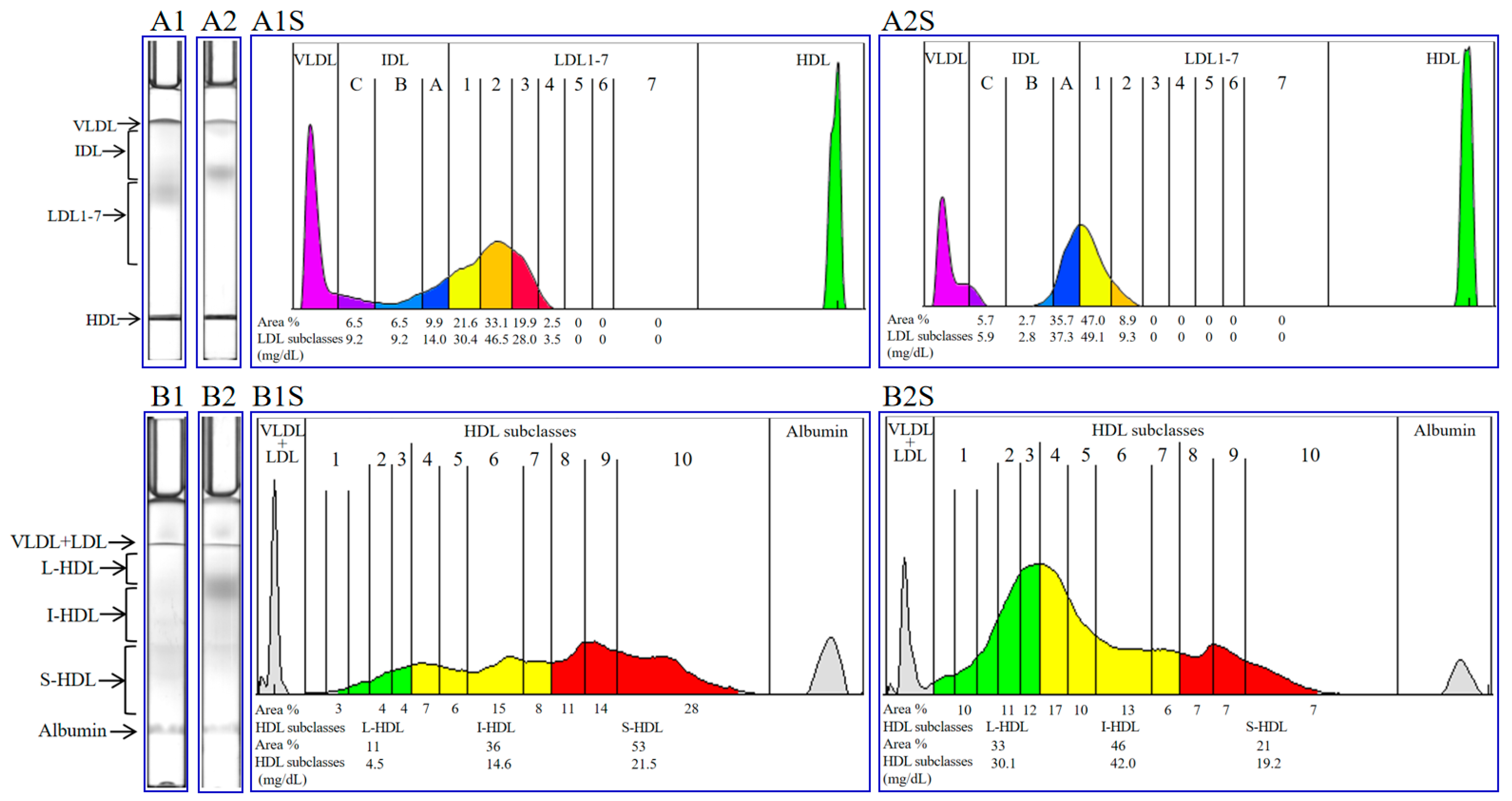
2.2. Profiles of Lipoproteins in Primary Open-Angle Glaucoma Patients
2.3. Subclasses of Lipoproteins in Primary Open-Angle Glaucoma Patients
2.4. Receiver Operating Characteristic (ROC) and Clinical Correlation Analyses
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Ophthalmic Examinations
4.3. Blood Collection and Lipoprotein Analysis
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 2183–2193. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Leung, C.K.; Crowston, J.G.; Medeiros, F.A.; Friedman, D.S.; Wiggs, J.L.; Martin, K.R. Primary open-angle glaucoma. Nat. Rev. Dis. Prim. 2016, 2, 16067. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.; Bhardwaj, A.; Yadav, A.; Dada, R.; Tanwar, M. Molecular genetics of primary open-angle glaucoma. Indian J. Ophthalmol. 2023, 71, 1739–1756. [Google Scholar] [CrossRef]
- Jammal, A.A.; Thompson, A.C.; Mariottoni, E.B.; Estrela, T.; Shigueoka, L.S.; Berchuck, S.I.; Medeiros, F.A. Impact of Intraocular Pressure Control on Rates of Retinal Nerve Fiber Layer Loss in a Large Clinical Population. Ophthalmology 2021, 128, 48–57. [Google Scholar] [CrossRef]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative Effectiveness of First-Line Medications for Primary Open-Angle Glaucoma: A Systematic Review and Network Meta-analysis. Ophthalmology 2016, 123, 129–140. [Google Scholar] [CrossRef]
- Gupta, D.; Chen, P.P. Glaucoma. Am. Fam. Physician 2016, 93, 668–674. [Google Scholar]
- Malihi, M.; Moura, F.E.; Hodge, D.O.; Sit, A.J. Long-term trends in glaucoma-related blindness in Olmsted County, Minnesota. Ophthalmology 2014, 121, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Huang, C.; Zheng, Y.; Yuan, X.L.; Chen, S.; Xu, Y.; Chen, L.J.; Pang, C.P.; Zhang, M.; Ng, T.K. Primary open-angle glaucoma risk prediction with ABCA1 and LOC102723944 variants and their genotype-phenotype correlations in southern Chinese population. Mol. Genet. Genom. 2023, 298, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Thorleifsson, G.; Walters, G.B.; Hewitt, A.W.; Masson, G.; Helgason, A.; DeWan, A.; Sigurdsson, A.; Jonasdottir, A.; Gudjonsson, S.A.; Magnusson, K.P.; et al. Common variants near CAV1 and CAV2 are associated with primary open-angle glaucoma. Nat. Genet. 2010, 42, 906–909. [Google Scholar] [CrossRef]
- Mukhamedova, N.; Hoang, A.; Cui, H.L.; Carmichael, I.; Fu, Y.; Bukrinsky, M.; Sviridov, D. Small GTPase ARF6 Regulates Endocytic Pathway Leading to Degradation of ATP-Binding Cassette Transporter A1. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 2292–2303. [Google Scholar] [CrossRef]
- Tan, M.; Ye, J.; Zhao, M.; Ke, X.; Huang, K.; Liu, H. Recent developments in the regulation of cholesterol transport by natural molecules. Phytother. Res. 2021, 35, 5623–5633. [Google Scholar] [CrossRef] [PubMed]
- Truong, T.Q.; Aubin, D.; Falstrault, L.; Brodeur, M.R.; Brissette, L. SR-BI, CD36, and caveolin-1 contribute positively to cholesterol efflux in hepatic cells. Cell Biochem. Funct. 2010, 28, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Joshi, R.S.; Adatiya, V.H. Study of the relationship between serum lipid levels and primary open-angle glaucoma. Indian J. Ophthalmol. 2023, 71, 1948–1952. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Boumenna, T.; Stein, J.D.; Khawaja, A.; Rosner, B.A.; Wiggs, J.L.; Pasquale, L.R. Association of Statin Use and High Serum Cholesterol Levels With Risk of Primary Open-Angle Glaucoma. JAMA Ophthalmol. 2019, 137, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, Y.; Zou, T.; Xue, B.; Yang, F.; Wang, X.; Huo, Y.; Yan, B.; Xu, Y.; He, S.; et al. Cholesterol homeostasis regulated by ABCA1 is critical for retinal ganglion cell survival. Sci. China-Life Sci. 2023, 66, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Wang, J.; Li, L.; Gao, Y.; Yan, Y. Meta-Analysis of Dyslipidemia and Blood Lipid Parameters on the Risk of Primary Open-Angle Glaucoma. Comput. Math. Method. Med. 2022, 2022, 1122994. [Google Scholar] [CrossRef]
- Xu, M.; Li, S.; Zhu, J.; Luo, D.; Song, W.; Zhou, M. Plasma lipid levels and risk of primary open angle glaucoma: A genetic study using Mendelian randomization. BMC Ophthalmol. 2020, 20, 390. [Google Scholar] [CrossRef]
- Newman-Casey, P.A.; Talwar, N.; Nan, B.; Musch, D.C.; Stein, J.D. The relationship between components of metabolic syndrome and open-angle glaucoma. Ophthalmology 2011, 118, 1318–1326. [Google Scholar] [CrossRef]
- Nusinovici, S.; Li, H.; Thakur, S.; Baskaran, M.; Tham, Y.C.; Zhou, L.; Sabanayagam, C.; Aung, T.; Silver, D.; Fan, Q.; et al. High-Density Lipoprotein 3 Cholesterol and Primary Open-Angle Glaucoma: Metabolomics and Mendelian Randomization Analyses. Ophthalmology 2022, 129, 285–294. [Google Scholar] [CrossRef]
- Jimenez, B.; Holmes, E.; Heude, C.; Tolson, R.F.; Harvey, N.; Lodge, S.L.; Chetwynd, A.J.; Cannet, C.; Fang, F.; Pearce, J.; et al. Quantitative Lipoprotein Subclass and Low Molecular Weight Metabolite Analysis in Human Serum and Plasma by (1)H NMR Spectroscopy in a Multilaboratory Trial. Anal. Chem. 2018, 90, 11962–11971. [Google Scholar] [CrossRef]
- Itabe, H.; Obama, T. The Oxidized Lipoproteins In Vivo: Its Diversity and Behavior in the Human Circulation. Int. J. Mol. Sci. 2023, 24, 5747. [Google Scholar] [CrossRef]
- Ivanova, E.A.; Myasoedova, V.A.; Melnichenko, A.A.; Grechko, A.V.; Orekhov, A.N. Small Dense Low-Density Lipoprotein as Biomarker for Atherosclerotic Diseases. Oxidative Med. Cell. Longev. 2017, 2017, 1273042. [Google Scholar] [CrossRef] [PubMed]
- Chapman, M.J.; Laplaud, P.M.; Luc, G.; Forgez, P.; Bruckert, E.; Goulinet, S.; Lagrange, D. Further resolution of the low density lipoprotein spectrum in normal human plasma: Physicochemical characteristics of discrete subspecies separated by density gradient ultracentrifugation. J. Lipid Res. 1988, 29, 442–458. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.M.; Deng, J.; Tomann, A.B.; Shah, A.S.; Lu, L.J.; Davidson, W.S. Multi-dimensional co-separation analysis reveals protein-protein interactions defining plasma lipoprotein subspecies. Mol. Cell. Proteom. 2013, 12, 3123–3134. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Garruti, G.; Liu, M.; Portincasa, P.; Wang, D.Q. Cholesterol and Lipoprotein Metabolism and Atherosclerosis: Recent Advances In reverse Cholesterol Transport. Ann. Hepatol. 2017, 16, s27–s42. [Google Scholar] [CrossRef] [PubMed]
- Woudberg, N.J.; Pedretti, S.; Lecour, S.; Schulz, R.; Vuilleumier, N.; James, R.W.; Frias, M.A. Pharmacological Intervention to Modulate HDL: What Do We Target? Front. Pharmacol. 2017, 8, 989. [Google Scholar] [CrossRef] [PubMed]
- Pokharel, Y.; Mouhanna, F.; Nambi, V.; Virani, S.S.; Hoogeveen, R.; Alonso, A.; Heiss, G.; Coresh, J.; Mosley, T.; Gottesman, R.F.; et al. ApoB, small-dense LDL-C, Lp(a), LpPLA(2) activity, and cognitive change. Neurology 2019, 92, e2580–e2593. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Nikiforov, N.G.; Markin, A.M.; Kashirskikh, D.A.; Myasoedova, V.A.; Gerasimova, E.V.; Orekhov, A.N. Overview of oxLDL and Its Impact on Cardiovascular Health: Focus on Atherosclerosis. Front. Pharmacol. 2020, 11, 613780. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Su, J.; Yan, Y.; Zhao, Q.; Ma, J.; Zhu, M.; He, X.; Zhang, B.; Xu, H.; Yang, X.; et al. Intermittent Fasting Inhibits High-Fat Diet-Induced Atherosclerosis by Ameliorating Hypercholesterolemia and Reducing Monocyte Chemoattraction. Front. Pharmacol. 2021, 12, 719750. [Google Scholar] [CrossRef]
- Zhang, X.; Qiu, B.; Wang, Q.; Sivaprasad, S.; Wang, Y.; Zhao, L.; Xie, R.; Li, L.; Kang, W. Dysregulated Serum Lipid Metabolism Promotes the Occurrence and Development of Diabetic Retinopathy Associated With Upregulated Circulating Levels of VEGF-A, VEGF-D, and PlGF. Front. Med. 2021, 8, 779413. [Google Scholar] [CrossRef]
- Fernandez-Friera, L.; Fuster, V.; Lopez-Melgar, B.; Oliva, B.; Garcia-Ruiz, J.M.; Mendiguren, J.; Bueno, H.; Pocock, S.; Ibanez, B.; Fernandez-Ortiz, A.; et al. Normal LDL-Cholesterol Levels Are Associated With Subclinical Atherosclerosis in the Absence of Risk Factors. J. Am. Coll. Cardiol. 2017, 70, 2979–2991. [Google Scholar] [CrossRef]
- Wilson, P.; Polonsky, T.S.; Miedema, M.D.; Khera, A.; Kosinski, A.S.; Kuvin, J.T. Systematic Review for the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1144–e1161. [Google Scholar] [CrossRef]
- Brown, M.S.; Goldstein, J.L. A receptor-mediated pathway for cholesterol homeostasis. Science 1986, 232, 34–47. [Google Scholar] [CrossRef]
- Superko, H.; Garrett, B. Small Dense LDL: Scientific Background, Clinical Relevance, and Recent Evidence Still a Risk Even with N‘ormal’ LDL-C Levels. Biomedicines 2022, 10, 829. [Google Scholar] [CrossRef]
- Tian, L.; Fu, M. The relationship between high density lipoprotein subclass profile and plasma lipids concentrations. Lipids Health Dis. 2010, 9, 118. [Google Scholar] [CrossRef]
- Yang, Y.; Yan, B.; Fu, M.; Xu, Y.; Tian, Y. Relationship between plasma lipid concentrations and HDL subclasses. Clin. Chim. Acta 2005, 354, 49–58. [Google Scholar] [CrossRef]
- Xiao, C.; Dash, S.; Morgantini, C.; Hegele, R.A.; Lewis, G.F. Pharmacological Targeting of the Atherogenic Dyslipidemia Complex: The Next Frontier in CVD Prevention Beyond Lowering LDL Cholesterol. Diabetes 2016, 65, 1767–1778. [Google Scholar] [CrossRef]
- Neels, J.G.; Leftheriotis, G.; Chinetti, G. Atherosclerosis Calcification: Focus on Lipoproteins. Metabolites 2023, 13, 457. [Google Scholar] [CrossRef]
- Thongtang, N.; Diffenderfer, M.R.; Ooi, E.; Barrett, P.; Turner, S.M.; Le, N.A.; Brown, W.V.; Schaefer, E.J. Metabolism and proteomics of large and small dense LDL in combined hyperlipidemia: Effects of rosuvastatin. J. Lipid Res. 2017, 58, 1315–1324. [Google Scholar] [CrossRef]
- Packard, C.J. Small dense low-density lipoprotein and its role as an independent predictor of cardiovascular disease. Curr. Opin. Lipidol. 2006, 17, 412–417. [Google Scholar] [CrossRef]
- Galeano, N.F.; Milne, R.; Marcel, Y.L.; Walsh, M.T.; Levy, E.; Ngu’Yen, T.D.; Gleeson, A.; Arad, Y.; Witte, L.; Al-Haideri, M.; et al. Apoprotein B structure and receptor recognition of triglyceride-rich low density lipoprotein (LDL) is modified in small LDL but not in triglyceride-rich LDL of normal size. J. Biol. Chem. 1994, 269, 511–519. [Google Scholar] [CrossRef]
- Anber, V.; Griffin, B.A.; McConnell, M.; Packard, C.J.; Shepherd, J. Influence of plasma lipid and LDL-subfraction profile on the interaction between low density lipoprotein with human arterial wall proteoglycans. Atherosclerosis 1996, 124, 261–271. [Google Scholar] [CrossRef]
- Ryu, W.S.; Woo, S.H.; Schellingerhout, D.; Jang, M.U.; Park, K.J.; Hong, K.S.; Jeong, S.W.; Na, J.Y.; Cho, K.H.; Kim, J.T.; et al. Stroke outcomes are worse with larger leukoaraiosis volumes. Brain 2017, 140, 158–170. [Google Scholar] [CrossRef]
- Moore, N.A.; Harris, A.; Wentz, S.; Verticchio, V.A.; Parekh, P.; Gross, J.; Hussain, R.M.; Thieme, C.; Siesky, B. Baseline retrobulbar blood flow is associated with both functional and structural glaucomatous progression after 4 years. Br. J. Ophthalmol. 2017, 101, 305–308. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, C.; Ko, T.; Kong, X.; Yu, X.; Min, W.; Shi, G.; Sun, X. Correlation between optic disc perfusion and glaucomatous severity in patients with open-angle glaucoma: An optical coherence tomography angiography study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1557–1564. [Google Scholar] [CrossRef]
- Nakazawa, T. Ocular Blood Flow and Influencing Factors for Glaucoma. Asia-Pac. J. Ophthalmol. 2016, 5, 38–44. [Google Scholar] [CrossRef]
- Tribble, D.L.; Holl, L.G.; Wood, P.D.; Krauss, R.M. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis 1992, 93, 189–199. [Google Scholar] [CrossRef]
- Tribble, D.L.; Rizzo, M.; Chait, A.; Lewis, D.M.; Blanche, P.J.; Krauss, R.M. Enhanced oxidative susceptibility and reduced antioxidant content of metabolic precursors of small, dense low-density lipoproteins. Am. J. Med. 2001, 110, 103–110. [Google Scholar] [CrossRef]
- Berliner, J.A.; Navab, M.; Fogelman, A.M.; Frank, J.S.; Demer, L.L.; Edwards, P.A.; Watson, A.D.; Lusis, A.J. Atherosclerosis: Basic mechanisms. Oxidation, inflammation, and genetics. Circulation 1995, 91, 2488–2496. [Google Scholar] [CrossRef]
- Yoshida, H.; Kisugi, R. Mechanisms of LDL oxidation. Clin. Chim. Acta 2010, 411, 1875–1882. [Google Scholar] [CrossRef]
- Zhan, R.; Zhao, M.; Zhou, T.; Chen, Y.; Yu, W.; Zhao, L.; Zhang, T.; Wang, H.; Yang, H.; Jin, Y.; et al. Dapsone protects brain microvascular integrity from high-fat diet induced LDL oxidation. Cell Death Dis. 2018, 9, 683. [Google Scholar] [CrossRef]
- Dammak, A.; Huete-Toral, F.; Carpena-Torres, C.; Martin-Gil, A.; Pastrana, C.; Carracedo, G. From Oxidative Stress to Inflammation in the Posterior Ocular Diseases: Diagnosis and Treatment. Pharmaceutics 2021, 13, 1376. [Google Scholar] [CrossRef]
- Helin-Toiviainen, M.; Ronkko, S.; Kaarniranta, K.; Puustjarvi, T.; Rekonen, P.; Ollikainen, M.; Uusitalo, H. Oxidized low-density lipoprotein, lipid and calcium aggregates reveal oxidative stress and inflammation in the conjunctiva of glaucoma patients. Acta Ophthalmol. 2017, 95, 378–385. [Google Scholar] [CrossRef]
- Ghanem, A.A.; Arafa, L.F.; El-Baz, A. Oxidative stress markers in patients with primary open-angle glaucoma. Curr. Eye Res. 2010, 35, 295–301. [Google Scholar] [CrossRef]
- Goyal, A.; Srivastava, A.; Sihota, R.; Kaur, J. Evaluation of oxidative stress markers in aqueous humor of primary open angle glaucoma and primary angle closure glaucoma patients. Curr. Eye Res. 2014, 39, 823–829. [Google Scholar] [CrossRef]
- Ferreira, S.M.; Lerner, S.F.; Brunzini, R.; Evelson, P.A.; Llesuy, S.F. Oxidative stress markers in aqueous humor of glaucoma patients. Am. J. Ophthalmol. 2004, 137, 62–69. [Google Scholar] [CrossRef]
- Camont, L.; Chapman, M.J.; Kontush, A. Biological activities of HDL subpopulations and their relevance to cardiovascular disease. Trends Mol. Med. 2011, 17, 594–603. [Google Scholar] [CrossRef]
- Du, X.M.; Kim, M.J.; Hou, L.; Le Goff, W.; Chapman, M.J.; Van Eck, M.; Curtiss, L.K.; Burnett, J.R.; Cartland, S.P.; Quinn, C.M.; et al. HDL particle size is a critical determinant of ABCA1-mediated macrophage cellular cholesterol export. Circ. Res. 2015, 116, 1133–1142. [Google Scholar] [CrossRef]
- Talbot, C.; Plat, J.; Ritsch, A.; Mensink, R.P. Determinants of cholesterol efflux capacity in humans. Prog. Lipid Res. 2018, 69, 21–32. [Google Scholar] [CrossRef]
- Wu, H.; Fang, F.; Wang, C.; Hong, X.; Chen, D.; Huang, X. Selective Molecular Recognition of Low Density Lipoprotein Based on beta-Cyclodextrin Coated Electrochemical Biosensor. Biosensors 2021, 11, 216. [Google Scholar] [CrossRef]
- Rohatgi, A.; Westerterp, M.; von Eckardstein, A.; Remaley, A.; Rye, K.A. HDL in the 21st Century: A Multifunctional Roadmap for Future HDL Research. Circulation 2021, 143, 2293–2309. [Google Scholar] [CrossRef]
- Genoux, A.; Lichtenstein, L.; Ferrieres, J.; Duparc, T.; Bongard, V.; Vervueren, P.L.; Combes, G.; Taraszkiewicz, D.; Elbaz, M.; Galinier, M.; et al. Serum levels of mitochondrial inhibitory factor 1 are independently associated with long-term prognosis in coronary artery disease: The GENES Study. BMC Med. 2016, 14, 125. [Google Scholar] [CrossRef]
- Duncan, M.S.; Vasan, R.S.; Xanthakis, V. Trajectories of Blood Lipid Concentrations Over the Adult Life Course and Risk of Cardiovascular Disease and All-Cause Mortality: Observations From the Framingham Study Over 35 Years. J. Am. Heart Assoc. 2019, 8, e11433. [Google Scholar] [CrossRef]
- Anderson, D.R.; Chauhan, B.; Johnson, C.; Katz, J.; Patella, V.M.; Drance, S.M. Criteria for progression of glaucoma in clinical management and in outcome studies. Am. J. Ophthalmol. 2000, 130, 827–829. [Google Scholar] [CrossRef]
- Dioszegi, A.; Lorincz, H.; Kaali, E.; Soltesz, P.; Perge, B.; Varga, E.; Harangi, M.; Tarr, T. Role of Altered Metabolism of Triglyceride-Rich Lipoprotein Particles in the Development of Vascular Dysfunction in Systemic Lupus Erythematosus. Biomolecules 2023, 13, 401. [Google Scholar] [CrossRef]
- Otrante, A.; Bounafaa, A.; Berrougui, H.; Essamadi, A.K.; Nguyen, M.; Fulop, T.; Khalil, A. Small Dense LDL Level and LDL/HDL Distribution in Acute Coronary Syndrome Patients. Biomedicines 2023, 11, 1198. [Google Scholar] [CrossRef]
- Zhou, P.; Shen, Y.; Wang, L.; Cao, Z.; Feng, W.; Liu, J.; Wang, L.; Meng, P.; Yang, J.; Xu, W.Y.; et al. Association between carotid intima media thickness and small dense low-density lipoprotein cholesterol in acute ischaemic stroke. Lipids Health Dis. 2020, 19, 177. [Google Scholar] [CrossRef]
- Woudberg, N.J.; Goedecke, J.H.; Blackhurst, D.; Frias, M.; James, R.; Opie, L.H.; Lecour, S. Association between ethnicity and obesity with high-density lipoprotein (HDL) function and subclass distribution. Lipids Health Dis. 2016, 15, 92. [Google Scholar] [CrossRef]
- Su, X.; Kong, Y.; Peng, D. Evidence for changing lipid management strategy to focus on non-high density lipoprotein cholesterol. Lipids Health Dis. 2019, 18, 134. [Google Scholar] [CrossRef]
- Contois, J.H.; Warnick, G.R.; Sniderman, A.D. Reliability of low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, and apolipoprotein B measurement. J. Clin. Lipidol. 2011, 5, 264–272. [Google Scholar] [CrossRef]
- Zhang, N.; Hu, X.; Zhang, Q.; Bai, P.; Cai, M.; Zeng, T.S.; Zhang, J.Y.; Tian, S.H.; Min, J.; Huang, H.T.; et al. Non-high-density lipoprotein cholesterol: High-density lipoprotein cholesterol ratio is an independent risk factor for diabetes mellitus: Results from a population-based cohort study. J. Diabetes 2018, 10, 708–714. [Google Scholar] [CrossRef]
- Johnston, N.; Jernberg, T.; Lagerqvist, B.; Siegbahn, A.; Wallentin, L. Oxidized low-density lipoprotein as a predictor of outcome in patients with unstable coronary artery disease. Int. J. Cardiol. 2006, 113, 167–173. [Google Scholar] [CrossRef]
- Yan, Z.; Fu, B.; He, D.; Zhang, Y.; Liu, J.; Zhang, X. The relationship between oxidized low-density lipoprotein and related ratio and acute cerebral infarction. Medicine 2018, 97, e12642. [Google Scholar] [CrossRef]
- Joint Committee on the Chinese Guidelines for Lipid Management. Chinese guidelines for lipid management (2023). Chin. Circ. J. 2023, 38, 237–271. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Elevated TC and/or LDL-C | Normal TC and LDL-C | ||||
|---|---|---|---|---|---|---|
| POAG (n = 10) | Control (n = 10) | p Value | POAG (n = 10) | Control (n = 10) | p Value | |
| Age (years) | 68.60 ± 7.12 | 65.30 ± 7.51 | 0.764 a | 68.40 ± 8.10 | 68.40 ± 9.20 | 1.000 a |
| Male/female sex | 7/3 | 5/5 | 0.361 b | 7/3 | 6/4 | 0.639 b |
| Right IOP (mmHg) | 14.30 ± 3.89 | 15.80 ± 3.91 | 0.401 a | 15.50 ± 5.32 | 12.70 ± 2.75 | 0.162 c |
| Left IOP (mmHg) | 14.00 ± 3.46 | 15.10 ± 3.04 | 0.460 a | 16.10 ± 4.04 | 12.90 ± 2.69 | 0.052 a |
| Mean IOP (mmHg) | 14.15 ± 2.97 | 15.45 ± 3.18 | 0.357 a | 15.80 ± 3.99 | 12.8 ± 2.37 | 0.060 c |
| BMI (kg/m2) | 24.43 ± 2.47 | 22.64 ± 3.41 | 0.215 a | 23.97 ± 3.70 | 23.02 ± 3.24 | 0.559 a |
| Glucose (mmol/L) | 6.82 ± 2.05 | 6.45 ± 1.16 | 0.971 d | 6.77 ± 1.54 | 6.20 ± 1.69 | 0.315 d |
| CRP (mg/L) | 1.12 ± 1.50 | 2.00 ± 1.06 | 0.055 d | 1.86 ± 2.79 | 0.73 ± 0.41 | 1.000 d |
| SBP (mmHg) | 137.50 ± 18.35 | 128.40 ± 11.40 | 0.120 a | 138.90 ± 14.45 | 138.10 ± 9.77 | 0.886 a |
| DBP (mmHg) | 81.00 ± 13.01 | 79.90 ± 9.42 | 0.831 a | 78.80 ± 6.46 | 82.70 ± 6.07 | 0.181 a |
| BCVA (logMAR) | 0.53 ± 0.34 | 0.80 ± 0.55 | 0.120 d | 0.49 ± 0.29 | 0.60 ± 0.28 | 0.396 a |
| AL (mm) | 23.26 ± 0.79 | 23.53 ± 0.51 | 0.377 a | 23.20 ± 0.84 | 23.73 ± 0.87 | 0.280 d |
| CCT (µm) | 549.30 ± 27.86 | 539.10 ± 35.16 | 0.481 a | 548.95 ± 55.88 | 526.60 ± 25.45 | 0.273 d |
| ACD (mm) | 3.35 ± 0.22 | 3.08 ± 0.44 | 0.010 a | 3.04 ± 0.17 | 3.23 ± 0.42 | 0.219 c |
| C/D ratio | 0.87 ± 0.05 | 0.32 ± 0.04 | <0.001 d | 0.88 ± 0.04 | 0.32 ± 0.04 | <0.001 d |
| Variables | Elevated TC and/or LDL-C | Normal TC and LDL-C | ||||
|---|---|---|---|---|---|---|
| POAG (n = 10) | Control (n = 10) | p Value | POAG (n = 10) | Control (n = 10) | p Value | |
| TC (mmol/L) | 6.31 ± 0.88 | 5.30 ± 0.40 | 0.006 c | 4.58 ± 0.42 | 4.16 ± 0.67 | 0.112 a |
| LDL-C (mmol/L) | 4.26 ± 0.90 | 3.53 ± 0.36 | 0.035 c | 2.66 ± 0.46 | 2.50 ± 0.53 | 0.483 a |
| HDL-C (mmol/L) | 1.39 ± 0.33 | 1.46 ± 0.43 | 0.688 a | 1.37 ± 0.25 | 1.28 ± 0.34 | 0.476 a |
| TG (mmol/L) | 2.08 ± 0.89 | 1.61 ± 0.74 | 0.222 a | 1.39 ± 0.64 | 1.07 ± 0.14 | 0.144 c |
| oxLDL (U/L) | 62.53 ± 14.31 | 50.05 ± 9.22 | 0.040 a | 49.03 ± 12.32 | 46.89 ± 9.79 | 0.672 a |
| Lpα (mg/L) | 133.90 ± 93.34 | 181.70 ± 145.34 | 0.393 a | 141.20 ± 127.41 | 95.30 ± 86.28 | 0.315 d |
| ApoB (g/L) | 1.10 ± 0.22 | 0.95 ± 0.13 | 0.064 a | 0.75 ± 0.16 | 0.75 ± 0.09 | 0.987 a |
| ApoAI (g/L) | 1.38 ± 0.30 | 1.31 ± 0.20 | 0.820 a | 1.24 ± 0.10 | 1.20 ± 0.23 | 0.639 c |
| ApoB/AI | 0.82 ± 0.16 | 0.74 ± 0.17 | 0.312 a | 0.61 ± 0.13 | 0.65 ± 0.16 | 0.535 a |
| IDL (mg/dL) | 48.41 ± 26.34 | 43.50 ± 11.76 | 0.600 a | 28.53 ± 10.22 | 24.65 ± 12.91 | 0.466 a |
| IDL-A (mg/dL) | 10.00 ± 4.09 | 10.57 ± 4.70 | 0.853 a | 9.27 ± 5.25 | 7.06 ± 3.20 | 0.270 a |
| IDL-B (mg/dL) | 4.77 ± 4.35 | 5.76 ± 4.04 | 0.570 d | 2.75 ± 2.74 | 1.95 ± 2.18 | 0.479 a |
| IDL-C (mg/dL) | 33.64 ± 22.93 | 27.18 ± 7.97 | 0.418 a | 16.51 ± 9.32 | 10.46 ± 3.31 | 0.847 a |
| LDL1 (mg/dL) | 53.14 ± 23.95 | 39.76 ± 13.68 | 0.142 a | 37.49 ± 10.92 | 36.80 ± 11.31 | 0.891 a |
| LDL2 (mg/dL) | 30.87 ± 16.49 | 31.94 ± 15.01 | 0.881 a | 20.65 ± 7.37 | 22.89 ± 9.98 | 0.576 a |
| LDL3 (mg/dL) | 29.43 ± 7.59 | 19.36 ± 10.49 | 0.025 a | 15.65 ± 9.90 | 10.93 ± 4.55 | 0.248 d |
| sdLDL (mg/dL) | 32.08 ± 6.69 | 21.36 ± 12.31 | 0.030 c | 16.17 ± 10.69 | 12.36 ± 5.10 | 0.481 d |
| L-HDL (mg/dL) | 11.40 ± 9.03 | 10.81 ± 8.09 | 0.971 d | 10.35 ± 6.48 | 9.15 ± 6.78 | 0.690 a |
| I-HDL (mg/dL) | 21.11 ± 7.75 | 23.44 ± 9.66 | 0.560 a | 21.76 ± 5.75 | 20.94 ± 7.40 | 0.787 a |
| S-HDL (mg/dL) | 21.07 ± 8.51 | 22.04 ± 4.86 | 0.759 a | 20.90 ± 5.78 | 19.20 ± 3.75 | 0.447 a |
| VLDL (mg/dL) | 51.00 ± 9.56 | 47.80 ± 5.83 | 0.378 a | 35.5 ± 4.97 | 33.6 ± 6.85 | 0.487 a |
| non-HDL (mmol/L) | 4.92 ± 0.67 | 3.85 ± 0.44 | 0.001 c | 3.21 ± 0.57 | 2.88 ± 0.52 | 0.192 a |
| TC/HDL-C ratio | 181.13 ± 29.40 | 150.42 ± 38.81 | 0.061 a | 133.44 ± 29.81 | 135.95 ± 40.64 | 0.739 a |
| oxLDL/HDL-C ratio | 46.67 ± 13.04 | 38.72 ± 19.16 | 0.301 a | 37.86 ± 15.71 | 39.53 ± 15.75 | 0.815 a |
| oxLDL/LDL-C ratio | 14.95 ± 3.04 | 14.38 ± 2.08 | 0.645 a | 18.47 ± 3.21 | 18.96 ± 2.72 | 0.716 a |
| oxLDL/TC ratio | 9.93 ± 1.90 | 9.60 ± 2.03 | 0.719 a | 10.70 ± 2.37 | 11.02 ± 1.40 | 0.717 a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, C.; Xu, J.; Chen, S.-L.; Chen, C.-B.; Liang, J.-J.; Liu, Z.; Huang, C.; Wu, Z.; Ng, T.K.; Zhang, M.; et al. Profile of Lipoprotein Subclasses in Chinese Primary Open-Angle Glaucoma Patients. Int. J. Mol. Sci. 2024, 25, 4544. https://doi.org/10.3390/ijms25084544
Fu C, Xu J, Chen S-L, Chen C-B, Liang J-J, Liu Z, Huang C, Wu Z, Ng TK, Zhang M, et al. Profile of Lipoprotein Subclasses in Chinese Primary Open-Angle Glaucoma Patients. International Journal of Molecular Sciences. 2024; 25(8):4544. https://doi.org/10.3390/ijms25084544
Chicago/Turabian StyleFu, Changzhen, Jianming Xu, Shao-Lang Chen, Chong-Bo Chen, Jia-Jian Liang, Zibo Liu, Chukai Huang, Zhenggen Wu, Tsz Kin Ng, Mingzhi Zhang, and et al. 2024. "Profile of Lipoprotein Subclasses in Chinese Primary Open-Angle Glaucoma Patients" International Journal of Molecular Sciences 25, no. 8: 4544. https://doi.org/10.3390/ijms25084544